
Review of Mix-and-Match Approach and Binocular Intraocular Lens Systems




Abstract
1. Introduction
2. Literature Search
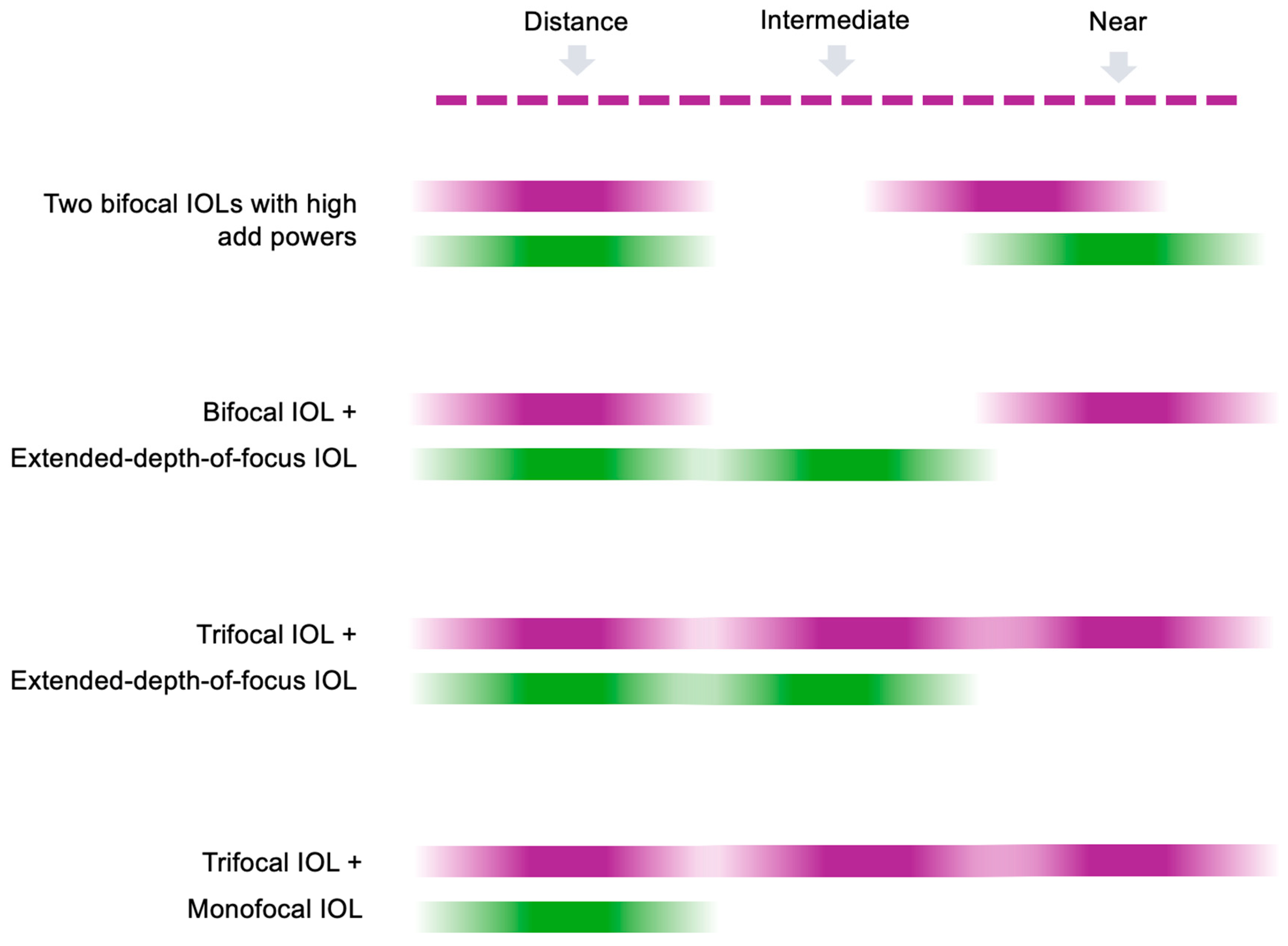
3. Mix-and-Match Approach
3.1. Combination of Two Bifocal IOLs with High Add Powers
3.2. Combination of Bifocal IOL with Extended-Depth-of-Focus IOL
3.3. Combination of Trifocal IOL with Extended-Depth-of-Focus or Monofocal IOL
3.4. Mix-and-Match Strategies in Complex Cases
4. Binocular IOL Systems
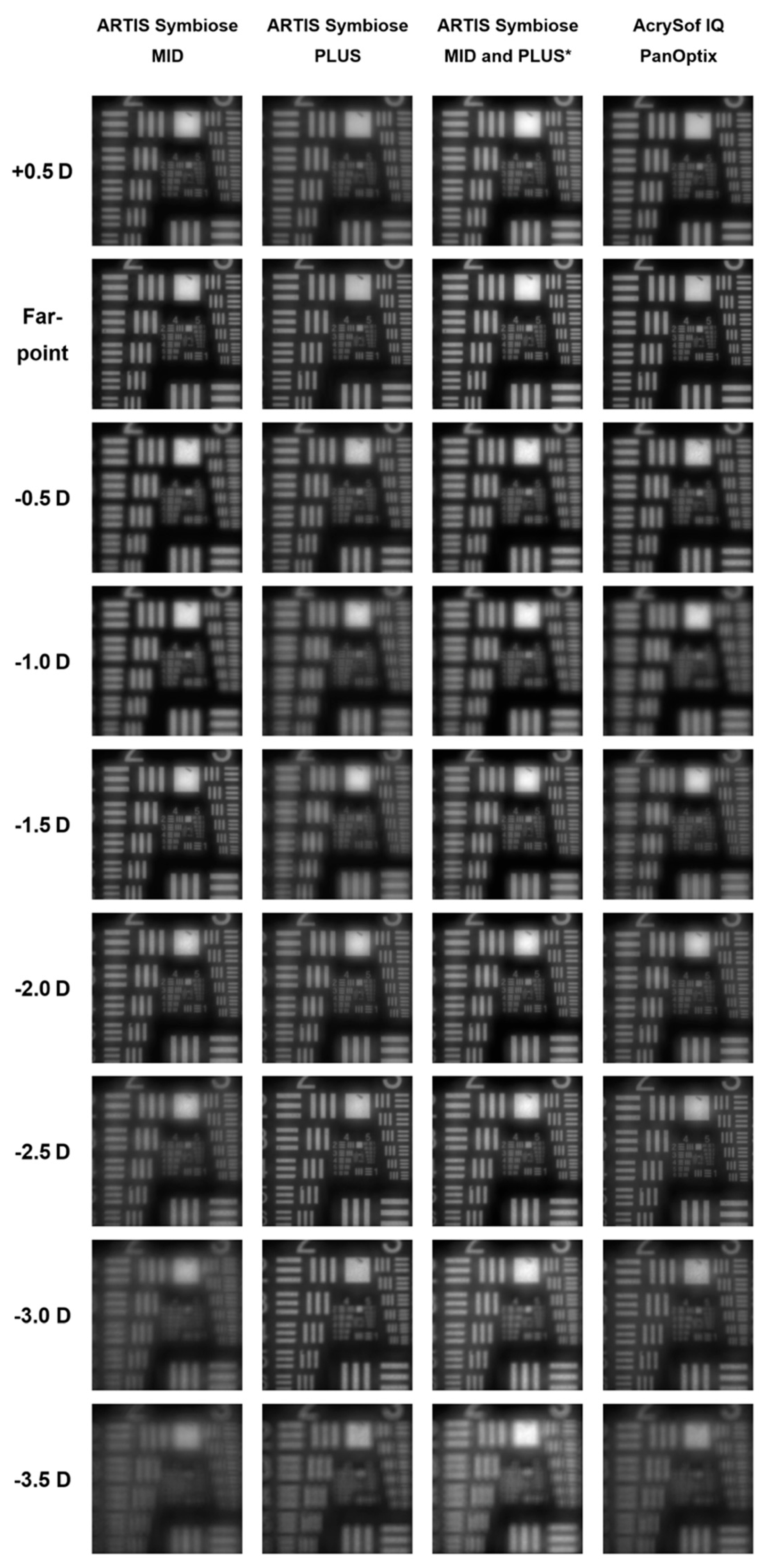
4.1. Artis Symbiose
4.2. WELL Fusion
5. Considerations When Implanting Two Different IOL Models
5.1. Tolerance to Differences in Visual Impression Between the Eyes
5.2. Differences in Contrast Perception
5.3. Stereopsis
5.4. Binocular Summation
5.5. Practical Considerations
5.6. Directions for Future Research
6. Conclusions
Funding
Conflicts of Interest
References
- Naujokaitis, T.; Auffarth, G.U.; Khoramnia, R.; Łabuz, G. Complementary system vs conventional trifocal intraocular lens: Comparison of optical quality metrics and unwanted light distribution. J. Cataract. Refract. Surg. 2023, 49, 84–90. [Google Scholar] [CrossRef] [PubMed]
- McNeely, R.N.; Stewart, S.A.; Moore, J.E. Visual performance and subjective experience 3 months and 12 months after combined implantation of 2 new complementary continuous phase multifocal intraocular lenses. J. Cataract. Refract. Surg. 2023, 49, 921–928. [Google Scholar] [CrossRef] [PubMed]
- Khoramnia, R.; Naujokaitis, T.; Łabuz, G.; Auffarth, G.U. Complex optical systems for individualized correction of presbyopia. Ophthalmologie 2024, 121, 706–713. (In German) [Google Scholar] [CrossRef]
- Jiang, Y.; Bu, S.; Tian, F.; Liang, J.; Wang, T.; Xing, X.; Zhang, H.; Zhang, X. Long-Term Clinical Outcomes after Mix and Match Implantation of Two Multifocal Intraocular Lenses with Different Adds. J. Ophthalmol. 2019, 2019, 6789263. [Google Scholar] [CrossRef]
- Liu, D.; Li, H.; Zheng, S.; Sun, J.; Bai, H.; Wu, X. Comparison of Visual Performance Between Mix-and-Match and Bilateral Implantation of Rotationally Asymmetric Multifocal Intraocular Lenses. Clin. Ophthalmol. 2024, 18, 3289–3295. [Google Scholar] [CrossRef]
- Lee, J.H.; Lee, H.; Lee, J.A.; Yoo, A.; Kim, J.Y.; Tchah, H. Clinical outcomes after mix-and-match implantation of diffractive multifocal intraocular lenses with +2.75 and +4.00 diopter add powers. BMC Ophthalmol. 2020, 20, 193. [Google Scholar] [CrossRef] [PubMed]
- Paik, D.W.; Park, J.S.; Yang, C.M.; Lim, D.H.; Chung, T.Y. Comparing the visual outcome, visual quality, and satisfaction among three types of multi-focal intraocular lenses. Sci. Rep. 2020, 10, 14832. [Google Scholar] [CrossRef]
- Goldberg, D.G.; Goldberg, M.H.; Shah, R.; Meagher, J.N.; Ailani, H. Pseudophakic mini-monovision: High patient satisfaction, reduced spectacle dependence, and low cost. BMC Ophthalmol. 2018, 18, 293. [Google Scholar] [CrossRef]
- Ito, M.; Shimizu, K.; Amano, R.; Handa, T. Assessment of visual performance in pseudophakic monovision. J. Cataract. Refract. Surg. 2009, 35, 710–714. [Google Scholar] [CrossRef]
- Yesilirmak, N.; Akova, Y.A.; Donmez, O. Comparison of Mix-and-Match Implanted Bifocal IOLs and Bilateral Implanted Trifocal IOLs After Femtosecond Laser-Assisted Cataract Surgery. J. Refract. Surg. 2019, 35, 559–564. [Google Scholar] [CrossRef]
- Bilbao-Calabuig, R.; González-López, F.; Amparo, F.; Alvarez, G.; Patel, S.R.; Llovet-Osuna, F. Comparison Between Mix-and-Match Implantation of Bifocal Intraocular Lenses and Bilateral Implantation of Trifocal Intraocular Lenses. J. Refract. Surg. 2016, 32, 659–663. [Google Scholar] [CrossRef] [PubMed]
- Xiong, T.; Chen, H.; Fan, W. Comparison of bilateral implantation of an extended depth of focus lenses and a blend approach of extended depth of focus lenses and bifocal lenses in cataract patients. BMC Ophthalmol. 2023, 23, 476. [Google Scholar] [CrossRef] [PubMed]
- Lee, J.H.; Chung, H.S.; Moon, S.Y.; Park, S.Y.; Lee, H.; Kim, J.Y.; Tchah, H. Clinical Outcomes after Mix-and-Match Implantation of Extended Depth of Focus and Diffractive Multifocal Intraocular Lenses. J. Ophthalmol. 2021, 2021, 8881794. [Google Scholar] [CrossRef] [PubMed]
- Koo, O.S.; Kang, J.W.; Park, J.K.; Kim, K.H. Visual performance and patient satisfaction after implantation of extended range-of-vision IOLs: Bilateral implantation vs 2 different mix-and-match approaches. J. Cataract. Refract. Surg. 2021, 47, 192–197. [Google Scholar] [CrossRef]
- Kim, S.; Yi, R.; Chung, S.H. Comparative Analysis of the Clinical Outcomes of Mix-and-Match Implantation of an Extended Depth-of-Focus and a Diffractive Bifocal Intraocular Lens. Eye Contact Lens. 2022, 48, 261–266. [Google Scholar] [CrossRef]
- Breyer, D.R.H.; Kaymak, H.; Ax, T.; Kretz, F.T.A.; Auffarth, G.U.; Hagen, P.R. Multifocal Intraocular Lenses and Extended Depth of Focus Intraocular Lenses. Asia Pac. J. Ophthalmol. 2017, 6, 339–349. [Google Scholar]
- Kanclerz, P.; Toto, F.; Grzybowski, A.; Alio, J.L. Extended Depth-of-Field Intraocular Lenses: An Update. Asia Pac. J. Ophthalmol. 2020, 9, 194–202. [Google Scholar] [CrossRef]
- Kohnen, T.; Suryakumar, R. Extended depth-of-focus technology in intraocular lenses. J. Cataract. Refract. Surg. 2020, 46, 298–304. [Google Scholar] [CrossRef]
- Rampat, R.; Gatinel, D. Multifocal and Extended Depth-of-Focus Intraocular Lenses in 2020. Ophthalmology 2021, 128, e164–e185. [Google Scholar] [CrossRef]
- de Medeiros, A.L.; de Araújo Rolim, A.G.; Motta, A.F.P.; Ventura, B.V.; Vilar, C.; Chaves, M.; Carricondo, P.C.; Hida, W.T. Comparison of visual outcomes after bilateral implantation of a diffractive trifocal intraocular lens and blended implantation of an extended depth of focus intraocular lens with a diffractive bifocal intraocular lens. Clin. Ophthalmol. 2017, 11, 1911–1916. [Google Scholar] [CrossRef]
- Song, J.E.; Khoramnia, R.; Son, H.S.; Knorz, M.C.; Choi, C.Y. Comparison Between Bilateral Implantation of a Trifocal IOL and Mix-and-Match Implantation of a Bifocal IOL and an Extended Depth of Focus IOL. J. Refract. Surg. 2020, 36, 528–535. [Google Scholar] [CrossRef] [PubMed]
- Acar, B.; Nurozler Tabakci, B. Clinical outcome comparison: Bilateral trifocal vs. mix-match extended depth of focus and trifocal intraocular lenses. Int. Ophthalmol. 2021, 41, 3675–3686. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.W.; Eom, Y.; Park, W.; Song, J.S.; Jeong, J.W.; Park, S.K.; Kim, H.M. Comparison of visual outcomes after two types of mix-and-match implanted trifocal extended-depth-of-focus and trifocal intraocular lenses. Graefes Arch. Clin. Exp. Ophthalmol. 2022, 260, 3275–3283. [Google Scholar] [CrossRef]
- Kim, B.; Son, H.S.; Khoramnia, R.; Auffarth, G.U.; Choi, C.Y. Comparison of clinical outcomes between different combinations of hybrid multifocal, extended-depth-of-focus and enhanced monofocal intraocular lenses. Br. J. Ophthalmol. 2024, 109, 565–571. [Google Scholar] [CrossRef] [PubMed]
- Tarib, I.; Kasier, I.; Herbers, C.; Hagen, P.; Breyer, D.; Kaymak, H.; Klabe, K.; Lucchesi, R.; Teisch, S.; Diakonis, V.F.; et al. Comparison of Visual Outcomes and Patient Satisfaction After Bilateral Implantation of an EDOF IOL and a Mix-and-Match Approach. J. Refract. Surg. 2019, 35, 408–416. [Google Scholar] [CrossRef]
- Danzinger, V.; Schartmüller, D.; Schwarzenbacher, L.; Röggla, V.; Abela-Formanek, C.; Menapace, R.; Leydolt, C. Clinical prospective intra-individual comparison after mix-and-match implantation of a monofocal EDOF and a diffractive trifocal IOL. Eye 2024, 38, 321–327. [Google Scholar] [CrossRef]
- Ke, S.; Wan, W.; Li, C. Comparisons of visual outcomes between bilateral implantation and mix-and-match implantation of three types intraocular lenses. Int. Ophthalmol. 2023, 43, 1143–1152. [Google Scholar] [CrossRef]
- Baur, I.D.; Auffarth, G.U.; Łabuz, G.; Mayer, C.S.; Khoramnia, R. Presbyopia correction after previous Intracor treatment: Combined implantation of a small-aperture and a non-diffractive extended-depth-of-focus lens. Am. J. Ophthalmol. Case Rep. 2022, 25, 101398. [Google Scholar] [CrossRef]
- Sánchez-González, J.M.; Sánchez-González, M.C.; De-Hita-Cantalejo, C.; Ballesteros-Sánchez, A. Small Aperture IC-8 Extended-Depth-of-Focus Intraocular Lens in Cataract Surgery: A Systematic Review. J. Clin. Med. 2022, 11, 4654. [Google Scholar] [CrossRef]
- Ang, R.E. Visual Performance of a Small-Aperture Intraocular Lens: First Comparison of Results After Contralateral and Bilateral Implantation. J. Refract. Surg. 2020, 36, 12–19. [Google Scholar] [CrossRef]
- Son, H.S.; Khoramnia, R.; Yildirim, T.M.; Baur, I.; Labuz, G.; Auffarth, G.U. Functional Outcomes and Reading Performance After Combined Implantation of a Small-Aperture Lens and a Segmental Refractive Bifocal Lens. J. Refract. Surg. 2019, 35, 551–558. [Google Scholar] [CrossRef] [PubMed]
- Lajara-Blesa, J.; Rodríguez-Izquierdo, M.; Vallés-San-Leandro, L.; Jutley, G.; de Los Remedios Ortega-García, M.; Zapata-Díaz, J.F. Standard Clinical Outcomes, Light Distortion, Stereopsis, and a Quality-of-Life Assessment of a New Binocular System of Complementary IOLs. J. Refract. Surg. 2023, 39, 654–661. [Google Scholar] [CrossRef] [PubMed]
- Zapata-Díaz, J.F.; Rodríguez-Izquierdo, M.A.; Ould-Amer, N.; Lajara-Blesa, J.; López-Gil, N. Total Depth of Focus of Five Premium Multifocal Intraocular Lenses. J. Refract. Surg. 2020, 36, 578–584. [Google Scholar] [CrossRef]
- Ivellio-Vellin, H.; Ruiss, M.; Hienert, J.; Georgiev, S.; Pilwachs, C.; Fisus, A.; Findl, O. Clinical outcomes after implantation of a novel binocular complementary extended depth of focus intraocular lens compared to bilateral low near-add multifocal intraocular lenses. Ophthalmic Res. 2024, 67, 549–557. [Google Scholar] [CrossRef]
- Mastropasqua, L.; Pedrotti, E.; Ruggeri, M.L.; Vecchiarino, L.; Bonacci, E.; Guarini, D.; Falconio, G.; Toto, L.M.; Marchini, G.M. Two-surgeon, two-center evaluation of a new combined EDOF intraocular lens approach. J. Cataract. Refract. Surg. 2023, 49, 512–517. [Google Scholar] [CrossRef] [PubMed]
- Greenbaum, S. Monovision pseudophakia. J. Cataract. Refract. Surg. 2002, 28, 1439–1443. [Google Scholar] [CrossRef]
- Hayashi, K.; Ogawa, S.; Manabe, S.; Yoshimura, K. Binocular visual function of modified pseudophakic monovision. Am. J. Ophthalmol. 2015, 159, 232–240. [Google Scholar] [CrossRef]
- Khoramnia, R.; Naujokaitis, T. Patient selection for multifocal intraocular lenses. Klin. Monbl. Augenheilkd. 2025; epub ahead of print. (In German). [Google Scholar] [CrossRef]
- Legge, G.E.; Rubin, G.S. Binocular interactions in suprathreshold contrast perception. Percept. Psychophys. 1981, 30, 49–61. [Google Scholar] [CrossRef]
- Bohac, M.; Jagic, M.; Biscevic, A.; Lukacevic, S.; Mravicic, I.; Suic, S.P.; Dekaris, I. Stereoacuity and Multifocal Intraocular Lenses—A Systematic Review. Acta Inform. Medica 2023, 31, 62–67. [Google Scholar] [CrossRef]
- Evans, B.J. Monovision: A review. Ophthalmic Physiol. Opt. 2007, 27, 417–439. [Google Scholar] [CrossRef]
- Tsaousis, K.T.; Plainis, S.; Dimitrakos, S.A.; Tsinopoulos, I.T. Binocularity enhances visual acuity of eyes implanted with multifocal intraocular lenses. J. Refract. Surg. 2013, 29, 246–250. [Google Scholar] [CrossRef] [PubMed]
- Cagenello, R.; Arditi, A.; Halpern, D.L. Binocular enhancement of visual acuity. J. Opt. Soc. Am. A Opt. Image Sci. Vis. 1993, 10, 1841–1848. [Google Scholar] [CrossRef] [PubMed]
- Plainis, S.; Petratou, D.; Giannakopoulou, T.; Atchison, D.A.; Tsilimbaris, M.K. Binocular summation improves performance to defocus-induced blur. Investig. Ophthalmol. Vis. Sci. 2011, 52, 2784–2789. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
| Study (Year of Publication) | Number of Patients | Binocular Visual Acuity | Binocular Defocus Curve | Spectacle Independence | Photic Phenomena |
|---|---|---|---|---|---|
| Artis Symbiose | |||||
| Lajara-Blesa et al. (2023) [32] | 23 (6-month data) | 6 months post-surgery: median (interquartile range) UDVA −0.10 (0.10) logMAR; Mean ± standard deviation CDVA −0.11 ± 0.10 logMAR; UIVA (90 cm) −0.03 ± 0.20 logMAR; DCIVA (90 cm) 0.05 ± 0.12 logMAR; UIVA (70 cm) 0.03 ± 0.11 logMAR; DCIVA (70 cm) 0.00 ± 0.09 logMAR; UNVA 0.06 ± 0.10 logMAR; DCNVA 0.04 ± 0.09 logMAR | 0.20 logMAR and better between −3.0 D and +1.0 D; 0.10 logMAR and better −3.0 D and +0.5 D | Not reported | Light Distortion Analyzer: Monocular MID lens: 12.57 (6.61) %, Monocular PLUS lens: 14.99 ± 5.70%, Binocular: 10.36 ± 4.42% |
| McNeely et al. (2023) [2] | 44 | 12 months post-surgery: UDVA −0.07 ± 0.06 logMAR UIVA 0.03 ± 0.10 logMAR UNVA 0.07 ± 0.08 logMAR | 0.20 logMAR and better between −3.0 D and +1.0 D; 0.10 logMAR and better −2.5 D and +0.5 D | 93.2% complete spectacle independence | Halo: 0.36 ± 0.53 (scale 0 to 3) Glare: 0.39 ± 0.62 (scale 0 to 3) |
| Ivellio-Vellin et al. (2024) [34] | 14 initially included in the Artis Symbiose group (28 patients in total), 11 excluded or lost to follow-up | 6 months post-surgery median (mean, range): UDVA 0.0 (0.0, −0.1 to 0.0) logMAR; CDVA −0.1 (−0.1, −0.1 to 0.0) logMAR; UIVA 0.1 (0.1, −0.1 to 0.3) logMAR; DCIVA 0.1 (0.1, −0.1 to 0.3) logMAR; UNVA 0.1 (0.1, 0.0 to 0.4) logMAR; DCNVA 0.1 (0.1, 0.0 to 0.5) logMAR | 0.20 logMAR and better between −2.0 D and +1.0 D; 0.10 logMAR and better −1.25 D and +0.5 D | Not reported | Binocular halo size: approx. 1.0° |
| WELL Fusion | |||||
| Mastropasqua et al. (2023) [35] | 30 | 3 months post-surgery: UDVA 0.03 ± 0.11 logMAR; CDVA −0.02 ± 0.08 logMAR; UIVA 0.05 ± 0.10 logMAR; DCIVA 0.06 ± 0.09 logMAR; UNVA (40 cm) −0.03 ± 0.08 logMAR; DCNVA (40 cm) −0.05 ± 0.05 logMAR; UNVA (33 cm) 0.06 ± 0.08 logMAR; DCNVA (33 cm) 0.05 ± 0.06 logMAR | 0.20 logMAR and better between −3.5 D and +1.0 D; 0.10 logMAR and better −2.5 D and +0.5 D | National Eye Institute Refractive Error Quality-of-Life instrument-42 Dependence on correction: approx. 90–93 out of 100 | National Eye Institute Refractive Error Quality-of-Life instrument-42 Glare: approx. 70–76 out of 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Naujokaitis, T.; Łabuz, G.; Khoramnia, R.; Auffarth, G.U. Review of Mix-and-Match Approach and Binocular Intraocular Lens Systems. J. Clin. Med. 2025, 14, 4263. https://doi.org/10.3390/jcm14124263
Naujokaitis T, Łabuz G, Khoramnia R, Auffarth GU. Review of Mix-and-Match Approach and Binocular Intraocular Lens Systems. Journal of Clinical Medicine. 2025; 14(12):4263. https://doi.org/10.3390/jcm14124263
Chicago/Turabian StyleNaujokaitis, Tadas, Grzegorz Łabuz, Ramin Khoramnia, and Gerd U. Auffarth. 2025. "Review of Mix-and-Match Approach and Binocular Intraocular Lens Systems" Journal of Clinical Medicine 14, no. 12: 4263. https://doi.org/10.3390/jcm14124263
APA StyleNaujokaitis, T., Łabuz, G., Khoramnia, R., & Auffarth, G. U. (2025). Review of Mix-and-Match Approach and Binocular Intraocular Lens Systems. Journal of Clinical Medicine, 14(12), 4263. https://doi.org/10.3390/jcm14124263