
Cognitive Enhancement Strategies for Older Adults: An Evaluation of Different Training Modalities to Improve Executive Function—A Systematic Review and Meta-Analysis

 ,
,  ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
2.1. Systematic Literature Search
2.2. Selection Criteria
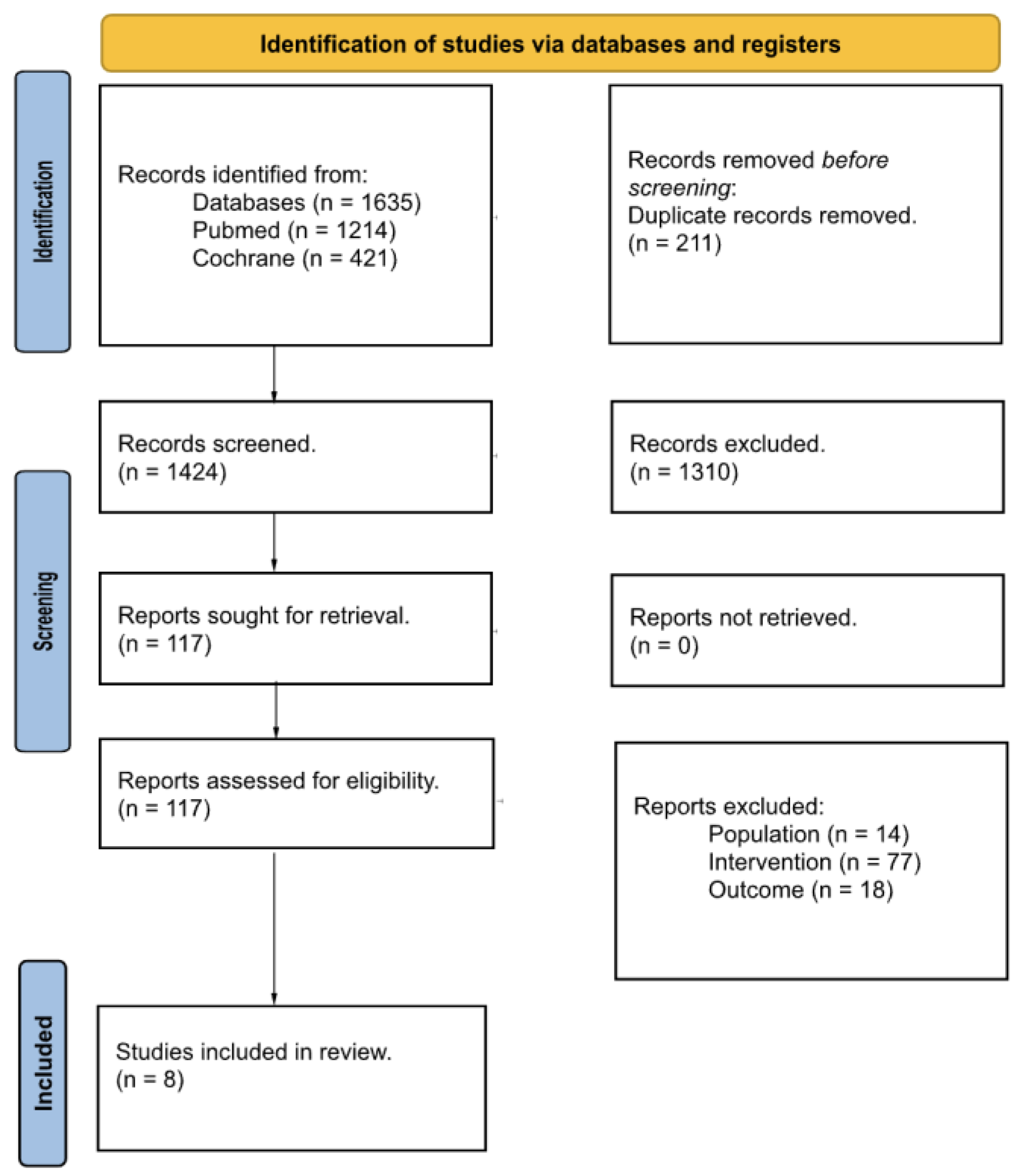
2.3. Screening, Selection Process, and Data Extraction
2.4. Assessment of Methodological Quality and Risk of Bias
2.5. Data Synthesis and Analysis
3. Results
3.1. Study Characteristics
3.2. PEDro Score
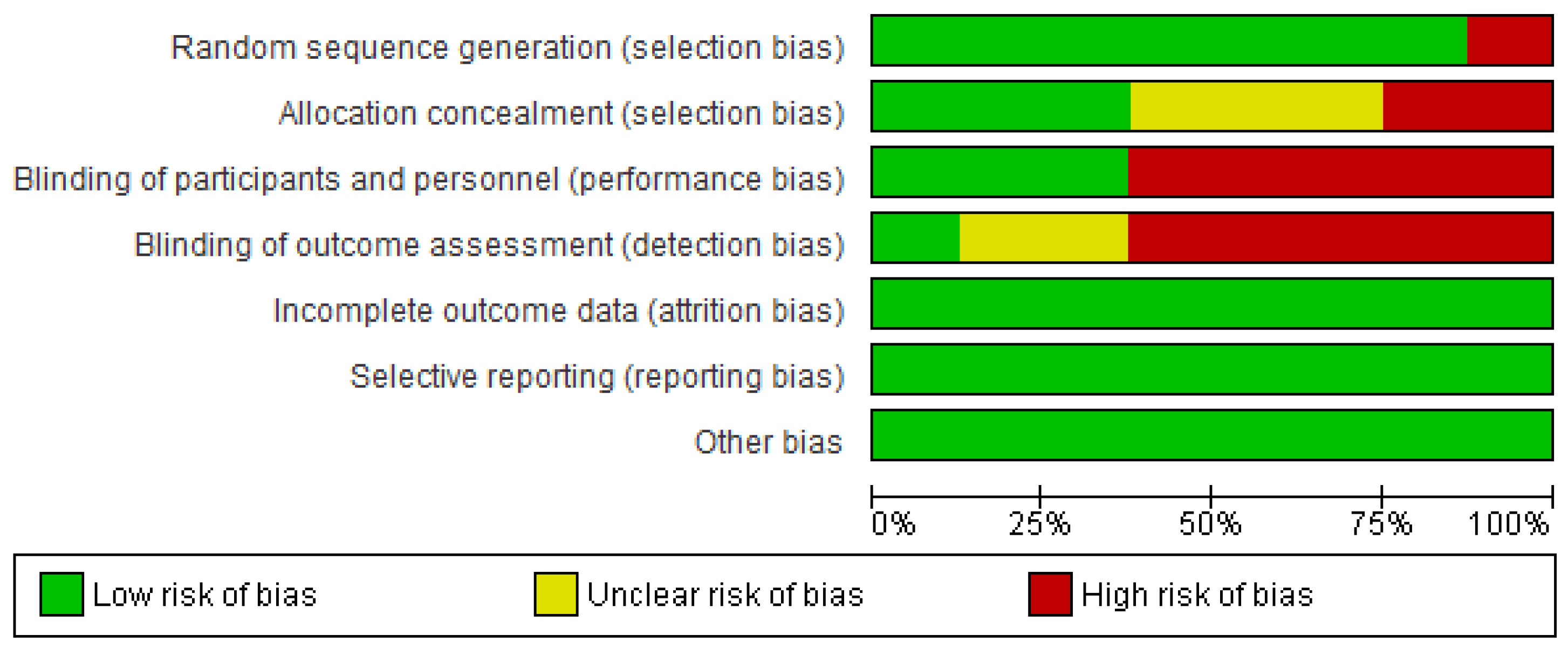
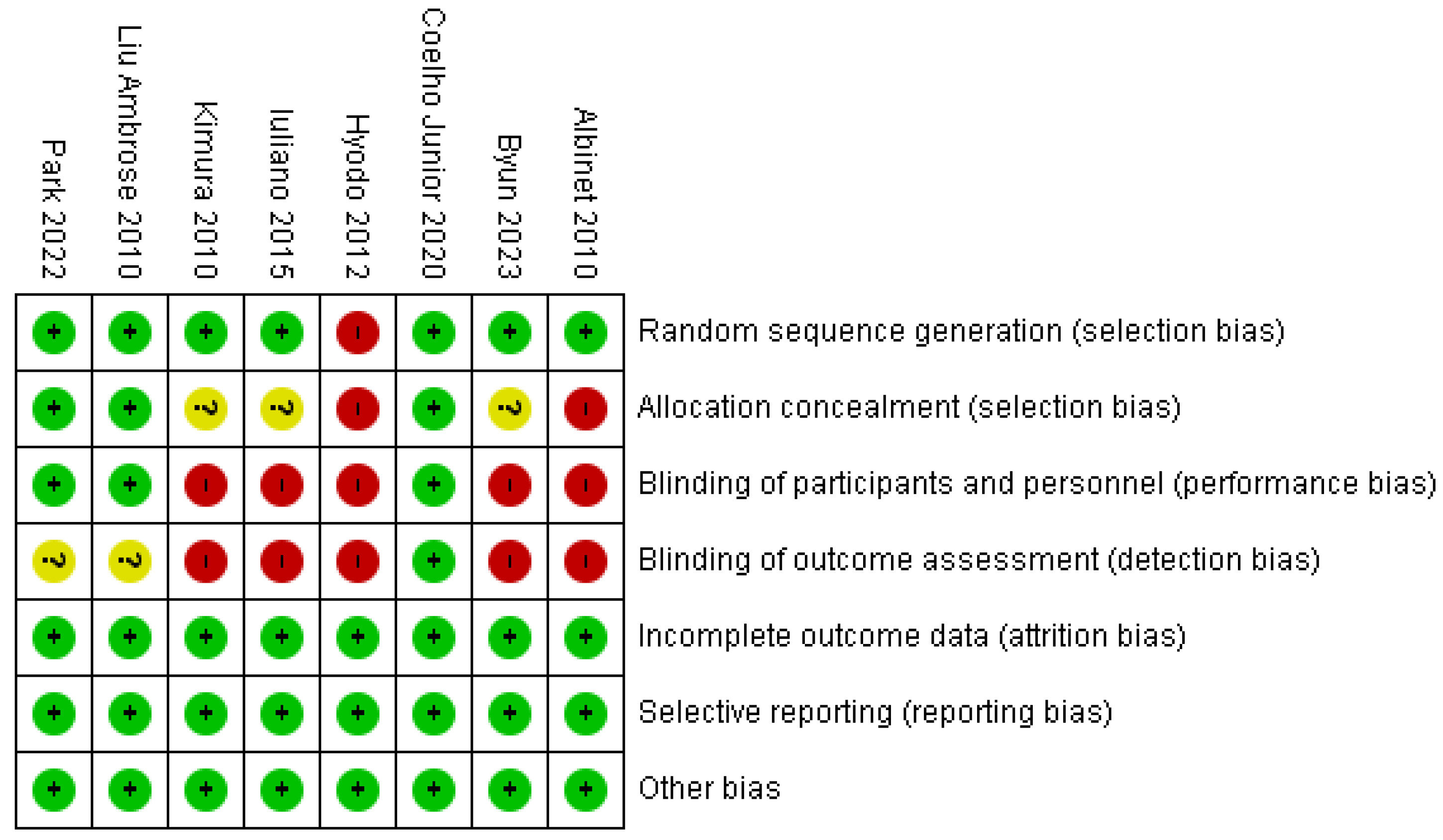
3.3. Risk of Bias Graph and Summary
3.4. Effectiveness of Interventions
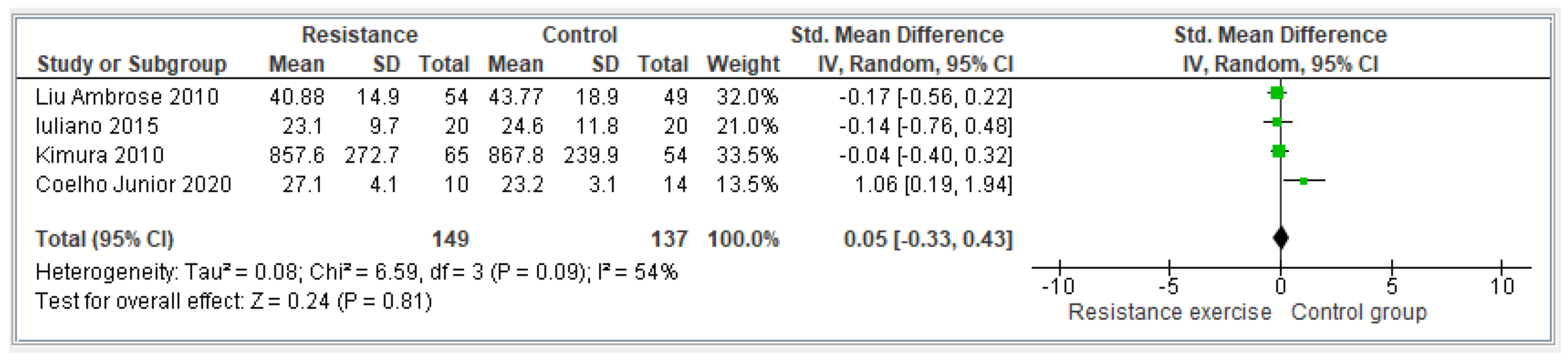
3.4.1. Resistance Exercise
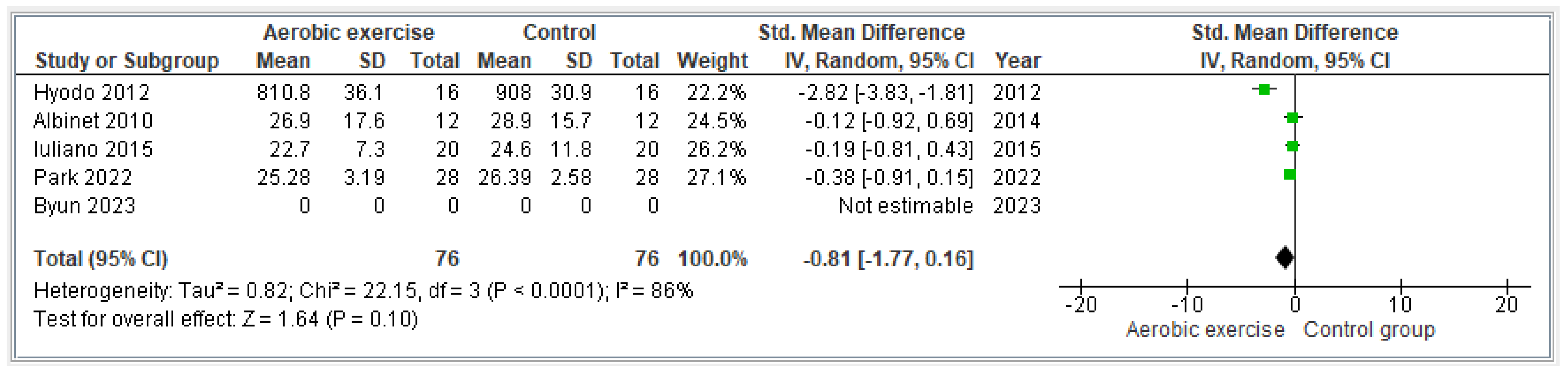
3.4.2. Aerobic Exercise
4. Discussion
4.1. Resistance Exercise
4.2. Aerobic Exercise
4.3. Need for New Therapeutic Strategies
4.4. Limitations of the Study
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- United Nations. World Population Ageing 2009; Edited by Division DoEaSAP; United Nations: New York City, NY, USA, 2009. [Google Scholar]
- Van Uffelen, J.G.; Chin A Paw, M.J.; Hopman-Rock, M.; van Mechelen, W. The effects of exercise on cognition in older adults with and without cognitive decline: A systematic review. Clin. J. Sport Med. 2008, 18, 486–500. [Google Scholar] [CrossRef] [PubMed]
- Vieweg, J.; Leinen, P.; Verwey, W.B.; Shea, C.H.; Panzer, S. The Cognitive Status of Older Adults: Do Reduced Time Constraints Enhance Sequence Learning? J. Mot. Behav. 2020, 52, 558–569. [Google Scholar] [CrossRef] [PubMed]
- Mehta, K.M.; Yae, K.; Covinsky, K.E. Cognitive impairment, depressive symptoms, and functional decline in older people. J. Am. Geriatr. Soc. 2002, 50, 1045–1050. [Google Scholar] [CrossRef] [PubMed]
- Fisher, G.G.; Chacon, M.; Chaee, D.S. Chapter 2—Theories of Cognitive Aging and Work. In Work Across the Lifespan; Baltes, B.B., Rudolph, C.W., Zacher, H., Eds.; Academic Press: Cambridge, MA, USA, 2019; pp. 17–45. [Google Scholar]
- Huang, C.; Lin, P.; Hung, C.; Chang, Y.; Hung, T. Type of physical exercise and inhibitory function in older adults: An event-related potential study. Psychol. Sport Exerc. 2014, 15, 205–211. [Google Scholar] [CrossRef]
- Miyake, A.; Friedman, N.P. The nature and Organization of Individual Differences in executive functions: Four general conclusions. Curr. Dir. Psychol. Sci. 2012, 21, 8–14. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Wang, J.; Cai, X.; Zhang, X.; Zhang, J.; Peng, M.; Xiao, D.; Ouyang, H.; Yan, F. Effects of physical activity interventions on executive function in older adults with dementia: A meta-analysis of randomized controlled trials. Geriatr. Nurs. 2023, 51, 369–377. [Google Scholar] [CrossRef] [PubMed]
- Martyr, A.; Clare, L. Executive function and activities of daily living in Alzheimer’s disease: A correlational meta-analysis. Dement. Geriatr. Cogn. Disord. 2012, 33, 189–203. [Google Scholar] [CrossRef]
- De Greeff, J.W.; Bosker, R.J.; Oosterlaan, J.; Visscher, C.; Hartman, E. Effects of Physical Activity on Executive Functions, Attention and Academic Performance in Preadolescent Children: A Meta-Analysis. J. Sci. Med. Sport 2018, 21, 501–507. [Google Scholar] [CrossRef]
- Van Impe, A.; Bruijn, S.M.; Coxon, J.P.; Wenderoth, N.; Sunaert, S.; Duysens, J.; Swinnen, S.P. Age-Related Neural Correlates of Cognitive Task Performance Under Increased Postural Load. Age 2013, 35, 2111–2124. [Google Scholar] [CrossRef]
- Park, D.; Reuter-Lorenz, P. The Adaptive Brain: Aging and Neurocognitive Scaffolding. Annu. Rev. Psychol. 2009, 60, 173–196. [Google Scholar] [CrossRef]
- Braga, P.L.G.; Henrique, J.S.; Almeida, S.S.; Arida, R.M.; Gomes da Silva, S. Factors affecting executive function performance of Brazilian elderly in the Stroop test. Braz. J. Med. Biol. Res. 2022, 55, e11917. [Google Scholar] [CrossRef] [PubMed]
- Keith, N.R.; Stump, T.E.; Clark, D.O. Developing a self-reported physical fitness survey. Med. Sci. Sport Exerc. 2012, 44, 1388–1394. [Google Scholar] [CrossRef] [PubMed]
- Suchy, Y.; Gereau Mora, M.; DesRuisseaux, L.A.; Brothers, S.L. It’s complicated: Executive functioning moderates impacts of daily busyness on everyday functioning in community-dwelling older adults. J. Int. Neuropsychol. Soc. 2023, 29, 850–858. [Google Scholar] [CrossRef] [PubMed]
- Sanders, L.M.J.; Hortobagyi, T.; Karssemeijer, E.G.A.; Van der Zee, E.A.; Scherder, E.J.A.; Van Heuvelen, M.J.G. Effects of low- and high-intensity physical exercise on physical and cognitive function in older persons with dementia: A randomized controlled trial. Alzheimers Res. Ther. 2020, 12, 28. [Google Scholar] [CrossRef] [PubMed]
- Yoon, D.H.; Lee, J.Y.; Song, W. Effects of resistance exercise training on cognitive function and physical performance in cognitive frailty: A randomized controlled trial. J. Nutr. Health Aging 2018, 22, 944–951. [Google Scholar] [CrossRef] [PubMed]
- Chen, F.T.; Etnier, J.L.; Chan, K.H.; Chiu, P.K.; Hung, T.M.; Chang, Y.K. Effects of Exercise Training Interventions on Executive Function in Older Adults: A Systematic Review and Meta-Analysis. Sports Med. 2020, 50, 1451–1467. [Google Scholar] [CrossRef]
- Cotman, C.W.; Berchtold, N.C.; Christie, L.A. Exercise builds brain health: Keyroles of growth factor cascades and inflammation. Trends Neurosci. 2007, 30, 464–472. [Google Scholar] [CrossRef]
- Nagamatsu, L.S.; Flicker, L.; Kramer, A.F.; Voss, M.W.; Erickson, K.I.; Hsu, C.L.; Liu-Ambrose, T. Exercise is medicine for the body and the brain. Br. J. Sports Med. 2014, 48, 943–944. [Google Scholar] [CrossRef]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 statement: An updated guideline for reporting systematic reviews. BMJ 2021, 134, 103–112. [Google Scholar]
- Ouzzani, M.; Hammady, H.; Fedorowicz, Z.; Elmagarmid, A. Rayyan—A web and mobile app for systematic reviews. Syst. Rev. 2016, 5, 210. [Google Scholar] [CrossRef] [PubMed]
- Sterne, J.A.C.; Savovic, J.; Page, M.; Elbers, R.; Blencowe, N.; Boutron, I.; Cates, C.J.; Cheng, H.-Y.; Corbett, M.S.; Eldridge, S.M.; et al. RoB 2: A revised tool for assessing risk of bias in randomised trials. BMJ 2019, 366, l4898. [Google Scholar] [CrossRef]
- Cashin, A.; McAuley, J. Clinimetrics: Physiotherapy evidence database (PEDro) scale. J. Physiother. 2020, 66, 59. [Google Scholar] [CrossRef]
- DerSimonian, R.; Laird, N. Meta-analysis in clinical trials. Control. Clin. Trials 1986, 7, 177–188. [Google Scholar] [CrossRef] [PubMed]
- Higgins, J.P.T.; Thompson, S.; Deeks, J.; Altman, D. Measuring inconsistency in metaanalyses. BMJ 2003, 327, 557–560. [Google Scholar] [CrossRef] [PubMed]
- Hyodo, K.; Dan, I.; Suwabe, K.; Kyutoku, Y.; Yamada, Y.; Akahori, M.; Byun, K.; Kato, M.; Soya, H. Acute moderate exercise enhances compensatory brain activation in older adults. Neurobiol. Aging 2012, 33, 2621–2632. [Google Scholar] [CrossRef] [PubMed]
- Kimura, K.; Obuchi, S.; Arai, T.; Nagasawa, H.; Shiba, Y.; Watanabe, S.; Kojima, M. The influence of short-term strength training on health-related quality of life and executive cognitive function. J. Physiol. Anthropol. 2010, 29, 95–101. [Google Scholar] [CrossRef] [PubMed]
- Iuliano, E.; di Cagno, A.; Aquino, G.; Fiorilli, G.; Mignogna, P.; Calcagno, G.; Di Costanzo, A. Effects of different types of physical activity on the cognitive functions and attention in older people: A randomized controlled study. Exp. Gerontol. 2015, 70, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Liu-Ambrose, T.; Nagamatsu, L.S.; Graf, P.; Beattie, B.L.; Ashe, M.C.; Handy, T.C. Resistance training and executive functions: A 12-month randomized controlled trial. Arch. Intern. Med. 2010, 170, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Coelho-Júnior, H.J.; Gonçalves, I.O.; Sampaio, R.A.C.; Sampaio, P.Y.S.; Lusa Cadore, E.; Calvani, R.; Picca, A.; Izquierdo, M.; Marzetti, E.; Uchida, M.C. Effects of Combined Resistance and Power Training on Cognitive Function in Older Women: A Randomized Controlled Trial. Int. J. Environ. Res. Public Health 2020, 17, 3435. [Google Scholar] [CrossRef]
- Albinet, C.T.; Boucard, G.; Bouquet, C.A.; Audiffren, M. Increased heart rate variability and executive performance after aerobic training in the elderly. Eur. J. Appl. Physiol. 2010, 109, 617–624. [Google Scholar] [CrossRef]
- Byun, K.; Hyodo, K.; Suwabe, K.; Fukuie, T.; Ha, M.S.; Damrongthai, C.; Kuwamizu, R.; Koizumi, H.; Yassa, M.A.; Soya, H. Mild exercise improves executive function with increasing neural efficiency in the prefrontal cortex of older adults. Geroscience 2023, 46, 309–325. [Google Scholar] [CrossRef] [PubMed]
- Park, J.H. Effects of acute moderate-intensity aerobic exercise on executive function and prefrontal cortex activity in community-dwelling older adults: A single-blind, randomized controlled trial. Geriatr. Gerontol. Int. 2022, 22, 227–232. [Google Scholar] [CrossRef] [PubMed]
- Northey, J.M.; Cherbuin, N.; Pumpa, K.L.; Smee, D.J.; Rattray, B. Exercise interventions for cognitive function in adults older than 50: A systematic review with meta-analysis. Br. J. Sports Med. 2018, 52, 154–160. [Google Scholar] [CrossRef] [PubMed]
- Chang, Y.K.; Nien, Y.H.; Tsai, C.L.; Etnier, J.L. Physical activity and cognition in older adults: The potential of Tai Chi Chuan. J. Aging Phys. Activ. 2010, 18, 451–472. [Google Scholar] [CrossRef]
- Snowden, M.; Steinman, L.; Mochan, K.; Grodstein, F.; Prohaska, T.R.; Thurman, D.J.; Brown, D.R.; Laditka, J.N.; Soares, J.; Zweiback, D.J.; et al. Effect of exercise on cognitive performance in community-dwelling older adults: Review of intervention trials and recommendations for public health practice and research. J. Am. Geriatr. Soc. 2011, 59, 704–716. [Google Scholar] [CrossRef] [PubMed]
- Angevaren, M.; Aufdemkampe, G.; Verhaar, H.J.; Aleman, A.; Vanhees, L. Physical activity and enhanced fitness to improve cognitive function in older people without known cognitive impairment. Cochrane Database Syst Rev. 2008, 3, CD005381. [Google Scholar]
- Kelly, M.E.; Loughrey, D.; Lawlor, B.A.; Robertson, I.H.; Walsh, C.; Brennan, S. The impact of exercise on the cognitive functioning of healthy older adults: A systematic review and meta-analysis. Ageing Res. Rev. 2014, 16, 12–31. [Google Scholar] [CrossRef]
- Li, Z.; Peng, X.; Xiang, W.; Han, J.; Li, K. The effect of resistance training on cognitive function in the older adults: A systematic review of randomized clinical trials. Aging Clin. Exp. Res. 2018, 30, 1259–1273. [Google Scholar] [CrossRef]
- Gomes-Osman, J.; Cabral, D.F.; Morris, T.P.; McInerney, K.; Cahalin, L.P.; Rundek, T.; Oliveira, A.; Pascual-Leone, A. Exercise for cognitive brain health in aging: A systematic review for an evaluation of dose. Neurol. Clin. Pract. 2018, 8, 257–265. [Google Scholar] [CrossRef]
- Frost, N.J.; Weinborn, M.; Gignac, G.E.; Rainey-Smith, S.R.; Markovic, S.; Gordon, N.; Sohrabi, H.R.; Laws, S.M.; Martins, R.N.; Peiffer, J.J.; et al. A Randomized Controlled Trial of High-Intensity Exercise and Executive Functioning in Cognitively Normal Older Adults. Am. J. Geriatr. Psychiatry 2021, 29, 129–140. [Google Scholar] [CrossRef]
- Smiley-Oyen, A.L.; Lowry, K.A.; Francois, S.J.; Kohut, M.L.; Ekkekakis, P. Exercise, fitness, and neurocognitive function in older adults: The “selective improvement” and “cardiovascular fitness” hypotheses. Ann. Behav. Med. 2008, 36, 280–291. [Google Scholar] [CrossRef] [PubMed]
- Coetsee, C.; Terblanche, E. The effect of three different exercise training modalities on cognitive and physical function in a healthy older population. Eur. Rev. Aging Phys. Act. 2017, 14, 13. [Google Scholar] [CrossRef] [PubMed]
- Kramer, A.F.; Hahn, S.; Cohen, N.J.; Banich, M.T.; McAuley, E.; Harrison, C.R.; Chason, J.; Vakil, E.; Bardell, L.; Boileau, R.A.; et al. Ageing, fitness and neurocognitive function. Nature 1999, 400, 418–419. [Google Scholar] [CrossRef] [PubMed]
- Fabre, C.; Chamari, K.; Mucci, P.; Massé-Biron, J.; Préfaut, C. Improvement of cognitive function by mental and/or individualized aerobic training in healthy elderly subjects. Int. J. Sports Med. 2002, 23, 415–421. [Google Scholar] [CrossRef] [PubMed]
- Izquierdo, M.; Merchant, R.A.; Morley, J.E.; Anker, S.D.; Aprahamian, I.; Arai, H.; Aubertin-Leheudre, M.; Bernabei, R.; Cadore, E.L.; Cesari, M.; et al. International Exercise Recommendations in Older Adults (ICFSR): Expert Consensus Guidelines. J. Nutr. Health Aging 2021, 25, 824–853. [Google Scholar] [CrossRef] [PubMed]
- Gronwald, T.; Törpel, A.; Herold, F.; Budde, H. Perspective of Dose and Response for Individualized Physical Exercise and Training Prescription. J. Funct. Morphol. Kinesiol. 2020, 5, 48. [Google Scholar] [CrossRef]
- Kim, K.H.; Lee, H.B. The effects of whole-body vibration exercise intervention on electroencephalogram activation and cognitive function in women with senile dementia. J. Exerc. Rehabil. 2018, 14, 586–591. [Google Scholar] [CrossRef]
- Heesterbeek, M.; Van der Zee, E.A.; van Heuvelen, M.J.G. Passive exercise to improve quality of life, activities of daily living, care burden and cognitive functioning in institutionalized older adults with dementia—A randomized controlled trial study protocol. BMC Geriatr. 2018, 18, 182. [Google Scholar] [CrossRef]






{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Study | N (IG/CG) | Age (±SD) | Gender (F/M) | Modality | Variable |
|---|---|---|---|---|---|
| Albinet et al., 2010 [32] | 24 (12/12) | 70.7 ± 4.2 | 13/11 | AE | WCST |
| Byun et al., 2023 [33] | 81 (40/41) | 68.2 | 61/20 | AE | SCT |
| Coelho Junior et al., 2020 [31] | 24 (10/14) | 67.0 ± 6.2/66.7 ± 4.8 * | 24/0 | RE | MMSE |
| Hyodo et al., 2012 [27] | 16 (16/16) | 69.3 ± 3.5 | 3/13 | AE | ST |
| Iuliano et al., 2015 [29] | 40 (20/20) | 65.8 ± 6.3/66.4 ± 6.3 * | 23/17 | RE | SCT |
| Iuliano et al., 2015 [29] | 40 (20/20) | 68.4 ± 6.4/66.4 ± 6.3 * | 24/16 | AE | SCT |
| Kimura et al., 2010 [28] | 119 (65/54) | 73.6 ± 4.7/75.2 ± 6.3 * | 70/39 | RE | TST |
| Liu Ambrose et al., 2010 [30] | 103 (54/49) | 69.6 ± 3 | 155/0 | RE | SCT |
| Park et al., 2022 [34] | 56 (28/28) | 67.7 ± 4.1/67.7 ± 4.9 * | 28/28 | AE | SCT |
| Author | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 | 11 | Total |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Albinet et al., 2010 [32] | 0 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Byun et al., 2023 [33] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 0 | 1 | 1 | 7 |
| Coelho Junior et al., 2020 [31] | 1 | 0 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 3 |
| Hyodo et al., 2012 [27] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 1 | 0 | 1 | 1 | 5 |
| Park et al. [34] | 1 | 1 | 1 | 1 | 0 | 0 | 1 | 1 | 1 | 1 | 1 | 8 |
| Iuliano et al., 2015 [29] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 1 | 1 | 1 | 5 |
| Kimura et al., 2010 [28] | 1 | 1 | 1 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 5 |
| Liu Ambrose et al., 2010 [30] | 1 | 1 | 0 | 1 | 0 | 0 | 0 | 0 | 0 | 1 | 1 | 4 |
| Average | 5 * |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Rodriguez-Rodríguez, S.; Canet-Vintró, M.; Wee, S.O.; Rodríguez-Sanz, J.; López-de-Celis, C.; Oviedo, G.R.; Labata-Lezaun, N.; Pérez-Bellmunt, A. Cognitive Enhancement Strategies for Older Adults: An Evaluation of Different Training Modalities to Improve Executive Function—A Systematic Review and Meta-Analysis. J. Clin. Med. 2024, 13, 1301. https://doi.org/10.3390/jcm13051301
Rodriguez-Rodríguez S, Canet-Vintró M, Wee SO, Rodríguez-Sanz J, López-de-Celis C, Oviedo GR, Labata-Lezaun N, Pérez-Bellmunt A. Cognitive Enhancement Strategies for Older Adults: An Evaluation of Different Training Modalities to Improve Executive Function—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine. 2024; 13(5):1301. https://doi.org/10.3390/jcm13051301
Chicago/Turabian StyleRodriguez-Rodríguez, Sergi, Max Canet-Vintró, Sang Ouk Wee, Jacobo Rodríguez-Sanz, Carlos López-de-Celis, Guillermo R. Oviedo, Noé Labata-Lezaun, and Albert Pérez-Bellmunt. 2024. "Cognitive Enhancement Strategies for Older Adults: An Evaluation of Different Training Modalities to Improve Executive Function—A Systematic Review and Meta-Analysis" Journal of Clinical Medicine 13, no. 5: 1301. https://doi.org/10.3390/jcm13051301
APA StyleRodriguez-Rodríguez, S., Canet-Vintró, M., Wee, S. O., Rodríguez-Sanz, J., López-de-Celis, C., Oviedo, G. R., Labata-Lezaun, N., & Pérez-Bellmunt, A. (2024). Cognitive Enhancement Strategies for Older Adults: An Evaluation of Different Training Modalities to Improve Executive Function—A Systematic Review and Meta-Analysis. Journal of Clinical Medicine, 13(5), 1301. https://doi.org/10.3390/jcm13051301