Influence of Biologically Oriented Preparation Technique on Peri-Implant Tissues; Prospective Randomized Clinical Trial with Three-Year Follow-Up. Part I: Hard Tissues

 ,
,  , ,
, ,
Abstract
1. Introduction
2. Materials and Methods
2.1. Inclusion/Exclusion Criteria
2.2. Surgical Procedure
2.3. Sample Randomization
2.4. Sample Size Calculation
2.5. Prosthetic Crown Fabrication
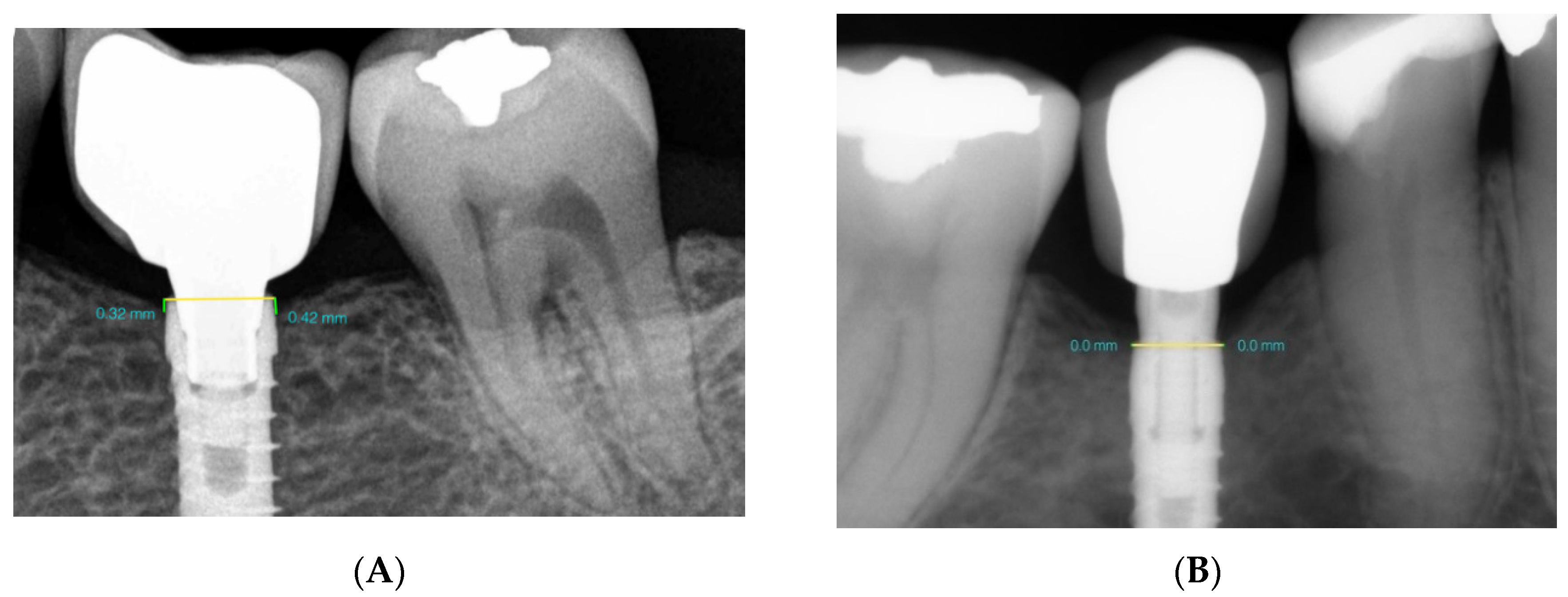
2.6. Radiological Marginal Bone Level Evaluation
2.7. Statistical Analysis
3. Results
3.1. Study Population
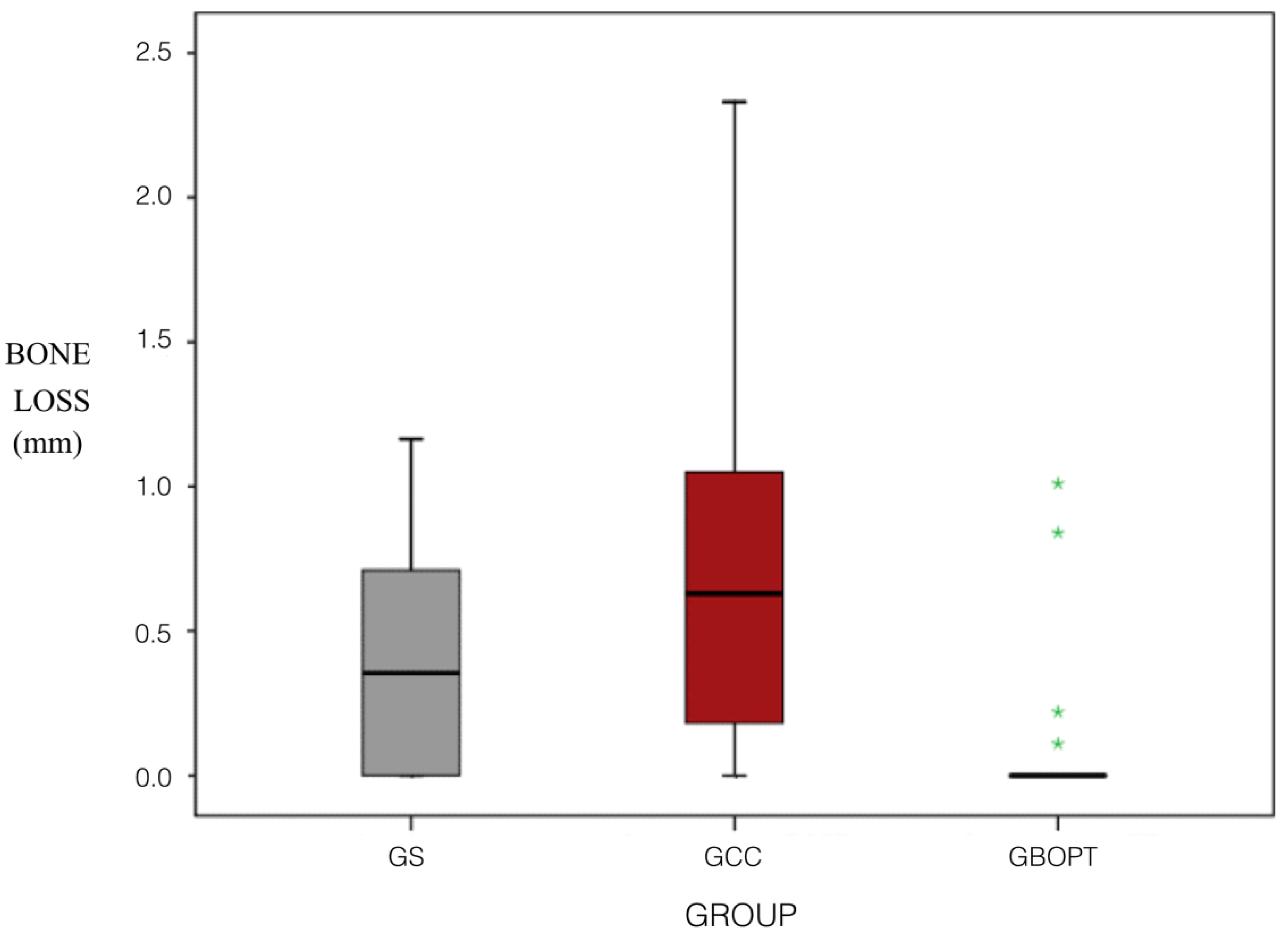
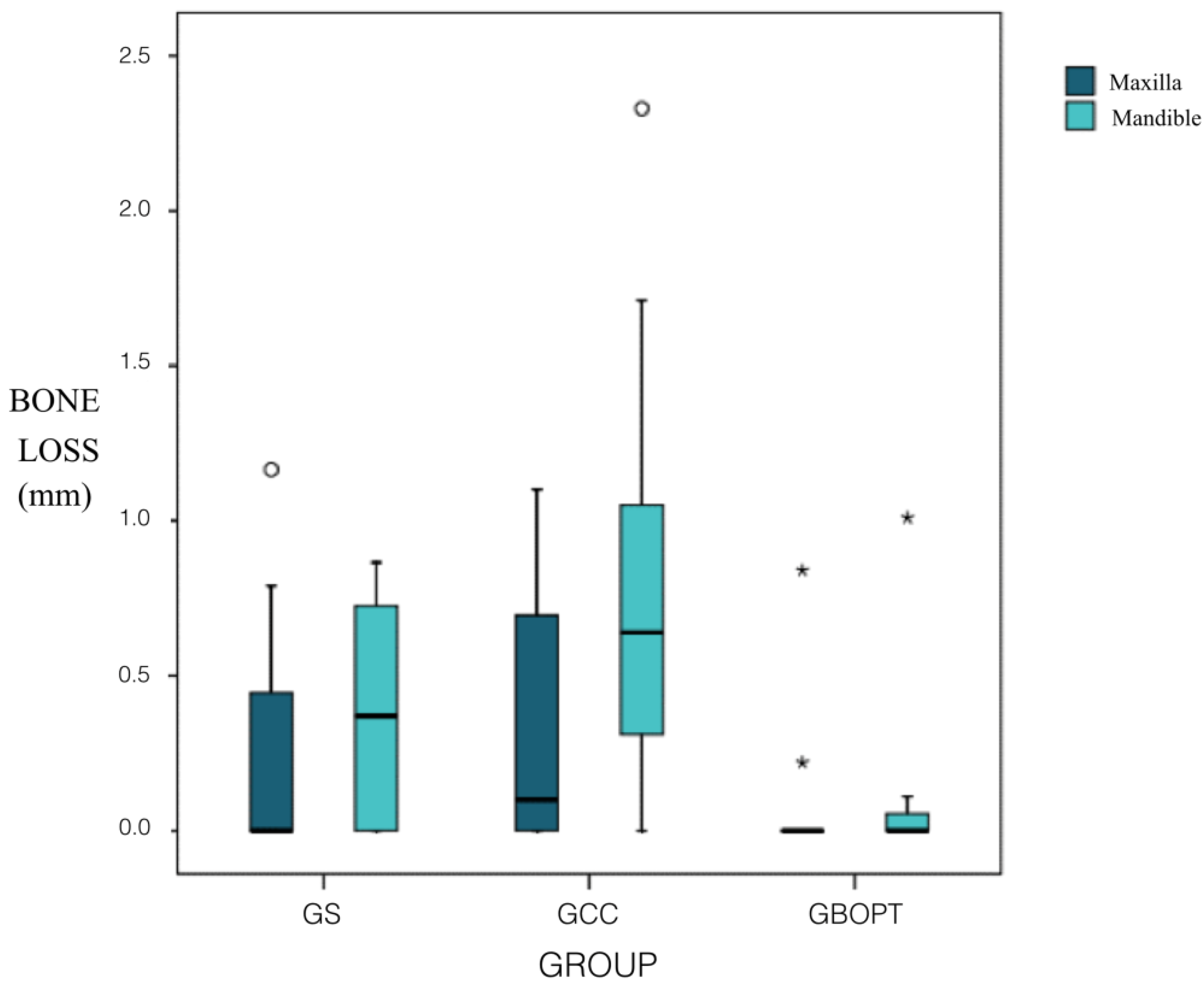
3.2. Bone Levels
3.3. Regression Analysis to Explore Sex, Age, and Position Factors
4. Discussion
5. Conclusions
Author Contributions
Acknowledgments
Conflicts of Interest
References
- Agustín-Panadero, R.; León-Martínez, R.; Labaig-Rueda, C.; Faus-López, J.; Solá-Ruíz, M.F. Influence of implant-prosthetic connection on peri-implant bone loss: A prospective clinical trial with 2-year follow-up. Int. J. Oral Maxillofac. Implants 2019, 34, 963–968. [Google Scholar] [CrossRef] [PubMed]
- Pellicer-Chover, H.; Peñarrocha-Oltra, D.; Aloy-Prosper, A.; Sanchis-Gonzalez, J.; Peñarrocha-Diago, M.; Peñarrocha-Diago, M. Comparison of peri-implant bone loss between conventional drilling with irrigation versus low-speed drilling without irrigation. Med. Oral Patol. Oral Cir. Bucal. 2017, 22, e730–e736. [Google Scholar] [CrossRef] [PubMed]
- Agustin-Panadero, R.; Serra-Pastor, B.; Roig-Vanaclocha, A.; Roman-Rodriguez, J.L.; Fons-Font, A. Mechanical behavior of provisional implant prosthetic abutments. Med. Oral Patol. Oral Cir. Bucal. 2015, 20, e94–e102. [Google Scholar] [CrossRef] [PubMed]
- Esposito, M.; Hirsch, J.-M.; Lekholm, U.; Thomsen, P. Biological factors contributing to failures of osseointegrated oral implants. (I). Success criteria and epidemiology. Eur. J. Oral Sci. 1998, 106, 527–551. [Google Scholar] [CrossRef]
- JOMI. The International Journal of Oral and Maxillofacial Implants, Official Journal of the Academy of Osseointegration. In Proceedings of the Fourth ITI Consensus Conference, Sponsored by the International Team for Implantology (ITI), Stuttgart, Germany, 26–28 August 2008. [Google Scholar]
- Dohan Ehrenfest, D.M.; Coelho, P.G.; Kang, B.-S.; Sul, Y.-T.; Albrektsson, T. Classification of osseointegrated implant surfaces: Materials, chemistry and topography. Trends Biotechnol. 2010, 28, 198–206. [Google Scholar] [CrossRef]
- Stanford, C.M. Biomechanical and functional behavior of implants. Adv. Dent. Res. 1999, 13, 88–92. [Google Scholar] [CrossRef]
- Buser, D.; Martin, W.; Belser, U.C. Optimizing esthetics for implant restorations in the anterior maxilla: Anatomic and surgical considerations. Int. J. Oral Maxillofac. Implants 2004, 14, 43–61. [Google Scholar]
- Heitz-Mayfield, L.J.A. Peri-implant diseases: Diagnosis and risk indicators. J. Clin. Periodontol. 2008, 35, 292–304. [Google Scholar] [CrossRef]
- Bornstein, M.M.; Cionca, N.; Mombelli, A. Systemic conditions and treatments as risks for implant therapy. Int. J. Oral Maxillofac. Implants 2009, 24, 12–27. [Google Scholar]
- Pjetursson, B.E.; Helbling, C.; Weber, H.-P.; Matuliene, G.; Salvi, G.E.; Brägger, U.; Schmidlin, K.; Zwahlen, M.; Lang, N.P. Peri-implantitis susceptibility as it relates to periodontal therapy and supportive care. Clin. Oral Implants Res. 2012, 23, 888–894. [Google Scholar] [CrossRef]
- Doornewaard, R.; Jacquet, W.; Cosyn, J.; De Bruyn, H. How do peri-implant biologic parameters correspond with implant survival and peri-implantitis? A critical review. Clin. Oral Implants Res. 2018, 29, 100–123. [Google Scholar] [CrossRef]
- Schwarz, F.; Derks, J.; Monje, A.; Wang, H.-L. Peri-implantitis. J. Clin. Periodontol. 2018, 45, S246–S266. [Google Scholar] [CrossRef]
- Sailer, I.; Mühlemann, S.; Zwahlen, M.; Hämmerle, C.H.F.; Schneider, D. Cemented and screw-retained implant reconstructions: A systematic review of the survival and complication rates. Clin. Oral Implants Res. 2012, 23, 163–201. [Google Scholar] [CrossRef]
- Linkevicius, T.; Vindasiute, E.; Puisys, A.; Peciuliene, V. The influence of margin location on the amount of undetected cement excess after delivery of cement-retained implant restorations: Cement excess around subgingival margins. Clin. Oral Implants Res. 2011, 22, 1379–1384. [Google Scholar] [CrossRef]
- Agar, J.R.; Cameron, S.M.; Hughbanks, J.C.; Parker, M.H. Cement removal from restorations luted to titanium abutments with simulated subgingival margins. J. Prosthet. Dent. 1997, 78, 43–47. [Google Scholar] [CrossRef]
- Wilson, T.G., Jr. The positive relationship between excess cement and peri-implant disease: A prospective clinical endoscopic study. J. Periodontol. 2009, 80, 1388–1392. [Google Scholar] [CrossRef]
- Cacaci, C.; Cantner, F.; Mücke, T.; Randelzhofer, P.; Hajtó, J.; Beuer, F. Clinical performance of screw-retained and cemented implant-supported zirconia single crowns: 36-month results. Clin. Oral Investig. 2017, 21, 1953–1959. [Google Scholar] [CrossRef]
- Chee, W.; Jivraj, S. Screw versus cemented implant supported restorations. Br. Dent. J. 2006, 201, 501–507. [Google Scholar] [CrossRef]
- Rismanchian, M.; Birang, R.; Shahmoradi, M.; Talebi, H.; Zare, R.J. Developing a new dental implant design and comparing its biomechanical features with four designs. Dent. Res. J. (Isfahan) 2010, 7, 70–75. [Google Scholar]
- Crespi, R.; Capparè, P.; Gastaldi, G.; Gherlone, E. Immediate occlusal loading of full-arch rehabilitations: Screw-retained versus cement-retained prosthesis. An 8-year clinical evaluation. Int. J. Oral Maxillofac. Implants 2014, 29, 1406–1411. [Google Scholar] [CrossRef]
- Cocchetto, R.; Canullo, L. The “hybrid abutment”: A new design for implant cemented restorations in the esthetic zones. Int. J. Esthet. Dent. 2015, 10, 186–208. [Google Scholar]
- Canullo, L.; Tallarico, M.; Pradies, G.; Marinotti, F.; Loi, I.; Cocchetto, R. Soft and hard tissue response to an implant with a convergent collar in the esthetic area: Preliminary report at 18 months. Int. J. Esthet. Dent. 2017, 12, 306–323. [Google Scholar]
- Canullo, L.; Menini, M.; Covani, U.; Pesce, P. Clinical outcomes of using a prosthetic protocol to rehabilitate tissue-level implants with a convergent collar in the esthetic zone: A 3-year prospective study. J. Prosthet. Dent. 2019. [Google Scholar] [CrossRef]
- Sanz-Martín, I.; Sanz-Sánchez, I.; Noguerol, F.; Cok, S.; Ortiz-Vigón, A.; Sanz, M. Randomized controlled clinical trial comparing two dental implants with different neck configurations. Clin. Implant Dent. Relat. Res. 2017, 19, 512–522. [Google Scholar] [CrossRef]
- Callan, D.P.; O’Mahony, A.; Cobb, C.M. Loss of crestal bone around dental implants: A retrospective study. Implant Dent. 1998, 7, 258–266. [Google Scholar] [CrossRef]
- Patri, C.; Zamparini, F.; Pirani, C. Multifactorial statistical analysis toward evaluation of MBL, PES and PI of a novel non submerged implant to restore a single tooth: A 1-year retrospective cohort study. J. Oral Sci. Rehabil. 2017, 3, 32–41. [Google Scholar]
- Peñarrocha-Diago, M.A.; Flichy-Fernández, A.J.; Alonso-González, R.; Peñarrocha-Oltra, D.; Balaguer-Martínez, J.; Peñarrocha-Diago, M. Influence of implant neck design and implant-abutment connection type on peri-implant health. Radiological study. Clin. Oral Implants Res. 2012, 24, 1192–1200. [Google Scholar] [CrossRef]
- Marconcini, S.; Giammarinaro, E.; Covani, U.; Mijiritsky, E.; Vela, X.; Rodríguez, X. The effect of tapered abutments on marginal bone level: A retrospective cohort study. J. Clin. Med. 2019, 8, 1305. [Google Scholar] [CrossRef]
- Piao, C.M.; Lee, J.E.; Koak, J.Y.; Kim, S.K.; Rhyu, I.C.; Han, C.H.; Herr, Y.; Heo, S.J. Marginal bone loss around three different implant systems: Radiographic evaluation after 1 year. J. Oral Rehabil. 2009, 36, 748–754. [Google Scholar] [CrossRef]
- Spinato, S.; Galindo-Moreno, P.; Bernardello, F.; Zaffe, D. Minimum abutment height to eliminate bone loss: Influence of implant neck design and platform switching. Int. J. Oral Maxillofac. Implants 2018, 33, 405–411. [Google Scholar] [CrossRef]
- Agustín-Panadero, R.; Martínez-Martínez, N.; Fernandez-Estevan, L.; Faus-López, J.; Solá-Ruíz, M.F. Influence of transmucosal area morphology on peri-implant bone loss in tissue-level implants. Int. J. Oral Maxillofac. Implants 2019, 34, 947–952. [Google Scholar] [CrossRef]
- Nissan, J.; Narobai, D.; Gross, O.; Ghelfan, O.; Chaushu, G. Long-term outcome of cemented versus screw-retained implant-supported partial restorations. Int. J. Oral Maxillofac. Implants 2011, 26, 1102–1107. [Google Scholar]
- Vigolo, P.; Odont, D.; Givani, A.; Majzoub, Z.; Cordioli, G. Cemented versus screw-retained implant-supported single-tooth crowns: A 4-year prospective clinical study. Eur. J. Oral Implantol. 2012, 5, 355–364. [Google Scholar]
- Weber, H.P.; Sukotjo, C. Does the type of implant prosthesis affect outcomes in the partially edentulous patient? Int. J. Oral Maxillofac. Implants 2007, 22, 140–172. [Google Scholar]
- Ghahroudi, A.R.; Talaeepour, A.; Mesgarzadeh, A.; Rokn, A.; Khorsand, A.; Mesgarzadeh, N.; Fard, M.K. Radiographic vertical bone loss evaluation around dental implants following one year of functional loading. J. Dent. (Tehran) 2010, 7, 89–97. [Google Scholar]
- Tawil, G.; Mawla, M.; Gottlow, J. Clinical and radiographic evaluation of the 5-mm diameter regular-platform Branemark fixture: 2- to 5-year follow-up. Clin. Implant Dent. Relat. Res. 2002, 4, 16–26. [Google Scholar] [CrossRef]
- Carlsson, G.E.; Lindquist, L.W.; Jemt, T. Long-term marginal periimplant bone loss in edentulous patients. Int. J. Prosthodont. 2000, 13, 295–302. [Google Scholar]
- Penarrocha, M.; Palomar, M.; Sanchís, J.M.; Guarinos, J.; Balaguer, J. Radiologic study of marginal bone loss around 108 dental implants and its relationship to smoking, implant location and morphology. Int. J. Oral Maxillofac. Implants 2004, 19, 861–867. [Google Scholar]
- Lopez, M.A.; AndreasiBassi, M.; Confalone, L.; Gaudio, R.M.; Lombardo, L.; Lauritano, D. The influence of ‘conical plus octagonal’ internal connection on implant survival and success rate: A retrospective study of 66 fixtures. J. Biol. Regul. Homeost. Agents 2016, 30, 49–54. [Google Scholar]
- Ho, K.-N.; Salamanca, E.; Lin, H.-K.; Lee, S.-Y.; Chang, W.-J. Marginal bone level evaluation after functional loading around two different dental implant designs. Biomed. Res. Int. 2016, 2016, 1472090. [Google Scholar] [CrossRef]
- Negri, M.; Galli, C.; Smerieri, A.; Macaluso, G.M.; Manfredi, E.; Ghiacci, G.; Toffoli, A.; Bonanini, M.; Lumetti, S. The effect of age, gender, and insertion site on marginal bone loss around endosseous implants: Results from a 3-year trial with premium implant system. Biomed. Res. Int. 2014, 2014, 369051. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Female | Male | Total | |
|---|---|---|---|
| Number of Patients | 49 | 26 | 75 |
| Number of Implants | 49 | 26 | 75 |
| Mean Age | − | − | 42.7 ± 10.6 |
| GROUP | ||||
|---|---|---|---|---|
| TOTAL | Screw-Retained | Cemented BOPT | Cemented Conventional | |
| N | 68 | 25 | 21 | 22 |
| Mean | 0.38 | 0.35 | 0.10 | 0.67 |
| Standard deviation | 0.50 | 0.37 | 0.28 | 0.62 |
| Minimum | 0.00 | 0.00 | 0.00 | 0.00 |
| Maximum | 2.33 | 1.17 | 1.01 | 2.33 |
| Median | 0.14 | 0.36 | 0.00 | 0.63 |
| Model | Unstandardized Coefficients | Standardized Coefficients | t | Sig. | 95% Confidence Interval for B | ||
|---|---|---|---|---|---|---|---|
| B | Std. Error | Beta | Lower Bound | Upper Bound | |||
| (Constant) | 0.173 | 0.273 | 0.634 | 0.529 | −0.373 | 0.719 | |
| GCC | 0.303 | 0.128 | 0.288 | 2.364 | 0.021 | 0.047 | 0.560 |
| GBOPT | −0.160 | 0.132 | −0.150 | −1.213 | 0.230 | −0.423 | 0.104 |
| ARCH (mdb) | 0.047 | 0.131 | 0.047 | 0.356 | 0.723 | −0.215 | 0.308 |
| MOLAR (yes) | 0.273 | 0.129 | 0.276 | 2.117 | 0.038 | 0.015 | 0.531 |
| SEX (female) | −0.097 | 0.111 | −0.097 | −0.879 | 0.383 | −0.319 | 0.124 |
| AGE | 0.001 | 0.005 | 0.016 | 0.149 | 0.882 | −0.010 | 0.011 |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Agustín-Panadero, R.; Bustamante-Hernández, N.; Solá-Ruíz, M.F.; Zubizarreta-Macho, Á.; Fons-Font, A.; Fernández-Estevan, L. Influence of Biologically Oriented Preparation Technique on Peri-Implant Tissues; Prospective Randomized Clinical Trial with Three-Year Follow-Up. Part I: Hard Tissues. J. Clin. Med. 2019, 8, 2183. https://doi.org/10.3390/jcm8122183
Agustín-Panadero R, Bustamante-Hernández N, Solá-Ruíz MF, Zubizarreta-Macho Á, Fons-Font A, Fernández-Estevan L. Influence of Biologically Oriented Preparation Technique on Peri-Implant Tissues; Prospective Randomized Clinical Trial with Three-Year Follow-Up. Part I: Hard Tissues. Journal of Clinical Medicine. 2019; 8(12):2183. https://doi.org/10.3390/jcm8122183
Chicago/Turabian StyleAgustín-Panadero, Rubén, Naia Bustamante-Hernández, María Fernanda Solá-Ruíz, Álvaro Zubizarreta-Macho, Antonio Fons-Font, and Lucía Fernández-Estevan. 2019. "Influence of Biologically Oriented Preparation Technique on Peri-Implant Tissues; Prospective Randomized Clinical Trial with Three-Year Follow-Up. Part I: Hard Tissues" Journal of Clinical Medicine 8, no. 12: 2183. https://doi.org/10.3390/jcm8122183
APA StyleAgustín-Panadero, R., Bustamante-Hernández, N., Solá-Ruíz, M. F., Zubizarreta-Macho, Á., Fons-Font, A., & Fernández-Estevan, L. (2019). Influence of Biologically Oriented Preparation Technique on Peri-Implant Tissues; Prospective Randomized Clinical Trial with Three-Year Follow-Up. Part I: Hard Tissues. Journal of Clinical Medicine, 8(12), 2183. https://doi.org/10.3390/jcm8122183