Total Reference Air Kerma is Associated with Late Bowel Morbidity in Locally Advanced Cervical Cancer Patients Treated with Image-Guided Adaptive Brachytherapy



Abstract
1. Introduction
2. Materials and methods
2.1. Patients
2.2. Treatments
2.3. Follow Up
2.4. Statistical Analysis
3. Results
3.1. Patients
3.2. Treatments
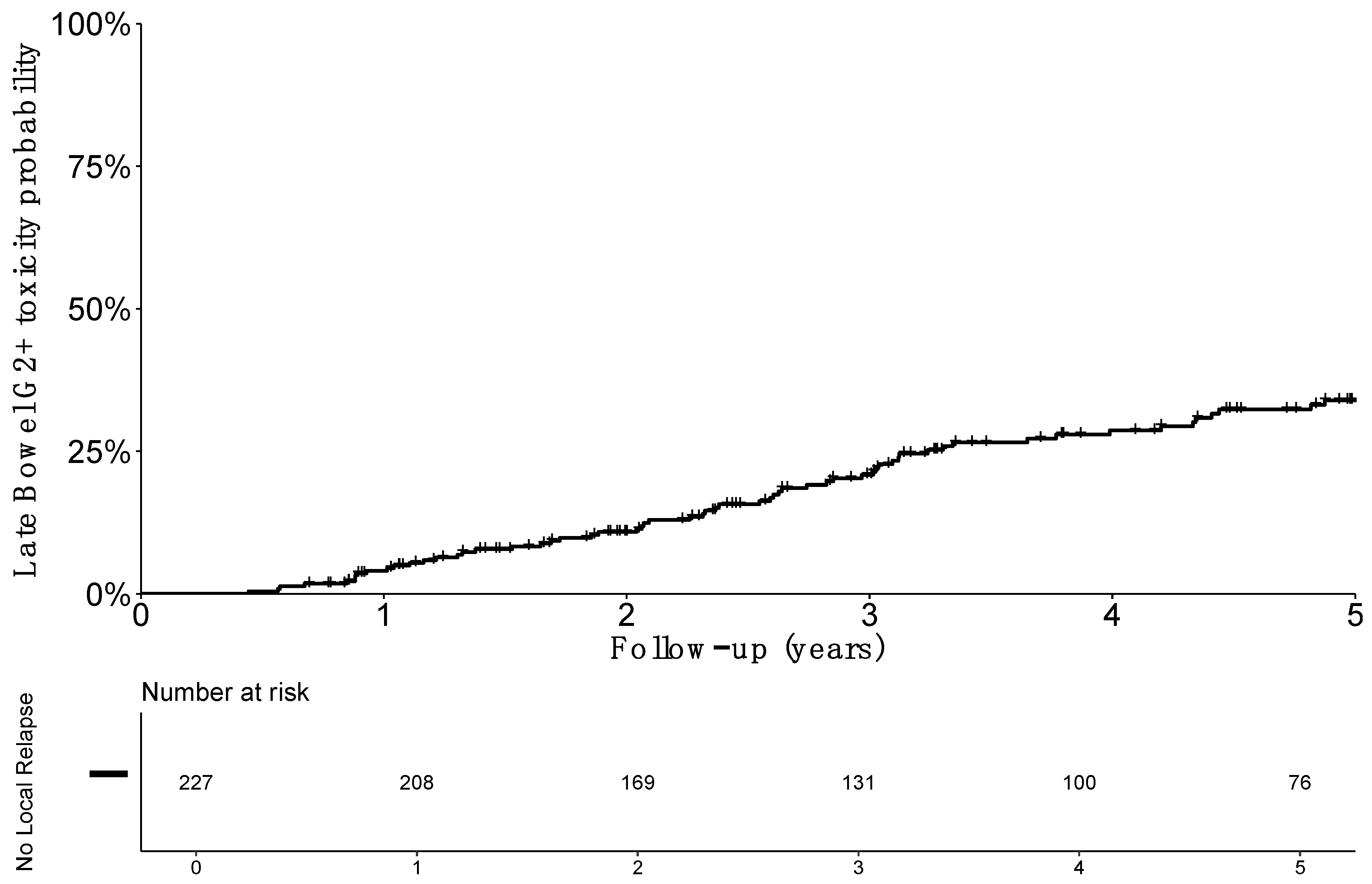
3.3. Toxicity
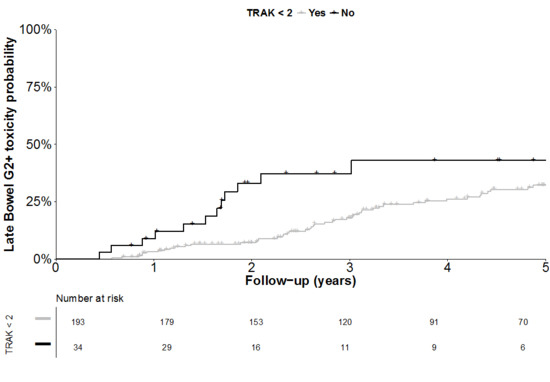
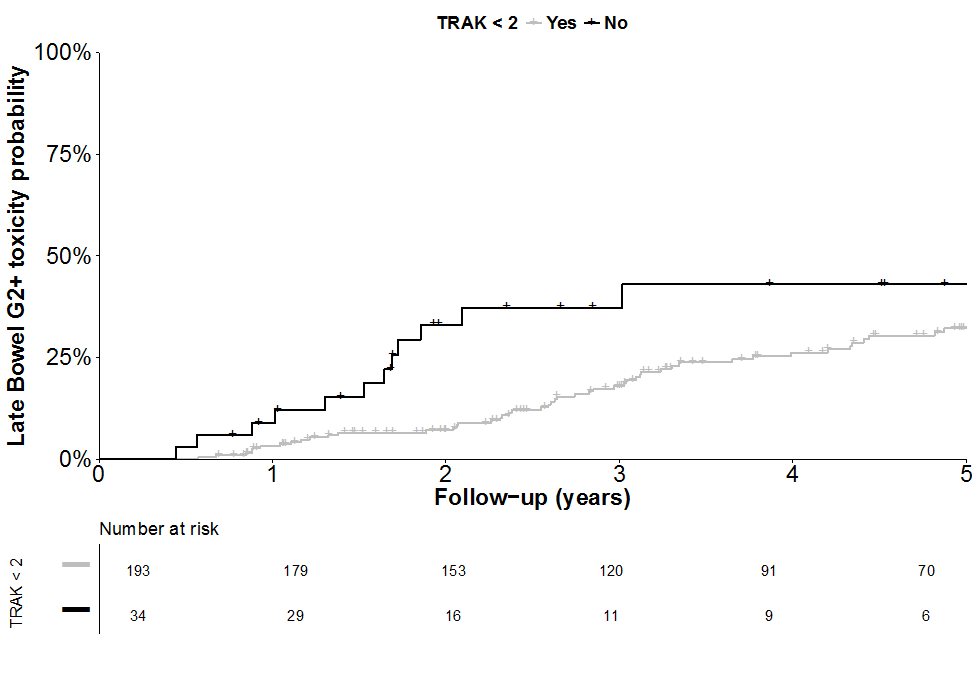
3.4. Factors Associated with Gastrointestinal Morbidity
4. Discussion
5. Conclusions
Author Contributions
Conflicts of Interest
References
- Haie-Meder, C.; Morice, P.; Castiglione, M. Cervical cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. Off. J. Eur. Soc. Med. Oncol. 2010, 21 (Suppl. 5), v37–v40. [Google Scholar] [CrossRef] [PubMed]
- Tanderup, K.; Eifel, P.J.; Yashar, C.M.; Pötter, R.; Grigsby, P.W. Curative Radiation Therapy for Locally Advanced Cervical Cancer: Brachytherapy Is NOT Optional. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 537–539. [Google Scholar] [CrossRef] [PubMed]
- Han, K.; Milosevic, M.; Fyles, A.; Pintilie, M.; Viswanathan, A.N. Trends in the Utilization of Brachytherapy in Cervical Cancer in the United States. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 111–119. [Google Scholar] [CrossRef] [PubMed]
- Prescribing, A. Recording, and Reporting Brachytherapy for Cancer of the Cervix. J. ICRU 2013, 13. [Google Scholar] [CrossRef]
- Haie-Meder, C.; Pötter, R.; Limbergen, E.V.; Briot, E.; Brabandere, M.D.; Dimopoulos, J.; Dumas, I.; Hellebust, T.P.; Kirisits, C.; Lang, S.; et al. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (I): Concepts and terms in 3D image based 3D treatment planning in cervix cancer brachytherapy with emphasis on MRI assessment of GTV and CTV. Radiother. Oncol. 2005, 74, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Pötter, R.; Haie-Meder, C.; Van Limbergen, E.; Barillot, I.; De Brabandere, M.; Dimopoulos, J.; Dumas, I.; Erickson, B.; Lang, S.; Nulens, A.; et al. Recommendations from gynaecological (GYN) GEC ESTRO working group (II): Concepts and terms in 3D image-based treatment planning in cervix cancer brachytherapy-3D dose volume parameters and aspects of 3D image-based anatomy, radiation physics, radiobiology. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2006, 78, 67–77. [Google Scholar] [CrossRef] [PubMed]
- Georg, P.; Pötter, R.; Georg, D.; Lang, S.; Dimopoulos, J.C.A.; Sturdza, A.E.; Berger, D.; Kirisits, C.; Dörr, W. Dose Effect Relationship for Late Side Effects of the Rectum and Urinary Bladder in Magnetic Resonance Image-Guided Adaptive Cervix Cancer Brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2012, 82, 653–657. [Google Scholar] [CrossRef]
- Mazeron, R.; Maroun, P.; Castelnau-Marchand, P.; Dumas, I.; del Campo, E.R.; Cao, K.; Slocker-Escarpa, A.; M’Bagui, R.; Martinetti, F.; Tailleur, A.; et al. Pulsed-dose rate image-guided adaptive brachytherapy in cervical cancer: Dose-volume effect relationships for the rectum and bladder. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2015, 116, 226–232. [Google Scholar] [CrossRef]
- Denham, J.W.; Hauer-Jensen, M. Radiation induced bowel injury: A neglected problem. Lancet Lond. Engl. 2013, 382, 2046–2047. [Google Scholar] [CrossRef]
- Kuku, S.; Fragkos, C.; McCormack, M.; Forbes, A. Radiation-induced bowel injury: The impact of radiotherapy on survivorship after treatment for gynaecological cancers. Br. J. Cancer 2013, 109, 1504–1512. [Google Scholar] [CrossRef]
- Rijkmans, E.C.; Nout, R.A.; Rutten, I.H.H.M.; Ketelaars, M.; Neelis, K.J.; Laman, M.S.; Coen, V.L.M.A.; Gaarenstroom, K.N.; Kroep, J.R.; Creutzberg, C.L. Improved survival of patients with cervical cancer treated with image-guided brachytherapy compared with conventional brachytherapy. Gynecol. Oncol. 2014, 135, 231–238. [Google Scholar] [CrossRef] [PubMed]
- Chopra, S.; Dora, T.; Chinnachamy, A.N.; Thomas, B.; Kannan, S.; Engineer, R.; Mahantshetty, U.; Phurailatpam, R.; Paul, S.N.; Shrivastava, S.K. Predictors of grade 3 or higher late bowel toxicity in patients undergoing pelvic radiation for cervical cancer: Results from a prospective study. Int. J. Radiat. Oncol. Biol. Phys. 2014, 88, 630–635. [Google Scholar] [CrossRef] [PubMed]
- Mabuchi, S.; Okazawa, M.; Isohashi, F.; Matsuo, K.; Ohta, Y.; Suzuki, O.; Yoshioka, Y.; Enomoto, T.; Kamiura, S.; Kimura, T. Radical hysterectomy with adjuvant radiotherapy versus definitive radiotherapy alone for FIGO stage IIB cervical cancer. Gynecol. Oncol. 2011, 123, 241–247. [Google Scholar] [CrossRef] [PubMed]
- Landoni, F.; Maneo, A.; Colombo, A.; Placa, F.; Milani, R.; Perego, P.; Favini, G.; Ferri, L.; Mangioni, C. Randomised study of radical surgery versus radiotherapy for stage Ib-IIa cervical cancer. Lancet Lond. Engl. 1997, 350, 535–540. [Google Scholar] [CrossRef]
- Petit, C.; Dumas, I.; Chargari, C.; Martinetti, F.; Maroun, P.; Doyeux, K.; Tailleur, A.; Haie-Meder, C.; Mazeron, R. MRI-guided brachytherapy in locally advanced cervical cancer: Small bowel [Formula: See text] and [Formula: See text] are not predictive of late morbidity. Brachytherapy 2016, 15, 463–470. [Google Scholar] [CrossRef] [PubMed]
- Holloway, C.L.; Racine, M.-L.; Cormack, R.A.; O’Farrell, D.A.; Viswanathan, A.N. Sigmoid dose using 3D imaging in cervical-cancer brachytherapy. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2009, 93, 307–310. [Google Scholar] [CrossRef]
- Georg, P.; Lang, S.; Dimopoulos, J.C.A.; Dörr, W.; Sturdza, A.E.; Berger, D.; Georg, D.; Kirisits, C.; Pötter, R. Dose-volume histogram parameters and late side effects in magnetic resonance image-guided adaptive cervical cancer brachytherapy. Int. J. Radiat. Oncol. Biol. Phys. 2011, 79, 356–362. [Google Scholar] [CrossRef]
- Mazeron, R.; Champoudry, J.; Gilmore, J.; Dumas, I.; Goulart, J.; Oberlander, A.-S.; del Campo, E.R.; Diallo, I.; Lefkopoulos, D.; Haie-Meder, C. Intrafractional organs movement in three-dimensional image-guided adaptive pulsed-dose-rate cervical cancer brachytherapy: Assessment and dosimetric impact. Brachytherapy 2015, 14, 260–266. [Google Scholar] [CrossRef]
- Sturdza, A.E.; Berger, D.; Lang, S.; Dimopoulos, J.; Thomas, G.; Georg, P.; Kirisits, C.; Poetter, R. Uncertainties in assessing sigmoid dose volume parameters in MRI-guided fractionated HDR brachytherapy. Brachytherapy 2008, 7, 109. [Google Scholar] [CrossRef]
- Morgia, M.; Cuartero, J.; Walsh, L.; Jezioranski, J.; Keeler, K.; Xie, J.; Massey, C.; Williamson, D.; Cho, Y.-B.; Oh, S.; et al. Tumor and normal tissue dosimetry changes during MR-guided pulsed-dose-rate (PDR) brachytherapy for cervical cancer. Radiother. Oncol. 2013, 107, 46–51. [Google Scholar] [CrossRef]
- Koom, W.S.; Sohn, D.K.; Kim, J.-Y.; Kim, J.W.; Shin, K.H.; Yoon, S.M.; Kim, D.Y.; Yoon, M.; Shin, D.; Park, S.Y.; et al. Computed tomography-based high-dose-rate intracavitary brachytherapy for uterine cervical cancer: Preliminary demonstration of correlation between dose-volume parameters and rectal mucosal changes observed by flexible sigmoidoscopy. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1446–1454. [Google Scholar] [CrossRef] [PubMed]
- Kavanagh, B.D.; Pan, C.C.; Dawson, L.A.; Das, S.K.; Li, X.A.; Haken, R.K.T.; Miften, M. Radiation Dose–Volume Effects in the Stomach and Small Bowel. Int. J. Radiat. Oncol. Biol. Phys. 2010, 76, S101–S107. [Google Scholar] [CrossRef] [PubMed]
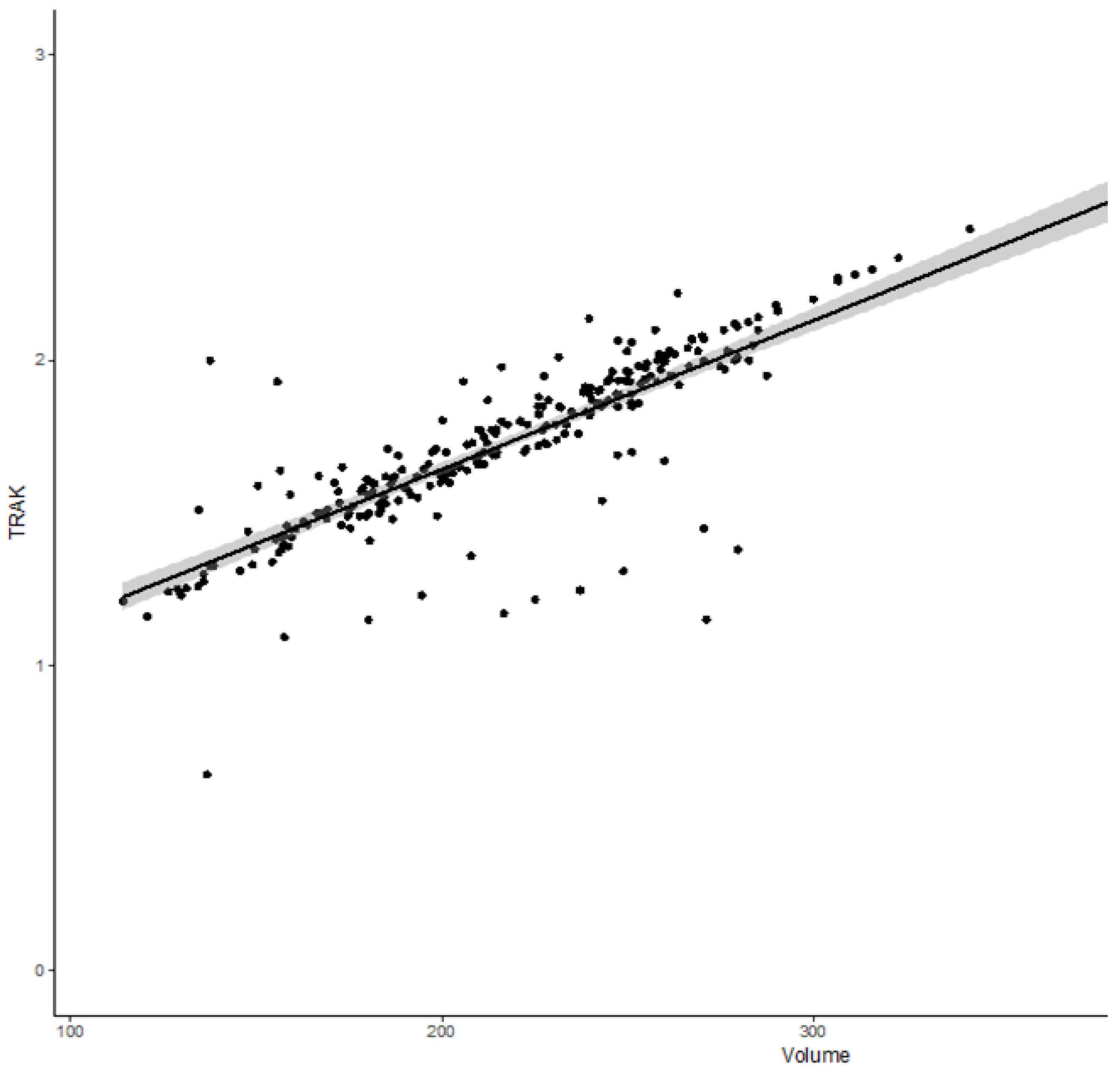
- Nkiwane, K.S.; Andersen, E.; Champoudry, J.; de Leeuw, A.; Swamidas, J.; Lindegaard, J.; Pötter, R.; Kirisits, C.; Tanderup, K. Total reference air kerma can accurately predict isodose surface volumes in cervix cancer brachytherapy. A multicenter study. Brachytherapy 2017, 16, 1184–1191. [Google Scholar] [CrossRef] [PubMed]
- Gouy, S.; Morice, P.; Narducci, F.; Uzan, C.; Gilmore, J.; Kolesnikov-Gauthier, H.; Querleu, D.; Haie-Meder, C.; Leblanc, E. Nodal-staging surgery for locally advanced cervical cancer in the era of PET. Lancet Oncol. 2012, 13, e212–e220. [Google Scholar] [CrossRef]
- Sun, R.; Mazeron, R.; Chargari, C.; Barillot, I. CTV to PTV in cervical cancer: From static margins to adaptive radiotherapy. Cancer Radiother. 2016, 20, 622–628. [Google Scholar] [CrossRef] [PubMed]
- Dimopoulos, J.C.A.; Petrow, P.; Tanderup, K.; Petric, P.; Berger, D.; Kirisits, C.; Pedersen, E.M.; van Limbergen, E.; Haie-Meder, C.; Pötter, R. Recommendations from Gynaecological (GYN) GEC-ESTRO Working Group (IV): Basic principles and parameters for MR imaging within the frame of image based adaptive cervix cancer brachytherapy. Radiother. Oncol. 2012, 103, 113–122. [Google Scholar] [CrossRef] [PubMed]
- Magné, N.; Chargari, C.; SanFilippo, N.; Messai, T.; Gerbaulet, A.; Haie-Meder, C. Technical aspects and perspectives of the vaginal mold applicator for brachytherapy of gynecologic malignancies. Brachytherapy 2010, 9, 274–277. [Google Scholar] [CrossRef] [PubMed]
- Jensen, N.B.K.; Pötter, R.; Kirchheiner, K.; Fokdal, L.; Lindegaard, J.C.; Kirisits, C.; Mazeron, R.; Mahantshetty, U.; Jürgenliemk-Schulz, I.M.; Segedin, B.; et al. Bowel morbidity following radiochemotherapy and image-guided adaptive brachytherapy for cervical cancer: Physician- and patient reported outcome from the EMBRACE study. Radiother. Oncol. J. Eur. Soc. Ther. Radiol. Oncol. 2018, 127, 431–439. [Google Scholar] [CrossRef] [PubMed]
- McGough, C.; Baldwin, C.; Frost, G.; Andreyev, H.J.N. Role of nutritional intervention in patients treated with radiotherapy for pelvic malignancy. Br. J. Cancer. 2004, 90, 2278–2287. [Google Scholar] [CrossRef] [PubMed]
- Abayomi, J.; Kirwan, J.; Hackett, A.; Bagnall, G. A study to investigate women’s experiences of radiation enteritis following radiotherapy for cervical cancer. J. Hum. Nutr. Diet. Off. J. Br. Diet. Assoc. 2005, 18, 353–363. [Google Scholar] [CrossRef]
- De Crevoisier, R.; Sanfilippo, N.; Gerbaulet, A.; Morice, P.; Pomel, C.; Castaigne, D.; Pautier, P.; Lhomme, C.; Duvillard, P.; Haie-meder, C. Exclusive radiotherapy for primary squamous cell carcinoma of the vagina. Radiother. Oncol. 2007, 85, 362–370. [Google Scholar] [CrossRef] [PubMed]
- Small, W.; Winter, K.; Levenback, C.; Iyer, R.; Gaffney, D.; Asbell, S.; Erickson, B.; Jhingran, A.; Greven, K. Extended-field irradiation and intracavitary brachytherapy combined with cisplatin chemotherapy for cervical cancer with positive para-aortic or high common iliac lymph nodes: Results of ARM 1 of RTOG 0116. Int. J. Radiat. Oncol. Biol. Phys. 2007, 68, 1081–1087. [Google Scholar] [CrossRef]
- Gandhi, A.K.; Sharma, D.N.; Rath, G.K.; Julka, P.K.; Subramani, V.; Sharma, S.; Manigandan, D.; Laviraj, M.A.; Kumar, S.; Thulkar, S. Early clinical outcomes and toxicity of intensity modulated versus conventional pelvic radiation therapy for locally advanced cervix carcinoma: A prospective randomized study. Int. J. Radiat. Oncol. Biol. Phys. 2013, 87, 542–548. [Google Scholar] [CrossRef] [PubMed]
- Klopp, A.H.; Yeung, A.R.; Deshmukh, S.; Gil, K.M.; Wenzel, L.; Westin, S.N.; Gifford, K.; Gaffney, D.K.; Small, W.; Thompson, S.; et al. Patient-Reported Toxicity during Pelvic Intensity-Modulated Radiation Therapy: NRG Oncology-RTOG 1203. J. Clin. Oncol. 2018, 36, 2538–2544. [Google Scholar] [CrossRef] [PubMed]
- Eifel, P.J.; Jhingran, A.; Bodurka, D.C.; Levenback, C.; Thames, H. Correlation of Smoking History and Other Patient Characteristics with Major Complications of Pelvic Radiation Therapy for Cervical Cancer. J. Clin. Oncol. 2002, 20, 3651–3657. [Google Scholar] [CrossRef]
- Fokdal, L.; Sturdza, A.; Mazeron, R.; Haie-Meder, C.; Tan, L.T.; Gillham, C.; Šegedin, B.; Jürgenliemk-Schultz, I.; Kirisits, C.; Hoskin, P.; et al. Image guided adaptive brachytherapy with combined intracavitary and interstitial technique improves the therapeutic ratio in locally advanced cervical cancer: Analysis from the retroEMBRACE study. Radiother. Oncol. 2016, 120, 434–440. [Google Scholar] [CrossRef]
- Pötter, R.; Tanderup, K.; Kirisits, C.; de Leeuw, A.; Kirchheiner, K.; Nout, R.; Tan, L.T.; Haie-Meder, C.; Mahantshetty, U.; Segedin, B.; et al. The EMBRACE II study: The outcome and prospect of two decades of evolution within the GEC-ESTRO GYN working group and the EMBRACE studies. Clin. Transl. Radiat. Oncol. 2018, 9, 48–60. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Patients | Performans Status | n (%) or Median (IQ) |
|---|---|---|
| Age (at diagnosis, in years) | 48.0 (41.2–55.3) | |
| Chronic disease * | 45 (17.4%) | |
| Active tobacco use | 82 (31.8%) | |
| Performance Status | 0 (0–1) | |
| 0 | 133 (51.1%) | |
| 1 | 109 (41.9%) | |
| 2 | 18 (7.0%) | |
| Tumors | ||
| FIGO | IB1-IIA | 79 (30.4%) |
| IIB | 112 (43.1%) | |
| IIIA-IVA | 38 (14.6%) | |
| IVB | 31 (11.9%) | |
| Treatments | ||
| Para-aortic lymph node dissection | 156 (60.0%) | |
| Overall treatment time (days) | 48 (44–52) | |
| Extended field radiotherapy | 31 (12%) | |
| Nodal boost delivery | 108 (41.5%) | |
| External beam radiotherapy technique | ||
| IMRT | 37 (14.2%) | |
| 3D conformal radiotherapy | 223 (85.8%) | |
| Chemotherapy | 241 (93.4%) | |
| Number of cycles | 5 (4–5) | |
| <3 | (0.8%) | |
| 3 | 7 (2.7%) | |
| 4 | 57 (22.1%) | |
| 5 | 166 (64.3%) | |
| 6 | 11 (4.3%) | |
| Cisplatin use | 210 (81.4%) | |
| Brachytherapy parameters | ||
| CTVHR volume (cm3) | 22.5 (16.4–32.8) | |
| CTVIR D90 (GyEQD2) | 68.2 (65.2–71.2) | |
| CTVHR D90 (GyEQD2) | 80.9 (73.9–88.4) | |
| 15 Gy isodose volume (cm3) | 216 (182–250) | |
| Sigmoid D0.1 cm3 (GyEQD2) | 63.3 (51.6–72.5) | |
| Sigmoid D2 cm3 (GyEQD2) | 56.0 (48.2–61.4) | |
| Bowel D0.1 cm3 (GyEQD2) | 76.1 (62.7–95.3) | |
| Bowel D2 cm3 (GyEQD2) | 61.4 (54.6–71.1) | |
| TRAK (cGy at 1 meter) | 1.73 (1.54–1.94) | |
| Interstitial brachytherapy use | 20 (7.7%) |
| Toxicity Patterns/Grade | n (%) or Median (IQ) |
|---|---|
| Grade 2+ | 33 (14.5%) |
| Grade 3+ | 3 (1.3%) |
| Diarrhea | 20 (8.8%) |
| Grade 2 | 19 (8.4%) |
| Grade 3 | 1 (0.4%) |
| Flatulence | 20 (8.8%) |
| Grade 2 | 20 (8.8%) |
| Stenosis of sigmoid | 1 (0.4%) |
| Grade 2 | 1 (0.4%) |
| Fistula of sigmoid | 2 (0.8%) |
| Grade 3 | 2 (0.8%) |
| p Value | HR | (95%CI) | ||
|---|---|---|---|---|
| Age > 65 years | 0.99 | 1.0 | (0.3–3.3) | |
| Tobacco use | 0.00 | 2.7 | (1.4–5.3) | |
| Chronic disease * | 0.81 | 1.1 | (0.5–2.8) | |
| Chemotherapy | 0.62 | 1.7 | (0.2–12.1) | |
| CTVHR volume > 25 cm3 | 0.03 | 2.1 | (1.1–4.2) | |
| Nodal boost irradiation | 0.06 | 2.0 | (1.0–3.9) | |
| Para-aortic lymph node dissection | 0.47 | 1.3 | (0.6–2.8) | |
| IMRT use | 0.27 | 0.4 | (0.1–1.9) | |
| Interstitial brachytherapy use | 0.24 | 1.6 | (0.7–3.5) | |
| Sigmoid D0.1 cm3 | ||||
| >70 GyEQD2 | 0.79 | 1.1 | (0.6–2.6) | |
| >65 GyEQD2 | 0.94 | 1.0 | (0.5–2.0) | |
| Sigmoid D2 cm3 | ||||
| >60 GyEQD2 | 0.39 | 1.2 | (0.6–2.6) | |
| >55 GyEQD2 | 0.50 | 0.8 | (0.4–1.5) | |
| Bowel D0.1 cm3 | ||||
| >75 GyEQD2 | 0.96 | 1.0 | (0.5–2.0) | |
| >70 GyEQD2 | 0.45 | 0.8 | (0.4–1.5) | |
| Bowel D2 cm3 | ||||
| >70 GyEQD2 | 0.76 | 0.9 | (0.4–1.9) | |
| >65 GyEQD2 | 0.57 | 0.8 | (0.4–1.7) | |
| TRAK | ≥1.8 | 0.01 | 2.6 | (1.2–5.3) |
| TRAK ≥ 2.0 | 0.01 | 3.4 | (1.6–7.2) |
© 2019 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Bockel, S.; Escande, A.; Dumas, I.; Manea, E.; Morice, P.; Gouy, S.; Deutsch, E.; Haie-Meder, C.; Chargari, C. Total Reference Air Kerma is Associated with Late Bowel Morbidity in Locally Advanced Cervical Cancer Patients Treated with Image-Guided Adaptive Brachytherapy. J. Clin. Med. 2019, 8, 125. https://doi.org/10.3390/jcm8010125
Bockel S, Escande A, Dumas I, Manea E, Morice P, Gouy S, Deutsch E, Haie-Meder C, Chargari C. Total Reference Air Kerma is Associated with Late Bowel Morbidity in Locally Advanced Cervical Cancer Patients Treated with Image-Guided Adaptive Brachytherapy. Journal of Clinical Medicine. 2019; 8(1):125. https://doi.org/10.3390/jcm8010125
Chicago/Turabian StyleBockel, Sophie, Alexandre Escande, Isabelle Dumas, Elena Manea, Philippe Morice, Sebastien Gouy, Eric Deutsch, Christine Haie-Meder, and Cyrus Chargari. 2019. "Total Reference Air Kerma is Associated with Late Bowel Morbidity in Locally Advanced Cervical Cancer Patients Treated with Image-Guided Adaptive Brachytherapy" Journal of Clinical Medicine 8, no. 1: 125. https://doi.org/10.3390/jcm8010125
APA StyleBockel, S., Escande, A., Dumas, I., Manea, E., Morice, P., Gouy, S., Deutsch, E., Haie-Meder, C., & Chargari, C. (2019). Total Reference Air Kerma is Associated with Late Bowel Morbidity in Locally Advanced Cervical Cancer Patients Treated with Image-Guided Adaptive Brachytherapy. Journal of Clinical Medicine, 8(1), 125. https://doi.org/10.3390/jcm8010125