

Smoking Status in Pregnancy: A Retrospective Analysis in Northern Greece


 , , , , and
, , , , and 
Abstract
1. Introduction
2. Material and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Vardavas, C.I.; Patelarou, E.; Chatzi, L.; Roumeliotaki, T.; Sarri, K.; Murphy, S.; Koutis, A.; Kafatos, A.G.; Kogevinas, M. Factors associated with active smoking, quitting, and secondhand smoke exposure among pregnant women in Greece. J. Epidemiol. 2010, 20, 355–362. [Google Scholar] [CrossRef] [PubMed]
- Vardavas, C.I.; Chatzi, L.; Patelarou, E.; Plana, E.; Sarri, K.; Kafatos, A.; Koutis, A.D.; Kogevinas, M. Smoking and smoking cessation during early pregnancy and its effect on adverse pregnancy outcomes and fetal growth. Eur. J. Pediatr. 2010, 169, 741–748. [Google Scholar] [CrossRef] [PubMed]
- Miyake, Y.; Tanaka, K.; Arakawa, M. Active and passive maternal smoking during pregnancy and birth outcomes: The Kyushu Okinawa maternal and child health study. BMC Pregnancy Childbirth 2013, 13, 157. [Google Scholar] [CrossRef]
- Kristjansson, A.L.; Thorisdottir, I.E.; Steingrimsdottir, T.; Allegrante, J.P.; Lilly, C.L.; Sigfusdottir, I.D. Maternal smoking during pregnancy and scholastic achievement in childhood: Evidence from the LIFECOURSE cohort study. Eur. J. Public Health 2017, 27, 850–855. [Google Scholar] [CrossRef] [PubMed]
- Kapaya, H.; Broughton-Pipkin, F.; Hayes-Gill, B.; Loughna, P.V. Smoking in pregnancy affects the fetal heart: Possible links to future cardiovascular disease. J. Matern. Fetal Neonatal Med. 2015, 28, 1664–1668. [Google Scholar] [CrossRef]
- World Health Organization. WHO Report on the Global Tobacco Epidemic, 2009: Implementing Smoke-Free Environments; World Health Organization: Geneva, Switzerland, 2009. [Google Scholar]
- Bonello, K.; Figoni, H.; Blanchard, E.; Vignier, N.; Avenin, G.; Melchior, M.; Cadwallader, J.S.; Chastang, J.; Ibanez, G. Prevalence of smoking during pregnancy and associated social inequalities in developed countries over the 1995–2020 period: A systematic review. Paediatr. Perinat. Epidemiol. 2023, 37, 555–565. [Google Scholar] [CrossRef] [PubMed]
- Lange, S.; Probst, C.; Rehm, J.; Popova, S. National, regional, and global prevalence of smoking during pregnancy in the general population: A systematic review and meta-analysis. Lancet Glob. Health 2018, 6, e769–e776. [Google Scholar] [CrossRef] [PubMed]
- Tsakiridis, I.; Mamopoulos, A.; Papazisis, G.; Petousis, S.; Liozidou, A.; Athanasiadis, A.; Dagklis, T. Prevalence of smoking during pregnancy and associated risk factors: A cross-sectional study in Northern Greece. Eur. J. Public Health 2018, 28, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Wade, D.T. Ethics, audit, and research: All shades of grey. BMJ 2005, 330, 468–471. [Google Scholar] [CrossRef] [PubMed]
- Tsakiridis, I.; Oikonomidou, A.C.; Bakaloudi, D.R.; Dagklis, T.; Papazisis, G.; Chourdakis, M. Substance Use During Pregnancy: A Comparative Review of Major Guidelines. Obstet. Gynecol. Surv. 2021, 76, 634–643. [Google Scholar] [CrossRef] [PubMed]
- Abraham, M.; Alramadhan, S.; Iniguez, C.; Duijts, L.; Jaddoe, V.W.; Den Dekker, H.T.; Crozier, S.; Godfrey, K.M.; Hindmarsh, P.; Vik, T.; et al. A systematic review of maternal smoking during pregnancy and fetal measurements with meta-analysis. PLoS ONE 2017, 12, e0170946. [Google Scholar] [CrossRef]
- Marufu, T.C.; Ahankari, A.; Coleman, T.; Lewis, S. Maternal smoking and the risk of still birth: Systematic review and meta-analysis. BMC Public Health 2015, 15, 239. [Google Scholar] [CrossRef] [PubMed]
- McEvoy, C.T.; Spindel, E.R. Pulmonary Effects of Maternal Smoking on the Fetus and Child: Effects on Lung Development, Respiratory Morbidities, and Life Long Lung Health. Paediatr. Respir. Rev. 2017, 21, 27–33. [Google Scholar] [CrossRef]
- Smedberg, J.; Lupattelli, A.; Mardby, A.C.; Nordeng, H. Characteristics of women who continue smoking during pregnancy: A cross-sectional study of pregnant women and new mothers in 15 European countries. BMC Pregnancy Childbirth 2014, 14, 213. [Google Scholar] [CrossRef] [PubMed]
- Ruta, F.; Avram, C.; Voidazan, S.; Marginean, C.; Bacarea, V.; Abram, Z.; Foley, K.; Fogarasi-Grenczer, A.; Penzes, M.; Tarcea, M. Active Smoking and Associated Behavioural Risk Factors before and during Pregnancy—Prevalence and Attitudes among Newborns’ Mothers in Mures County, Romania. Central Eur. J. Public Health 2016, 24, 276–280. [Google Scholar] [CrossRef]
- Penn, G.; Owen, L. Factors associated with continued smoking during pregnancy: Analysis of socio-demographic, pregnancy and smoking-related factors. Drug Alcohol Rev. 2002, 21, 17–25. [Google Scholar] [CrossRef]
- Al-Sahab, B.; Saqib, M.; Hauser, G.; Tamim, H. Prevalence of smoking during pregnancy and associated risk factors among Canadian women: A national survey. BMC Pregnancy Childbirth 2010, 10, 24. [Google Scholar] [CrossRef] [PubMed]
- Houston-Ludlam, A.N.; Bucholz, K.K.; Grant, J.D.; Waldron, M.; Madden, P.A.F.; Heath, A.C. The interaction of sociodemographic risk factors and measures of nicotine dependence in predicting maternal smoking during pregnancy. Drug Alcohol. Depend. 2019, 198, 168–175. [Google Scholar] [CrossRef] [PubMed]
- Gikas, A.; Merkouris, P.; Skliros, E.; Sotiropoulos, A. Urban-rural differences in smoking prevalence in Greece. Eur. J. Public Health 2007, 17, 402. [Google Scholar] [CrossRef]
- Skalis, G.; Archontakis, S.; Thomopoulos, C.; Andrianopoulou, I.; Papazachou, O.; Vamvakou, G.; Aznaouridis, K.; Katsi, V.; Makris, T. A single-center, prospective, observational study on maternal smoking during pregnancy in Greece: The HELENA study. Tob. Prev. Cessat. 2021, 7, 16. [Google Scholar] [CrossRef] [PubMed]
- Trust, N. Smoking in Pregnancy. Available online: https://www.nuffieldtrust.org.uk/resource/smoking-in-pregnancy (accessed on 9 January 2024).
- Gollenberg, A.; Pekow, P.; Markenson, G.; Tucker, K.L.; Chasan-Taber, L. Dietary behaviors, physical activity, and cigarette smoking among pregnant Puerto Rican women. Am. J. Clin. Nutr. 2008, 87, 1844–1851. [Google Scholar] [CrossRef] [PubMed]
- Albanes, D.; Jones, D.Y.; Micozzi, M.S.; Mattson, M.E. Associations between smoking and body weight in the US population: Analysis of NHANES II. Am. J. Public Health 1987, 77, 439–444. [Google Scholar] [CrossRef] [PubMed]
- Filozof, C.; Fernandez Pinilla, M.C.; Fernandez-Cruz, A. Smoking cessation and weight gain. Obes. Rev. 2004, 5, 95–103. [Google Scholar] [CrossRef]
- Klesges, R.C.; Meyers, A.W.; Klesges, L.M.; La Vasque, M.E. Smoking, body weight, and their effects on smoking behavior: A comprehensive review of the literature. Psychol. Bull. 1989, 106, 204–230. [Google Scholar] [CrossRef] [PubMed]
- Watanabe, T.; Tsujino, I.; Konno, S.; Ito, Y.M.; Takashina, C.; Sato, T.; Isada, A.; Ohira, H.; Ohtsuka, Y.; Fukutomi, Y.; et al. Association between Smoking Status and Obesity in a Nationwide Survey of Japanese Adults. PLoS ONE 2016, 11, e0148926. [Google Scholar] [CrossRef] [PubMed]
- Kaneita, Y.; Tomofumi, S.; Takemura, S.; Suzuki, K.; Yokoyama, E.; Miyake, T.; Harano, S.; Ibuka, E.; Kaneko, A.; Tsutsui, T.; et al. Prevalence of smoking and associated factors among pregnant women in Japan. Prev. Med. 2007, 45, 15–20. [Google Scholar] [CrossRef] [PubMed]
- Kahn, R.S.; Certain, L.; Whitaker, R.C. A reexamination of smoking before, during, and after pregnancy. Am. J. Public Health 2002, 92, 1801–1808. [Google Scholar] [CrossRef]
- Colman, G.J.; Joyce, T. Trends in smoking before, during, and after pregnancy in ten states. Am. J. Prev. Med. 2003, 24, 29–35. [Google Scholar] [CrossRef] [PubMed]
- The Practice Committee of American Society for Reproductive Medicine. Smoking and infertility. Fertil. Steril. 2008, 90, S254–S259. [Google Scholar] [CrossRef]
- Chatkin, R.; Mottin, C.C.; Chatkin, J.M. Smoking among morbidly obese patients. BMC Pulm. Med. 2010, 10, 61. [Google Scholar] [CrossRef]
- Fahey, M.C.; Dahne, J.; Wahlquist, A.E.; Carpenter, M.J. The Impact of Older Age on Smoking Cessation Outcomes After Standard Advice to Quit. J. Appl. Gerontol. 2023, 42, 1477–1485. [Google Scholar] [CrossRef] [PubMed]
- Almeda, N.; Gomez-Gomez, I. The Impact of the COVID-19 Pandemic on Smoking Consumption: A Systematic Review of Longitudinal Studies. Front. Psychiatry 2022, 13, 941575. [Google Scholar] [CrossRef] [PubMed]
- Sarich, P.; Cabasag, C.J.; Liebermann, E.; Vaneckova, P.; Carle, C.; Hughes, S.; Egger, S.; O’Connell, D.L.; Weber, M.F.; da Costa, A.M.; et al. Tobacco smoking changes during the first pre-vaccination phases of the COVID-19 pandemic: A systematic review and meta-analysis. EClinicalMedicine 2022, 47, 101375. [Google Scholar] [CrossRef] [PubMed]
- Wiley, R.C.; Oliver, A.C.; Snow, M.B.; Bunn, J.Y.; Barrows, A.J.; Tidey, J.W.; Lee, D.C.; Sigmon, S.C.; Gaalema, D.E.; Heil, S.H.; et al. The Impact of the Covid-19 Pandemic on Smoking Among Vulnerable Populations. Nicotine Tob. Res. 2023, 25, 282–290. [Google Scholar] [CrossRef]
- Hong, S.; Woo, S.; Kim, S.; Park, J.; Lee, M.; Kim, S.; Koyanagi, A.; Smith, L.; Kim, M.S.; Lopez Sanchez, G.F.; et al. National prevalence of smoking among adolescents at tobacco tax increase and COVID-19 pandemic in South Korea, 2005–2022. Sci. Rep. 2024, 14, 7823. [Google Scholar] [CrossRef]
- Bednarczuk, N.; Williams, E.E.; Absalom, G.; Olaitan-Salami, J.; Greenough, A. The impact of COVID-19 on smoking cessation in pregnancy. J. Perinat. Med. 2022, 50, 1001–1004. [Google Scholar] [CrossRef] [PubMed]
- Tigka, M.; Metallinou, D.; Tzeli, M.; Lykeridou, K. Maternal tobacco, alcohol and caffeine consumption during the perinatal period: A prospective cohort study in Greece during the COVID-19 pandemic. Tob. Induc. Dis. 2023, 21, 80. [Google Scholar] [CrossRef] [PubMed]
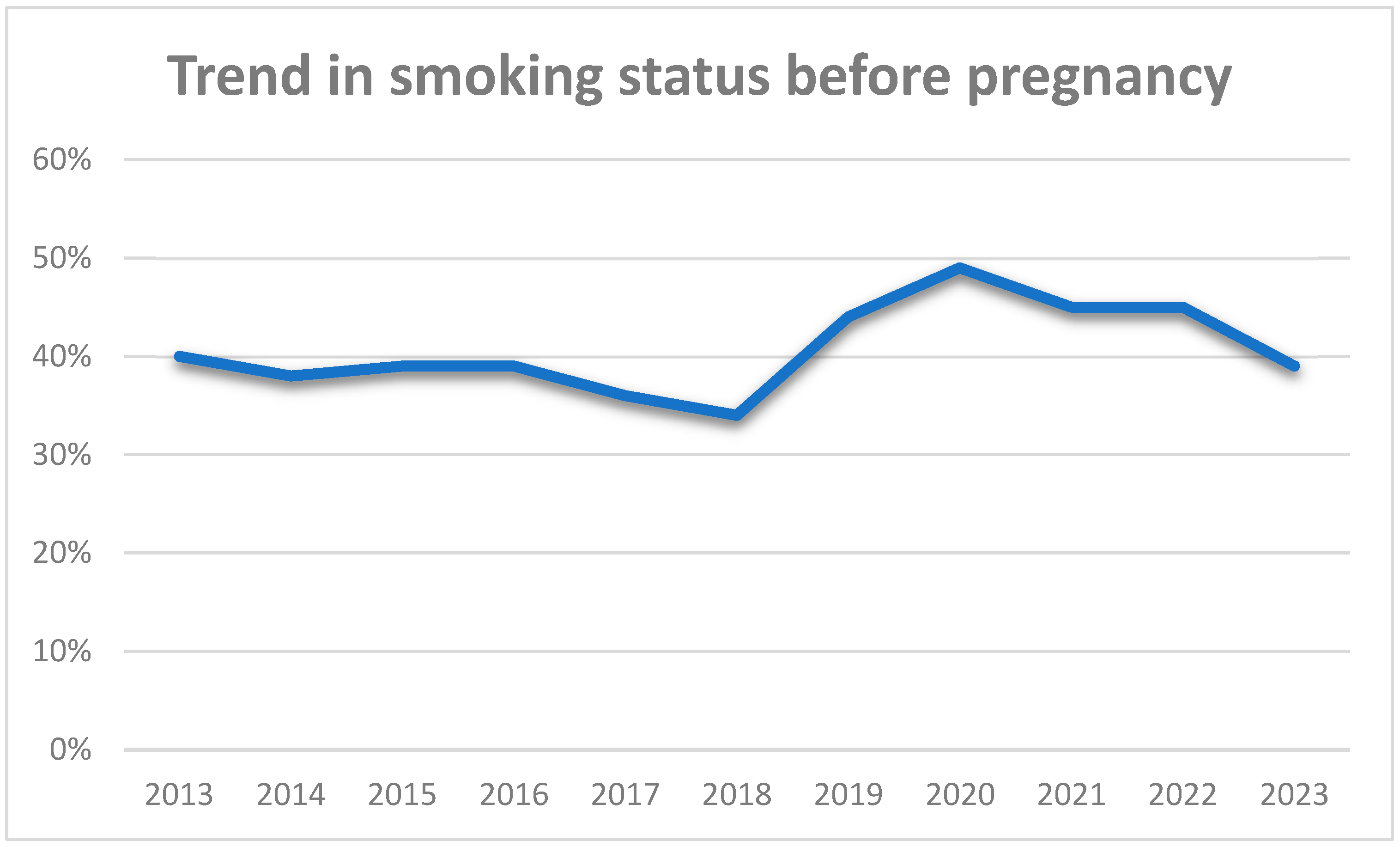

{kind=link}
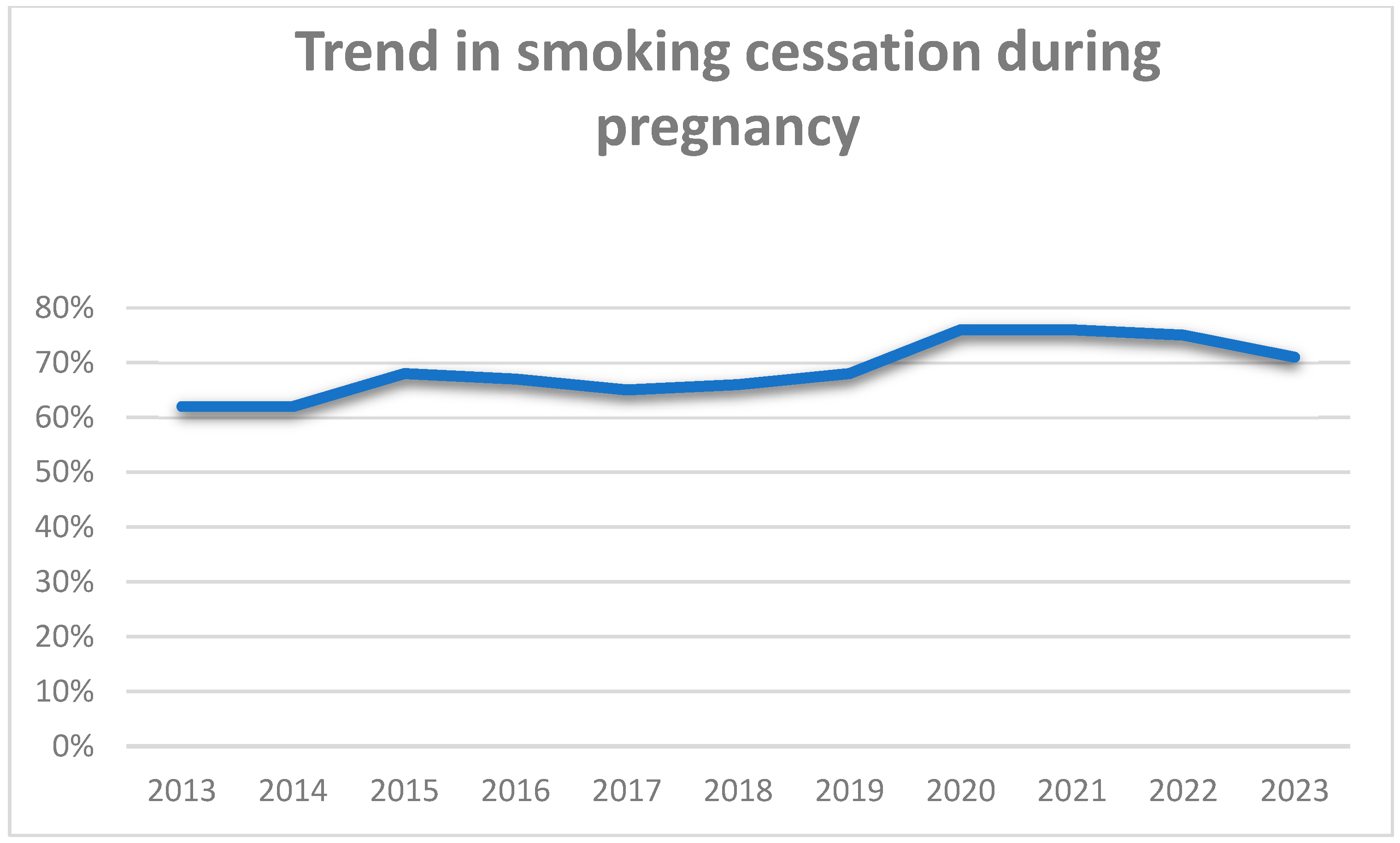
{kind=link}
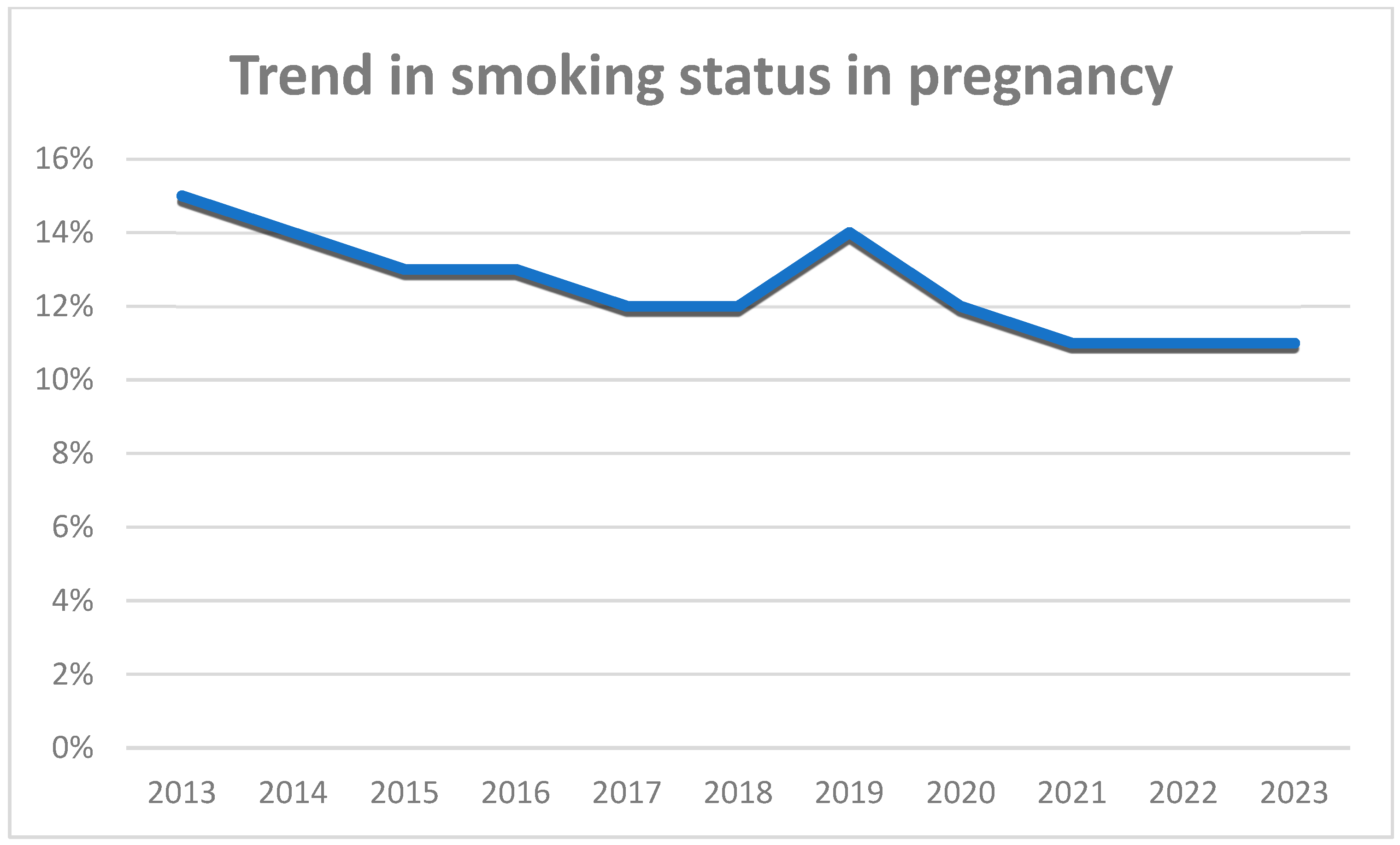
{kind=link}
| Characteristics | Frequency | Percentage (%) |
|---|---|---|
| Maternal Age (Years) | ||
| <35 | 8667 | 71.8% |
| ≥35 | 3407 | 28.2% |
| Parity | ||
| Nulliparous | 6442 | 53.4% |
| Multiparous | 5632 | 46.6% |
| Method of conception | ||
| Spontaneous | 11,373 | 94.2% |
| ARTs | 701 | 5.8% |
| BMI (kg/m2) | ||
| <30 | 10,502 | 87% |
| ≥30 | 1572 | 13% |
| Smoking before pregnancy | ||
| No | 7069 | 58.5% |
| Yes | 5005 | 41.5% |
| Current smoker | ||
| No | 10,585 | 87.7% |
| Yes | 1489 | 12.3% |
| Smoking cessation due to pregnancy | ||
| No | 8558 | 70.8% |
| Yes | 3516 | 29.1% |
| Type of gestation | ||
| Singleton | 11,725 | 97.1% |
| Twins | 349 | 2.9% |
| Explanatory Variables | Current Smoking | Smoking Before Pregnancy | Smoking Cessation |
|---|---|---|---|
| Univariate Analysis | |||
| OR (95% CI) | |||
| Mode of conception (ARTs vs. spontaneous conception) | 0.54 (0.4–0.72) *** | 1.01 (0.87–1.18) | 2.08 (1.53–2.83) *** |
| Twins (singleton vs. multiple gestation) | 0.83 (0.59–1.18) | 1.1 (0.91–1.4) | 0.73 (0.5–1.06) |
| Parity | 1.2 (1.09–1.35) *** | 0.8 (0.77–0.89) *** | 0.66 (0.59–0.75) *** |
| Maternal age | 1.1 (0.97–1.24) | 1.1 (1.03–1.21) * | 1.02 (0.9–1.17) |
| BMI | 1.66 (1.44–1.92) *** | 1.4 (1.2–1.5) *** | 0.69 (0.59–0.81) *** |
| Explanatory Variables | Current Smoking | Smoking Before Pregnancy | Smoking Cessation |
|---|---|---|---|
| Multivariate Analysis | |||
| OR (95% CI) | |||
| Mode of conception (ARTs vs. spontaneous conception) | 0.52 (0.38–0.70) *** | 0.861 (0.72–1.02) | 1.9 (1.38–2.69) *** |
| Twins (singleton vs. multiple gestation) | 1.06 (0.73–1.53) | 1.12 (0.89–1.4) | 0.99 (0.66–1.48) |
| Parity | 1.12 (1.008–1.26) * | 0.79 (0.73–0.85) *** | 0.7 (0.62–0.8) *** |
| Maternal age | 1.1 (0.98–1.26) | 1.17 (1.07–1.27) *** | 1.02 (0.89–1.17) |
| BMI | 1.65 (1.43–1.9) *** | 1.44 (1.29–1.6) *** | 0.72 (0.61–0.85) *** |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mitta, K.; Tsakiridis, I.; Drizou, S.; Michos, G.; Kalogiannidis, I.; Mamopoulos, A.; Christodoulaki, C.; Panagopoulos, P.; Dagklis, T. Smoking Status in Pregnancy: A Retrospective Analysis in Northern Greece. J. Clin. Med. 2025, 14, 431. https://doi.org/10.3390/jcm14020431
Mitta K, Tsakiridis I, Drizou S, Michos G, Kalogiannidis I, Mamopoulos A, Christodoulaki C, Panagopoulos P, Dagklis T. Smoking Status in Pregnancy: A Retrospective Analysis in Northern Greece. Journal of Clinical Medicine. 2025; 14(2):431. https://doi.org/10.3390/jcm14020431
Chicago/Turabian StyleMitta, Kyriaki, Ioannis Tsakiridis, Smaragda Drizou, Georgios Michos, Ioannis Kalogiannidis, Apostolos Mamopoulos, Chryssi Christodoulaki, Periklis Panagopoulos, and Themistoklis Dagklis. 2025. "Smoking Status in Pregnancy: A Retrospective Analysis in Northern Greece" Journal of Clinical Medicine 14, no. 2: 431. https://doi.org/10.3390/jcm14020431
APA StyleMitta, K., Tsakiridis, I., Drizou, S., Michos, G., Kalogiannidis, I., Mamopoulos, A., Christodoulaki, C., Panagopoulos, P., & Dagklis, T. (2025). Smoking Status in Pregnancy: A Retrospective Analysis in Northern Greece. Journal of Clinical Medicine, 14(2), 431. https://doi.org/10.3390/jcm14020431