
RETRACTED: An Admission-to-Discharge BNP Increase Is a Predictor of Six-Month All-Cause Death in ADHF Patients: Inferences from Multivariate Analysis Including Admission BNP and Various Clinical Measures of Congestion


Abstract
:1. Introduction
2. Aims
3. Methods
3.1. Statistical Analysis
4. Results
4.1. Patient Characteristics
4.2. Clinical and Objective Markers of Congestion
4.3. Six-Month Mortality
5. Discussion
Study Limitations
6. Conclusions
Author Contributions
Conflicts of Interest
References
- O’Brien, R.J.; Squire, I.B.; Demme, B.; Davies, J.E.; Ng, L.L. Pre-discharge, but not admission, levels of NT-proBNP predict adverse prognosis following acute LVF. Eur. J. Heart Fail. 2003, 5, 499–506. [Google Scholar] [CrossRef]
- Waldo, S.W.; Beede, J.; Isakson, S.; Villard-Saussine, S.; Fareh, J.; Clopton, P.; Fitzgerald, R.L.; Maisel, A.S. Pro-B-type natriuretic peptide levels in acute decompensated heart failure. J. Am. Coll. Cardiol. 2008, 51, 1874–1882. [Google Scholar] [CrossRef] [PubMed]
- Bettencourt, P.; Azevedo, A.; Pimenta, J.; Friões, F.; Ferreira, S.; Ferreira, A. N-terminal-pro-brain natriuretic peptide predicts outcome after hospital discharge in heart failure patients. Circulation 2004, 110, 2168–2174. [Google Scholar] [CrossRef] [PubMed]
- Kociol, R.D.; Horton, J.R.; Fonarow, G.C.; Reyes, E.M.; Shaw, L.K.; O’Connor, C.M.; Felker, G.M.; Hernandez, A.F. Admission, discharge, or change in B-type natriuretic peptide and long-term outcomes: Data from Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF) linked to Medicare claims. Circ. Heart Fail. 2011, 4, 628–636. [Google Scholar] [CrossRef] [PubMed]
- Cowie, M.R.; Jourdain, P.; Maisel, A.; Dahlstrom, U.; Follath, F.; Isnard, R.; Luchner, A.; McDonagh, T.; Mair, J.; Nieminen, M.; et al. Clinical applications of B-type natriuretic peptide (BNP) testing. Eur. Heart J. 2003, 24, 1710–1718. [Google Scholar] [CrossRef]
- Emdin, M.; Clerico, A.; Clemenza, F.; Galvani, M.; Latini, R.; Masson, S.; Mulè, P.; Panteghini, M.; Valle, R.; Zaninotto, M.; et al. Recommendations for the clinical use of cardiac natriuretic peptides. Ital. Heart J. Suppl. 2005, 6, 308–325. (In Italian) [Google Scholar] [PubMed]
- Drazner, M.H.; Hellkamp, A.S.; Leier, C.V.; Shah, M.R.; Miller, L.W.; Russell, S.D.; Young, J.B.; Califf, R.M.; Nohria, A. Value of Clinician Assessment of Hemodynamics in Advanced Heart Failure: the ESCAPE Trial. Circ. Heart Fail. 2008, 1, 170–177. [Google Scholar] [CrossRef] [PubMed]
- Gheorghiade, M.; Follath, F.; Ponikowski, P.; Barsuk, J.H.; Blair, J.E.; Cleland, J.G.; Dickstein, K.; Drazner, M.H.; Fonarow, G.C.; Jaarsma, T.; et al. Assessing and grading congestion in acute heart failure: A scientific statement from the acute heart failure committee of the Heart Failure Association of the European Society of Cardiology and endorsed by the European Society of Intensive Care Medicine. Eur. J. Heart Fail. 2010, 12, 423–433. [Google Scholar] [CrossRef] [PubMed]
- Goonewardena, S.N.; Gemignani, A.; Ronan, A.; Vasaiwala, S.; Blair, J.; Brennan, J.M.; Shah, D.P.; Spencer, K.T. Comparison of hand-carried ultrasound assessment of the inferior vena cava and N-terminal pro-brain natriuretic peptide for predicting readmission after hospitalization for acute decompensated heart failure. JACC Cardiovasc. Imaging 2008, 1, 595–601. [Google Scholar] [CrossRef] [PubMed]
- De Vecchis, R.; Ciccarelli, A.; Ariano, C. Inferior Vena Cava collapsibility and heart failure signs and symptoms: New insights about possible links. Arq. Bras. Cardiol. 2012, 98, 544–552. [Google Scholar] [CrossRef] [PubMed]
- De Vecchis, R.; Baldi, C. Inferior Vena Cava and hemodynamic congestion. Res. Cardiovasc. Med. 2015, 4, e28913. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, C.M.; Abraham, W.T.; Albert, N.M.; Clare, R.; Gattis Stough, W.; Gheorghiade, M.; Greenberg, B.H.; Yancy, C.W.; Young, J.B.; Fonarow, G.C. Predictors of mortality after discharge in patients hospitalized with heart failure: An analysis from the Organized Program to Initiate Lifesaving Treatment in Hospitalized Patients with Heart Failure (OPTIMIZE-HF). Am. Heart J. 2008, 156, 662–673. [Google Scholar] [CrossRef] [PubMed]
- Khazanie, P.; Heizer, G.M.; Hasselblad, V.; Armstrong, P.W.; Califf, R.M.; Ezekowitz, J.; Dickstein, K.; Levy, W.C.; McMurray, J.J.; Metra, M.; et al. Predictors of clinical outcomes in acute decompensated heart failure: Acute Study of Clinical Effectiveness of Nesiritide in Decompensated Heart Failure outcome models. Am. Heart J. 2015, 170, 290–297. [Google Scholar] [CrossRef] [PubMed]
- Fonarow, G.C.; Adams, K.F., Jr.; Abraham, W.T.; Yancy, C.W.; Boscardin, W.J. ADHERE Scientific Advisory Committee, Study Group, and Investigators. Risk stratification for in-hospital mortality in acutely decompensated heart failure: classification and regression tree analysis. JAMA 2005, 293, 572–580. [Google Scholar] [CrossRef] [PubMed]
- McCullough, P.A. Clinical applications of B-type natriuretic peptide levels in the care of cardiovascular patients. Min. Cardioangiol. 2004, 52, 479–489. [Google Scholar]
- Fonarow, G.C.; Peacock, W.F.; Phillips, C.O.; Givertz, M.M.; Lopatin, M. ADHERE Scientific Advisory Committee and Investigators. Admission B-type natriuretic peptide levels and in-hospital mortality in acute decompensated heart failure. J. Am. Coll. Cardiol. 2007, 49, 1943–1950. [Google Scholar] [CrossRef] [PubMed]
- Maisel, A.; Mueller, C.; Adams, K., Jr.; Anker, S.D.; Aspromonte, N.; Cleland, J.G.; Cohen-Solal, A.; Dahlstrom, U.; DeMaria, A.; Di Somma, S.; et al. State of the art: Using natriuretic peptide levels in clinical practice. Eur. J. Heart Fail. 2008, 10, 824–839. [Google Scholar] [CrossRef] [PubMed]
- De Vecchis, R.; Esposito, C.; Cantatrione, S. Natriuretic peptide-guided therapy: Further research required for still-unresolved issues. Herz 2013, 38, 618–628. [Google Scholar] [CrossRef] [PubMed]
- Ponikowski, P.; Voors, A.A.; Anker, S.D.; Bueno, H.; Cleland, J.G.; Coats, A.J.; Falk, V.; González-Juanatey, J.R.; Harjola, V.-P.; Jankowska, E.A.; et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: The Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur. J. Heart Fail. 2016, 18, 891–975. [Google Scholar] [PubMed]

{kind=link}
{kind=link}
| BNP Decrease on Discharge (no. 124 Patients) | BNP Increase on Discharge (no. 53 Patients) | p-Value | |
|---|---|---|---|
| Baseline Demographics | |||
| Age (years, mean ± SD) | 75 ± 13.5 | 76 ± 14.2 | 0.6573 |
| Male sex % (n) | 72.5% (90) | 77.5% (41) | 0.5074 |
| BMI on admission (Kg/m2, mean ± SD) | 29.19 ± 6.87 | 28.68 ± 5.86 | 0.6350 |
| Heart rate on admission (bts/min, mean ± SD) | 99 ± 19 | 103 ± 20 | 0.2084 |
| Heart rate on discharge (bts/min,mean ± SD) | 64± 18 | 70±20 | 0.0511 |
| SBP on admission (mmHg, mean ± SD) | 165 ± 26 | 155 ± 20 | 0.0133 |
| SBP on discharge (mmHg, mean ± SD) | 110 ± 21 | 107 ± 18 | 0.3657 |
| Comorbidities | |||
| Ischemic etiology of HF % (n) | 50.8% (63) | 54.7% (29) | 0.7545 |
| Valvular etiology of HF % (n) | 7.2% (9) | 11.32% (6) | 0.6024 |
| Atrial fibrillation % (n) | 29.83% (37) | 33.96% (18) | 0.7146 |
| CABG % (n) | 25% (31) | 35.84% (19) | 0.1984 |
| History of hypertension % (n) | 69.35% (86) | 71.69% (38) | 0.8645 |
| DM on isulin % (n) | 17.74% (22) | 15.09% (8) | 0.8327 |
| COPD % (n) | 16.12% (20) | 18.86% (10) | 0.8211 |
| ICD % (n) | 13.7% (17) | 16.98% (9) | 0.7404 |
| NYHA class IV at baseline % (n) | 84.67% (105) | 90.56% (48) | 0.4189 |
| Hematochemical Variables | |||
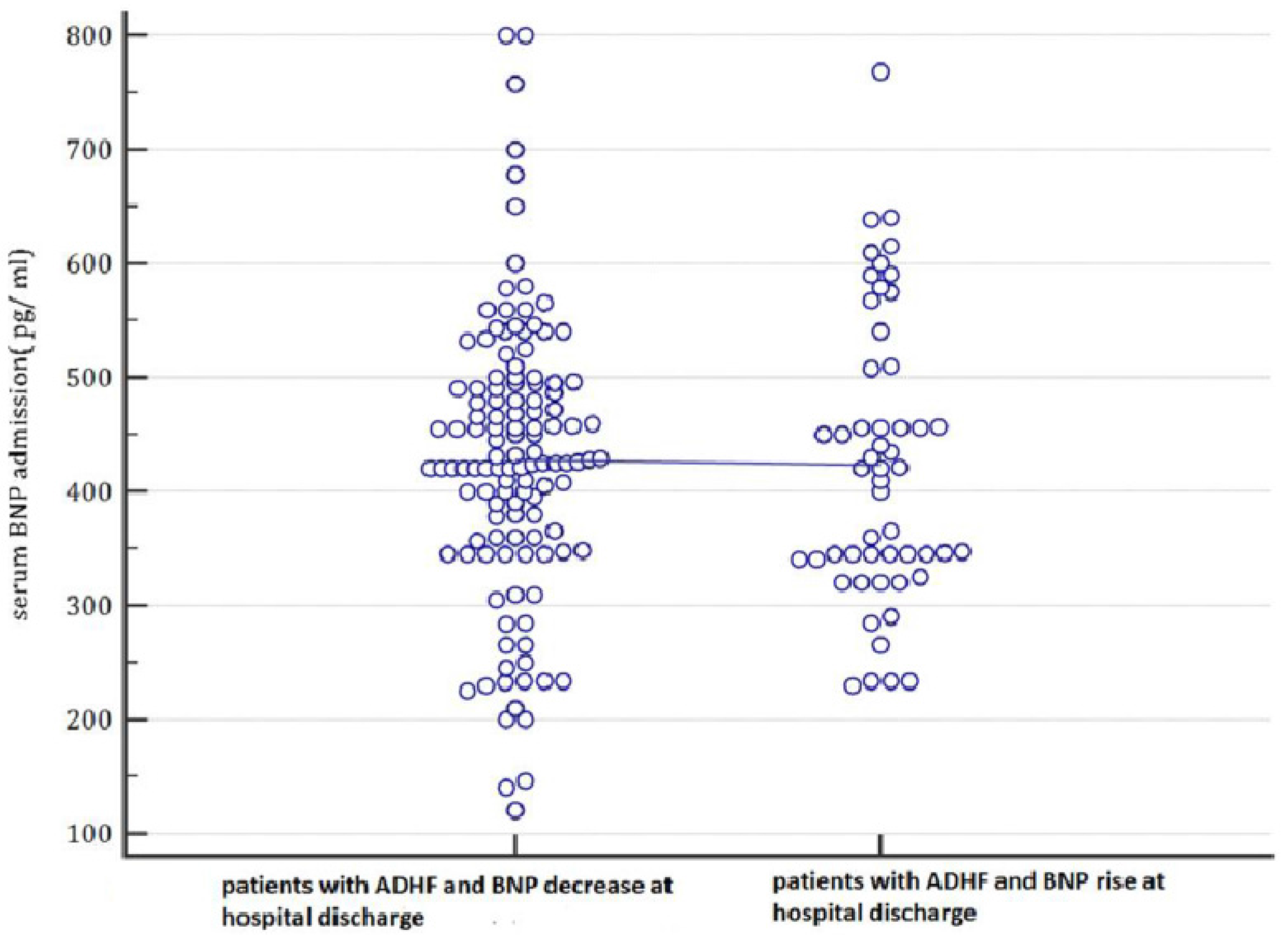
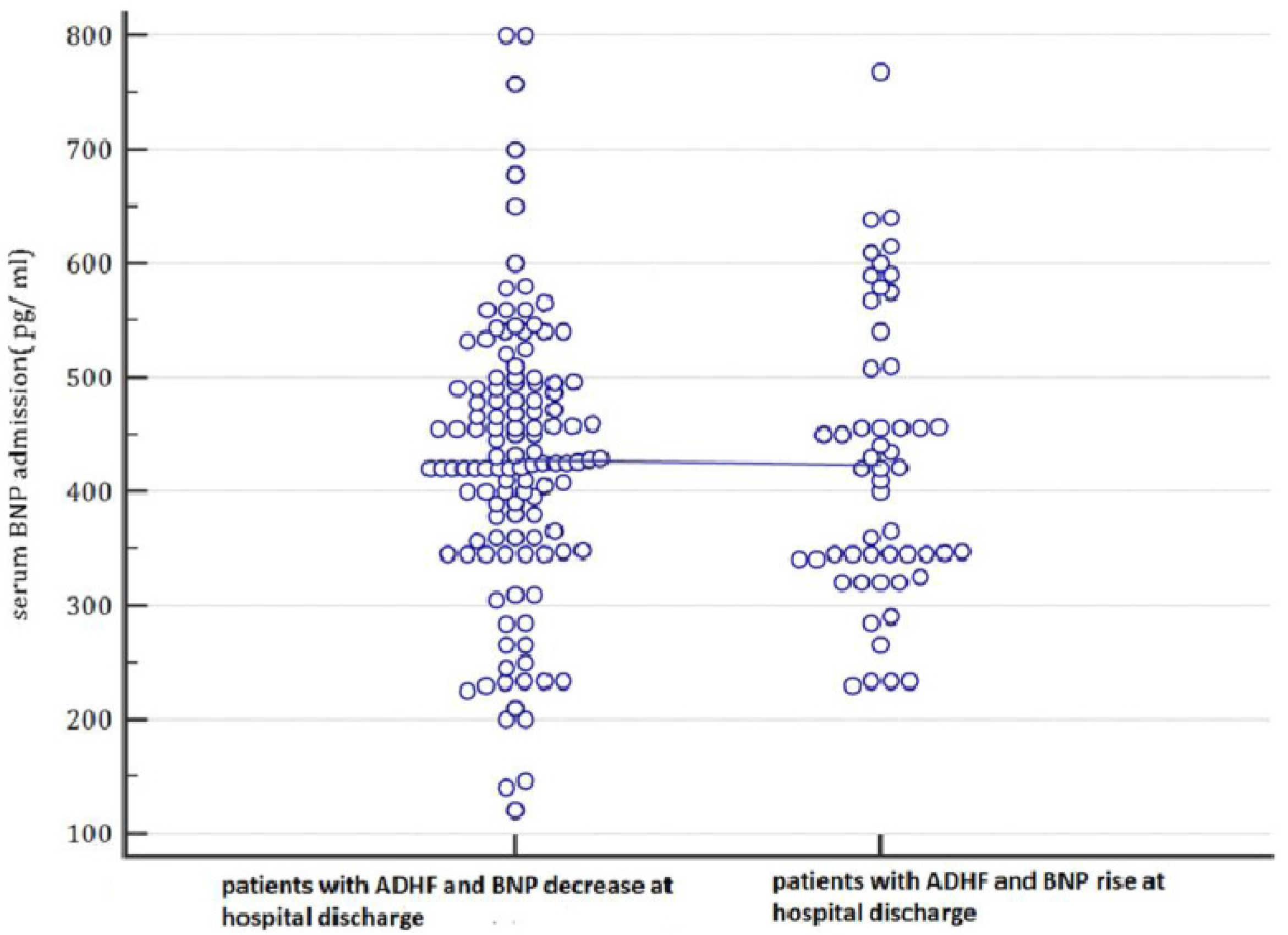
| Admission BNP (pg/mL, mean ± SD) | 427.84 ± 123.22 | 423.22 ± 124.286 | 0.820 |
| Discharge BNP (pg/dL, mean ± SD) * | 170.31 ± 90.10 | 591.47 ± 213.81 | p < 0.001 |
| Serum creatinine (mL/dL, mean ± SD) | 1.46 ± 0.55 | 1.6 ± 0.4 | 0.0962 |
| Albumin (g/dL, mean ± SD) | 3.70 ± 0.58 | 3.65 ± 0.56 | 0.5911 |
| AST (U/L, mean ± SD) | 43 ± 22.64 | 43.80 ± 29.6 | 0.8451 |
| Serum Na+ (meq/L, mean ± SD) | 137.5 ± 10 | 135.4 ± 8.6 | 0.1845 |
| Serum K+ (meq/L, mean ± SD) | 4.2 ± 0.65 | 4 ± 0.85 | 0.0902 |
| WBC/mm3 (mean ± SD) | 7000 ± 2450 | 7900 ± 4010 | 0.0692 |
| Hb (g/dL, mean ± SD) | 12.5 ± 2.1 | 12.1 ± 1.60 | 0.2164 |
| Echocardiographic Data on Admission | |||
| LVEF % (mean ± SD) | 38.45 ± 6 | 37 ± 5.5 | 0.1331 |
| LVESD (mm, mean ± SD) | 59 ± 10 | 58 ± 14 | 0.5916 |
| E/A ratio (mean ± SD) | 2.4 ± 1.25 | 3.2 ± 1.35 | p < 0.001 |
| Deceleration time (ms, mean ± SD) | 142 ± 25 | 138 ± 22 | 0.3142 |
| Jugular Venous Distention (jvd) | |||
|---|---|---|---|
| JVD Persistence | JVD Regression | Total | |
| BNP increase at discharge | |||
| yes | 32 | 21 | 53 |
| no | 36 | 88 | 124 |
| Total | 68 | 109 | 177 |
| Odds ratio | 3.7249 | ||
| 95% CI | 1.8997–7.3034 | ||
| z statistic | 3.828 | ||
| Significance level | p = 0.0001 | ||
| Orthopnea | |||
|---|---|---|---|
| Persistence of Orthopnea | Regression of Orthopnea | Total | |
| BNP increase at discharge | |||
| yes | 34 | 19 | 53 |
| no | 47 | 77 | 124 |
| Total | 81 | 96 | 177 |
| Odds ratio | 2.9317 | ||
| 95% CI | 1.5025–5.7203 | ||
| z statistic | 3.154 | ||
| Significance level | p = 0.0016 | ||
| Covariate | Hazard Ratio | 95% CI | p-Value |
|---|---|---|---|
| Persistent JVD | 1.6666 | 0.5877–4.7265 | 0.3393 |
| Persistent Orthopnea | 1.2329 | 0.4347–3.4964 | 0.6953 |
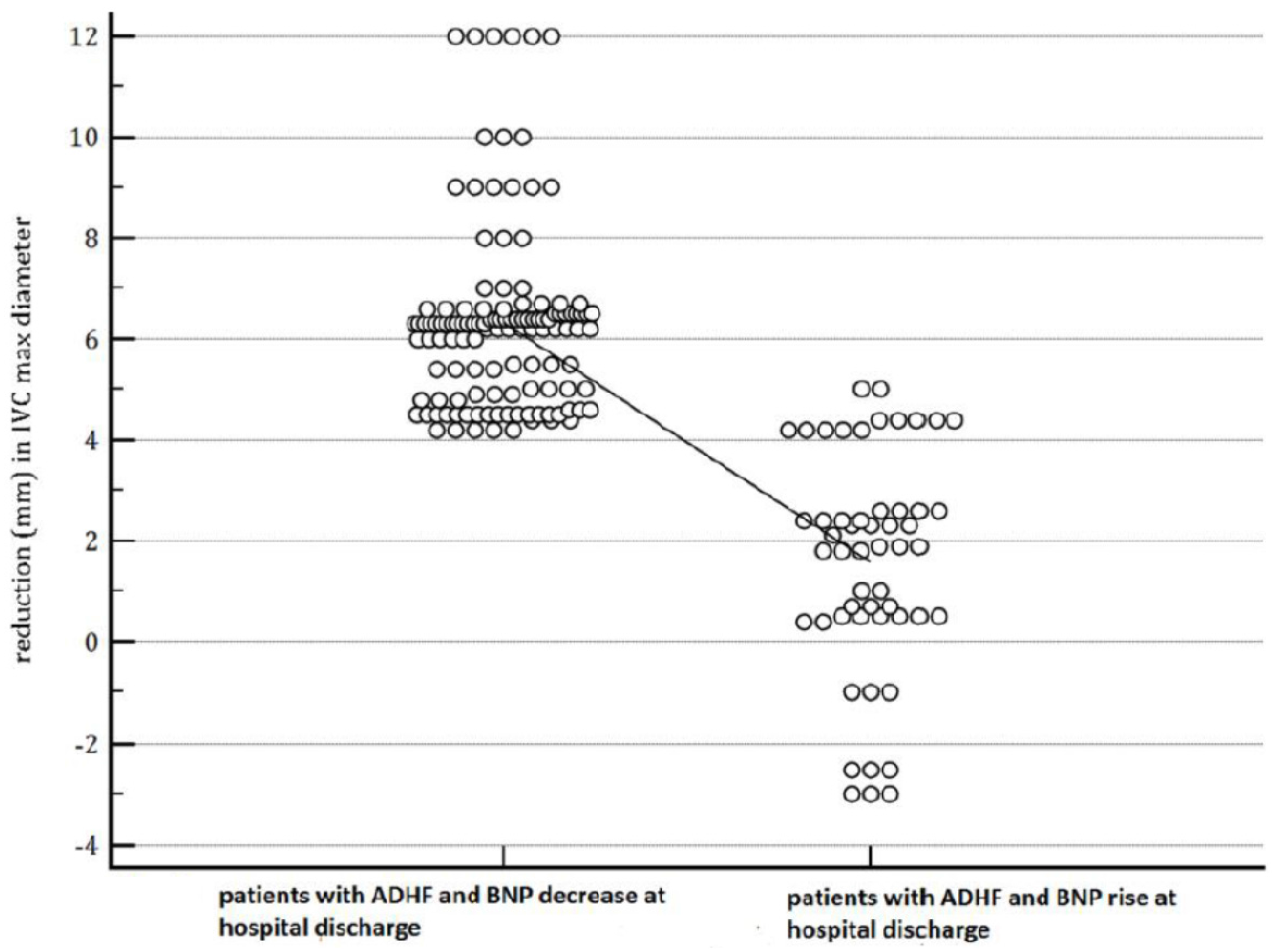
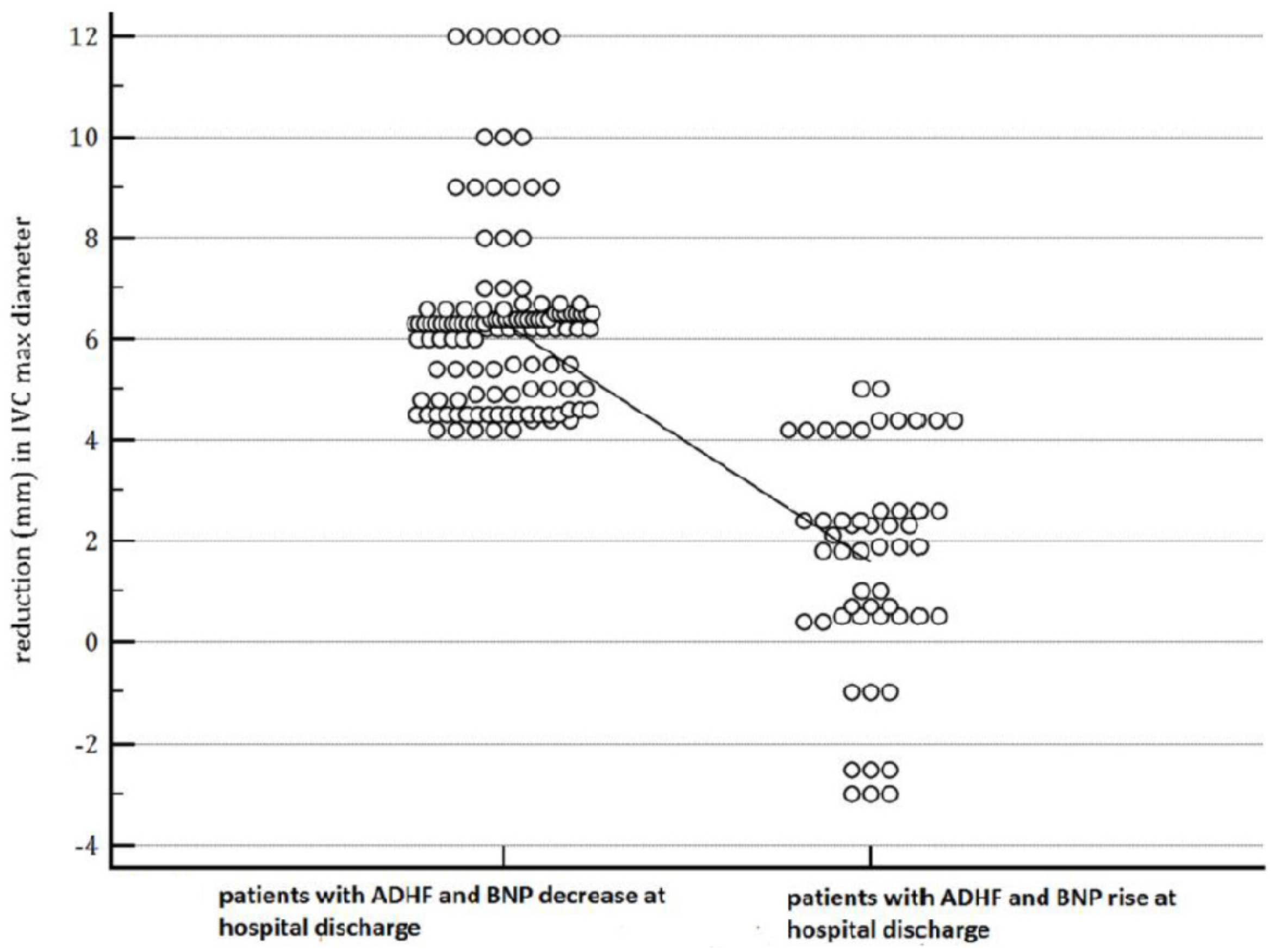
| Reduction (mm) in IVC max diameter at discharge | 0.7791 | 0.6676–0.9092 | 0.0016 * |
| Weight loss at discharge | 1.0412 | 0.8034–1.3495 | 0.7612 |
| SBP at admission | 0.9315 | 0.9002–0.9638 | <0.0001 * |
| Urea at discharge | 1.0526 | 1.0231–1.0829 | 0.0004 * |
| BNP at admission | 1.0026 | 0.9985–1.0067 | 0.2162 |
| BNP increase at discharge relative to admission | 37.7761 | 4.9906–285.9448 | 0.0005 * |
| BNP at discharge | 1.0064 | 1.0046–1.0082 | <0.0001 * |
| Model 1 (Seven Covariates) | |||
| Overall Model Fit: Chi-Squared = 49.206; d.f. = 7; Significance Level: p < 0.0001 | |||
| Covariate | Hazard Ratio | 95% CI | p-Value |
| Persistent JVD | 0.5503 | 0.1567–1.9329 | 0.3539 |
| Persistent Orthopnea | 2.5678 | 0.6537–10.0868 | 0.1789 |
| Reduction (mm) in IVC max diameter at discharge | 0.7641 | 0.5904–0.9890 | 0.0420 * |
| Weight loss at discharge | 1.1080 | 0.8345–1.4709 | 0.4806 |
| SBP at admission | 0.9374 | 0.8999–0.9765 | 0.0020 * |
| Urea at discharge | 1.0629 | 1.0264–1.1007 | 0.0007 * |
| BNPs at admission | 1.0011 | 0.9961–1.0061 | 0.6710 |
| Model 2 (Eight Covariates) | |||
| Overall Model Fit: Chi-Squared = 56.673; d.f. = 8; Significance Level: p < 0.0001 | |||
| Covariate | Hazard Ratio | 95% CI | p-Value |
| Persistent JVD | 0.4075 | 0.1150–1.4437 | 0.1664 |
| Persistent Orthopnea | 3.1278 | 0.6885–14.2091 | 0.1418 |
| Reduction (mm) in IVC max diameter at discharge | 0.9752 | 0.7117–1.3363 | 0.8767 |
| Weight loss at discharge | 1.1446 | 0.8548–1.5326 | 0.3671 |
| SBP at admission | 0.9682 | 0.9278–1.0104 | 0.1396 |
| Urea at discharge | 1.0736 | 1.0345–1.1142 | 0.0002 * |
| BNP at admission | 0.9996 | 0.9947–1.0045 | 0.8785 |
| BNP increase at discharge relative to admission | 30.5424 | 1.7409–535.8294 | 0.0199 * |
| Model 3 (Nine Covariates) | |||
| Overall Model Fit: Chi-squared = 69.840; d.f. = 9; significance level: p < 0.0001 | |||
| Covariate | Hazard Ratio | 95% CI | p-Value |
| Persistent JVD | 0.1686 | 0.0381–0.7469 | 0.0197 * |
| Persistent Orthopnea | 6.1573 | 0.9606–39.466 | 0.0564 |
| Reduction (mm) in IVC max diameter at discharge | 0.8871 | 0.6198–1.2717 | 0.5167 |
| Weight loss at discharge | 0.9178 | 0.6421–1.3118 | 0.6395 |
| SBP at admission | 0.9570 | 0.9150–1.0009 | 0.0560 |
| Urea at discharge | 1.0509 | 1.0078–1.0959 | 1.0209 * |
| BNP at admission | 1.0004 | 0.9940–1.0069 | 0.8976 |
| BNP increase at discharge relative to admission | 1.4121 | 0.0502–39.722 | 0.8402 |
| BNP at discharge | 1.0056 | 1.0022–1.0090 | 0.0012 * |
© 2016 by the authors; licensee MDPI, Basel, Switzerland. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license ( http://creativecommons.org/licenses/by/4.0/).
Share and Cite
De Vecchis, R.; Ariano, C.; Baldi, C. RETRACTED: An Admission-to-Discharge BNP Increase Is a Predictor of Six-Month All-Cause Death in ADHF Patients: Inferences from Multivariate Analysis Including Admission BNP and Various Clinical Measures of Congestion. J. Clin. Med. 2016, 5, 99. https://doi.org/10.3390/jcm5110099
De Vecchis R, Ariano C, Baldi C. RETRACTED: An Admission-to-Discharge BNP Increase Is a Predictor of Six-Month All-Cause Death in ADHF Patients: Inferences from Multivariate Analysis Including Admission BNP and Various Clinical Measures of Congestion. Journal of Clinical Medicine. 2016; 5(11):99. https://doi.org/10.3390/jcm5110099
Chicago/Turabian StyleDe Vecchis, Renato, Carmelina Ariano, and Cesare Baldi. 2016. "RETRACTED: An Admission-to-Discharge BNP Increase Is a Predictor of Six-Month All-Cause Death in ADHF Patients: Inferences from Multivariate Analysis Including Admission BNP and Various Clinical Measures of Congestion" Journal of Clinical Medicine 5, no. 11: 99. https://doi.org/10.3390/jcm5110099
APA StyleDe Vecchis, R., Ariano, C., & Baldi, C. (2016). RETRACTED: An Admission-to-Discharge BNP Increase Is a Predictor of Six-Month All-Cause Death in ADHF Patients: Inferences from Multivariate Analysis Including Admission BNP and Various Clinical Measures of Congestion. Journal of Clinical Medicine, 5(11), 99. https://doi.org/10.3390/jcm5110099