Predictive Factors of 2-Year Postoperative Outcomes in Patients with Spontaneous Cerebellar Hemorrhage



 and
and
Abstract
:1. Introduction
2. Methods
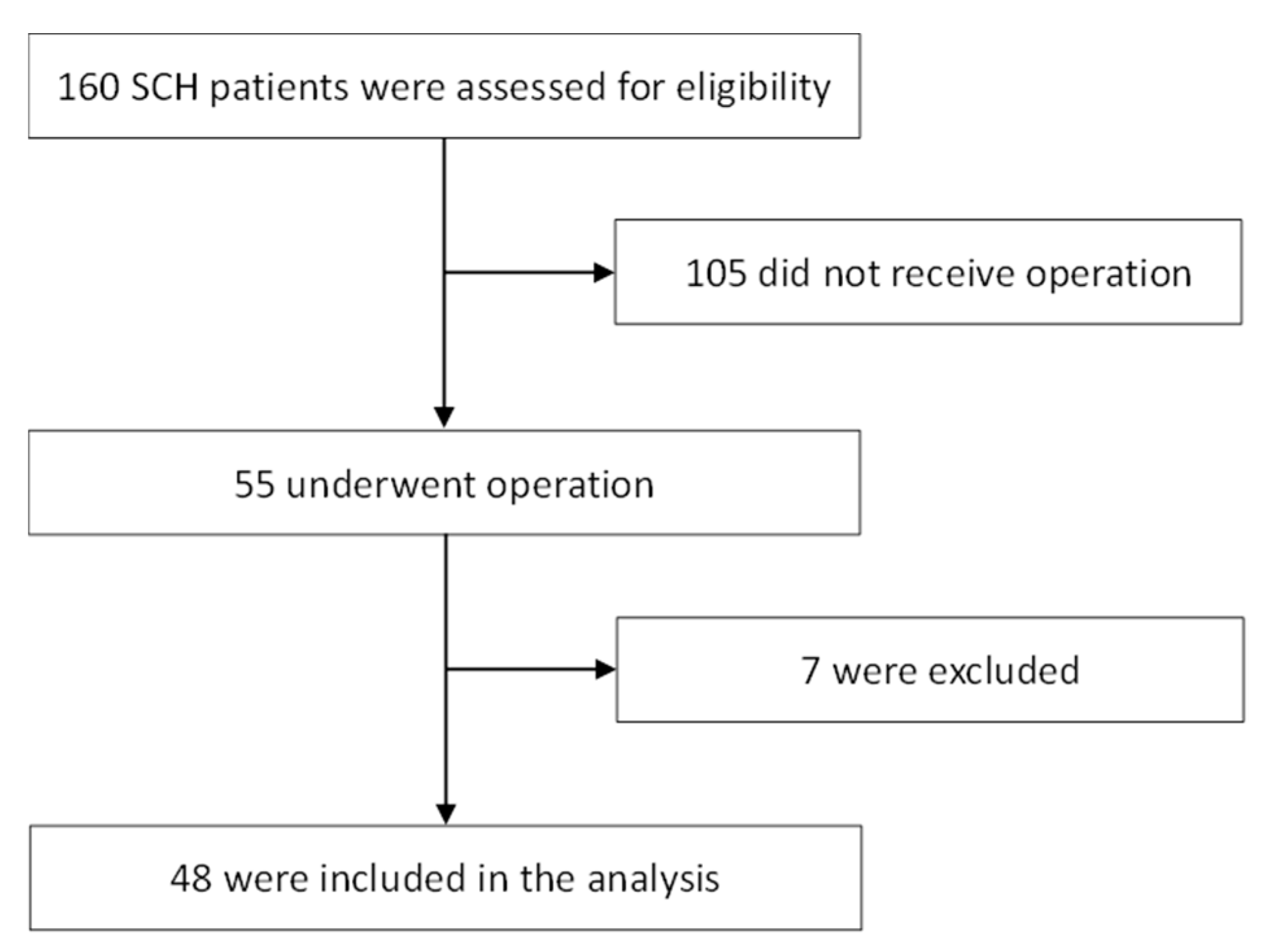
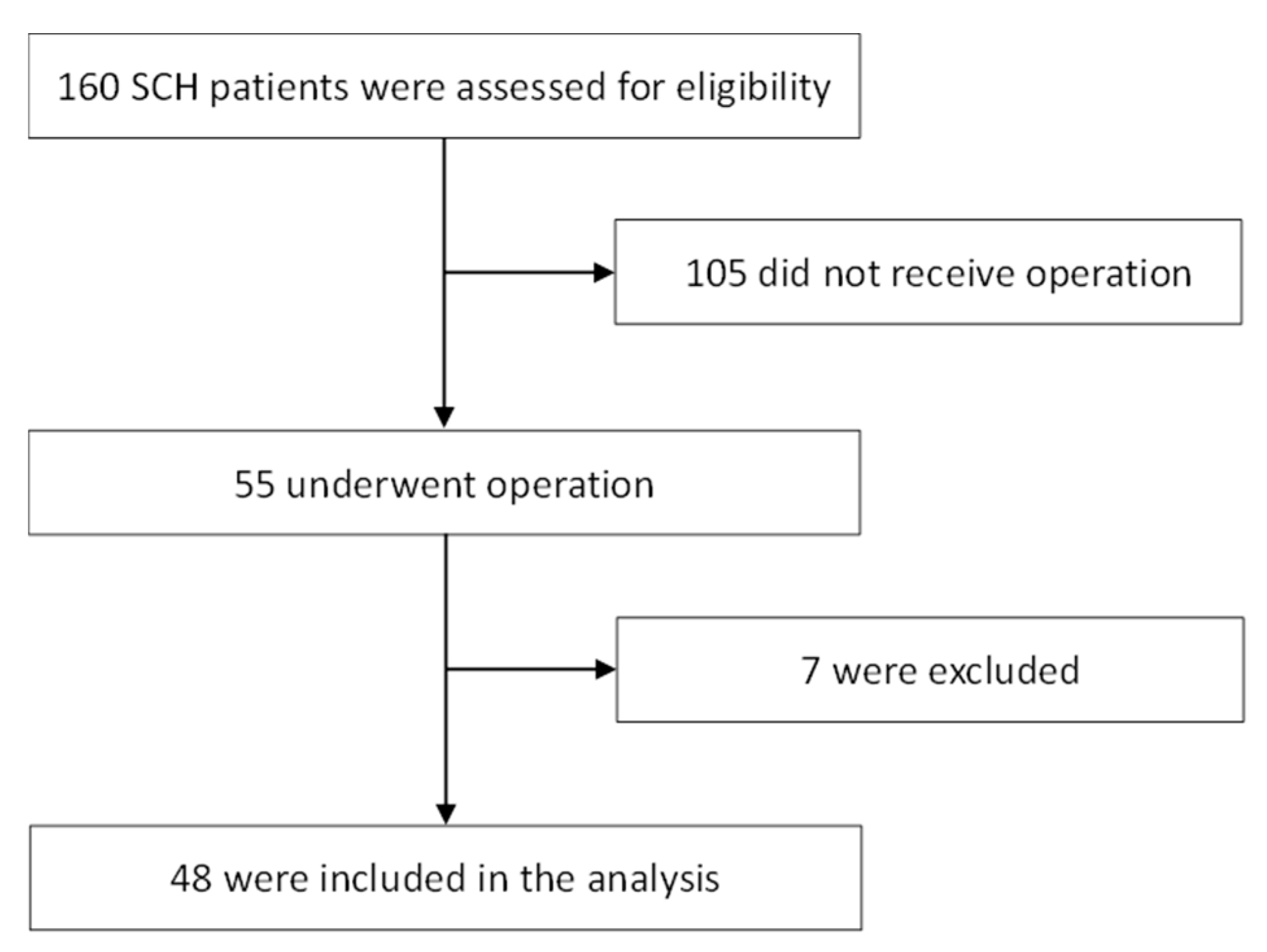
2.1. Patients and Study Design
2.2. Statistical Analysis
3. Results
3.1. Baseline Characteristics
3.2. Initial Radiological Findings
3.3. Surgical Treatment and Postoperative Outcome
3.4. Analysis of Factors with an Impact on Clinical Outcome
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
Availability of Data and Materials
Abbreviations
| AHA/ASA | American Heart Association and the American Stroke Association; |
| CT | Computed tomography; |
| EVD | External ventricular drainage; |
| ICH | Intracerebral hemorrhage; |
| GOS | Glasgow outcome scale; |
| GCS | Glasgow Coma Scale; |
| NIHSS | National Institutes of Health Stroke Scale; |
| SCH | Spontaneous cerebellar hemorrhage; |
| SD | Standard deviation |
References
- Lin, C.Y.; Chang, C.Y.; Sun, C.H.; Li, T.Y.; Chen, L.C.; Chang, S.T.; Wu, Y.T. Platelet count and early outcome in patients with spontaneous cerebellar hemorrhage: A retrospective study. PLoS ONE 2015, 10, e0119109. [Google Scholar] [CrossRef] [PubMed]
- Heros, R.C. Cerebellar hemorrhage and infarction. Stroke 1982, 13, 106–109. [Google Scholar] [CrossRef] [PubMed]
- Kirollos, R.W.; Tyagi, A.K.; Ross, S.A.; van Hille, P.T.; Marks, P.V. Management of spontaneous cerebellar hematomas: A prospective treatment protocol. Neurosurgery 2001, 49, 1378–1386; discussion 1386–1387. [Google Scholar] [CrossRef] [PubMed]
- Pong, V.; Chan, K.H.; Chong, B.H.; Lui, W.M.; Leung, G.K.; Tse, H.F.; Pu, J.K.; Siu, C.W. Long-term outcome and prognostic factors after spontaneous cerebellar hemorrhage. Cerebellum 2012, 11, 939–945. [Google Scholar] [CrossRef] [PubMed]
- Dammann, P.; Asgari, S.; Bassiouni, H.; Gasser, T.; Panagiotopoulos, V.; Gizewski, E.R.; Stolke, D.; Sure, U.; Sandalcioglu, I.E. Spontaneous cerebellar hemorrhage—Experience with 57 surgically treated patients and review of the literature. Neurosurg. Rev. 2011, 34, 77–86. [Google Scholar] [CrossRef] [PubMed]
- Hemphill, J.C., 3rd; Greenberg, S.M.; Anderson, C.S.; Becker, K.; Bendok, B.R.; Cushman, M.; Fung, G.L.; Goldstein, J.N.; Macdonald, R.L.; Mitchell, P.H.; et al. Guidelines for the Management of Spontaneous Intracerebral Hemorrhage: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2015, 46, 2032–2060. [Google Scholar] [CrossRef]
- Haley, E.C., Jr.; Kassell, N.F.; Torner, J.C. A randomized controlled trial of high-dose intravenous nicardipine in aneurysmal subarachnoid hemorrhage. A report of the Cooperative Aneurysm Study. J. Neurosurg. 1993, 78, 537–547. [Google Scholar] [CrossRef] [PubMed]
- Kothari, R.U.; Brott, T.; Broderick, J.P.; Barsan, W.G.; Sauerbeck, L.R.; Zuccarello, M.; Khoury, J. The ABCs of measuring intracerebral hemorrhage volumes. Stroke 1996, 27, 1304–1305. [Google Scholar] [CrossRef]
- Weisberg, L.A. Acute cerebellar hemorrhage and CT evidence of tight posterior fossa. Neurology 1986, 36, 858–860. [Google Scholar] [CrossRef]
- Herman, W.H.; Wareham, N.J. The diagnosis and classification of diabetes mellitus in nonpregnant adults. Prim. Care 1999, 26, 755–770. [Google Scholar] [CrossRef]
- Chobanian, A.V.; Bakris, G.L.; Black, H.R.; Cushman, W.C.; Green, L.A.; Izzo, J.L., Jr.; Jones, D.W.; Materson, B.J.; Oparil, S.; Wright, J.T., Jr.; et al. National High Blood Pressure Education Program Coordinating, C. The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure: The JNC 7 report. JAMA 2003, 289, 2560–2572. [Google Scholar] [CrossRef] [PubMed]
- Salvati, M.; Cervoni, L.; Raco, A.; Delfini, R. Spontaneous cerebellar hemorrhage: Clinical remarks on 50 cases. Surg. Neurol. 2001, 55, 156–161; discussion 161. [Google Scholar] [CrossRef]
- Van der Hoop, R.G.; Vermeulen, M.; van Gijn, J. Cerebellar hemorrhage: Diagnosis and treatment. Surg. Neurol. 1988, 29, 6–10. [Google Scholar] [CrossRef]
- Lui, T.N.; Fairholm, D.J.; Shu, T.F.; Chang, C.N.; Lee, S.T.; Chen, H.R. Surgical treatment of spontaneous cerebellar hemorrhage. Surg. Neurol. 1985, 23, 555–558. [Google Scholar] [CrossRef]
- Little, J.R.; Tubman, D.E.; Ethier, R. Cerebellar hemorrhage in adults. Diagnosis by computerized tomography. J. Neurosurg. 1978, 48, 575–579. [Google Scholar] [CrossRef] [PubMed]
- Freeman, R.E.; Onofrio, B.M.; Okazaki, H.; Dinapoli, R.P. Spontaneous intracerebellar hemorrhage. Diagnosis and surgical treatment. Neurology 1973, 23, 84–90. [Google Scholar] [CrossRef]
- Cohen, Z.R.; Ram, Z.; Knoller, N.; Peles, E.; Hadani, M. Management and outcome of non-traumatic cerebellar haemorrhage. Cerebrovasc. Dis. 2002, 14, 207–213. [Google Scholar] [CrossRef]
- Da Pian, R.; Bazzan, A.; Pasqualin, A. Surgical versus medical treatment of spontaneous posterior fossa haematomas: A cooperative study on 205 cases. Neurol. Res. 1984, 6, 145–151. [Google Scholar] [CrossRef]
- Firsching, R.; Huber, M.; Frowein, R.A. Cerebellar haemorrhage: Management and prognosis. Neurosurg. Rev. 1991, 14, 191–194. [Google Scholar] [CrossRef]
- Van Loon, J.; Van Calenbergh, F.; Goffin, J.; Plets, C. Controversies in the management of spontaneous cerebellar haemorrhage. A consecutive series of 49 cases and review of the literature. Acta Neurochir. 1993, 122, 187–193. [Google Scholar] [CrossRef]
- Mezzadri, J.J.; Otero, J.M.; Ottino, C.A. Management of 50 spontaneous cerebellar haemorrhages. Importance of obstructive hydrocephalus. Acta Neurochir. 1993, 122, 39–44. [Google Scholar] [CrossRef]
- Dolderer, S.; Kallenberg, K.; Aschoff, A.; Schwab, S.; Schwarz, S. Long-term outcome after spontaneous cerebellar haemorrhage. Eur. Neurol. 2004, 52, 112–119. [Google Scholar] [CrossRef]
- Dunne, J.W.; Chakera, T.; Kermode, S. Cerebellar haemorrhage—Diagnosis and treatment: A study of 75 consecutive cases. Q. J. Med. 1987, 64, 739–754. [Google Scholar]
- Kobayashi, S.; Sato, A.; Kageyama, Y.; Nakamura, H.; Watanabe, Y.; Yamaura, A. Treatment of hypertensive cerebellar hemorrhage—Surgical or conservative management? Neurosurgery 1994, 34, 246–250; discussion 250–251. [Google Scholar] [CrossRef]
- Shenkin, H.A.; Zavala, M. Cerebellar strokes: Mortality, surgical indications, and results of ventricular drainage. Lancet 1982, 2, 429–432. [Google Scholar] [CrossRef]
- St Louis, E.K.; Wijdicks, E.F.; Li, H.; Atkinson, J.D. Predictors of poor outcome in patients with a spontaneous cerebellar hematoma. Can. J. Neurol. Sci. 2000, 27, 32–36. [Google Scholar] [CrossRef]
- Pollak, L.; Rabey, J.M.; Gur, R.; Schiffer, J. Indication to surgical management of cerebellar hemorrhage. Clin. Neurol. Neurosurg. 1998, 100, 99–103. [Google Scholar] [CrossRef]
- Donauer, E.; Loew, F.; Faubert, C.; Alesch, F.; Schaan, M. Prognostic factors in the treatment of cerebellar haemorrhage. Acta Neurochir. 1994, 131, 59–66. [Google Scholar] [CrossRef]
- Brott, T.; Adams, H.P., Jr.; Olinger, C.P.; Marler, J.R.; Barsan, W.G.; Biller, J.; Spilker, J.; Holleran, R.; Eberle, R.; Hertzberg, V.; et al. Measurements of acute cerebral infarction: A clinical examination scale. Stroke 1989, 20, 864–870. [Google Scholar] [CrossRef]
- Kwiatkowski, T.G.; Libman, R.B.; Frankel, M.; Tilley, B.C.; Morgenstern, L.B.; Lu, M.; Broderick, J.P.; Lewandowski, C.A.; Marler, J.R.; Levine, S.R.; et al. Effects of tissue plasminogen activator for acute ischemic stroke at one year. National Institute of Neurological Disorders and Stroke Recombinant Tissue Plasminogen Activator Stroke Study Group. N. Engl. J. Med. 1999, 340, 1781–1787. [Google Scholar] [CrossRef]
- Adams, H.P., Jr.; Davis, P.H.; Leira, E.C.; Chang, K.C.; Bendixen, B.H.; Clarke, W.R.; Woolson, R.F.; Hansen, M.D. Baseline NIH Stroke Scale score strongly predicts outcome after stroke: A report of the Trial of Org 10172 in Acute Stroke Treatment (TOAST). Neurology 1999, 53, 126–131. [Google Scholar] [CrossRef]
- Olavarria, V.V.; Delgado, I.; Hoppe, A.; Brunser, A.; Carcamo, D.; Diaz-Tapia, V.; Lavados, P.M. Validity of the NIHSS in predicting arterial occlusion in cerebral infarction is time-dependent. Neurology 2011, 76, 62–68. [Google Scholar] [CrossRef]
- Fischer, U.; Arnold, M.; Nedeltchev, K.; Brekenfeld, C.; Ballinari, P.; Remonda, L.; Schroth, G.; Mattle, H.P. NIHSS score and arteriographic findings in acute ischemic stroke. Stroke 2005, 36, 2121–2125. [Google Scholar] [CrossRef]
- Singer, O.C.; Dvorak, F.; du Mesnil de Rochemont, R.; Lanfermann, H.; Sitzer, M.; Neumann-Haefelin, T. A simple 3-item stroke scale: Comparison with the National Institutes of Health Stroke Scale and prediction of middle cerebral artery occlusion. Stroke 2005, 36, 773–776. [Google Scholar] [CrossRef]

{kind=link}
| Glasgow Outcome Scale (2 years) | p Value | ||
|---|---|---|---|
| Good (n = 14) | Poor (n = 34) | ||
| Sex | 0.045 | ||
| Male | 11 (78.6) | 16 (47.1) | |
| Female | 3 (21.4) | 18 (52.9) | |
| Surgical timing | 0.575 | ||
| ≤6 h | 7 (50.0) | 14 (41.2) | |
| >6 h | 7 (50.0) | 20 (58.8) | |
| Operative method | 0.944 | ||
| Suboccipital craniectomy only | 3 (21.4) | 6 (17.6) | |
| Ventriculostomy only | 1 (7.1) | 3 (8.8) | |
| Suboccipital craniectomy and ventriculostomy | 10 (71.4) | 25 (73.5) | |
| Postoperative rebleeding | 0.656 | ||
| No | 13 (92.9) | 29 (85.3) | |
| Yes | 1 (7.1) | 5 (14.7) | |
| Alcohol | 1.000 | ||
| No | 12 (85.7) | 30 (88.2) | |
| Yes | 2 (14.3) | 4 (11.8) | |
| Smoking | 0.339 | ||
| No | 11 (78.6) | 31 (91.2) | |
| Yes | 3 (21.4) | 3 (8.8) | |
| Diabetes mellitus | 0.656 | ||
| No | 13 (92.9) | 29 (85.3) | |
| Yes | 1 (7.1) | 5 (14.7) | |
| GOS at 2 Years | p Value | ||
|---|---|---|---|
| Good (n = 14) | Poor (n = 34) | ||
| Age | 61.1 ± 11.4 (63, 43–77) | 63.8 ± 9.6 (63, 48–84) | 0.401 |
| GCS on admission | 11.9 ± 3.0 (13, 6–15) | 7.5 ± 4.6 (6, 3–15) | 0.002 |
| Pre-operative GCS | 10.5 ± 2.9 (9, 6–14) | 5.9 ± 3.6 (4, 3–15) | <0.001 |
| NIHSS at discharge | 10.6 ± 4.8 (12, 3–19) | 30.4 ± 9.9 (36, 7–38) | <0.001 |
| Hematoma volume | 16.6 ± 5.2 (16, 8–27) | 23.2 ± 7.9 (22, 14–39) | 0.006 |
| Hematoma diameter | 46.5 ± 9.0 (46, 31–63) | 48.6 ± 7.9 (47, 30–65) | 0.426 |
| Poor Outcome | ||
|---|---|---|
| Odds Ratio (95% CI) | p Value | |
| Age | 1.028 (0.965–1.096) | 0.393 |
| Sex (female) | 0.242 (0.057–1.027) | 0.054 |
| GCS on admission | 0.790 (0.669–0.933) | 0.006 |
| Pre-operative GCS | 0.721 (0.590–0.880) | 0.001 |
| NIHSS at discharge | 1.310 (1.086–1.580) | 0.005 |
| Hematoma volume | 1.165 (1.032–1.316) | 0.014 |
| Poor Outcome | ||
|---|---|---|
| Odds Ratio (95% CI) | p Value | |
| Age | 0.988 (0.862–1.132) | 0.862 |
| Sex (female) | 0.758 (0.063–9.197) | 0.828 |
| GCS on admission | 1.068 (0.648–1.760) | 0.795 |
| Pre-operative GCS | 0.687 (0.357–1.323) | 0.261 |
| NIHSS at discharge | 1.285 (1.045–1.580) | 0.018 |
| Hematoma volume | 0.966 (0.768–1.215) | 0.767 |
| Poor Outcome-Postoperative Mortality | ||
|---|---|---|
| Odds Ratio (95% CI) | p Value | |
| Age | 1.039 (0.944–1.145) | 0.433 |
| Sex (female) | 1.539 (0.302–7.838) | 0.603 |
| GCS on admission | 0.989 (0.766–1.277) | 0.932 |
| Pre-operative GCS | 0.815 (0.561–1.183) | 0.281 |
| NIHSS at discharge | 1.103 (1.012–1.202) | 0.025 |
| Hematoma volume | 0.983 (0.879–1.099) | 0.757 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lee, T.-H.; Huang, Y.-H.; Su, T.-M.; Chen, C.-F.; Lu, C.-H.; Lee, H.-L.; Tsai, H.-P.; Sung, W.-W.; Kwan, A.-L. Predictive Factors of 2-Year Postoperative Outcomes in Patients with Spontaneous Cerebellar Hemorrhage. J. Clin. Med. 2019, 8, 818. https://doi.org/10.3390/jcm8060818
Lee T-H, Huang Y-H, Su T-M, Chen C-F, Lu C-H, Lee H-L, Tsai H-P, Sung W-W, Kwan A-L. Predictive Factors of 2-Year Postoperative Outcomes in Patients with Spontaneous Cerebellar Hemorrhage. Journal of Clinical Medicine. 2019; 8(6):818. https://doi.org/10.3390/jcm8060818
Chicago/Turabian StyleLee, Tsung-Han, Yu-Hua Huang, Tsung-Ming Su, Chih-Feng Chen, Cheng-Hsien Lu, Hsiang-Lin Lee, Hui-Ping Tsai, Wen-Wei Sung, and Aij-Lie Kwan. 2019. "Predictive Factors of 2-Year Postoperative Outcomes in Patients with Spontaneous Cerebellar Hemorrhage" Journal of Clinical Medicine 8, no. 6: 818. https://doi.org/10.3390/jcm8060818
APA StyleLee, T.-H., Huang, Y.-H., Su, T.-M., Chen, C.-F., Lu, C.-H., Lee, H.-L., Tsai, H.-P., Sung, W.-W., & Kwan, A.-L. (2019). Predictive Factors of 2-Year Postoperative Outcomes in Patients with Spontaneous Cerebellar Hemorrhage. Journal of Clinical Medicine, 8(6), 818. https://doi.org/10.3390/jcm8060818