
Predictors for Improvement of Global Functioning in Patients with Axial Spondyloarthritis


Abstract
1. Introduction
2. Materials and Methods
2.1. Study Patients
2.2. Clinical Variables
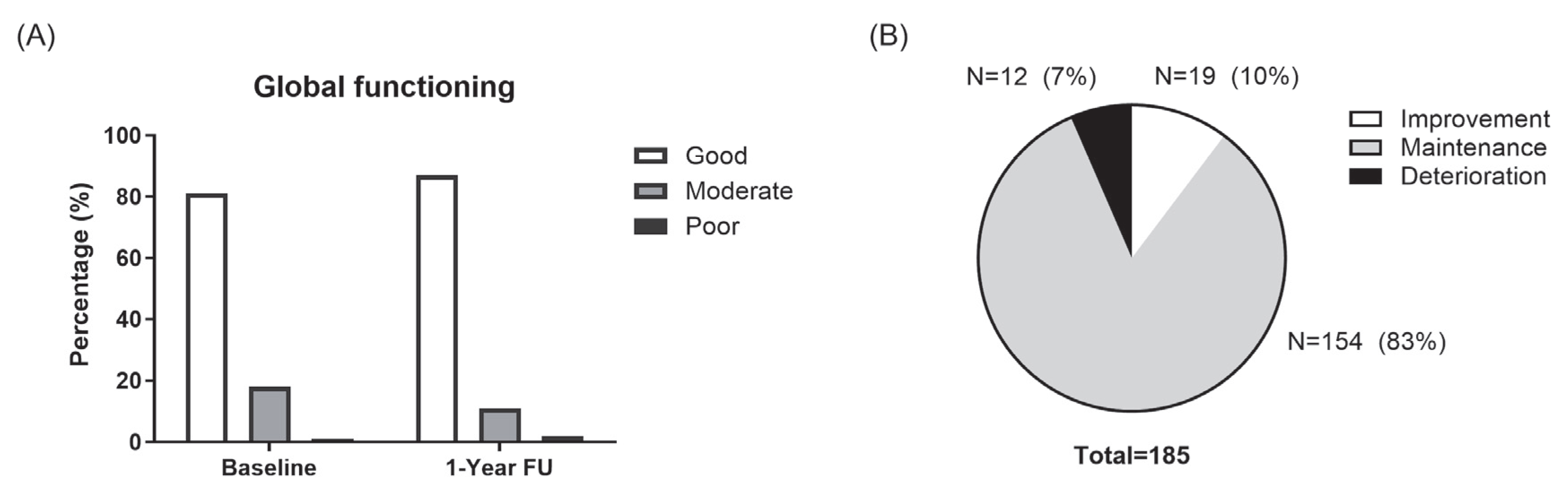
2.3. Assessment of Global Functioning
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Sieper, J.; Poddubnyy, D. Axial spondyloarthritis. Lancet 2017, 390, 73–84. [Google Scholar] [CrossRef]
- Dagfinrud, H.; Kjeken, I.; Mowinckel, P.; Hagen, K.B.; Kvien, T.K. Impact of functional impairment in ankylosing spondylitis: Impairment, activity limitation, and participation restrictions. J. Rheumatol. 2005, 32, 516–523. [Google Scholar] [PubMed]
- Ramiro, S.; Nikiphorou, E.; Sepriano, A.; Ortolan, A.; Webers, C.; Baraliakos, X.; Landewé, R.B.M.; Van den Bosch, F.E.; Boteva, B.; Bremander, A.; et al. ASAS-EULAR recommendations for the management of axial spondyloarthritis: 2022 update. Ann. Rheum. Dis. 2023, 82, 19–34. [Google Scholar] [CrossRef] [PubMed]
- Alonso, S.; Morante, I.; Alperi, M.; Queiro, R. The ASAS Health Index: A New Era for Health Impact Assessment in Spondyloarthritis. J. Rheumatol. 2022, 49, 8–15. [Google Scholar] [CrossRef] [PubMed]
- Kiltz, U.; van der Heijde, D.; Boonen, A.; Akkoc, N.; Bautista-Molano, W.; Burgos-Vargas, R.; Wei, J.C.; Chiowchanwisawakit, P.; Dougados, M.; Duruoz, M.T.; et al. Measurement properties of the ASAS Health Index: Results of a global study in patients with axial and peripheral spondyloarthritis. Ann. Rheum. Dis. 2018, 77, 1311–1317. [Google Scholar] [CrossRef] [PubMed]
- Kiltz, U.; van der Heijde, D.; Boonen, A.; Cieza, A.; Stucki, G.; Khan, M.A.; Maksymowych, W.P.; Marzo-Ortega, H.; Reveille, J.; Stebbings, S.; et al. Development of a health index in patients with ankylosing spondylitis (ASAS HI): Final result of a global initiative based on the ICF guided by ASAS. Ann. Rheum. Dis. 2015, 74, 830–835. [Google Scholar] [CrossRef]
- Navarro-Compán, V.; Boel, A.; Boonen, A.; Mease, P.J.; Dougados, M.; Kiltz, U.; Landewé, R.B.M.; Baraliakos, X.; Bautista-Molano, W.; Chiowchanwisawakit, P.; et al. Instrument selection for the ASAS core outcome set for axial spondyloarthritis. Ann. Rheum. Dis. 2022, 82, 763–772. [Google Scholar] [CrossRef]
- Molto, A.; López-Medina, C.; Van den Bosch, F.E.; Boonen, A.; Webers, C.; Dernis, E.; van Gaalen, F.A.; Soubrier, M.; Claudepierre, P.; Baillet, A.; et al. Efficacy of a tight-control and treat-to-target strategy in axial spondyloarthritis: Results of the open-label, pragmatic, cluster-randomised TICOSPA trial. Ann. Rheum. Dis. 2021, 80, 1436–1444. [Google Scholar] [CrossRef]
- Regierer, A.C.; Weiß, A.; Kiltz, U.; Sieper, J.; Schwarze, I.; Bohl-Bühler, M.; Kellner, H.; Poddubnyy, D.; Zink, A.; Braun, J.; et al. The Sensitivity to Change of the ASAS Health Index in an Observational Real-Life Cohort Study. J. Rheumatol. 2023, 50, 185–191. [Google Scholar] [CrossRef]
- Queiro, R.; Alonso-Castro, S.; Alperi, M. ASAS Health Index as an Addition to Routine Clinical Practice. J. Rheumatol. 2021, 48, 787. [Google Scholar] [CrossRef]
- Rodrigues-Manica, S.; Cruz, E.; Ramiro, S.; Sousa, S.; Aguiar, R.; Sepriano, A.; Machado, P.; Branco, J.; Kiltz, U.; Pimentel-Santos, F. The European Portuguese version of the ASAS Health Index for Patients with Spondyloarthritis: Measurement properties. Acta Reum. Port. 2020, 45, 26–33. [Google Scholar]
- Alonso-Castro, S.; Pardo, E.; Charca, L.; Pino, M.; Fernández, S.; Alperi, M.; Arboleya, L.; Queiro, R. Performance of the ASAS Health Index for the Evaluation of Spondyloarthritis in Daily Practice. J. Rheumatol. 2020, 47, 1483–1489. [Google Scholar] [CrossRef] [PubMed]
- Bautista-Molano, W.; Landewé, R.B.M.; Kiltz, U.; Valle-Oñate, R.; van der Heijde, D. Validation and reliability of translation of the ASAS Health Index in a Colombian Spanish-speaking population with spondyloarthritis. Clin. Rheumatol. 2018, 37, 3063–3068. [Google Scholar] [CrossRef] [PubMed]
- Walsh, J.A.; Magrey, M.N.; Baraliakos, X.; Inui, K.; Weng, M.Y.; Lubrano, E.; van der Heijde, D.; Boonen, A.; Gensler, L.S.; Strand, V.; et al. Improvement of Functioning and Health with Ixekizumab in the Treatment of Active Nonradiographic Axial Spondyloarthritis in a 52-Week, Randomized, Controlled Trial. Arthritis Care Res. 2022, 74, 451–460. [Google Scholar] [CrossRef]
- Kiltz, U.; Wei, J.C.; van der Heijde, D.; van den Bosch, F.; Walsh, J.A.; Boonen, A.; Gensler, L.S.; Hunter, T.; Carlier, H.; Dong, Y.; et al. Ixekizumab Improves Functioning and Health in the Treatment of Radiographic Axial Spondyloarthritis: Week 52 Results from 2 Pivotal Studies. J. Rheumatol. 2021, 48, 188–197. [Google Scholar] [CrossRef]
- Kang, K.Y.; Ju, J.H.; Park, S.H.; Hong, Y.S. Longitudinal Association Between Trabecular Bone Loss and Disease Activity in Axial Spon-dyloarthritis: A 4-year Prospective Study. J. Rheumatol. 2020, 47, 1330–1337. [Google Scholar] [CrossRef]
- Rudwaleit, M.; Landewé, R.; van der Heijde, D.; Listing, J.; Brandt, J.; Braun, J.; Burgos-Vargas, R.; Collantes-Estevez, E.; Davis, J.; Dijkmans, B.; et al. The development of Assessment of SpondyloArthritis international Society classification criteria for axial spondyloarthritis (part I): Classification of paper patients by expert opinion including uncertainty appraisal. Ann. Rheum. Dis. 2009, 68, 770–776. [Google Scholar] [CrossRef]
- van der Linden, S.; Valkenburg, H.A.; Cats, A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984, 27, 361–368. [Google Scholar] [CrossRef] [PubMed]
- Garrett, S.; Jenkinson, T.; Kennedy, L.G.; Whitelock, H.; Gaisford, P.; Calin, A. A new approach to defining disease status in anky-losing spondylitis: The Bath Ankylosing Spondylitis Disease Activity Index. J. Rheumatol. 1994, 21, 2286–2291. [Google Scholar]
- van der Heijde, D.; Lie, E.; Kvien, T.K.; Sieper, J.; Van den Bosch, F.; Listing, J.; Braun, J.; Landewe, R.; ASAS. ASDAS, a highly discriminatory ASAS-endorsed disease activity score in patients with ankylosing spondylitis. Ann. Rheum. Dis. 2009, 68, 1811–1818. [Google Scholar] [CrossRef]
- Calin, A.; Garrett, S.; Whitelock, H.; Kennedy, L.G.; O’Hea, J.; Mallorie, P.; Jenkinson, T. A new approach to defining functional ability in ankylosing spondylitis: The development of the Bath Ankylosing Spondylitis Functional Index. J. Rheumatol. 1994, 21, 2281–2285. [Google Scholar] [PubMed]
- Wanders, A.J.; Landewé, R.B.; Spoorenberg, A.; Dougados, M.; van der Linden, S.; Mielants, H.; van der Tempel, H.; van der Heijde, D.M.F.M. What is the most appropriate radiologic scoring method for ankylosing spondylitis? A comparison of the available methods based on the Outcome Measures in Rheumatology Clinical Trials filter. Arthritis Rheum. 2004, 50, 2622–2632. [Google Scholar] [CrossRef] [PubMed]
- Choi, J.H.; Kim, T.J.; Shin, K.; Choi, C.B.; Kim, J.H.; Kim, S.H.; Kim, N.I.; Ahn, M.J.; Jung, H.J.; Lee, K.E.; et al. The reliability and validity of a Korean translation of the ASAS Health Index and Environmental Factors in Korean patients with axial spondyloarthritis. J. Korean Med. Sci. 2014, 29, 334–337. [Google Scholar] [CrossRef]
- Kiltz, U.; van der Heijde, D.; Boonen, A.; Braun, J. The ASAS Health Index (ASAS HI)—A new tool to assess the health status of patients with spondyloarthritis. Clin. Exp. Rheumatol. 2014, 32, S-105–S-108. [Google Scholar]
- Essers, I.; Hiligsmann, M.; Kiltz, U.; Bansback, N.; Braun, J.; van der Heijde, D.; Boonen, A. Development of one general and six country-specific algorithms to assess societal health utilities based on ASAS HI. RMD Open 2019, 5, e000872. [Google Scholar] [CrossRef]
- Min, H.K.; Lee, J.; Ju, J.H.; Park, S.H.; Kwok, S.K. Predictors of Assessment of Spondyloarthritis International Society (ASAS) Health Index in Axial Spondyloarthritis and Comparison of ASAS Health Index between Ankylosing Spondylitis and Nonradiographic Axial Spondyloarthritis: Data from the Catholic Axial Spondyloarthritis COhort (CASCO). J. Clin. Med. 2019, 8, 467. [Google Scholar] [CrossRef]
- Kiltz, U.; Wiatr, T.; Redeker, I.; Baraliakos, X.; Fedorov, K.; Braun, J. Effects of patient and disease characteristics on global functioning in patients with axial spondyloarthritis in routine care. Semin. Arthritis Rheum. 2022, 55, 152006. [Google Scholar] [CrossRef]
- Smith, J.A.; Colbert, R.A. Review: The Interleukin-23/Interleukin-17 Axis in Spondyloarthritis Pathogenesis: Th17 and Beyond. Arthritis Rheumatol. 2014, 66, 231–241. [Google Scholar] [CrossRef]
- Wu, B.; Nakamura, A. Deep Insight into the Role of MIF in Spondyloarthritis. Curr. Rheumatol. Rep. 2022, 24, 269–278. [Google Scholar] [CrossRef]
- Reveille, J.D.; Ximenes, A.; Ward, M.M.; Deodhar, A.; Clegg, D. Economic Considerations of the Treatment of Ankylosing Spondylitis. Am. J. Med. Sci. 2012, 343, 371–374. [Google Scholar] [CrossRef]
- Kiltz, U.; Baraliakos, X.; Karakostas, P.; Igelmann, M.; Kalthoff, L.; Klink, C.; Krause, D.; Schmitz-Bortz, E.; Flörecke, M.; Bollow, M.; et al. The degree of spinal inflammation is similar in patients with axial spondyloarthritis who report high or low levels of disease activity: A cohort study. Ann. Rheum. Dis. 2012, 71, 1207–1211. [Google Scholar] [CrossRef] [PubMed]
- Landewé, R.B.M.; van der Heijde, D. Use of multidimensional composite scores in rheumatology: Parsimony versus subtlety. Ann. Rheum. Dis. 2021, 80, 280–285. [Google Scholar] [CrossRef]

{kind=link}
| Variable | Total (N = 185, N (%) or Mean ± SD) |
|---|---|
| Age, years | 37.4 ± 10.8 |
| Male | 155 (84) |
| Body mass index, kg/m2 | 24.7 ± 3.9 |
| Symptom duration, years | 9.7 ± 7.9 |
| HLA-B27-positive | 164 (89) |
| Current smoking | 77 (42) |
| Alcohol drinking, days of alcohol consumption per week | 1.0 ± 1.1 |
| ASAS HI (0–17) | 2.7 ± 2.9 |
| BASFI (0–10) | 0.9 ± 1.3 |
| BASDAI (0–10) | 2.3 ± 1.9 |
| ASDAS | 1.7 ± 1.2 |
| CRP, mg/L | 4.6 ± 9.1 |
| Radiographic sacroiliitis | 128 (69) |
| mSASSS | 7.7 ± 12.0 |
| Number of syndesmophytes | 3.1 ± 5.6 |
| NSAIDs | 173 (94) |
| Sulfasalazine | 93 (50) |
| TNF inhibitors | 37 (20) |
| Variable | Baseline | 1 Year Follow-Up | p-Value |
|---|---|---|---|
| ASAS HI (0–7) | 2.7 ± 2.9 | 2.4 ± 2.7 | 0.03 |
| BASFI score (0–10) | 0.9 ± 1.3 | 0.7 ± 1.1 | <0.01 |
| BASDAI score (0–10) | 2.3 ± 1.9 | 1.9 ± 1.5 | <0.01 |
| ASDAS | 1.7 ± 1.2 | 1.3 ± 0.9 | <0.01 |
| CRP, mg/L | 4.6 ± 9.1 | 3.3 ± 6.0 | 0.06 |
| Changes of ASAS HI Score | ||
|---|---|---|
| r | p-Value | |
| Changes in the BASFI score (0–10) | 0.31 | <0.01 |
| Changes in the BASDAI score (0–10) | 0.37 | <0.01 |
| Changes in the ASDAS | 0.12 | <0.01 |
| Changes in CRP level, mg/L | 0.15 | 0.047 |
| Variables | Univariate Analysis | Multivariate Analysis # | ||
|---|---|---|---|---|
| β (95% CI) | p-Value | β (95% CI) | p-Value | |
| Age, years | 0.01 (−0.02–0.03) | 0.70 | ||
| Male sex | 0.45 (−0.33–1.25) | 0.27 | ||
| Body mass index, kg/m2 | 0.09 (0.01–0.16) | 0.02 | 0.06 (−0.00–0.13) | 0.08 |
| Current smoking | 0.16 (−0.43–0.76) | 0.60 | ||
| Alcohol drinking, days of alcohol consumption per week | −0.05 (−0.32–0.23) | 0.75 | ||
| HLA-B27-positive | 0.34 (−0.58–1.27) | 0.47 | ||
| Radiographic sacroiliitis | −0.37 (−1.00–0.27) | 0.26 | ||
| Number of syndesmophytes | −0.04 (−0.09–0.02) | 0.17 | ||
| NSAIDs | 0.21 (−0.72–1.13) | 0.66 | ||
| Sulfasalazine | −0.29 (−0.87–0.30) | 0.34 | ||
| TNF inhibitor | 0.64 (0.00–1.28) | 0.048 | 0.43 (−0.15–1.04) | 0.14 |
| Change in BASFI score | 0.56 (0.32–0.81) | <0.01 | 0.33 (0.06–0.60) | 0.02 |
| Change in BASDAI score | 0.47 (0.30–0.64) | <0.01 | 0.33 (0.13–0.52) | <0.01 |
| Change in ASDAS | 0.24 (−0.04–0.51) | 0.10 | ||
| Change in CRP, mg/L | 0.03 (0.00–0.06) | 0.04 | ||
| Variables | Univariate Analysis | Multivariate Analysis # | ||
|---|---|---|---|---|
| Odds Ratio (95% CI) | p-Value | Odds Ratio (95% CI) | p-Value | |
| Age, years | 1.01 (0.97–1.06) | 0.65 | ||
| Male sex | 1.73 (0.38–7.89) | 0.48 | ||
| Body mass index, kg/m2 | 1.08 (0.96–1.21) | 0.22 | ||
| Current smoking | 1.64 (0.63–4.26) | 0.31 | ||
| Alcohol drinking, days of alcohol consumption per week | 1.05 (0.68–1.63) | 0.82 | ||
| HLA-B27-positive | 1.10 (0.24–5.13) | 0.91 | ||
| Radiographic sacroiliitis | 0.58 (0.22–1.52) | 0.27 | ||
| Number of syndesmophytes | 0.97 (0.87–1.08) | 0.56 | ||
| NSAIDs | 2.47 (0.31–19.49) | 0.39 | ||
| Sulfasalazine | 0.67 (0.25–1.80) | 0.43 | ||
| TNF inhibitor | 2.35 (0.90–6.15) | 0.08 | ||
| Change in BASFI score | 1.80 (1.28–2.51) | <0.01 | 1.47 (1.01–2.14) | 0.047 |
| Change in BASDAI score | 1.64 (1.25–2.15) | <0.01 | 1.41 (1.04–1.91) | 0.03 |
| Change in ASDAS | 1.87 (1.25–2.81) | <0.01 | ||
| Change in CRP, mg/L | 1.05 (1.01–1.09) | 0.02 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kang, K.Y.; Adler, B.L.; Chung, T.H. Predictors for Improvement of Global Functioning in Patients with Axial Spondyloarthritis. J. Clin. Med. 2025, 14, 4474. https://doi.org/10.3390/jcm14134474
Kang KY, Adler BL, Chung TH. Predictors for Improvement of Global Functioning in Patients with Axial Spondyloarthritis. Journal of Clinical Medicine. 2025; 14(13):4474. https://doi.org/10.3390/jcm14134474
Chicago/Turabian StyleKang, Kwi Young, Brittany L. Adler, and Tae Hwan Chung. 2025. "Predictors for Improvement of Global Functioning in Patients with Axial Spondyloarthritis" Journal of Clinical Medicine 14, no. 13: 4474. https://doi.org/10.3390/jcm14134474
APA StyleKang, K. Y., Adler, B. L., & Chung, T. H. (2025). Predictors for Improvement of Global Functioning in Patients with Axial Spondyloarthritis. Journal of Clinical Medicine, 14(13), 4474. https://doi.org/10.3390/jcm14134474