
Morphological Variability and Clinical Significance of the Fibularis Tertius Muscle: An Extensive Literature Review
 ,
,  ,
,  and
and
Abstract
1. Introduction
2. Methods and Review Design
- -
- Manuscripts written in any language other than English.
- -
- Insufficient information regarding the description of the study.
- -
- Types of articles that include expert opinions, letters to the editor or conference reports.
- -
- Publications dated after August 2024.
3. Results and Discussion
3.1. The Fibularis Tertius (FT) Typical Descriptive and Functional Anatomy
3.1.1. Typical Descriptive Anatomy
3.1.2. Functional Anatomy
3.2. Reported Variants of the Fibularis Tertius (FT)
3.2.1. Prevalence of the FT Presence
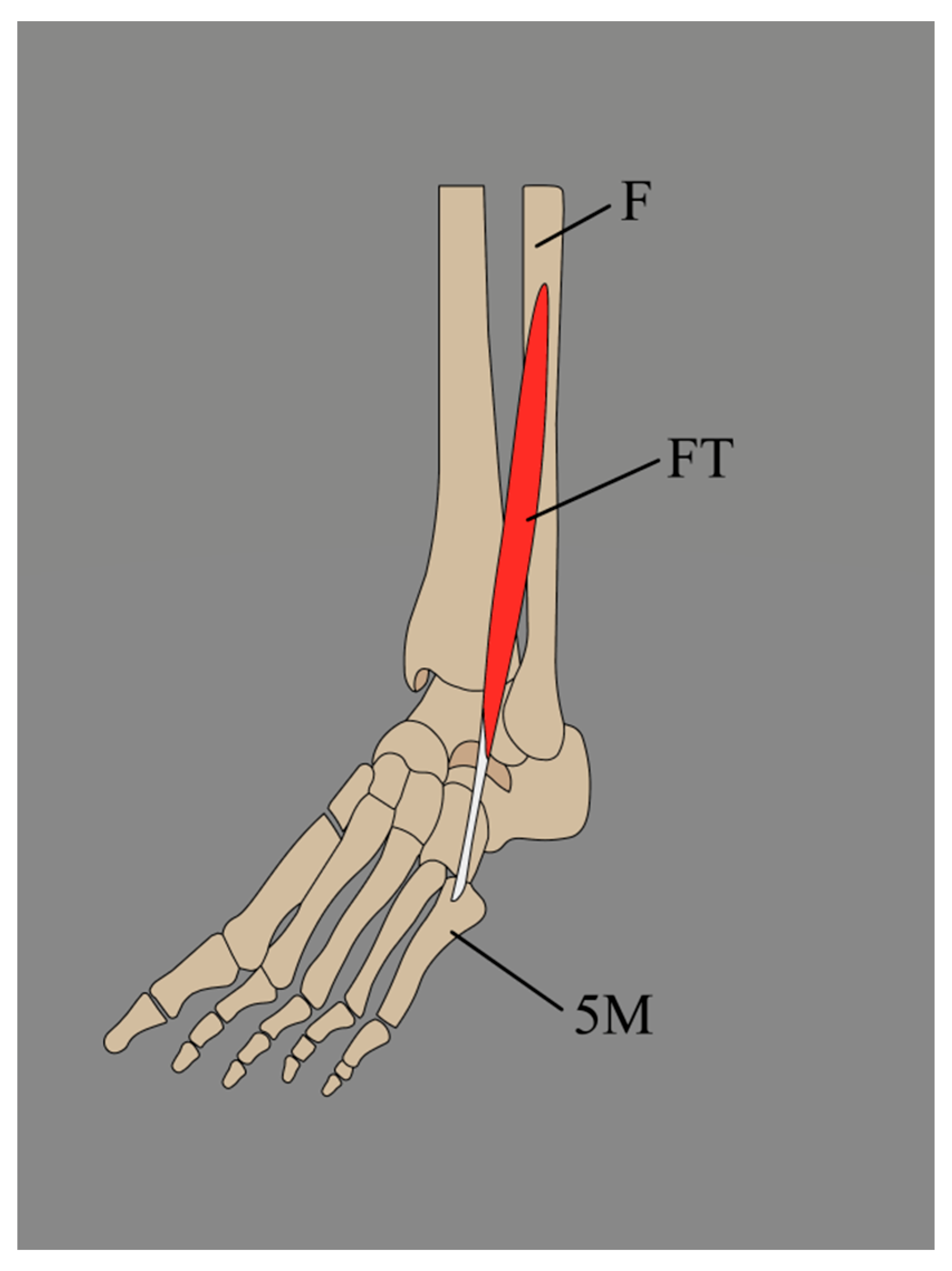
3.2.2. Variations in the Origin of the Fibularis Tertius (FT)
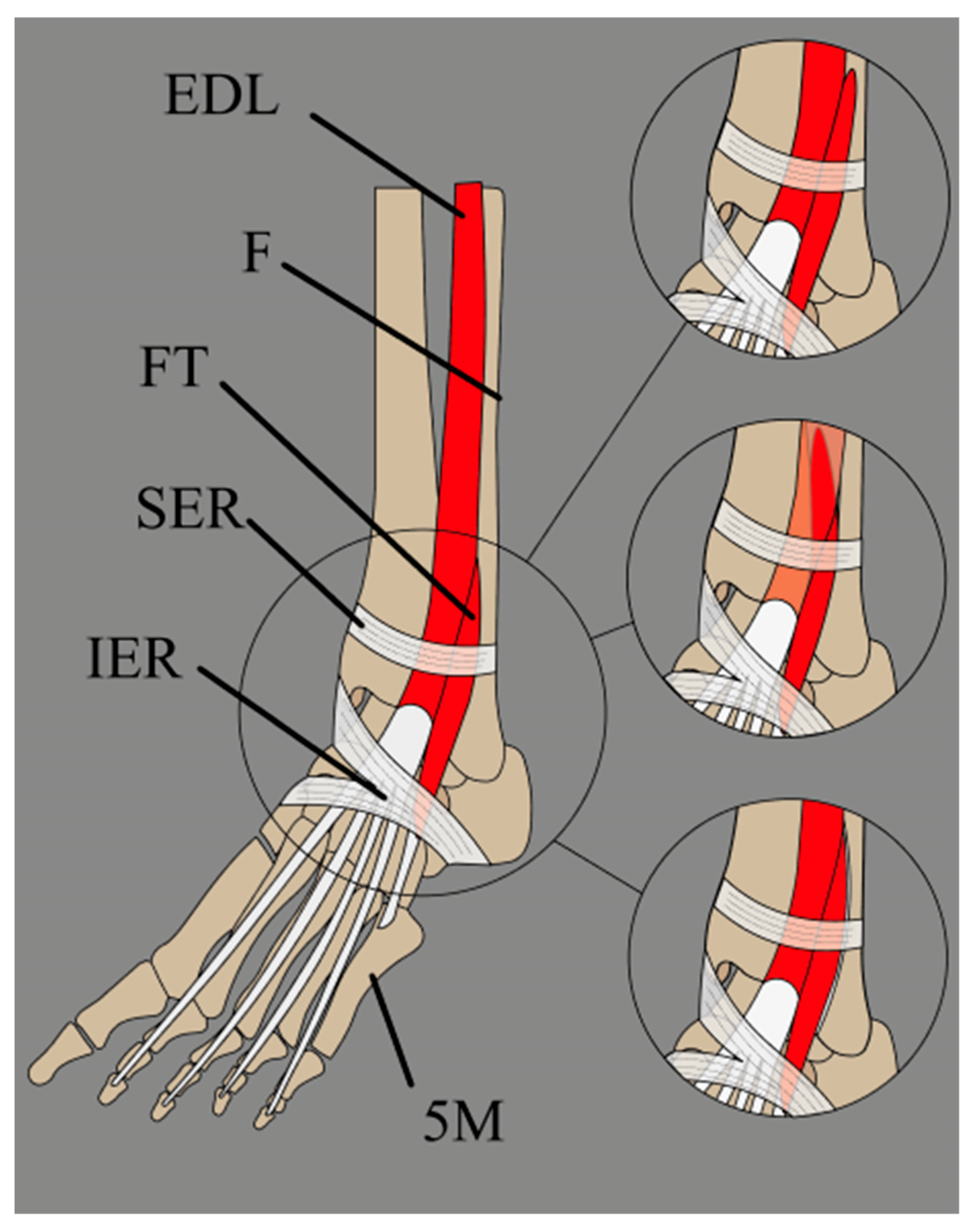
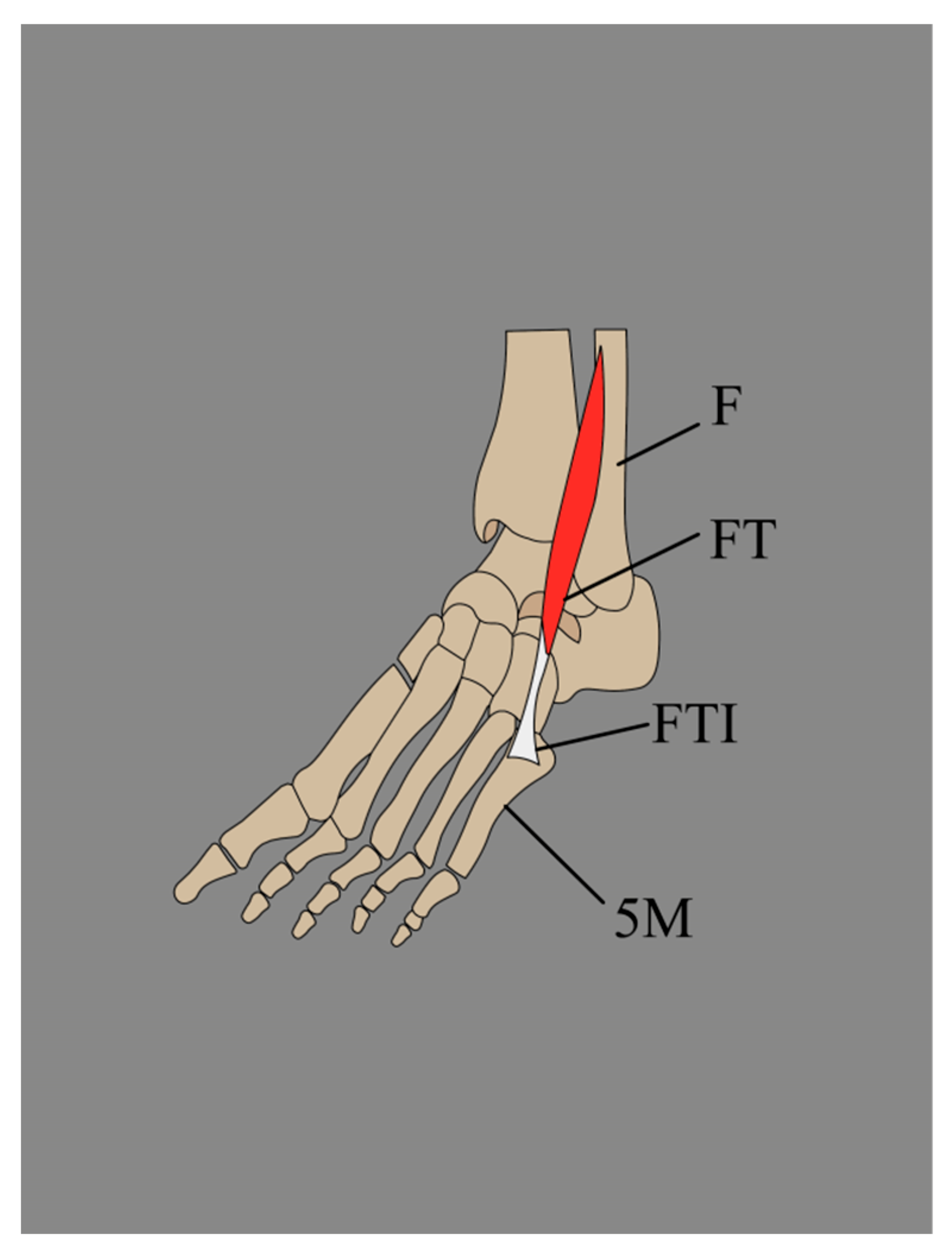
3.2.3. Variations in the Insertion of the Fibularis Tertius (FT)
- A single tendon, band-shaped, inserted into the shaft of the fifth metatarsal bone (45%).
- A single tendon, fan-shaped, inserted at the base of the fifth metatarsal bone (22%).
- A single tendon, fan-shaped, inserted into the fascia covering the fourth interosseous space and the base and shaft of the sixth metatarsal bone (16.5%).
- A bifurcated tendon consisting of both band and fan shapes. The main fan-shaped tendon is inserted at the base of the fifth metatarsal bone, while the accessory tendon is attached to its shaft (8.8%).
- A bifurcated tendon, fan-shaped, where the main tendon is inserted at the base of the fifth metatarsal bone, and the secondary tendon attaches to the base of the fourth metatarsal bone (5.5%).
- This tendon fuses with an additional band from the FB, which gives rise to the fourth interosseous dorsalis muscle (2.2%).
3.2.4. Fibularis Tertius Tendon (FTT) Morphology
3.2.5. FT Accessory Forms
4. Embryological Development and Occurrence Among Other Species
4.1. Evolution and Prevalence Among Other Species
4.2. Embryological Development Among Humans
4.3. Prevalence of the FT Among Fetuses
4.4. Variation of the FT Origin Among Fetuses
4.5. Variation of the FT Insertion Among Fetuses
4.6. Fibularis Tertius Tendon (FTT) Morphology in Fetuses
4.7. Accessory Forms of FT in Fetuses
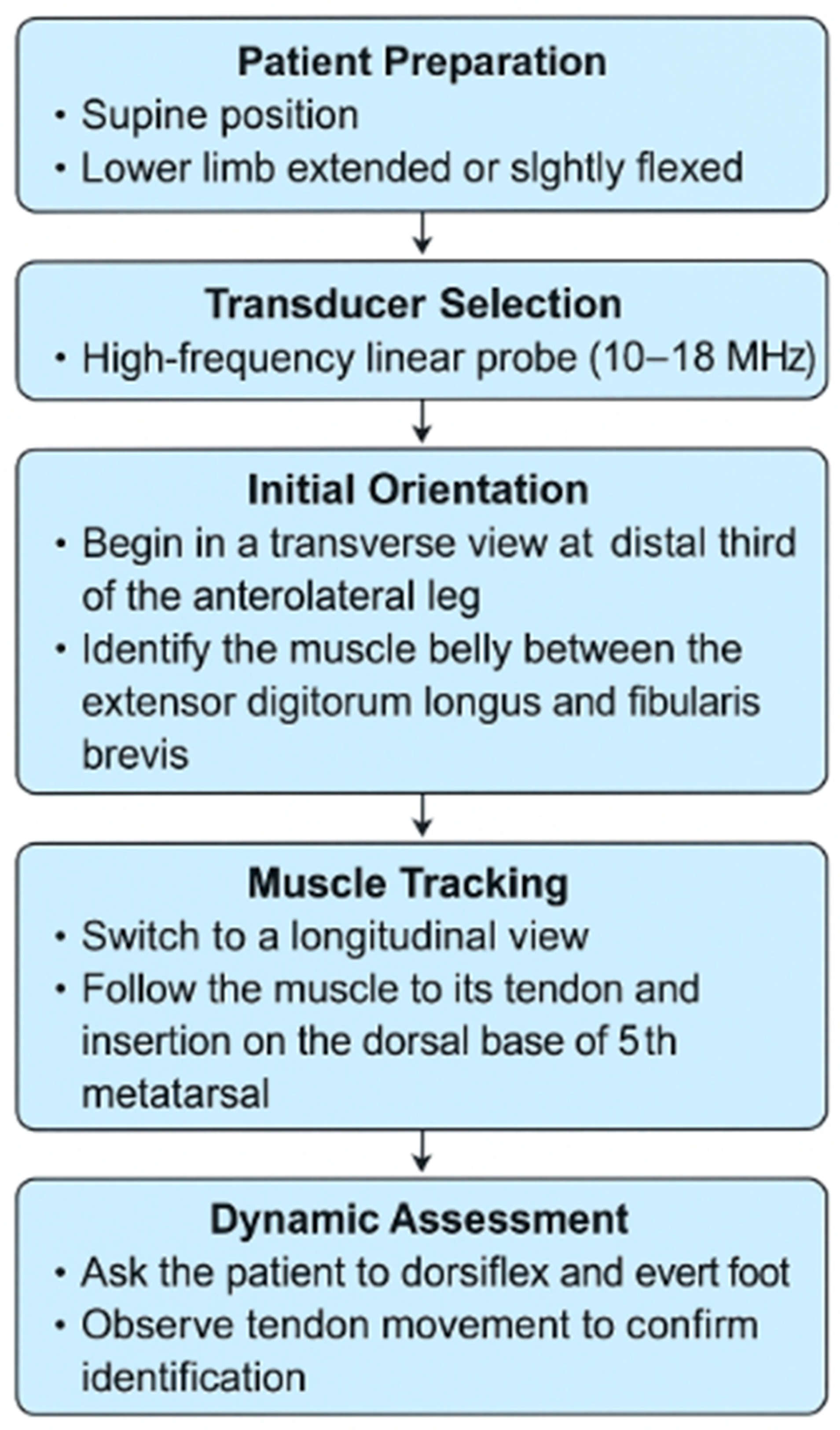
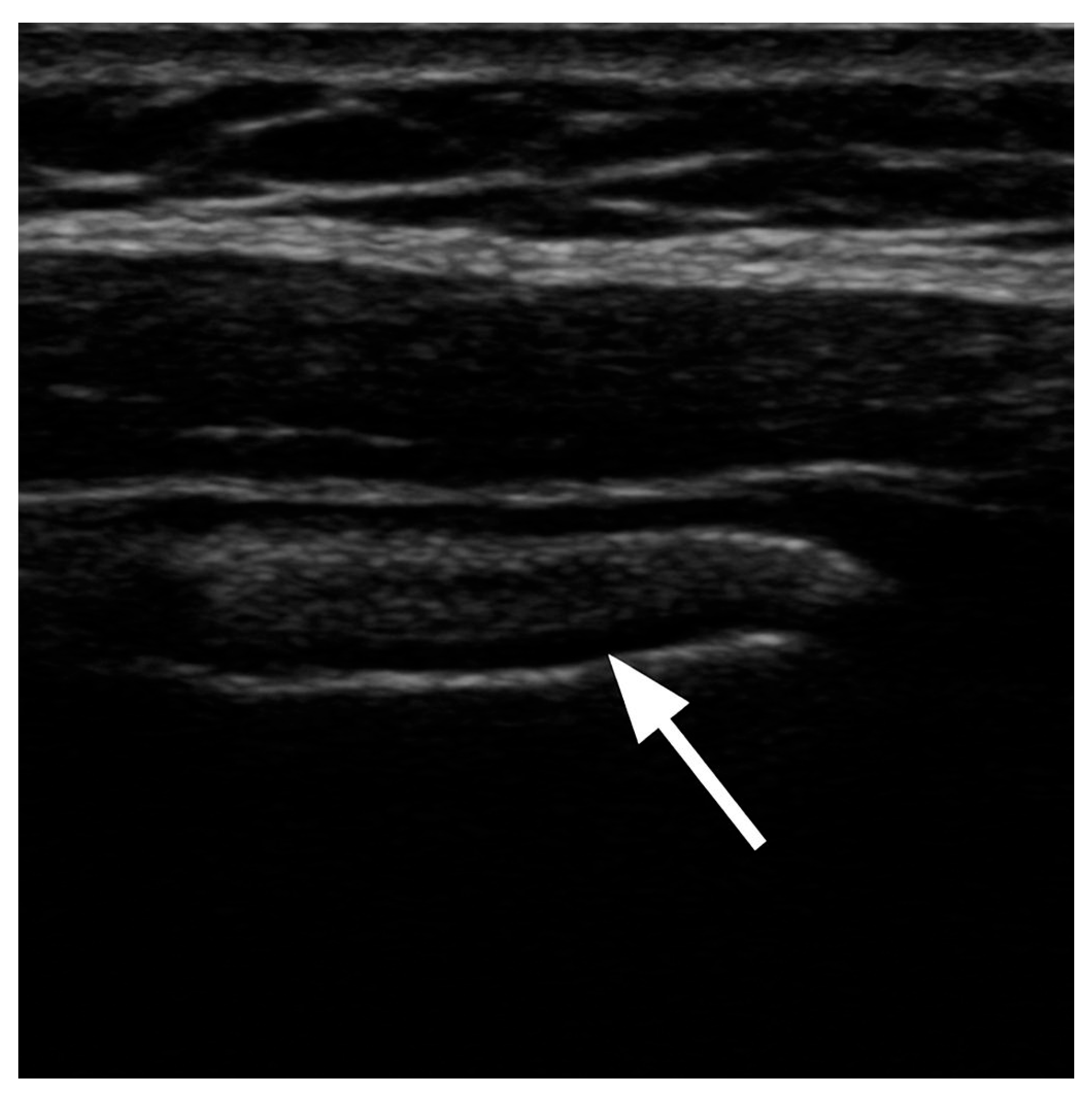
5. Visualization and Imaging Studies
6. Clinical Significance—Pathological Background
6.1. Fibularis Tertius or Peroneus Tertius Syndrome (FTS or PTS)
6.2. Fibularis Tendon Tertius (FTT) Tear
6.3. Intra-Tendinous Ganglion Cyst
7. Clinical Application
7.1. Ankle Arthroscopy and FTT
7.2. Local Muscle Flap Transposition
7.3. Equinovarus Deformity
7.4. Lateral Ankle Stabilization
8. Conclusions
Funding
Conflicts of Interest
References
- Moore, K.; Dalley, A.F.; Agur, A.M.R. Clinically Oriented Anatomy, 7th ed.; Wilkins, Lippincott Williams and Wilkins: Philadelphia, PA, USA, 2014. [Google Scholar]
- Pośnik, M.; Zielinska, N.; Tubbs, R.S.; Ruzik, K.; Olewnik, Ł. Morphological Variability of the Leg Muscles: Potential Traps on Ultrasound That Await Clinicians. Folia Morphol. 2023, 83, 275–293. [Google Scholar] [CrossRef] [PubMed]
- Lambert, H.W. Leg Muscles. In Bergman’s Comprehensive Encyclopedia of Human Anatomic Variation; Wiley: Hoboken, NJ, USA, 2016; pp. 421–437. [Google Scholar] [CrossRef]
- Standring, S. Gray’s Anatomy, 41st ed.; Elsevier Churchill Livingstone: Edinburgh, UK, 2016. [Google Scholar]
- Jungers, W.L.; Meldrum, D.J.; Stern, J.T. The Functional and Evolutionary Significance of the Human Peroneus Tertius Muscle. J. Hum. Evol. 1993, 25, 377–386. [Google Scholar] [CrossRef]
- Rourke, K.; Dafydd, H.; Parkin, I.G. Fibularis Tertius: Revisiting the Anatomy. Clin. Anat. 2007, 20, 946–949. [Google Scholar] [CrossRef] [PubMed]
- Yammine, K.; Erić, M. The Fibularis (Peroneus) Tertius Muscle in Humans: A Meta-Analysis of Anatomical Studies with Clinical and Evolutionary Implications. Biomed. Res. Int. 2017, 2017, 6021707. [Google Scholar] [CrossRef] [PubMed]
- Witvrouw, E.; Borre, K.V.; Willems, T.M.; Huysmans, J.; Broos, E.; De Clercq, D. The significance of peroneus tertius muscle in ankle injuries: A prospective study. Am. J. Sports Med. 2006, 34, 1159–1163. [Google Scholar] [CrossRef]
- Kimura, K.; Takahashi, Y. The Peroneus Tertius Muscle in the Crab-Eating Monkey. Okajimas Folia Anat. Jpn. 1985, 62, 173–185. [Google Scholar] [CrossRef]
- Yammine, K. The Accessory Peroneal (Fibular) Muscles: Peroneus Quartus and Peroneus Digiti Quinti. A Systematic Review and Meta-Analysis. Surg. Radiol. Anat. 2015, 37, 617–627. [Google Scholar] [CrossRef]
- Palomo-López, P.; Losa-Iglesias, M.E.; Calvo-Lobo, C.; Rodríguez-Sanz, D.; Navarro-Flores, E.; Becerro-de-Bengoa-Vallejo, R.; López-López, D. Fibularis Tertius Muscle in Women & Men: A Surface Anatomy Cross-Sectional Study across Countries. PLoS ONE 2019, 14, e0215118. [Google Scholar] [CrossRef]
- Eliot, D.J.; Jungers, W.L. Fifth Metatarsal Morphology Does Not Predict Presence or Absence of Fibularis Tertius Muscle in Hominids. J. Hum. Evol. 2000, 38, 333–342. [Google Scholar] [CrossRef]
- Jana, R.; Roy, T.S. Variant Insertion of the Fibularis Tertius Muscle Is an Evidence of the Progressive Evolutionary Adaptation for the Bipedal Gait. Clin. Pract. 2011, 1, e81. [Google Scholar] [CrossRef]
- Lambert, H.W.; Atsas, S. An Anterior Fibulocalcaneus Muscle: An Anomalous Muscle Discovered in the Anterior Compartment of the Leg. Clin. Anat. 2010, 23, 911–914. [Google Scholar] [CrossRef]
- Olewnik, Ł. Fibularis Tertius: Anatomical Study and Review of the Literature. Clin. Anat. 2019, 32, 1082–1093. [Google Scholar] [CrossRef]
- Bejjani, F.J.; Jahss, M.H. Le Double’s Study of Muscle Variations of the Human Body Part I: Muscle Variations of the Leg. Foot Ankle Int. 1985, 6, 111–134. [Google Scholar] [CrossRef]
- Olewnik, Ł.; Gonera, B.; Podgórski, M.; Polguj, M.; Jezierski, H.; Topol, M. A Proposal for a New Classification of Pes Anserinus Morphology. Knee Surg. Sports Traumatol. Arthrosc. 2019, 27, 2984–2993. [Google Scholar] [CrossRef] [PubMed]
- Olewnik, Ł.; Wysiadecki, G.; Polguj, M.; Topol, M. Anatomic Study Suggests That the Morphology of the Plantaris Tendon May Be Related to Achilles Tendonitis. Surg. Radiol. Anat. 2017, 39, 69–75. [Google Scholar] [CrossRef]
- Chaney, M.E.; Dao, T.V.; Brechtel, B.S.; Belovich, S.J.; Siesel, K.J.; Fredieu, J.R. The Fibularis Digiti Quinti Tendon: A Cadaveric Study with Anthropological and Clinical Considerations. Foot 2018, 34, 45–47. [Google Scholar] [CrossRef] [PubMed]
- Wells, L.H. A Peroneus Tertius Muscle in a Chacma Baboon (Papio Porcarius). J. Anat. 1935, 69, 508–514. [Google Scholar] [PubMed]
- Loth, E. Etude anthropologique sur l’apon’ evrose plantaire. Bull. Mem. Soci. D’anthropologie Paris 1913, 4, 601–609. [Google Scholar] [CrossRef]
- Krammer, E.B.; Lischka, M.F.; Gruber, H. Gross Anatomy and Evolutionary Significance of the Human Peroneus III. Anat. Embryol. 1979, 155, 291–302. [Google Scholar] [CrossRef]
- Hicks, J.H. The Mechanics of the Foot. IV. The Action of Muscles on the Foot in Standing. Acta Anat. 1956, 27, 180–192. [Google Scholar] [CrossRef]
- Karauda, P.; Paulsen, F.; Polguj, M.; Diogo, R.; Olewnik, Ł. Morphological Variability of the Fibularis Tertius Tendon in Human Foetuses. Folia Morphol. 2022, 81, 451–457. [Google Scholar] [CrossRef]
- Bardeen, C.R.; Lewis, W.H. Development of the Limbs, Body-wall and Back in Man. Am. J. Anat. 1901, 1, 1–35. [Google Scholar] [CrossRef]
- Diogo, R.; Siomava, N.; Gitton, Y. Development of Human Limb Muscles Based on Whole-Mount Immunostaining and the Links between Ontogeny and Evolution. Development 2019, 146, dev180349. [Google Scholar] [CrossRef] [PubMed]
- Albay, S.; Candan, B. Evaluation of Fibular Muscles and Prevalence of Accessory Fibular Muscles on Fetal Cadavers. Surg. Radiol. Anat. 2017, 39, 1337–1341. [Google Scholar] [CrossRef]
- Ruzik, K.; Westrych, K.; Zielinska, N.; Podgórski, M.; Karauda, P.; Diogo, R.; Paulsen, F.; Polguj, M.; Olewnik, Ł. The Morphological Variability of Fibularis Tertius Origin in Human Foetuses. Ann. Anat. 2022, 243, 151920. [Google Scholar] [CrossRef] [PubMed]
- Iceman, K.; Magnus, M.K.; Thompson, M.J.; Abicht, B.P. Peroneus Tertius Syndrome: A Rare Cause of Anterolateral Ankle and Rearfoot Pain. J. Foot Ankle Surg. 2020, 59, 131–135. [Google Scholar] [CrossRef] [PubMed]
- Derrick, E.; Flores, M.; Scherer, K.; Bancroft, L. Peroneus Tertius Tendon Tear: A Rare Cause of Lateral Ankle Pain. Cureus 2016, 8, e577. [Google Scholar] [CrossRef]
- McGoldrick, N.P.; Bergin, D.; Kearns, S.R. Peroneus Tertius Tendon Tear Causing Lateral Ankle Pain in a Child. J. Foot Ankle Surg. 2017, 56, 854–856. [Google Scholar] [CrossRef]
- Lee, S.J.; Jacobson, J.A.; Kim, S.-M.; Fessell, D.; Jiang, Y.; Dong, Q.; Morag, Y.; Choo, H.J.; Lee, S.-M. Ultrasound and MRI of the Peroneal Tendons and Associated Pathology. Skelet. Radiol. 2013, 42, 1191–1200. [Google Scholar] [CrossRef]
- Taljanovic, M.S.; Alcala, J.N.; Gimber, L.H.; Rieke, J.D.; Chilvers, M.M.; Latt, L.D. High-Resolution US and MR Imaging of Peroneal Tendon Injuries. RadioGraphics 2015, 35, 179–199. [Google Scholar] [CrossRef]
- Barchi, E.; Rose, D. Unlikely SuspectPeroneus Tertius Tear in a Professional Ballet Dancer. Bull. Hosp. Jt. Dis. 2020, 78, 275–276. [Google Scholar]
- Lee, J.W.; Joo, M.W.; Sung, J.-K.; Ahn, J.-H.; Kang, Y.-K. Origin of Satellite Ganglion Cysts with Effusion in the Flexor Hallucis Longus Tendon Sheath around the Hallux. Clin. Orthop. Surg. 2018, 10, 94. [Google Scholar] [CrossRef]
- Gude, W.; Morelli, V. Ganglion Cysts of the Wrist: Pathophysiology, Clinical Picture, and Management. Curr. Rev. Musculoskelet. Med. 2008, 1, 205–211. [Google Scholar] [CrossRef] [PubMed]
- Walls, R.C.; Ubillus, H.A.; Azam, M.T.; Kennedy, J.G.; Walls, R.J. Intra-Tendinous Ganglion Cyst of the Peroneus Tertius: A Case Report and Literature Review. Am. J. Case Rep. 2023, 24, e938498. [Google Scholar] [CrossRef] [PubMed]
- Ilyas, J. Ankle Arthroscopy. In Regional Arthroscopy; InTech: Rijeka, Croatia, 2013. [Google Scholar]
- Stotter, C.; Klestil, T.; Chemelli, A.; Naderi, V.; Nehrer, S.; Reuter, P. Anterocentral Portal in Ankle Arthroscopy. Foot Ankle Int. 2020, 41, 1133–1142. [Google Scholar] [CrossRef]
- Arnold, P.G.; Yugueros, P.; Hanssen, A.D. Muscle flaps in osteomyelitis of the lower extremity: A 20-year account. Plast Reconstr. Surg. 1999, 104, 107–110. [Google Scholar] [CrossRef] [PubMed]
- Wang, X.; Zhang, M.; Zhu, T.; Wei, Q.; Liu, G.; Ding, J. Flourishing Antibacterial Strategies for Osteomyelitis Therapy. Adv. Sci. 2023, 10, 2206154. [Google Scholar] [CrossRef]
- Zhao, X.; Shen, Y. Island Perforator Muscle Flaps for Chronic Osteomyelitis of the Lower Extremities: A Retrospective Analysis of 21 Consecutive Cases. Plast. Reconstr. Surg. 2022, 150, 677–687. [Google Scholar] [CrossRef]
- Lullo, B.; Nazareth, A.; Rethlefsen, S.; Illingworth, K.D.; Abousamra, O.; Kay, R.M. Split Tibialis Anterior Tendon Transfer to The Peroneus Brevis or Tertius for the Treatment of Varus Foot Deformities in Children with Static Encephalopathy: A Retrospective Case Series. JAAOS Glob. Res. Rev. 2020, 4, e20.00044. [Google Scholar] [CrossRef]
- Hoffer, M.M.; Reiswig, J.A.; Garrett, A.M.; Perry, J. The Split Anterior Tibial Tendon Transfer in the Treatment of Spastic Varus Hindfoot of Childhood. Orthop. Clin. N. Am. 1974, 5, 31–38. [Google Scholar] [CrossRef]
- Dong, Q.Y.; Jiang, J.Y.; Su, P.; Su, B.; Bai, L. Bin Anterior or Posterior Tibial Tendon Transfer to the Peroneus Tertius for Equinovarus Deformity. Orthop. Surg. 2024, 16, 2115–2122. [Google Scholar] [CrossRef] [PubMed]
- Camacho, L.D.; Roward, Z.T.; Deng, Y.; Daniel Latt, L. Surgical Management of Lateral Ankle Instability in Athletes. J. Athl. Train. 2019, 54, 639–649. [Google Scholar] [CrossRef] [PubMed]
- James Sammarco, G.; Carrasquillo, H.A. Surgical Revision after Failed Lateral Ankle Reconstruction. Foot Ankle Int. 1995, 16, 748–753. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author(s) | Year | Ethnicity | Study Type | Prevalence (%) |
|---|---|---|---|---|
| Unknown | - | Bahrain | Cadaver | 42.0 |
| Unknown | - | Saudi | Cadaver | 38.5 |
| Unknown | - | Kuwaiti | Cadaver | 41.2 |
| Wood | 1866 | British | Cadaver | 95.3 |
| Le Double | 1897 | French | Cadaver | 94.2 |
| Koganei et al. | 1903 | Japanese | Cadaver | 96.7 |
| Adachi | 1909 | Japanese | Cadaver | 95.0 |
| Loth | 1913 | African | Cadaver | 90.2 |
| Nakano | 1923 | Chinese | Cadaver | 89.3 |
| Posmykiewicz | 1934 | Polish | Clinical | 92.6 |
| Werneck | 1957 | Caucasian, Black | Cadaver | 95.6 |
| Sokolowska-Pituchowa et al. | 1974 | Polish | Cadaver | 92.0 |
| Krammer et al. | 1979 | Austrian | Cadaver | 92.9 |
| Testut, Latarjet | 1979 | Israeli | Cadaver | 10.0 |
| Reimann | 1981 | German | Cadaver | 90.0 |
| Bertelli and Khoury | 1991 | French | Cadaver | 91.0 |
| Stevens et al. | 1993 | British | Cadaver | 95.0 |
| Da-Yae Choi1 | 2001 | Korean | Cadaver | 92.6 |
| Larico and Jordan | 2005 | Bolivian | Cadaver | 100.0 |
| Joshi et al. | 2006 | Indian | Cadaver | 89.6 |
| Kunnika et al. | 2006 | Thai | Cadaver | 95.6 |
| Marin et al. | 2006 | Brazilian | Cadaver | 94.0 |
| Marin et al. | 2006 | Brazilian | Cadaver | 93.8 |
| Witvrouw et al. | 2006 | Belgian | Clinical | 81.5 |
| Rourke et al. | 2007 | British | Cadaver | 93.9 |
| Bhatt et al. | 2010 | Indian | Cadaver | 89.4 |
| Ramirez et al. | 2010 | Chilean | Clinical | 50.9 |
| Bourdon and Petitdant | 2012 | French | Clinical | 88.4 |
| Ashaolu et al. | 2013 | Nigerian | Clinical | 63.0 |
| de Gusmão et al. | 2013 | Brazilian | Cadaver | 96.9 |
| Oyedun et al. | 2014 | Nigerian | Clinical | 88.5 |
| Surekha et al. | 2015 | Indian | Cadaver | 87.0 |
| Verma and Seema | 2015 | Indian | Cadaver | 100.0 |
| Ercikti et al. | 2016 | Turkish | Cadaver | 95.5 |
| Losa-Iglesias et al. | 2017 | Spanish | Clinical | 38.2 |
| Salem et al. | 2018 | Tunisian | Clinical | 67.7 |
| Salem et al. | 2018 | Egyptian | Clinical | 52.8 |
| Author | Year | Origin [%] | ||
|---|---|---|---|---|
| Distal Half Fibula | Distal Third Fibula | EDL Tendon | ||
| Kaneff | 1980 | 75.7 | 0 | 24.3 |
| Bertelli and Khoury | 1991 | 100 | 0 | 0 |
| Stevens et al. | 1993 | 92.11 | - | - |
| Marin et al. | 2006 | 83.3 | 16.7 | 0 |
| Rourke et al. | 2007 | 100 | 0 | 0 |
| Bhatt et al. | 2010 | 92.8 | 0 | 7.14 |
| de Gusmão et al. | 2013 | 45.2 | 54.8 | 0 |
| Surekha et al. | 2015 | 91.9 | 0 | 8.04 |
| Verma and Seema | 2015 | 98.3 | 0 | 1.66 |
| Olewnik | 2019 | 67 | 22 | 11 |
| Author(s) | Year | Insertion Sites % | ||||
|---|---|---|---|---|---|---|
| Shaft M5 | Base M5 | M4–M5 | M4 | EDL Tendon | ||
| Wood | 1866 | 90.2 | 3.28 | 6.5 | 0 | |
| Wood | 1867 | 93.3 | 6.7 | 0 | ||
| Wood | 1868 | 88.4 | 2.90 | 4.3 | 4.3 | |
| Johnson | 1973 | 10.9 | 47.3 | 12.4 | 1.2 | 16 |
| Kaneff | 1980 | 14 | 75.7 | 10 | 0 | 0 |
| Bertelli and Khoury | 1991 | 10 | 80 | 0 | 0 | 10 |
| Stevens et al. | 1993 | 82.5 | - | - | - | 10 |
| Domagala et al. | 2006 | 9.9 | 0 | 90 | 0 | 0 |
| Marin et al. | 2006 | 90 | 7 | 3 | 0 | 0 |
| Rourke et al. | 2007 | 0 | 0 | 100 | 0 | 0 |
| de Gusmão et al. | 2013 | 77.4 | 0 | 22.6 | 0 | 0 |
| Surekha et al. | 2015 | 0 | 44.8 | 25.3 | 24.1 | 0 |
| Verma and Seema | 2015 | 100 | 0 | 0 | 0 | |
| Olewnik | 2019 | 45 | 22 | 0 | 0 | 0 |
| Author(s) | Year | Ethnicity | Study Type | Fetuses | Prevalence |
|---|---|---|---|---|---|
| Sokolowska-Pituchowa et al. | 1979 | Polish | Cadaver | Fetuses | 78.6% |
| Kaneff | 1980 | French | Cadaver | Fetuses | 88.2% |
| Domagala et al. | 2006 | Polish | Cadaver | Fetuses | 83.2% |
| Albay and Candan | 2017 | Turkish | Cadaver | Fetuses | 80.0% |
| Karauda et al. | 2021 | Polish | Cadaver | Fetuses | 50.0% |
| Ruzik et al. | 2022 | Polish | Cadaver | Fetuses | 50.0% |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2025 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Pośnik, M.; Węgiel, A.; Zielinska, N.; Ruzik, K.; Olewnik, Ł.; Triantafyllou, G.; Piagkou, M.; Podgórski, M. Morphological Variability and Clinical Significance of the Fibularis Tertius Muscle: An Extensive Literature Review. J. Clin. Med. 2025, 14, 3991. https://doi.org/10.3390/jcm14113991
Pośnik M, Węgiel A, Zielinska N, Ruzik K, Olewnik Ł, Triantafyllou G, Piagkou M, Podgórski M. Morphological Variability and Clinical Significance of the Fibularis Tertius Muscle: An Extensive Literature Review. Journal of Clinical Medicine. 2025; 14(11):3991. https://doi.org/10.3390/jcm14113991
Chicago/Turabian StylePośnik, Marta, Andrzej Węgiel, Nicol Zielinska, Kacper Ruzik, Łukasz Olewnik, George Triantafyllou, Maria Piagkou, and Michał Podgórski. 2025. "Morphological Variability and Clinical Significance of the Fibularis Tertius Muscle: An Extensive Literature Review" Journal of Clinical Medicine 14, no. 11: 3991. https://doi.org/10.3390/jcm14113991
APA StylePośnik, M., Węgiel, A., Zielinska, N., Ruzik, K., Olewnik, Ł., Triantafyllou, G., Piagkou, M., & Podgórski, M. (2025). Morphological Variability and Clinical Significance of the Fibularis Tertius Muscle: An Extensive Literature Review. Journal of Clinical Medicine, 14(11), 3991. https://doi.org/10.3390/jcm14113991