Phase I/II Study of Docetaxel and S-1 in Previously-Treated Patients with Advanced Non-Small Cell Lung Cancer: LOGIK0408

 , and
, and
Abstract
1. Introduction
2. Experimental Section
2.1. Eligibility
2.2. Treatment and Dose Escalation Schedules in the Phase I Study
2.3. Toxicity and Response Evaluation
2.4. Statistical Considerations
3. Results
3.1. Phase I Study
3.2. Patient Characteristics in Phase II Study
3.3. Toxicity
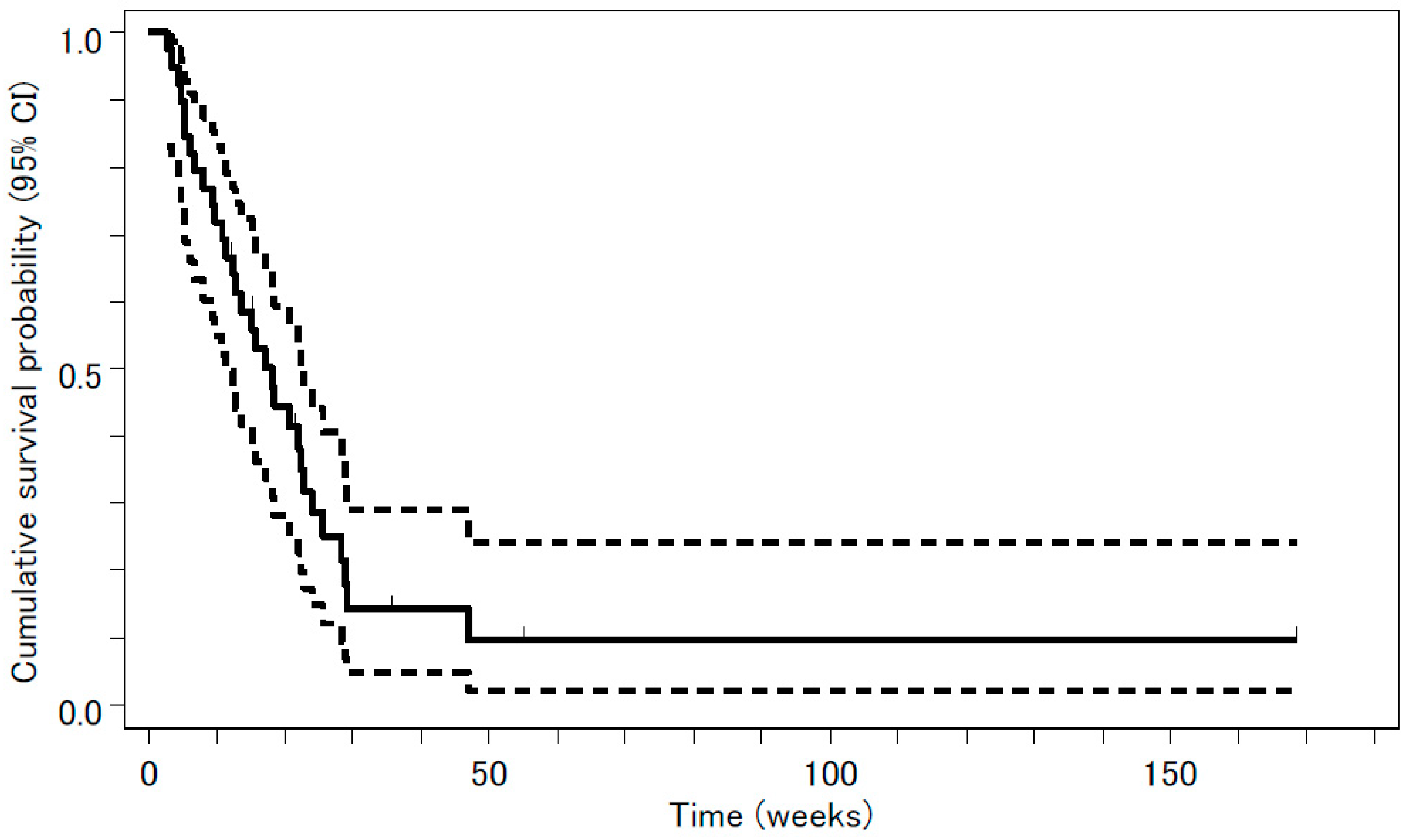
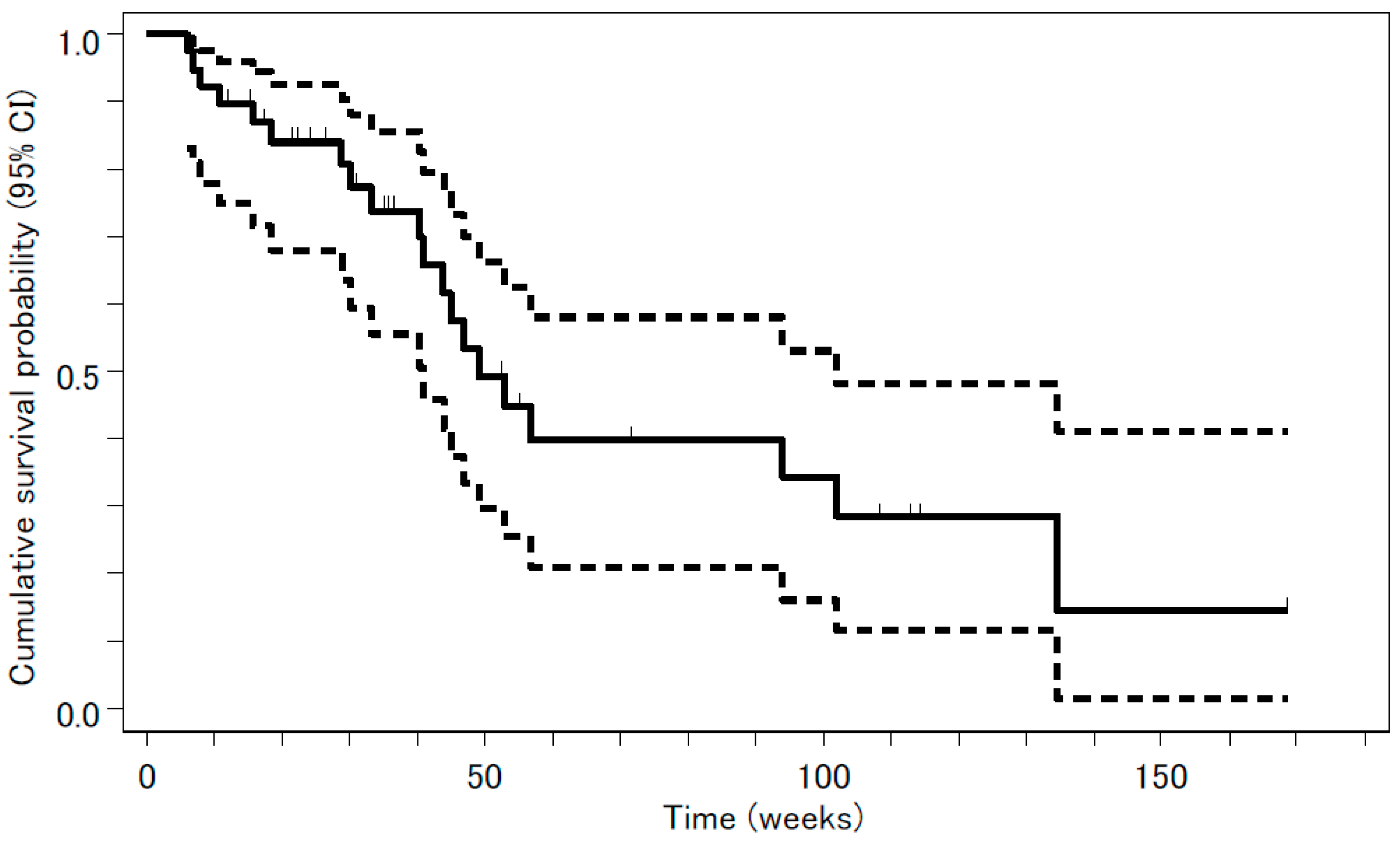
3.4. Efficacy
4. Discussion
Author Contributions
Funding
Acknowledgments
Conflicts of Interest
References
- Shepherd, F.A.; Dancey, J.; Ramlau, R.; Mattson, K.; Gralla, R.; O’Rourke, M.; Levitan, N.; Gressot, L.; Vincent, M.; Burkes, R.; et al. Prospective randomized trial of docetaxel versus best supportive care in patients with non-small cell lung cancer previously treated with platinum-based chemotherapy. J. Clin. Oncol. 2000, 18, 2095–2103. [Google Scholar] [CrossRef] [PubMed]
- Ringel, I.; Horwitz, S.B. Studies with RP 56976 (taxotere): A semisynthetic analogue of taxol. J. Natl. Cancer Inst. 1991, 83, 288–291. [Google Scholar] [CrossRef]
- Fossella, F.V.; DeVore, R.; Kerr, R.N.; Crawford, J.; Natale, R.R.; Dunphy, F.; Kalman, L.; Miller, V.; Lee, J.S.; Moore, M.; et al. Randomized phase III trial of docetaxel versus vinorelbine or ifosfamide in patients with advanced non-small cell lung cancer previously treated with platinum-containing chemotherapy regimens. J. Clin. Oncol. 2000, 18, 2354–2362. [Google Scholar] [CrossRef] [PubMed]
- Kubota, K.; Watanabe, K.; Kunitoh, H.; Noda, K.; Ichinose, Y.; Katakami, N.; Sugiura, T.; Kawahara, M.; Yokoyama, A.; Yokota, S.; et al. Phase III randomized trial of docetaxel plus cisplatin versus vindesine plus cisplatin in patients with stage IV non-small cell lung cancer: The Japanese Taxotere Lung Cancer Study Group. J. Clin. Oncol. 2004, 22, 254–261. [Google Scholar] [CrossRef] [PubMed]
- Fossella, F.V.; Rigas, J. The use of docetaxel (Taxotere) in patients with advanced non-small cell lung cancer previously treated with platinum-containing chemothepy regimens. Semin. Oncol. 1999, 26, 9–12. [Google Scholar] [PubMed]
- Kawahara, M.; Furuse, K.; Segawa, Y.; Yoshimori, K.; Matsui, K.; Kudoh, S.; Hasegawa, K.; Niitani, H.; S-1 Cooperative Study Group (Lung Cancer Working Group). Phase II study of S-1, a novel oral fluorouracil, in advanced non-small-cell lung cancer. Br. J. Cancer 2001, 85, 939–943. [Google Scholar] [CrossRef] [PubMed]
- Yoshida, K.; Ninomiya, N.; Takakura, N.; Hirabayashi, N.; Takiyama, W.; Sato, Y.; Todo, S.; Terashima, M.; Gotoh, M.; Sakamoto, J.; et al. Phase II study of docetaxel and S-1 combination therapy for advanced or recurrent gastric cancer. Clin. Cancer Res. 2006, 12, 3402–3407. [Google Scholar] [CrossRef]
- Kano, Y.; Akutsu, M.; Tsunoda, S.; Ando, J.; Matsui, J.; Suzuki, K.; Ikeda, T.; Inoue, Y.; Adachi, K. Schedule-dependent interaction between paclitaxel and 5-fluorouracil in human carcinoma cell lines in vitro. Br. J. Cancer 1996, 74, 704–710. [Google Scholar] [CrossRef][Green Version]
- Wada, Y.; Yoshida, K.; Suzuki, T.; Mizuiri, H.; Konishi, K.; Ukon, K.; Tanabe, K.; Sakata, Y.; Fukushima, M. Synergistic effects of docetaxel and S-1 by modulating the expression of metabolic enzymes of 5-fluorouracil in human gastric cancer cell lines. Int. J. Cancer 2006, 119, 783–791. [Google Scholar] [CrossRef]
- Yamaguchi, K.; Shimamura, T.; Hyodo, I.; Koizumi, W.; Doi, T.; Narahara, H.; Komatsu, Y.; Kato, T.; Saitoh, S.; Akiya, T.; et al. Phase I/II study of docetaxel and S-1 in patients with advanced gastric cancer. Br. J. Cancer 2006, 94, 1803–1808. [Google Scholar] [CrossRef]
- Park, S.R.; Kim, H.K.; Kim, C.G.; Choi, I.J.; Lee, J.S.; Lee, J.H.; Ryu, K.W.; Kim, Y.W.; Bae, J.M.; Kim, N.K. Phase I/II study of S-1 combined with weekly docetaxel in patients with metastatic gastric carcinoma. Br. J. Cancer 2008, 98, 1305–1311. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, M.; Miyajima, A.; Kosaka, T.; Yasumizu, Y.; Tanaka, N.; Maeda, T.; Shirotake, S.; Ide, H.; Kikuchi, E.; Oya, M. Low-dose docetaxel enhances the sensitivity of S-1 in a xenograft model of human castration resistant prostate cancer. Int. J. Cancer 2012, 130, 431–442. [Google Scholar] [CrossRef] [PubMed]
- Atagi, S.; Kawahara, M.; Kusunoki, Y.; Takada, M.; Kawaguchi, T.; Okishio, K.; Kubo, A.; Uehira, K.; Yumine, K.; Tomizawa, Y.; et al. Phase I/II study of docetaxel and S-1 in patients with previously treated non-small cell lung cancer. J. Thorac. Oncol. 2008, 3, 1012–1017. [Google Scholar] [CrossRef] [PubMed]
- Segawa, Y.; Kiura, K.; Hotta, K.; Takigawa, N.; Tabata, M.; Matsuo, K.; Yoshioka, H.; Hayashi, H.; Kawai, H.; Aoe, K.; et al. A randomized phase II study of a combination of docetaxel and S-1 versus docetaxel monotherapy in patients with non-small cell lung cancer previously treated with platinum-based chemotherapy. J. Thorac. Oncol. 2010, 5, 1430–1434. [Google Scholar] [CrossRef] [PubMed]
- Yanagihara, K.; Yoshimura, K.; Niimi, M.; Yasuda, H.; Sasaki, T.; Nishimura, T.; Ishiguro, H.; Matsumoto, S.; Kitano, T.; Kanai, M.; et al. Phase II study of S-1 and docetaxel for previously treated patients with locally advanced or metastatic non-small cell lung cancer. Cancer Chemother. Pharmacol. 2010, 66, 913–918. [Google Scholar] [CrossRef][Green Version]
- Oki, Y.; Hirose, T.; Yamaoka, T.; Kusumoto, S.; Shirai, T.; Sugiyama, T.; Okuda, K.; Nakashima, M.; Murata, Y.; Ohmori, T.; et al. Phase II study of S-1, a novel oral fluoropyrimidine, and biweekly administration of docetaxel for previously treated advanced non-small-cell lung cancer. Cancer Chemother. Pharmacol. 2011, 67, 791–797. [Google Scholar] [CrossRef][Green Version]
- Takiguchi, Y.; Tada, Y.; Gemma, A.; Kudoh, S.; Hino, M.; Yoshimori, K.; Yoshimura, A.; Nagao, K.; Niitani, H. Phase I/II study of docetaxel and S-1, an oral fluorinated pyrimidine, for untreated advanced non-small cell lung cancer. Lung Cancer 2010, 68, 409–414. [Google Scholar] [CrossRef]
- Maruyama, R.; Nishiwaki, Y.; Tamura, T.; Yamamoto, N.; Tsuboi, M.; Nakagawa, K.; Shinkai, T.; Negoro, S.; Imamura, F.; Eguchi, K.; et al. Phase III study, V-15-32, of gefitinib versus docetaxel in previously treated Japanese patients with non-small cell lung cancer. J. Clin. Oncol. 2008, 26, 4244–4252. [Google Scholar] [CrossRef]
- Takeda, M.; Okamoto, I.; Hirabayashi, N.; Kitano, M.; Nakagawa, K. Thymidiylate synthase and dihydropyrimidine dehydrogenase expression levels are associated with response to S-1 plus carboplatin in advanced non-small cell lung cancer. Lung Cancer 2011, 73, 103–109. [Google Scholar] [CrossRef]
- Ceppi, P.; Volante, M.; Saviozzi, S.; Rapa, I.; Novello, S.; Cambieri, A.; Lacono, M.L.; Cappia, S.; Papotti, M.; Scagliotti, G.V. Squamous cell carcinoma of the lung compared with other histotypes shows higher messenger RNA and protein levels for thymidylate synthase. Cancer 2006, 107, 1589–1596. [Google Scholar] [CrossRef]
- Chen, C.Y.; Chang, Y.L.; Shih, J.Y.; Lin, J.W.; Chen, K.Y.; Yang, C.H.; Yu, C.J.; Yang, P.C. Thymidylate synthase and dihydrofolate reductase expression in non-small cell lung carcinoma: The association with treatment efficacy of pemetrexed. Lung Cancer 2011, 74, 132–138. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
| Characteristics | N = 39 |
|---|---|
| Age, years | |
| Median (range) | 64 (46–75) |
| Sex | |
| Men | 31 |
| Women | 8 |
| ECOG PS | |
| 0 | 18 |
| 1 | 21 |
| Stage | |
| IIIb | 10 |
| IV | 29 |
| Histology | |
| Adenocarcinoma | 24 |
| Squamous cell carcinoma | 11 |
| Not specified | 4 |
| Toxicity | Grade | ||
|---|---|---|---|
| 3 | 4 | 3 + 4 | |
| Hematologic | |||
| Leukocytopenia | 15 (38.5%) | 2 (5.1%) | 17 (43.6%) |
| Neutropenia | 14 (35.9%) | 12 (30.8%) | 26 (66.7%) |
| Anemia | 0 (0%) | 0 (0%) | 0 (0%) |
| Thrombocytopenia | 0 (0%) | 0 (0%) | 0 (0%) |
| Nonhematologic | |||
| Loss of appetite | 3 (7.7%) | 0 (0%) | 3 (7.7%) |
| Fever | 2 (5.1%) | 0 (0%) | 2 (5.1%) |
| Pneumonitis | 1 (2.6%) | 1 (2.6%) | 2 (5.1%) |
| Stomatitis | 1 (2.6%) | 0 (0%) | 1 (2.6%) |
| Diarrhea | 1 (2.6%) | 0 (0%) | 1 (2.6%) |
| Hypercalcemia | 1 (2.6%) | 0 (0%) | 1 (2.6%) |
| Elevation of γGTP | 1 (2.6%) | 0 (0%) | 1 (2.6%) |
| Author | ||||
|---|---|---|---|---|
| Atagi et al. [12] | Yanagihara et al. [14] | Segawa et al. [13] | Oki et al. [15] | |
| N | 29 | 28 | 31 | 49 |
| Docetaxel | 40 mg/m2, day 1 every 3 weeks | 40 mg/m2, day 1 every 3 weeks | 40 mg/m2, day 1 every 3 weeks | 35 mg/m2, day 1, 15 every 4 weeks |
| S-1 | 80 mg/m2, days 1–14 | 80 mg/m2, days 1–14 | 80 mg/m2, days 1–15 | 80 mg/m2, days 1–14 |
| ORR | 24.1% | 18.4% | 16.1% | 16.3% |
| PFS (mo) | 3.9 | 4.4 | 3.4 | 3 |
| OS (mo) | 11.8 | 16.1 | 8.7 | 9 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Takayama, K.; Uchino, J.; Fujita, M.; Tokunaga, S.; Imanaga, T.; Morinaga, R.; Ebi, N.; Saeki, S.; Matsukizono, K.; Wataya, H.; et al. Phase I/II Study of Docetaxel and S-1 in Previously-Treated Patients with Advanced Non-Small Cell Lung Cancer: LOGIK0408. J. Clin. Med. 2019, 8, 2196. https://doi.org/10.3390/jcm8122196
Takayama K, Uchino J, Fujita M, Tokunaga S, Imanaga T, Morinaga R, Ebi N, Saeki S, Matsukizono K, Wataya H, et al. Phase I/II Study of Docetaxel and S-1 in Previously-Treated Patients with Advanced Non-Small Cell Lung Cancer: LOGIK0408. Journal of Clinical Medicine. 2019; 8(12):2196. https://doi.org/10.3390/jcm8122196
Chicago/Turabian StyleTakayama, Koichi, Junji Uchino, Masaki Fujita, Shoji Tokunaga, Tomotoshi Imanaga, Ryotaro Morinaga, Noriyuki Ebi, Sho Saeki, Kazuya Matsukizono, Hiroshi Wataya, and et al. 2019. "Phase I/II Study of Docetaxel and S-1 in Previously-Treated Patients with Advanced Non-Small Cell Lung Cancer: LOGIK0408" Journal of Clinical Medicine 8, no. 12: 2196. https://doi.org/10.3390/jcm8122196
APA StyleTakayama, K., Uchino, J., Fujita, M., Tokunaga, S., Imanaga, T., Morinaga, R., Ebi, N., Saeki, S., Matsukizono, K., Wataya, H., Yamada, T., & Nakanishi, Y. (2019). Phase I/II Study of Docetaxel and S-1 in Previously-Treated Patients with Advanced Non-Small Cell Lung Cancer: LOGIK0408. Journal of Clinical Medicine, 8(12), 2196. https://doi.org/10.3390/jcm8122196