

Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients
 , , , , , , ,
, , , , , , ,
Abstract
1. Introduction
2. Methods
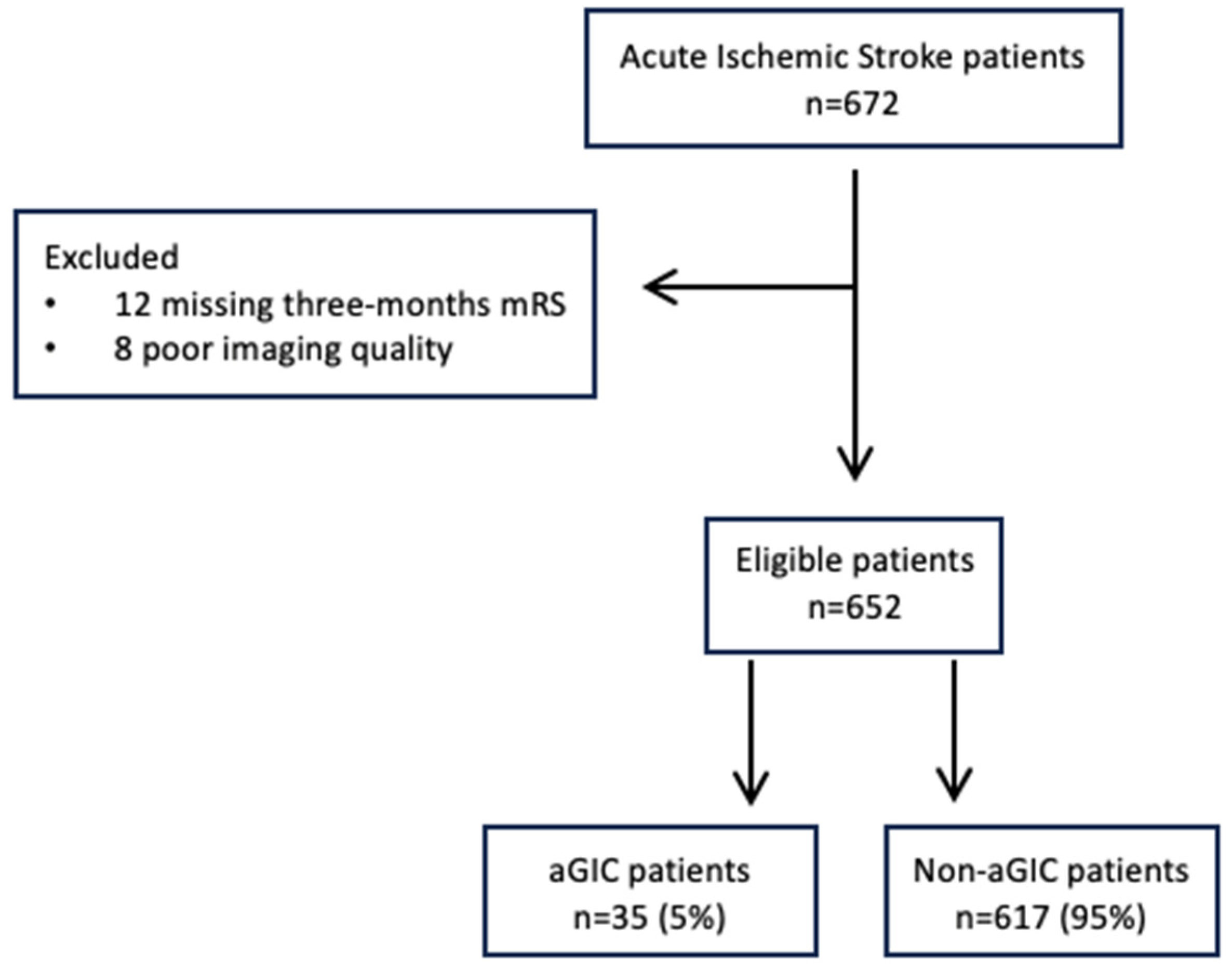
2.1. Patient Selection
2.2. Clinical Assessment
2.3. Imaging Acquisition
2.4. Imaging Processing and Analysis
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Baron, J.C. The core/penumbra model: Implications for acute stroke treatment and patient selection in 2021. Eur. J. Neurol. 2021, 28, 2794–2803. [Google Scholar] [CrossRef] [PubMed]
- Albers, G.W.; Marks, M.P.; Kemp, S.; Christensen, S.; Tsai, J.P.; Ortega-Gutierrez, S.; McTaggart, R.A.; Torbey, M.T.; Kim-Tenser, M.; Leslie-Mazwi, T.; et al. DEFUSE 3 Investigators. Thrombectomy for stroke at 6 to 16 hours with selection by perfusion imaging. N. Engl. J. Med. 2018, 378, 708–718. [Google Scholar] [CrossRef] [PubMed]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Damaerschalk, B.M.; Hoh, B.; et al. Guidelines for the early management of patients with acute ischemic stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A guideline for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [PubMed]
- Nogueira, R.G.; Jadhav, A.P.; Haussen, D.C.; Bonafe, A.; Budzik, R.F.; Bhuva, P.; Yavagal, D.R.; Ribo, M.; Cognard, C.; Hanel, R.A.; et al. DAWN Trial Investigators. Thrombectomy 6 to 24 hours after stroke with a mismatch between deficit and infarct. N. Engl. J. Med. 2018, 378, 11–21. [Google Scholar] [CrossRef] [PubMed]
- Mendelson, S.J.; Prabhakaran, S. Diagnosis and management of transient ischemic attack and acute ischemic stroke. JAMA 2021, 11, 1088–1098. [Google Scholar] [CrossRef]
- Albers, G.W. Late window paradox. Stroke 2018, 49, 768–771. [Google Scholar] [CrossRef]
- Olivot, J.M.; Albucher, J.F.; Guenego, A.; Thalamas, C.; Mlynash, M.; Rousseasu, V.; Drif, A.; Christensen, S.; Sommet, A.; Viguier, A.; et al. Mismatch profile influences outcome after mechanical thrombectomy. Stroke 2021, 52, 232–240. [Google Scholar] [CrossRef]
- Ballout, A.A.; Oh, S.Y.; Huang, B.; Patsalides, A.; Libman, R.B. Ghost infarct core: A systematic review of the frequency, magnitude, and variables of CT perfusion overestimation. J. Neuroimaging 2023, 33, 716–724. [Google Scholar] [CrossRef]
- Boned, S.; Padroni, M.; Rubiera, M.; Tomasello, A.; Coscojuela, P.; Tomero, N.; Muchada, M.; Rodriguez-Luna, D.; Flores, A.; Rodriguez, N.; et al. Admission CT perfusion may overestimate initial infarct core: The ghost infarct core concept. J. Neurointerv. Surg. 2017, 9, 66–69. [Google Scholar] [CrossRef]
- Martins, N.; Aires, A.; Mendez, B.; Boned, S.; Rubiera, M.; Tomasello, A.; Coscojuela, P.; Hernandez, D.; Muchada, M.; Rodriguez-Luna, D.; et al. Ghost infarct core and admission computed tomography perfusion: Redefining the role of neuroimaging in acute ischemic stroke. Interv. Neurol. 2018, 7, 513–521. [Google Scholar] [CrossRef]
- Rotem, S.H.; Saban, M.; Buxbaum, C.; Firas, S.; Elliot, S.; Ayelet, E.; Eitan, A.; Gregory, T. Infarct core reliability by CT perfusion is a time-dependent phenomenon. J. Neuroimaging 2020, 30, 240–245. [Google Scholar] [PubMed]
- Garcia-Tornel, A.; Campos, D.; Rubiera, M.; Boned, S.; Olivè-Gadea, M.; Requenza, M.; Ciolli, L.; Muchada, M.; Pagola, J.; Rodriguez-Luna, D.; et al. Ischemic core overestimation on computed tomography perfusion. Stroke 2021, 52, 1751–1760. [Google Scholar] [CrossRef] [PubMed]
- Ospel, J.M.; Rex, N.; Rinkel, L.; Kashani, N.; Buck, B.; Rempel, J.; Sahlas, D.; Kelly, M.E.; Budzik, R.; Tymianski, M.; et al. Prevalence of “ghost infarct core” after endovascular thrombectomy. AJNR Am. J. Neuroradiol. 2024, 45, 291–295. [Google Scholar] [CrossRef] [PubMed]
- Broocks, G.; Meyer, L.; Winkelmeier, L.; Kniep, H.; Heitkamp, C.; Christensen, S.; Lansberg, M.G.; Thaler, C.; Kemmling, A.; Schon, G.; et al. Overestimation of the ischemic core is associated with higher core lesion volume and degree of reperfusion after thrombectomy. Radiology 2024, 312, e231750. [Google Scholar] [CrossRef]
- Hoving, J.W.; Marquering, H.A.; Majoie, C.B.L.M.; Yassi, N.; Sharma, G.; Liebeskind, D.S.; van der Lugt, A.; Roos, Y.B.; van Zwam, W.; van Oostenbrugge, R.J.; et al. Volumetric and spatial accuracy of computed tomography perfusion estimated ischemic core volume in patients with Acute ischemic stroke. Stroke 2018, 49, 2368–2375. [Google Scholar] [CrossRef]
- Rodrigues, G.M.; Mohammaden, M.H.; Haussen, D.C.; Bouslama, M.; Ravindran, K.; Pisani, L.; Prater, A.; Frenkel, M.R.; Nogueira, R.G. Ghost infarct core following endovascular reperfusion: A risk for computed tomography perfusion misguided selection in stroke. Int. J. Stroke 2022, 17, 897–905. [Google Scholar] [CrossRef]
- Sarraj, A.; Campbell, B.C.V.; Christensen, S.; Sitton, C.W.; Khanpara, S.; Riascos, R.F.; Pujara, D.; Shaker, F.; Sharma, G.; Lansberg, M.G.; et al. Accuracy of CT perfusion-based core estimation of follow-up infarction: Effects of time since last known well. Neurology 2022, 982, 2084–2096. [Google Scholar] [CrossRef]
- Xu, X.Q.; Ma, G.; Lu, S.S.; Shen, G.C.; Cao, Y.Z.; Liu, S.; Shi, H.B.; Wu, F.Y. Predictors of ghost infarct core on baseline computed tomography perfusion in stroke patients with successful recanalization after mechanical thrombectomy. Eur. Radiol. 2023, 33, 1792–1800. [Google Scholar] [CrossRef]
- Ospel, J.M.; Menon, B.K.; Qiu, W.; Kashani, N.; Mayank, A.; Singh, N.; Cimflova, P.; Marko, M.; Nogueira, R.G.; McTaggart, R.A. A detailed analysis of infarct patterns and volumes at 24-hour non-contrast CT and diffusion-weighted MRI in acute ischemic stroke due to large vessel occlusion: Results from the ESCAPE-NA1 trial. Radiology 2021, 300, 152–159. [Google Scholar] [CrossRef]
- Broocks, G.; Hanning, U.; Faizy, T.D.; Scheibel, A.; Nawabi, J.; Schon, G.; Forkert, N.D.; Langner, S.; Fiehler, J.; Gelliben, S. Ischemic lesion growth in acute stroke: Water uptake quantification distinguishes between edema and tissue infarct. J. Cereb. Blood Flow Metab. 2020, 40, 823–832. [Google Scholar] [CrossRef]
- Tipirneni-Sajja, A.; Christensen, S.; Straka, M.; Inoue, M.; Lansberg, M.G.; Mlynash, M.; Bammer, R.; Parsons, M.W.; Donnan, G.Y.; Davis, S.M.; et al. Prediction of final infarct volume on subacute MRI by quantifying cerebral edema in ischemic stroke. J. Cereb. Blood Flow Metab. 2017, 37, 3077–3084. [Google Scholar] [CrossRef] [PubMed]
- Federau, C.; Mlynash, M.; Christensen, S.; Zaharchuk, G.; Cha, B.; Lansberg, M.G.; Wintermark, M.; Albers, G.W. Evolution of volume and signal intensity on Fluid-Attenuated Inversion Recovery MR images after endovascular treatment stroke therapy. Radiology 2016, 280, 184–192. [Google Scholar] [CrossRef] [PubMed]
- Hernandez-Perez, M.; Werner, M.; Remollo, S.; Martin, C.; Cortes, J.; Valls, A.; Ramos, A.; Dorado, L.; Serena, J.; Munuera, J. Early and delayed infarct growth in patients undergoing mechanical thrombectomy: A prospective, serial MRI Study. Stroke 2023, 54, 217–225. [Google Scholar] [CrossRef] [PubMed]
- Luby, M.; Hsia, A.W.; Lomahan, C.A.; Uche, V.; Davis, R.; Kim, Y.; Somani, S.; Burton, S.; Cabatbat, R.; Craft, V.; et al. Late lesion growth following endovascular therapy: Is 24 h too early to assess acute infarct size including the effects of secondary injury? Cerebrovasc. Dis. 2025, 54, 129–137. [Google Scholar]
- Rinkel, L.A.; Ospel, J.M.; Brown, S.B.; Campbell, B.C.V.; Dippel, D.W.J.; Demchuk, A.M.; Majoie, C.B.L.M.; Mitchell, O.J.; Bracard, S.; Guillemin, F.; et al. What is a meaningful difference when using infarct volume as the primary outcome? Results from the HERMES database. Stroke 2024, 55, 866–873. [Google Scholar] [CrossRef]
- Puetz, V.; Dzialowski, I.; Hill, M.D.; Demchuk, A.M. The Alberta stroke program early CT score in clinical practice: What have we learned? Int. J. Stroke 2009, 4, 354–364. [Google Scholar] [CrossRef]
- Busto, G.; Casetta, I.; Morotti, A.; Barra, A.; Maccaglia, M.G.; Bianchi, A.; Moretti, M.; Capasso, F.; Toffali, M.; Arba, F.; et al. Multi-phase CT-Angiography outperforms angiographic careggi collateral score and predicts functional outcome in acute ischemic stroke. Neurol Sci 2025, 46, 249–256. [Google Scholar] [CrossRef]
- Zaidat, O.O.; Yoo, A.J.; Khatri, P.; Tomsick, T.A.; von Kummer, R.; Saver, J.L.; Marks, M.P.; Prabhakaran, S.; Kallmes, D.F.; Fitzsimmons, B.F.M.; et al. Cerebral angiographic revascularization grading (CARG) collaborators; STIR revascularization working group; STIR thrombolysis in cerebral infarction (TICI) task force. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: A consensus statement. Stroke 2013, 44, 2650–2663. [Google Scholar]
- Busto, G.; Morotti, A.; Casetta, I.; Barra, A.; Fiorenza, A.; Di Pasquale, F.; Maccaglia, M.; Toffali, M.; Mancini, S.; Carlesi, E.; et al. Hypoperfusion intensity ratio correlates with collaterals and predicts outcome and infarct volume in acute ischemic stroke patients. Eur. J. Clin. Investig. 2024, 10, e14264. [Google Scholar] [CrossRef]
- Campbell, B.C.V.; Christensen, S.; Levi, C.R.; Desmond, P.M.; Donnan, G.A.; Davis, S.M.; Parsons, M. Cerebral blood flow is the optimal CT perfusion parameter for assessing infarct core. Stroke 2011, 42, 3435–3440. [Google Scholar] [CrossRef]
- Bivard, A.; Kleinig, T.; Miteff, F.; Butcher, K.; Lin, L.; Levi, C.; Parsons, M. Ischemic core thresholds change with time to reperfusion: A case control study. Ann. Neurol. 2017, 82, 995–1003. [Google Scholar] [CrossRef] [PubMed]
- Busto, G.; Morotti, A.; Carlesi, E.; Fiorenza, A.; Di Pasquale, F.; Mancini, S.; Lombardo, I.; Scola, E.; Gadda, D.; Moretti, M.; et al. Pivotal role of multiphase computed tomography angiography for collateral assessment in patients with acute ischemic stroke. Radiol. Med. 2023, 128, 944–959. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Ospel, J.M.; Menon, B.J.; Almekhlafi, M.; Jayaraman, M.; Fiehler, J.; Psychogios, M.; Chapot, R.; van der Lugt, A.; Liu, J.; et al. Challenging the ischemic core concept in acute ischemic stroke imaging. Stroke 2020, 51, 3147–3155. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Variable | Patients With Absolute Ghost Core | Patients Without Absolute Ghost Core |
|---|---|---|
| n = 35 | n = 617 | |
| Age, mean (±SD), years | 76.0 (12.3) | 74.5 (12.9) |
| Sex, woman, n (%) | 18 (51.4) | 330 (53.4) |
| Admission NIHSS, median (IQR) | 16 (9–21) | 18 (12–22) |
| ASPECTS, median (IQR) | 10 (9–10) | 8 (7–9) |
| tPA before EVT, n (%) | 16 (45.7) | 248 (40.1) |
| Time from onset to NCCT, minutes, median (IQR) | 160 (90–250) | 290 (192–555) |
| Time from onset to NCCT <6 h, n (%) | 32 (91.4) | 362 (58.6) |
| Time from onset to NCCT >6 h, n (%) | 3 (8.6) | 255 (41.4) |
| Occlusion site, left n (%) | 23 (65.7) | 333 (53.9) |
| M1 segment, n (%) | 19 (54.3) | 364 (58.9) |
| M2 segment, n (%) | 9 (25.7) | 113 (18.4) |
| ICA segment, n (%) | 7 (20.0) | 140 (22.7) |
| Collateral score, median (IQR) | 3 (3–4) | 4 (3–4) |
| Poor, n (%) | 23 (71.4) | 227 (36.7) |
| Good, n (%) | 12 (28.6) | 390 (63.3) |
| Hypoperfusion intensity ratio, median (IQR) | 0.50 (0.30–0.60) | 0.34 (0.20–0.50) |
| Infarct core (rCBF<40%) at baseline in mL, median (IQR) | 26.2 (19.9–32.2) | 23.7 (9.9–44.3) |
| Ischemic penumbra volume, median (IQR), mL | 65.0 (39.0–109.3) | 56.4 (28.5–93.1) |
| mTICI score 2b–3, n (%) | 35 (100.0) | 500 (81.0) |
| Onset to reperfusion time, minutes, median (IQR) | 330 (265–385) | 425 (310–715) |
| Infarct volume at 24 h in mL, median (IQR) | 0 (0–0) | 29.5 (15.3–69.6) |
| NIHSS at 24 h, median (IQR) | 4 (2-8) | 13 (5-20) |
| mRS at three-months 0-2, n (%) | 23 (65.7) | 270 (43.7) |
| Univariable | Multivariable | |||
|---|---|---|---|---|
| OR (95% CI) | p | OR (95% CI) | p | |
| Age, years | 1.02 (0.98–1.07) | 0.222 | ||
| Sex, woman | 0.82 (0.29–2.33) | 0.714 | ||
| Admission NIHSS | 1.05 (0.97–1.14) | 0.192 | ||
| ASPECTS | 2.36 (1.52–3.67)) | <0.001 | 2.37 (1.61–3.48) | <0.001 |
| tPA before EVT | 0.67 (0.25–1.77) | 0.426 | ||
| Onset-to-CT time | 0.99 (0.98–0.99) | 0.016 | 0.99 (0.99–1.01) | .034 |
| Onset-to-reperfusion time | 1.00 (0.99–1.01) | 0.116 | ||
| mTICI score 2b-3 | 0.86 (0.31–2.56) | 0.996 | ||
| Collateral score | 0.21 (0.10–0.42) | <0.001 | 0.24 (0.12–0.45) | <0.001 |
| Hypoperfusion intensity ratio | 8.88 (2.9–27.0) | <0.001 | 23.2 (1.54–48.9) | <0.001 |
| Infarct core (rCBF <40%) | 0.97 (0.95–1.00) | 0.100 | ||
| Ischemic penumbra volume | 0.99 (098–1.01) | 0.365 | ||
| NIHSS at 24 h | 0.80 (0.72–0.89) | <0.001 | ||
| mRS at three months 0–2 | 1.11 (0.38–3.25) | 0.023 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Busto, G.; Morotti, A.; Casetta, I.; Poggesi, A.; Gadda, D.; Ginestroni, A.; Arcara, G.; Rustici, A.; Zini, A.; Padovani, A.; et al. Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients. J. Clin. Med. 2025, 14, 2991. https://doi.org/10.3390/jcm14092991
Busto G, Morotti A, Casetta I, Poggesi A, Gadda D, Ginestroni A, Arcara G, Rustici A, Zini A, Padovani A, et al. Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients. Journal of Clinical Medicine. 2025; 14(9):2991. https://doi.org/10.3390/jcm14092991
Chicago/Turabian StyleBusto, Giorgio, Andrea Morotti, Ilaria Casetta, Anna Poggesi, Davide Gadda, Andrea Ginestroni, Giorgio Arcara, Arianna Rustici, Andrea Zini, Alessandro Padovani, and et al. 2025. "Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients" Journal of Clinical Medicine 14, no. 9: 2991. https://doi.org/10.3390/jcm14092991
APA StyleBusto, G., Morotti, A., Casetta, I., Poggesi, A., Gadda, D., Ginestroni, A., Arcara, G., Rustici, A., Zini, A., Padovani, A., & Fainardi, E. (2025). Ct-Perfusion Absolute Ghost Infarct Core Is a Rare Phenomenon Associated with Poor Collateral Status in Acute Ischemic Stroke Patients. Journal of Clinical Medicine, 14(9), 2991. https://doi.org/10.3390/jcm14092991