Abstract
Background: Work-related injuries remain a considerable global burden; nevertheless, progress in occupational safety has been made in decreasing the time to return to work. This study aimed to assess the pooled incidence of Return to Work (RTW) among workers with occupational injuries and to identify the key factors influencing RTW outcomes. Methods: A systematic review was conducted by searching electronic databases (PubMed, Embase, Cochrane CENTRAL, Web of Science, and Scopus) to include eligible cohorts. Meta-analysis was undertaken using R software 4.5.1 with random-effects models, and heterogeneity was evaluated using the I2 statistic. Results: This meta-analysis included 16 cohorts, with 4164 workers. A pooled analysis of 14 studies showed that 79% of workers successfully returned to their jobs after treatment for work-related injuries (95% CI: 0.67–0.88; p < 0.0001; I2 = 97.5%). Meta-regression identified age as a significant moderator, with older workers showing a higher incidence of RTW. The mean time to RTW, pooled from 9 studies, was approximately 102 days, with no significant age association (p = 0.222). Regarding predictors, male workers had a significantly higher RTW rate than females (p < 0.0001). Married persons showed greater RTW rates (p < 0.0001). Also, workers with higher education levels were more likely to return to work (p = 0.0033). For injury type, lacerations were related to a greater RTW rate than crushing injuries. Conclusions: This meta-analysis underscored a significant overall return-to-work rate after work-related injuries, with age, sex, marital status, education level, and injury type affecting results. Advanced age and male sex were substantially correlated with increased return-to-work rates. These findings support the necessity for personalized rehabilitation programs and focused support to enhance work reintegration following occupational accidents.
1. Introduction
Every year, millions of workers in different industries suffer from work-related injuries, which are a serious concern in all occupational settings [1,2]. With about 340 million work-related accidents and 160 million work-related illnesses reported annually worldwide, the incidence of occupational injuries remains high despite improvements in workplace safety and technology [2]. Mechanical injuries are the primary and most-often documented injury in the industrial, construction, agricultural, and transportation sectors. They usually arise from different conditions, such as operator error, equipment malfunction, ineffective safety measures, and a failure to control machinery effectively [3].
Moreover, workers may be injured by being caught in or struck by moving machine parts, entanglement of clothing or hair, contact with sharp or abrasive surfaces, or the collapse or malfunction of heavy equipment, such as cranes and powered industrial trucks. Additional hazards encompass falls from elevations, overexertion, repetitive strain, crushing accidents, lacerations, and avulsions [3,4].
The consequences of these injuries can be serious, ranging from superficial lacerations and contusions to amputations, musculoskeletal abnormalities, or death. Specific populations, including younger and older employees and individuals in high-risk sectors, such as fishing, agriculture, and manufacturing, are particularly vulnerable [5,6,7].
Following an industrial injury, the time taken for individuals to return to work (TRTW) is a major concern with great consequences for organizational stakeholders as well as people. TRTW varies among individuals, depending on the injury severity, injury site, worker’s health condition, and the nature of the work. Extended absence combined with loss of income threatens employees’ financial stability [8,9].
The efficacy of recovery largely depends on the proficient management of the rehabilitation process. Timely intervention and tailored care plans implemented in structured rehabilitation programs have demonstrated efficacy in expediting physical recovery and reducing the likelihood of long-term disability. Integrating physiotherapy and ergonomic evaluations mitigates injury exacerbation and promotes safer reintegration into occupational environments. Enhancing employee capability typically yields improved success rates for firms that monitor progress and implement changes per healthcare providers [10,11].
TRTW schedules enhance productivity and assist in diminishing the long-term financial costs associated with recurrent absences. Multiple studies have shown that individuals re-entering the workforce via phased programs, such as part-time hours or diminished responsibilities, display superior job retention rates and faster full recovery than those returning without such provisions. Organizations gain from reduced turnover costs and retained institutional expertise, while employees attain financial security and support. A manufacturing company that adopted graduated work schedules experienced a 30% reduction in absenteeism-related costs after six months, highlighting the financial benefits of early reintegration strategies [12,13].
Older age, more severe injuries, higher pain levels, and the existence of comorbid conditions, all of which have been repeatedly linked to longer work absences, are some of the factors that influence TRTW and the incidence of RTW. On the other hand, it has been demonstrated that early graded return to work programs and greater educational attainment reduce the time spent away from work [14,15].
While multiple studies have assessed factors influencing the RTW process, the current body of evidence remains fragmented. A number of systematic reviews have examined RTW outcomes in specific populations, such as individuals with musculoskeletal disorders, low-back pain, or traumatic brain injuries, or within particular occupational sectors [16,17]. However, these reviews are typically limited in scope, focusing either on narrowly defined clinical subgroups or on intervention-specific outcomes, thereby constraining the generalizability of their findings. Therefore, the purpose of this study is to investigate how often employees who have suffered work-related injuries return to their jobs and the factors that influence this occurrence.
2. Materials and Methods
2.1. Study Design
Following the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines, a systematic review and meta-analysis of published literature was conducted [18].
2.2. Search Strategy
Several electronic databases were searched, including PubMed, Embase, Cochrane Library, Web of Science (WoS), Cochrane CENTRAL, Scopus, APA PsycInfo, and Ovid. Search terms combined MeSH keywords related to “return to work,” “work-related injuries,” “occupational accident,” “industrial injury,” “vocational rehabilitation,” and “employment outcomes”.
2.3. Eligibility Criteria
Studies were eligible for inclusion if they involved adult participants (≥18 years) who sustained work-related injuries in occupational settings and reported outcomes related to return to work. Eligible outcomes included, but were not limited to, incidence of return to work, time to first return, and predictors of RTW, such as sex, age, educational status, type of injury, and marital status. Only observational cohort studies (prospective or retrospective) were included. Studies were excluded if they focused on non-occupational injuries, lacked quantitative return-to-work data, or were case reports, cross-sectional studies, or conference abstracts without full texts.
2.4. Screening Process
The records were screened twice by two separate reviewers. First, abstracts and titles were examined for appropriateness. The eligibility of full-text articles was then evaluated using the inclusion and exclusion criteria. Reviewers’ disagreements were settled by discussion.
2.5. Data Extraction
Using a standardized Excel form, two reviewers extracted data separately. Risk factors affecting return to work, demographic traits, and return-to-work outcomes (such as incidence and time to return) were among the extracted variables. Reviewers’ disagreements were settled by discussion.
2.6. Risk of Bias Assessment
The methodological quality of included studies was assessed independently by two reviewers using the National Institutes of Health (NIH) Quality Assessment Tool for Observational Cohort Studies. Any disagreements were resolved through discussion and consensus. The tool evaluated aspects such as clarity of research objectives, participant selection, exposure and outcome measures, follow-up rates, confounding control, and statistical analysis.
2.7. Statistical Analysis
R software 4.5.1 was used for all statistical analyses. For dichotomous outcomes, risk ratios (RRs) were computed along with 95% CIs. In single-arm studies, overall means were reported for continuous outcomes. The I2 statistic was used to evaluate heterogeneity. If significant heterogeneity was found, a random-effects model was used. Sensitivity analyses were performed to examine the strength of the results by eliminating studies with a high risk of bias or showing statistical outliers in effect size. Confounders were also used in regression analysis and subgrouping to help investigate the source of heterogeneity.
2.8. Ethical Considerations
Ethical approval was not required as this study utilized data from previously published literature without directly involving human participants.
3. Results
A total of 2044 articles were initially retrieved from five electronic databases. Following the removal of duplicates, 1209 studies underwent title and abstract screening. Of these, 75 articles were selected for full-text assessment based on the eligibility criteria. In the end, 16 studies met the inclusion criteria and were included in the final analysis [8,9,19,20,21,22,23,24,25,26,27,28,29,30,31,32], as illustrated in Figure 1.
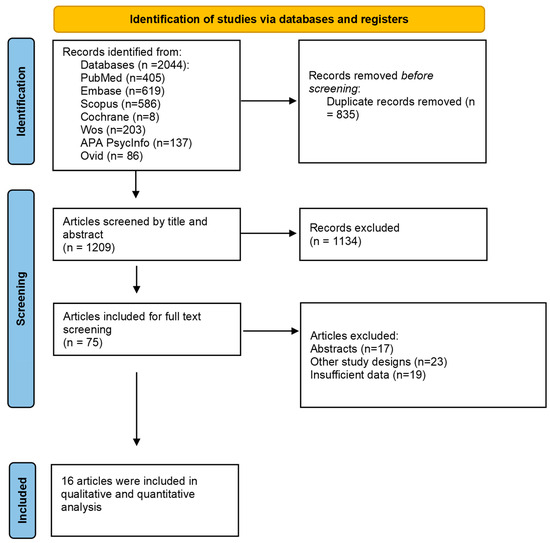
Figure 1.
Prisma flow diagram.
Out of the included 16 articles, five were prospective cohorts, while the rest were retrospective. A total of 4164 patients were included in this meta-analysis. Hand injuries were the most reported injuries among the included studies. Most of the studies were in Taiwan (37.5%). The majority were males aged between 25 and 60, as shown in Table 1.

Table 1.
Baseline characteristics and quality assessment of included studies.
3.1. Risk of Bias Assessment
Using the NIH tool, seven studies were of good quality, seven were of moderate quality, and two were of low quality, as mentioned in Table 2.
Table 2.
Quality assessment of included studies using NIH tool.
3.2. Outcomes
3.2.1. Incidence of RTW
A meta-analysis of fourteen studies was undertaken to explore the incidence of return to work among workers who had work-related injuries. A total of 79% of workers returned to their work after a successful treatment strategy (95% CI: 0.67–0.88, p < 0.0001, I2 = 97.5%). A random-effects model was employed, as shown in Figure 2.
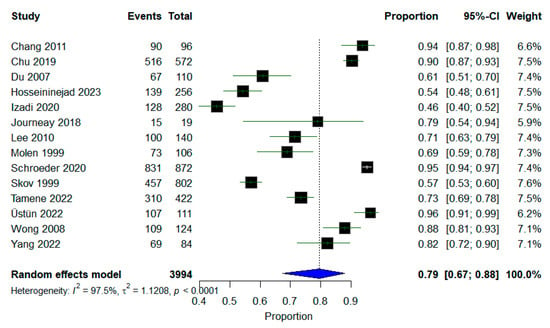
Figure 2.
A forest plot of the incidence of workers who returned to their jobs.
Subgroup analysis was conducted based on the country’s continent; most of the studies were of Asian origin, but heterogeneity was high among all subgroups, with I2 equal to 97.1%. North American studies showed I2 = 97.3%, with no change in the context of results, as shown in Figure 3.
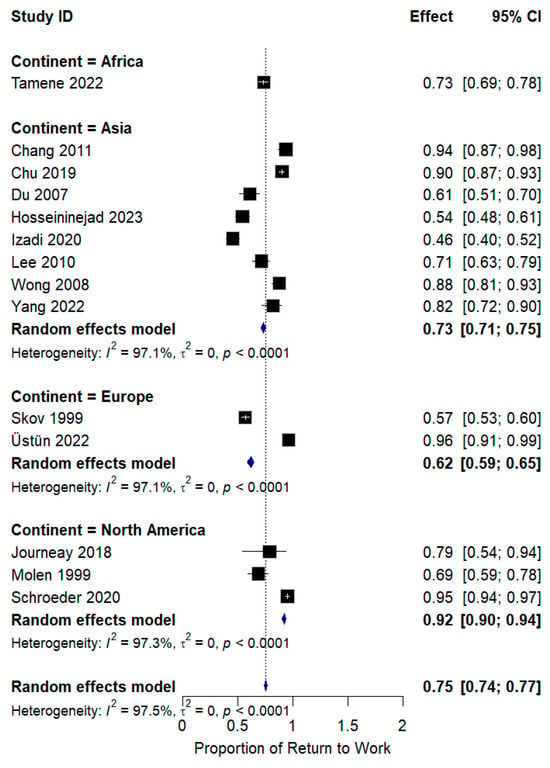
Figure 3.
Subgroup analysis of RTW incidence according to continent.
Subgroup analysis was also performed based on the year of publication; we found that heterogeneity was reduced among all groups except studies published after 2020, especially for studies published between 2011 and 2020, with a significant OR of 0.90 and I2 = 48.6%, as shown in Figure 4.
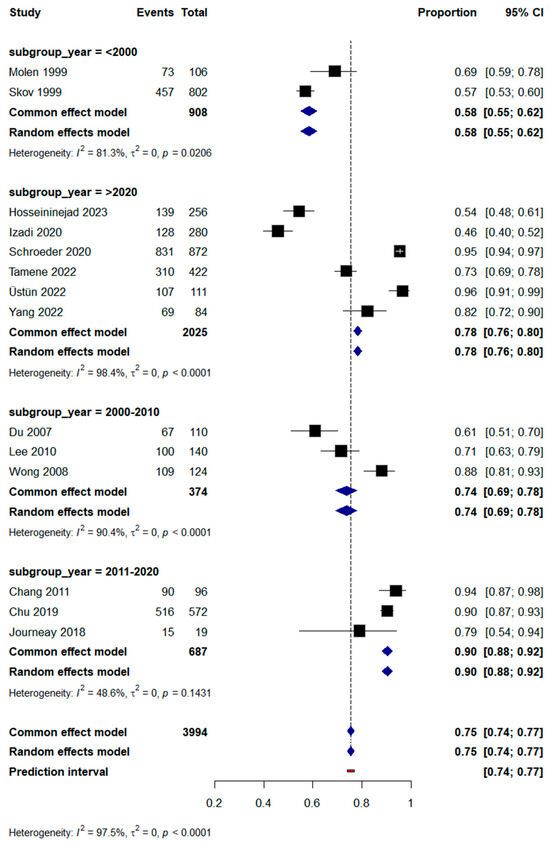
Figure 4.
Subgroup analysis of RTW incidence based on year of publication.
3.2.2. Meta-Regression
Meta-regression based on age demonstrated that age was a statistically significant moderator of the treatment effect across studies. The regression coefficient for age was 0.1453 (SE = 0.0446), indicating that for each additional year of mean participant age, log RR increased by approximately 0.15 units. This effect was statistically significant (t = 3.26, df = 12, p = 0.0068), with a 95% confidence interval ranging from 0.0481 to 0.2424, suggesting a consistent and positive relationship between age and treatment effect. Older workers were associated with a higher incidence of RTW, as shown in Figure 5.
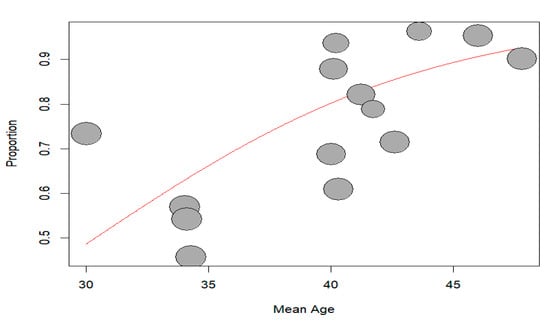
Figure 5.
Bubble plot of meta-regression of RTW based on age.
Visual inspection of the funnel plot suggested asymmetry indicative of publication bias. Egger’s test for funnel plot asymmetry was performed to assess potential publication bias in the meta-analysis. The test yielded a bias coefficient of 6.2134 (SE = 3.1211), with a t-value of 1.99 (df = 12) and a corresponding p-value of 0.0698, suggesting no strong evidence of publication bias, as shown in Figure 6.
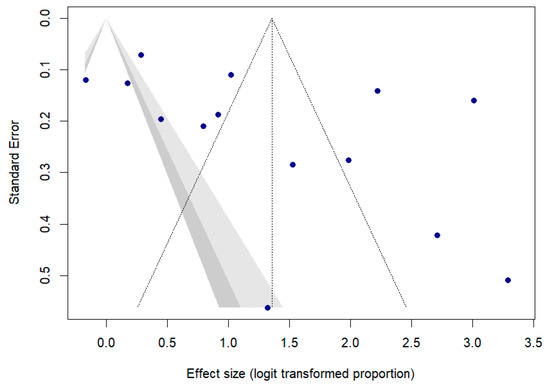
Figure 6.
Funnel plot of return to work.
3.2.3. Time to Return to Work
Nine studies reported the mean time to return to work; a meta-analysis was conducted to calculate the overall mean TRTW. A random-effects model was employed. The pooled mean time to return to work was 101.98 days (95% CI: 38.57–165.19, I2 = 99.5%), as shown in Figure 7.
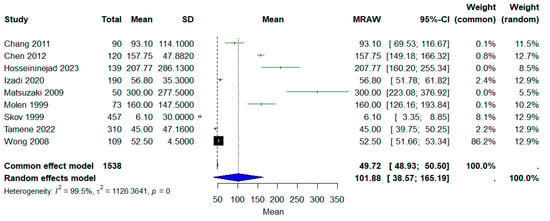
Figure 7.
Forest plot of mean time to return to work.
With respect to exploring potential heterogeneity, no significant association was observed between age and time to return to work, with p equal to 0.2224, as shown in Figure 8.
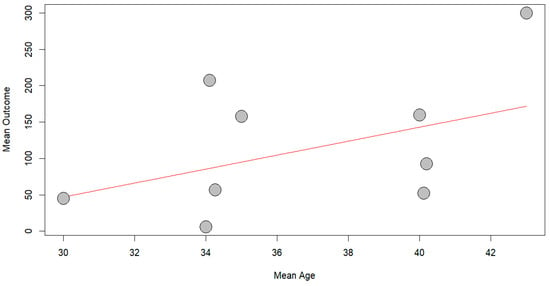
Figure 8.
Bubble plot of meta-regression of TRTW based on age.
3.2.4. Predictors of RTW
Sex:
A meta-analysis comparing the incidence of RTW between males and females showed a significantly higher likelihood of RTW among males. The pooled risk ratio was 6.12 (95% CI: 2.33–16.06, p < 0.0001; I2 = 95.8%). Subgroup analysis was performed based on the year of publication before and after 2015; it was found that heterogeneity was reduced among studies published before 2015, with I2 = 74.7%, while it increased among papers after 2015 to 97.2%, as summarized in Table 3.
Table 3.
Summary of meta-analysis for predictors of return to work (RTW).
Marital Status:
Meta-analysis revealed a significant difference between single and married workers with an RR of 0.43 (95% CI: 0.18–1.02, p < 0.0001; I2 = 88.3%), meaning that 57% of married workers return to their jobs. A random-effects model was used. A sensitivity analysis was performed by excluding Hosseininejad et al. [19]; heterogeneity was reduced to 46.1%, with a change in the context of the results showing no statistically significant difference between both groups, with p 0.1563, as summarized in Table 3.
Educational Status:
Workers with education more than grade 12 were more likely to return to work than those with less education, with a pooled RR of 0.54 (95% CI: 0.34–0.87, p = 0.0033; I2 = 78.1%). A sensitivity analysis excluding Tamene et al.’s study [9] showed a trend reversal, favoring lower-educated workers, with an RR of 0.47 (95% CI: 0.29–0.77, p = 0.2562; I2 = 26.6%). All results were obtained using a random-effects model, as summarized in Table 3.
Injury:
In terms of injury, three studies mentioned crushing and laceration injuries among workers. A meta-analysis of three studies showed that workers with lacerations had a higher incidence of RTW compared to crushing injuries, with an RR of 1.89 (95% CI: 0.11–33.74, p < 0.0001; I2 = 91.6%). A sensitivity analysis was performed by excluding Du et al., where heterogeneity was reduced to 19.1%, shifting results towards insignificance, supporting no difference between both groups with p = 0.2667, as summarized in Table 3.
4. Discussion
Occupational injuries are increasing nowadays, which calls for attention to explain their causes and update the incidence. This study explored the incidence and mean time to return to work.
4.1. Incidence and Timing of RTW
Our overall RTW incidence of 79% aligns with higher estimates for less severe or well-managed injuries. Nevertheless, the majority of injured workers eventually resumed employment, which aligns with prior evidence showing that over 60% of workers with traumatic injuries return by 6 months post-injury [33]. Several meta-analyses of return to work after injury have reported RTW rates ranging from just over 50% in major trauma populations to over 80% in specific injury cohorts. For instance, a systematic review of mild traumatic brain injury found that more than half of patients had returned by one month and over 80% by six months post-injury [17,34]. In workers with back pain, 80–90% return-to-work rates have been described for short-term absences. After major trauma, patterns and predictors of RTW revealed early sustained RTW in 51.6% of respondents and complete non-RTW in 19.7% of respondents [10]. Also, a recent meta-analysis of post-COVID-19 RTW showed a pooled RTW proportion of 60.9% at 12 weeks [35].
The persistently high RTW rates noted, even in cases of serious damage, indicate that with enough support, numerous workers can successfully reintegrate into the labor field. Timely and proactive return-to-work facilitation is essential. Several studies emphasized that multidisciplinary approaches coordinating clinical care with workplace accommodations are useful in enhancing RTW results [17]. For example, ergonomic adjustments, graded return programs, and vocational rehabilitation should be standard considerations in management plans [36].
Clinicians should, therefore, not only treat the injury but also manage pain adequately and screen for issues like depression or catastrophic thinking. Intervening on these factors, through pain management, psychosocial support, and work-focused therapy, can improve a patient’s chances of successful RTW [26].
4.2. Influence of Age
Generally, age has been considered a risk factor for delayed or unsuccessful RTW. Across various health conditions, older age (e.g., >50 years) is strongly associated with longer work disability and lower likelihood of RTW [11].
In contrast to numerous studies that recognize younger age as a promoter of RTW, our meta-regression revealed that older age correlated with increased RTW rates. More research is needed to study this relationship. Cancelliere et al. revealed that, across diverse injury and illness conditions, advanced age is generally associated with reduced RTW rates; however, this association is not universally consistent and may be influenced by additional factors such as employment stability, job classification, and workplace support systems [17]. Possible reasons include age-related comorbidities, slower physical recovery, and the fact that older individuals are closer to retirement. Yet our findings align with a subset of evidence suggesting a more complex reality. Some prior studies on workplace injury have noted that, when other factors are controlled, older workers can have outcomes as good as or even better than younger workers [37]. Furthermore, older employees often occupy more stable or senior positions that may be more accommodating of injury-related limitations. They may have access to light-duty roles or administrative tasks, enabling earlier return. Additionally, older workers may be especially motivated to resume work quickly, recognizing that finding new employment later in life is challenging. This heightened motivation and employer flexibility could explain why older age appeared as a favorable factor in our analysis. Socioeconomic and policy factors are also crucial in interpreting this age paradox. It is possible that many older individuals in our included studies were in higher-income or salaried positions that came with better benefits and return-to-work support. In contrast, younger injured workers, who might be overrepresented in manual labor or lower-income jobs, could face more barriers [33,38].
Our findings also indicate that younger workers may have been overrepresented in high-risk categories, while older workers with established careers benefited from resources and support that aided their return. Certain cultures or regions may have standards and regulations that promote the continued employment of older workers, so the cultural context contributes to this explanation, as most of the included studies were of Asian origin. A study of injured workers in Israel indicated that older workers were more likely to return to work in the short term, potentially due to a strong work ethic and fear of job loss [38]. However, those nearing retirement age exhibited a higher risk of exiting the workforce through early retirement. Our review indicates that the “older” workers were generally middle-aged (in their 40s or 50s) rather than at the conventional retirement age, which may partially account for the positive association observed. These individuals likely retained significant financial obligations and career commitments, motivating them to return to work. Conversely, workers approaching retirement may opt to retire following a significant injury; however, such instances may be underrepresented in the data. The finding that older age correlates with higher rates of return to work can be elucidated by various socioeconomic and cultural factors. Older workers who continue to participate in the labor force typically represent a distinct subset characterized by enhanced job security, elevated motivation, and more flexible work environments, all of which facilitate RTW [37,38]. There is a need for additional research on the impact of workplace accommodations, seniority benefits, and cultural attitudes towards older workers on successful RTW outcomes, aiming to develop effective strategies applicable to all age groups.
4.3. Sex Differences
Men are more likely to work than women and have a higher and faster recovery compared to women. We found that males were over six times more likely to RTW than females, with consistent results before and after 2015. Etuknwa et al. also reported inconsistent results regarding gender differences in RTW rates [39]. Conversely, findings from Rijik et al., a cohort study from the Netherlands, demonstrated no differences between males and females regarding RTW after occupational injury [40].
4.4. Marital Status and Education
Our findings showed that married workers initially appeared more likely to RTW, while sensitivity analysis attenuated this effect. Social support from spouses has been posited as a facilitator of RTW in chronic conditions [41], but findings have been inconsistent after sensitivity analysis, which needs further investigation in future studies. Educational attainment was positively associated with RTW, aligning with studies reporting that higher education and socioeconomic status enhance access to resources, health literacy, and workplace flexibility [42,43].
4.5. Impact of Injury Type
This study found that workers with lacerations had a higher RTW incidence than those with crushing injuries, echoing prognostic studies in hand trauma where injury severity inversely correlates with RTW prospects. Crushing injuries often entail more extensive soft-tissue and neurovascular compromise, prolonging recovery and complicating return. This aligns with prior prognostic studies in hand trauma and the general injury literature, where the severity and complexity of injury inversely correlate with RTW prospects [44].
4.6. Strengths and Limitations
Although this study provides a comprehensive assessment of RTW, several limitations should be mentioned. First, most of our analyses had high heterogeneity (I2 > 90%), reducing confidence in the pooled estimates. The predominance of retrospective cohort studies also indicates a potential selection and information bias. Moreover, there was a significant publication bias among the included studies, as suggested by funnel plot asymmetry, which further limits the reliability of the findings. Additionally, the geographical concentration of studies in Asia and the lack of representation from low-resource settings constrain the external validity and generalizability of the results. Furthermore, the sensitivity analyses caused a shift in results, which need to be studied further in future studies.
Future research should focus on establishing standardized metrics for RTW, including clear distinctions between sustainable and initial RTW, alongside consistent follow-up durations. Large-scale, prospective multicenter cohort studies are recommended to mitigate bias and allow for the evaluation of time-varying predictors. Moreover, incorporating psychosocial variables, such as self-efficacy, workplace support, and mental health, may clarify the non-clinical determinants of RTW. Intervention trials assessing the efficacy of targeted RTW programs, including workplace accommodations and graded return protocols, using randomized designs, are also needed. Finally, expanding research to include underrepresented regions and occupational sectors would enhance the global applicability of findings.
This review highlighted the need for improved research quality in occupational injury rehabilitation, focusing on potential directions for future studies. We suggest using prospective designs with thorough follow-up to generate more dependable prognostic evidence. Standardization of outcome measurement is crucial, and understanding the long-term employment pathways of injured workers is essential. Comparative studies across different countries or labor systems can elucidate the impact of policies on return-to-work rates. Qualitative research can offer insights into personal, cultural, and organizational factors affecting return to work, and addressing modifiable factors is essential. Employer training and workplace accommodation programs can enhance return-to-work outcomes. Addressing these gaps will enhance guidance for clinicians and policymakers.
5. Conclusions
This meta-analysis demonstrated that approximately 80% of injured workers return to work within an average of 102 days. Factors such as older age, male gender, and higher levels of education were associated with more favorable RTW incidence. Implementing individualized rehabilitation strategies and supportive workplace policies remains essential to improve RTW outcomes across various injury types and worker populations, so further studies are warranted to explore these points.
Author Contributions
Conceptualization, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; methodology, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; software, W.S., G.M., A.H.Z. and R.L.; validation, W.S. and R.L.; formal analysis, W.S., G.M., A.H.Z. and R.L.; investigation, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; resources, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; data curation, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; writing—original draft preparation, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; writing—review and editing, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; visualization, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L.; supervision, W.S., C.R., R.I., A.L., A.D., G.M., A.H.Z. and R.L. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Primary data for the systematic literature review are reported in the referenced publications.
Conflicts of Interest
The authors declare no conflicts of interest.
Abbreviations
The following abbreviations are used in this manuscript:
| CI | Confidence Interval |
| PRISMA | Preferred Reporting Items for Systematic Reviews and Meta-Analyses |
| RTW | Return to Work |
References
- McMullin, B.; Fraser, J.; Robinson, B.; French, J.; Adisesh, A. Work-related injuries and attendance at a Canadian regional emergency department. Occup. Med. 2023, 73, 138–141. [Google Scholar] [CrossRef] [PubMed]
- Takala, J.; Hämäläinen, P.; Sauni, R.; Nygård, C.H.; Gagliardi, D.; Neupane, S. Global-, regional-and country-level estimates of the work-related burden of diseases and accidents in 2019. Scand. J. Work Environ. Health 2024, 50, 73–82. [Google Scholar] [CrossRef] [PubMed]
- Debela, M.B.; Azage, M.; Begosaw, A.M. Prevalence of Occupational Injury among Workers in the Construction, Manufacturing, and Mining Industries in Africa: A Systematic Review and Meta-analysis. J. Occup. Health Epidemiol. 2021, 10, 113–126. [Google Scholar] [CrossRef]
- Abdalla, S.; Apramian, S.S.; Cantley, L.F.; Cullen, M.R. Occupation and Risk for Injuries, 3rd ed.; Mock, C.N., Nugent, R., Kobusingye, O., Smith, K., Eds.; The International Bank for Reconstruction and Development: Washington, DC, USA, 2017. [Google Scholar]
- Ronconi, L.; Anchorena, J.; Paz, J. The incidence and severe consequences of occupational injuries among informal workers in a developing country. Int. J. Occup. Saf. Ergon. 2025, 31, 560–567. [Google Scholar] [CrossRef] [PubMed]
- Salminen, S. Have young workers more injuries than older ones? An international literature review. J. Saf. Res. 2004, 35, 513–521. [Google Scholar] [CrossRef]
- Khorshidi, H.A.; Marembo, M.; Aickelin, U. Predictors of Return to Work for Occupational Rehabilitation Users in Work-Related Injury Insurance Claims: Insights from Mental Health. J. Occup. Rehabil. 2019, 29, 740–753. [Google Scholar] [CrossRef]
- Skov, O.; Jeune, B.; Lauritsen, J.M.; Barfred, T. Time Off Work After Occupational Hand Injuries. J. Hand Surg. Br. Eur. Vol. 1999, 24, 187–189. [Google Scholar] [CrossRef]
- Tamene, A.; Habte, A.; Derilo, H.T.; Endale, F.; Gizachew, A.; Sulamo, D.; Afework, A. Time to Return to Work After an Occupational Injury and Its Prognostic factors Among Employees of Large-Scale Metal Manufacturing Facilities in Ethiopia: A Retrospective Cohort. Environ. Health Insights 2022, 16, 11786302221109372. [Google Scholar] [CrossRef]
- Kalski, L.; Völkel, L.; Häußler, S.; Wolfarth, B.; Jacobs, K.; Soer, R. Efficacy of occupational rehabilitation in return to work for back pain: A systematic literature review. Work 2023, 78, 29–43. [Google Scholar] [CrossRef]
- Williams, R.M.; Westmorland, M.G.; Lin, C.A.; Schmuck, G.; Creen, M. Effectiveness of workplace rehabilitation interventions in the treatment of work-related low back pain: A systematic review. Disabil. Rehabil. 2007, 29, 607–624. [Google Scholar] [CrossRef]
- Grabe, E.M. Gradual Return to Work: Maximizing Benefits to Corporations and Their Caregiver Employees. J. Corp Law 2012, 37, 699. [Google Scholar]
- Flynn, S.; Ghent, A.C.; Nair, V. Determinants and Consequences of Return to Office Policies. SSRN Electron. J. 2024. Available online: https://api.semanticscholar.org/CorpusID:269102390 (accessed on 13 June 2025).
- Maas, E.T.; Koehoorn, M.; McLeod, C.B. Does gradually returning to work improve time to sustainable work after a work-acquired musculoskeletal disorder in British Columbia, Canada? A matched cohort effectiveness study. Occup. Environ. Med. 2021, 78, 715. [Google Scholar] [CrossRef] [PubMed]
- Duong, H.P.; Garcia, A.; Hilfiker, R.; Léger, B.; Luthi, F. Systematic Review of Biopsychosocial Prognostic Factors for Return to Work After Acute Orthopedic Trauma: A 2020 Update. Front. Rehabil. Sci. 2022, 2, 791351. [Google Scholar] [CrossRef] [PubMed]
- Cullen, K.L.; Irvin, E.; Collie, A.; Clay, F.; Gensby, U.; Jennings, P.A.; Hogg-Johnson, S.; Kristman, V.; Laberge, M.; McKenzie, D.; et al. Effectiveness of workplace interventions in return-to-work for musculoskeletal, pain-related and mental health conditions: An update of the evidence and messages for practitioners. J. Occup. Rehabil. 2018, 28, 1–15. [Google Scholar] [CrossRef]
- Cancelliere, C.; Donovan, J.; Stochkendahl, M.J.; Biscardi, M.; Ammendolia, C.; Myburgh, C.; Cassidy, J.D. Factors affecting return to work after injury or illness: Best evidence synthesis of systematic reviews. Chiropr. Man. Ther. 2016, 24, 32. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef]
- Hosseininejad, M.; Javadifar, S.; Mohammadi, S.; Mirzamohammadi, E. Assessment of the relationship between the return to work and the severity of work-related upper limb injuries using the whole person impairment. Chin. J. Traumatol. 2023, 26, 77–82. [Google Scholar] [CrossRef]
- Chen, Y.H.; Lin, H.T.; Chao, Y.H.; Lin, C.H.; Wei, F.C.; Lien, S.H. Self-perceived health and return to work following work-related hand injury. Occup. Med. 2012, 62, 295–297. [Google Scholar] [CrossRef]
- Chang, J.-H.; Wu, M.; Lee, C.-L.; Guo, Y.-L.; Chiu, H.-Y. Correlation of return to work outcomes and hand impairment measures among workers with traumatic hand injury. J. Occup. Rehabil. 2011, 21, 9–16. [Google Scholar] [CrossRef]
- Mink Van Der Molen, A.B.; Matloub, H.S.; Dzwierzynski, W.; Sanger, J.R. The Hand Injury Severity Scoring System and Workers’ Compensation Cases in Wisconsin, USA. J. Hand Surg. 1999, 24, 184–186. [Google Scholar] [CrossRef]
- Wong, J.Y.P. Time Off Work in Hand Injury Patients. J. Hand Surg. 2008, 33, 718–725. [Google Scholar] [CrossRef] [PubMed]
- Matsuzaki, H.; Narisawa, H.; Miwa, H.; Toishi, S. Predicting Functional Recovery and Return to Work After Mutilating Hand Injuries: Usefulness of Campbell’s Hand Injury Severity Score. J. Hand Surg. 2009, 34, 880–885. [Google Scholar] [CrossRef] [PubMed]
- Journeay, W.S.; Pauley, T.; Kowgier, M.; Devlin, M. Return to work after occupational and non-occupational lower extremity amputation. Occup. Med. 2018, 68, 438–443. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.L.; Yin, Y.R.; Chu, C.M.; Tang, P.L. Does category of strength predict return-to-work after occupational injury? BMC Public Health 2022, 22, 1472. [Google Scholar] [CrossRef]
- Lee, Y.Y.; Chang, J.H.; Shieh, S.J.; Lee, Y.C.; Kuo, L.C.; Lee, Y.L. Association between the initial anatomical severity and opportunity of return to work in occupational hand injured patients. J. Trauma 2010, 69, E88–E93. [Google Scholar] [CrossRef]
- von Schroeder, H.P.; Xue, C.; Yak, A.; Gandhi, R. Factors associated with unsuccessful return-to-work following work-related upper extremity injury. Occup. Med. 2020, 70, 434–438. [Google Scholar] [CrossRef]
- Üstün, G.G.; Küçük, K.Y.; Sert, G.; Kara, M.; Uzun, H. Factors Influencing the Time to Return to Work After Occupational Hand Injuries. Acta Med. 2022, 53, 362–366. [Google Scholar] [CrossRef]
- Izadi, N.; Jamshidi, S.; Mehrdad, R.; Nasibi, E. Predictors of return to work in patients with occupational hand injury. Hand Surg. Rehabil. 2020, 39, 218–222. [Google Scholar] [CrossRef]
- Chu, P.-C.; Chin, W.-S.; Guo, Y.L.; Shiao, J.S.-C. Long-term effects of psychological symptoms after occupational injury on return to work: A 6-year follow-up. Int. J. Environ. Res. Public Health 2019, 16, 235. [Google Scholar] [CrossRef]
- Du, C.-L.; Lai, C.-F.; Wang, J.-D. Delayed Return-to-work in Workers After Non-severe Occupational Upper Extremity Fracture in Taiwan. J. Formos. Med. Assoc. 2007, 106, 887–893. [Google Scholar] [CrossRef]
- Shi, Q.; Sinden, K.; MacDermid, J.C.; Walton, D.; Grewal, R. A systematic review of prognostic factors for return to work following work-related traumatic hand injury. J. Hand Ther. 2014, 27, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Bloom, B.; Thomas, S.; Ahrensberg, J.M.; Weaver, R.; Fowler, A.; Bestwick, J.; Harris, T.; Pearse, R. A systematic review and meta-analysis of return to work after mild Traumatic brain injury. Brain Inj. 2018, 32, 1623–1636. [Google Scholar] [CrossRef] [PubMed]
- Ottiger, M.; Poppele, I.; Sperling, N.; Schlesinger, T.; Müller, K. Work ability and return-to-work of patients with post-COVID-19: A systematic review and meta-analysis. BMC Public Health 2024, 24, 1811. [Google Scholar] [CrossRef] [PubMed]
- Beemster, T.T.; van Bennekom, C.A.M.; van Velzen, J.M.; Frings-Dresen, M.H.W.; Reneman, M.F. Vocational rehabilitation with or without work module for patients with chronic musculoskeletal pain and sick leave from work: Longitudinal impact on work participation. J. Occup. Rehabil. 2021, 31, 72–83. [Google Scholar] [CrossRef]
- Pransky, G.S.; Benjamin, K.L.; Savageau, J.A.; Currivan, D.; Fletcher, K. Outcomes in work-related injuries: A comparison of older and younger workers. Am. J. Ind. Med. 2005, 47, 104–112. [Google Scholar] [CrossRef]
- Savitsky, B.; Radomislensky, I.; Goldman, S.; Gitelson, N.; Frid, Z.; Peleg, K. Socio-economic disparities and returning to work following an injury. Isr. J. Health Policy Res. 2020, 9, 35. [Google Scholar] [CrossRef]
- Etuknwa, A.; Daniels, K.; Eib, C. Sustainable Return to Work: A Systematic Review Focusing on Personal and Social Factors. J. Occup. Rehabil. 2019, 29, 679–700. [Google Scholar] [CrossRef]
- De Rijk, A.; Nijhuis, F.; Alexanderson, K. Gender Differences in Work Modifications and Changed Job Characteristics During the Return-To-Work Process: A Prospective Cohort Study. J. Occup. Rehabil. 2009, 19, 185–193. [Google Scholar] [CrossRef]
- Panisoara, G.; Serban, M. Marital Status and Work-Life Balance. Procedia Soc. Behav. Sci. 2013, 78, 21–25. [Google Scholar] [CrossRef]
- Skagseth, M.; Fimland, M.; Rise, M.; Nilsen, T.; Aasdahl, L. Return-to-work self-efficacy after occupational rehabilitation for musculoskeletal and common mental health disorders: Secondary outcomes of a randomized clinical trial. J. Rehabil. Med. 2021, 53, jrm00146. [Google Scholar] [CrossRef]
- Matos, J.; Henriques, A.; Moura, A.; Alves, E. Professional reintegration of stroke survivors and their mental health, quality of life and community integration. Qual. Life Res. 2024, 33, 3259–3273. [Google Scholar] [CrossRef]
- Brenneman, F.D.; Redelmeier, D.A.; Boulanger, B.R.; McLellan, B.A.; Culhane, J.P. Long-term Outcomes in Blunt Trauma: Who Goes Back to Work? J. Trauma Acute Care Surg. 1997, 42, 778–781. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).