
Current Concepts of Cervical Spine Alignment, Sagittal Deformity, and Cervical Spine Surgery

 ,
,  and
and
Abstract
1. Introduction
2. Degenerative Cervical Myelopathy (DCM)
3. Cervical Kyphosis and Myelopathy
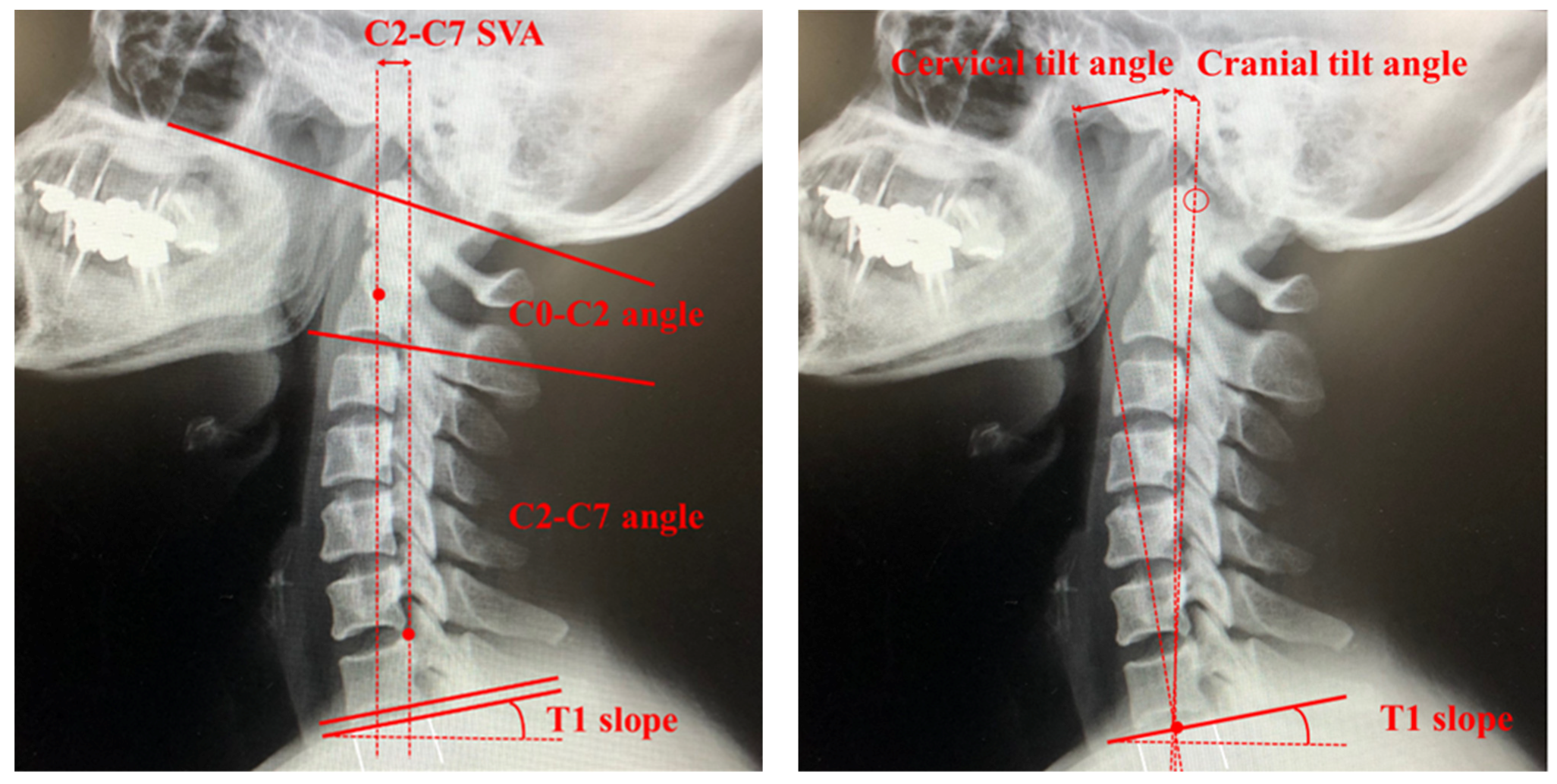
4. Cervical Spine Alignment Parameters
5. Systematic Review of Cervical Deformity and Cervical Spine Surgery
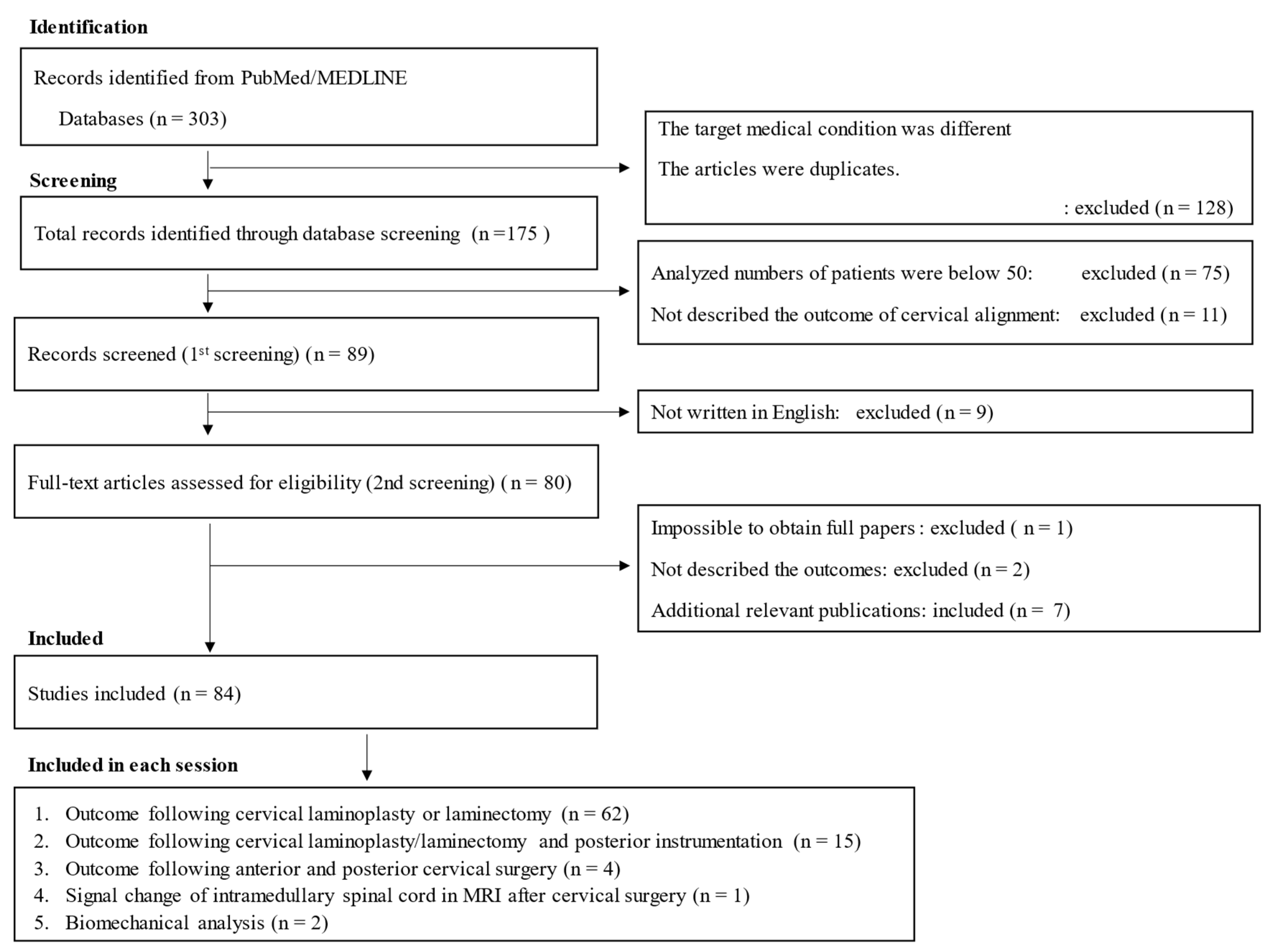
5.1. Literature Search and Inclusion Criteria
5.2. Study Selection
5.3. Assessment of Quality and Risk of Bias
6. Selection of Surgical Techniques for DCM and Cervical Spine Alignment [30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100,101,102,103,104,105,106,107,108,109,110,111,112,113,114,115]
6.1. Laminoplasty Following Posterior Approach
6.1.1. Cervical Spondylotic Myelopathy [38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72] (Table 2)
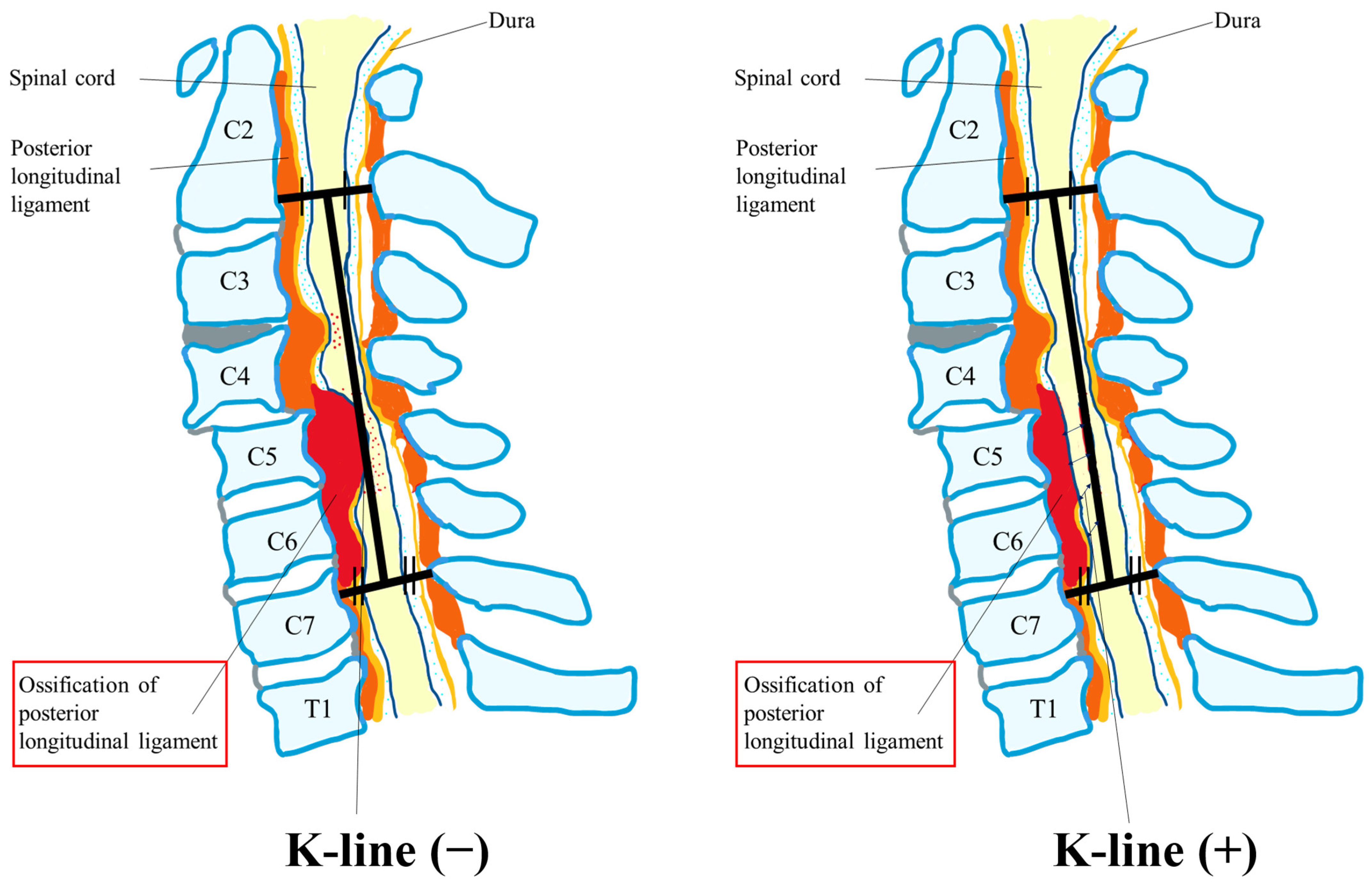
6.1.2. Ossification of the Posterior Longitudinal Ligament [73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99,100] (Table 2)

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| 1st Author | Year | Patient’s Number (CSM/OPLL) | Definition of Cervical Deformity | Type of Laminoplasty (LAMP) | Risk Factors of Postoperative Malalignment | Prediction Factors of Postoperative Malalignment before Surgery | Occurrence Rate of Postoperative Cervical Deformity | Risk Factors of Poor HRQOL Outcome |
|---|---|---|---|---|---|---|---|---|
| Sakai K [37] | 2016 | CSM: 174 | - | Double-door LAMP | - |
| 5.2% | Cervical JOA score was in the kyphotic deformity (+) group were inferior. |
| Oe S [38] | 2023 | CSM and OPLL: 193 | SVA ≥ 40 mm C2–7 angle ≤ −10° | Laminectomy Double/Open-door LAMP | Decompression of the C2 or C7 lamina. |
| 13.9% | No difference in post-cervical deformity |
| Kim BJ [39] | 2021 | CSM: 26, OPLL: 27 | - | Open/French-door LAMP (Opening lamina was fixed with a titanium miniplate) | - |
| - | - |
| Abe T [40] | 2022 | CSM: 110 | - | Double-door LAMP (Hydroxyapatite spinous process pacers) | Increase in O–C2 angle |
| - | - |
| Ninomiya K [41] | 2022 | CSM: 732 | Anterior cervical spondylolisthesis (Slippage of ≥2 mm) C2–7 angle ≤ −5° | Double/Open-door Selective LAMP | Anterior cervical spondylolisthesis with kyphosis |
| 2.3% | Preoperative cervical kyphosis |
| Zhang H [42] | 2015 | CSM: 198 | - | Open-door LAMP | No risk of different angles in lamina open-door | -- | - | No difference in different angles in lamina open-door |
| Nurboja B [43] | 2012 | CSM: 268 | - | Laminectomy Four or more cervical levels LAMP | - | |||
| Guo Q [44] | 2022 | CSM: 92 | - | Muscle preserved vs. conventional open-door LAMP | No difference | No difference | - | No difference |
| Lee DG [45] | 2013 | CSM and OPLL: 64 | - | Open-door vs. French-door LAMP | No difference | - | - | No difference |
| Nori S [46] | 2020 | CSM: 159 | - | Muscle-preserving selective laminectomy | Flexion K-line (−) |
| - | Flexion K-line (−) group |
| Jain A [47] | 2017 | CSM: 68 | - | Conventional laminectomy | - |
| No difference in post-cervical lordosis | |
| Liu C [48] | 2023 | CSM: 79 | C2–7 angle ≤ −10° | Open-door LAMP (mini titanium plate system) | Low ext. ROM |
| - | Low ext. ROM |
| Fujishiro T [49] | 2021 | CSM: 111 | - | Double-door LAMP | Gap ROM exceeding 30° |
| - | - |
| Lin BJ [50] | 2015 | CSM: 26 | - | Open-door LAMP | C2–7 angle ≤ 10° |
| - | Morphology was that of a neutral or posterior convexity-type spinal cord accompanied by kyphotic deformity |
| Chen HY [51] | 2020 | CSM: 85 | Kyphosis: C2–7 angle < 0° | Spinous process splitting LAMP | - |
| - |
|
| Takasawa E [52] | 2023 | CSM: 90 (age ≥ 65) | - | Open-door LAMP | - |
| 13.3% |
|
| Wang Z [53] | 2021 | CSM: 72 | T1 Spino-cranial angle > 20°: cervical imbalance | LAMP | - |
| - |
|
| Ikeda T [54] | 2023 | CSM/OPLL /CDH: 70 | K-line (+)/(−) | Miyazaki and Kirita’s method (n = 66) Kurokawa’s method (n = 4) |
|
| - |
|
| Nori S [55] | 2022 | CSM: 81 | Neck-flexed position K-line (+)/(−) | C4–C6 LAMP with C3 and C7 partial laminectomy | Neck-flexed position K-line (−) | Neck-flexed position K-line (−) | - | Neck-flexed position K-line (−) |
| Cao J [56] | 2017 | CSM: 194 (without preoperative kyphotic alignment) | - | Open-door LAMP (mini titanium plate system) |
|
| 10.8% |
|
| Kurihara K [57] | 2022 | CSM: 178 | Spondylolisthesis (slippage > 2 mm) | Selective LAMP | No risk | No risk | 16.3% | No risk |
| Laiginhas AR [58] | 2015 | CSM: 57 |
| LAMP | - | - | 8.8% | - |
| Minamide A [59] | 2017 | CSM: 78 | - | Microendoscopic laminotomy vs. conventional LAMP | Conventional LAMP | - | - | - |
| Taniyama T [60] | 2014 | CSM: 61 |
| Miyazaki and Kirita’s method LAMP | - | Minimal interval between the K-line and most anterior feature of the spinal canal | - | Minimal interval between the K-line and most anterior feature of the spinal canal |
| Ninomiya K [61] | 2021 | CSM: 379 |
| Selective LAMP | - |
| - | - |
| Chen G [62] | 2020 | CSM: 369 |
| Open-door LAMP (mini titanium plate system) | - |
| 7.8% | - |
| Machino M [63] | 2020 | CSM: 1025 |
| Modified double-door LAMP | - |
| 14.7% (Preoperative C2–7 angle ≤ 7°) | - |
| Yang Y [64] | 2023 | CSM: 266 | - | Open-door LAMP | - |
| 9.77% | No difference in alignment |
| Zhang JT [65] | 2017 | CSM: 41 (C2–7 angle > 5°) | - | Open-door LAMP (plate system) |
| - | - | |
| Shimizu T [66] | 2022 | CSM: 120 |
| Double-door LAMP | - |
| 33.3% | Residual anterior spinal cord compression |
| Obo T [67] | 2022 | CSM: 138 |
| LAMP |
|
|
| - |
| Chang H [68] | 2017 | CSM: 67 | - | Selective laminectomy vs. C3-6 LAMP | No difference | - | - | No difference |
| Sivaraman A [69] | 2010 | CSM: 50 | - | Skip Laminectomy vs. LAMP | - | - | Skip laminectomy: better outcome | |
| Nagoshi N [70] | 2021 | CSM: 80 |
| Expansive unilateral open-door LAMP | Smaller C7 slopes | Preoperative kyphosis | - | Preoperative kyphosis: No risk |
| Rao H [71] | 2019 | CSM: 85 | T1 slope minus C2–C7 lordosis < 20° | Open-door LAMP | - | T1 slope minus C2–C7 lordosis < 20° | - | - |
| Machino M [72] | 2018 | CSM: 1025 (<65/65–74/≥75 years) | - | Modified double-door LAMP | - | Elderly patients | - | Elderly patients |
| Yeh KT [73] | 2016 | DCM: 65 | - | Modified expansive open-door LAMP | - | none | - | - |
| Kanbara S [74] | 2018 | OPLL: 100 | K-line (+)/(−) | Double-door LAMP | Postoperative flexion value > 0 (Flexion ROM minus extension ROM) | K-line (−) | - | K-line (−) |
| Kawaguchi Y [75] | 2019 | OPLL: 153 | - | en bloc cervical LAMP | - | - | - |
|
| Chen Z [76] | 2016 | OPLL: 819 | - | Anterior corpectomy and fusion with LAMP vs. LAMP | - | - | - |
|
| Kim B [77] | 2016 | OPLL: 64 | Loss of cervical lordosis | LAMP | - |
| - | - |
| Liu X [78] | 2019 | OPLL: 132 (OPLL locating at the C2 segment) | - | C2–C7 vs. C3–7 LAMP | C2–C7 LAMP: no risk for malalignment | - | - | No difference |
| Nakashima H [79] | 2023 | OPLL: 165 | Postoperative loss of cervical lordosis > 10° or >20° | LAMP | - |
| 19.4% | Postoperative loss of cervical lordosis > 20° |
| Li C [80] | 2022 | OPLL: 81 | K-line (+)/(−) | Single-door LAMP | - | K-line (−) and lordosis < 7° | K-line (−): 30.77% | K-line (−) |
| Sakai K [81] | 2023 | OPLL: 62 |
| Double-door LAMP | - | K-line tilts > 20° | 6.5–9.7% | Kyphotic deformity |
| Yoo S [82] | 2017 | OPLL: 73 | - | Laminectomy vs. LAMP | Laminectomy: no risk for malalignment in continuous-type OPLL | - | 7.9–8.6% | Laminectomy: no risk for malalignment in continuous-type OPLL |
| Saito J [83] | 2020 | OPLL: 72 | - | LAMP for K-line (+) OPLL | - |
| - | Preoperative segmental ROM at the peak of OPLL |
| Xu C [84] | 2020 | OPLL: 181 | - | LAMP | - |
| - | Postoperative lordosis loss |
| Kim SW [85] | 2020 | DCM: 83 |
| Double-door LAMP (Hydroxyapatite spinous process pacers) | Non-reducible ROM |
| - | -- |
| Shimizu K [86] | 2021 | DCM: 113 | - | Open- or double-door LAMP (Semispinalis cervicis muscles: preservation (vs. detachment) | Detaching the semispinalis cervicis muscle | - | - | - |
| Chen H [87] | 2015 | DCM: 57 | - | Open-door LAMP (Mini-plate fixation vs. Suture suspension fixation) | Open-door LAMP: Suture suspension fixation | - | - | Open-door LAMP: Suture suspension fixation |
| Sakamoto R [88] | 2022 | DCM: 100 | - | Double-door LAMP | - | T1 slope minus cervical lordosis > 20° | - | T1 slope minus cervical lordosis > 20° |
| Qian S [89] | 2018 | DCM: 137 | - | Open-door LAMP |
|
| - | Kyphosis |
| Fujiwara H [90] | 2018 | DCM: 57 | - | Open-door LAMP | - | - | - | No correlation with radiologic parameters |
| Kato S [91] | 2021 | DCM: 109 | - | LAMP |
|
| - |
|
| Kim SW [92] | 2013 | CSM: 28 OPLL: 30 | - | Double-door LAMP (Preoperative C2–C7 angle < 10° vs. ≥10°) | No risk | No risk | - | No difference |
| Sakaura H [93] | 2011 | DCM: 53 | Kyphosis and lordosis were defined as C2–7 angle < 10° and ≥10° | Open-door LAMP (minimum 5-year follow-up) | No risk | No risk | - | No risk |
| Ebata S [94] | 2015 | DCM: 66 | - | Double-door LAMP (Short length of rest with a cervical orthosis: 8, 4, or 2 weeks) | No risk | No risk | - | No difference |
| Matsuoka Y [95] | 2018 | DCM: 84 |
| LAMP | - | Small SVA with lumbar hyper-lordosis (Patients having no preoperative cervical and global spinal sagittal imbalance) | 25.6% | - |
| Wang Z [96] | 2021 | DCM: 68 | - | LAMP (with a plate fixation System) | - | Too high or low preoperative spino cranial angle | - | - |
| Kire N [97] | 2019 | DCM: 110 | - | LAMP (Patients with C2–C7 > 10°, lordotic) | No risk | No risk | - | No risk |
| Kong Q [98] | 2011 | DCM: 76 | - | LAMP (Patients with a straight or lordotic cervical spine) | - | Little space available at cephalad levels is key factor in predicting cord shift distance in laminoplasty | - | Whether the anterior indirect decompression was adequate or not. |
6.2. Laminectomy/Laminoplasty and Posterior Fusion Following the Posterior Approach
6.2.1. Laminectomy and Posterior Fusion for CSM [101,102,103,104,105,106,107] (Table 3)
6.2.2. Laminectomy and Posterior Fusion for OPLL and DCM [108,109,110,111,112,113,114,116] (Table 3)
| 1st Author | Year | Patient’s Number (CSM/OPLL) | Definition of Cervical Deformity | Surgical Techniques (vs. Other Surgical Approach) | Risk Factors of Postoperative Malalignment | Prediction Factors of Postoperative Malalignment before Surgery | Risk Factors of Poor HRQOL Outcome |
|---|---|---|---|---|---|---|---|
| Du W [101] | 2022 | CSM: 117 | C2–7 angle ≤ 0° | Laminectomy with posterior screw fixation (L-F) (vs. Anterior decompression with fusion, ADF) | L-F | - | No difference between ADF and L-F |
| Li XY [102] | 2023 | CSM: 167 | Kyphosis: C2–7 angle < 0° | L-F (vs. ADF and LAMP) | C2–7 angle < 10° | - | - |
| Liu H [103] | 2021 | CSM: 97 | - | L-F (vs. ADF) | L-F | - | Malalignment of C7 slope, occipito-C2 angle, external auditory meatus tilt, and cervical sagittal vertical axis. |
| Lau D [104] | 2017 | CSM: 145 | - | L-F (vs. LAMP) | No difference between L-F and LAMP | - | L-F > LAMP |
| Miyamoto H [105] | 2012 | CSM: 60 (Local kyphosis ≥ 5°) | Local kyphosis ≥ 5° | L-F (vs. LAMP) | LAMP | - | LAMP > L-F |
| Ashana AO [106] | 2021 | CSM: 66 | Kyphosis: C2–7 angle < 0° | L-F (vs. LAMP) | LAMP | -- | L-F = LAMP |
| Lee JJ [107] | 2022 | CSM: 67 | - | L-F (posterior cervical fusion at C5/6 with those at C7/T1.) | End of posterior cervical fusion at C5/6 | - | End of posterior cervical fusion at C5/6 |
| Koda M [108] | 2016 | OPLL: 48 | K-line (+)/(−) | L-F (vs. LAMP) | LAMP for K-line (−) | K-line (−) | LAMP > L-F |
| Nakashima H [109] | 2022 | OPLL: 189 | - | L-F (vs. LAMP) | No difference | No difference | L-F = LAMP |
| Lee CH [110] | 2016 | OPLL: 57 | - | L-F (vs. LAMP) | LAMP | - | LAMP (SVA ≥ 40 mm) |
| Liu X [111] | 2017 | OPLL: 67 | - | L-F (vs. LAMP) | LAMP | - | L-F > LAMP |
| Moon BJ [112] | 2018 | OPLL: 352 | - | L-F (vs. ADF) | - | - |
|
| Perez EA [113] | 2022 | DCM: 198 | - | L-F | BMI > 25 with CSM undergoing P-F (greater increase in SVA) | BMI > 25 with CSM undergoing P-F (greater increase in SVA) | - |
| Schroeder GD [114] | 2016 | DCM: 219 | - | L-F Multilevel posterior cervical fusions ending at C7 vs. T1 vs. T2-T4 | No difference | - | Construct terminated at C7 |
| Kato S [116] | 2018 | DCM: 178 | C2–7 angle < −10° (kyphosis) and/or SVA > 40 mm. | L-F (vs. ADF, combine) |
| Preoperative deformity | Post/Preoperative deformity |
6.3. Anterior Fusion and Posterior Decompression for CSM/OPLL [117,118,119,120,121]
6.4. Others
7. Discussion
8. Conclusions and Outlook
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tundo, F.; Avila, M.J.; Willard, L.; Fanous, S.; Curri, C.; Hussain, I.; Baaj, A.A. Spinal alignment, surgery, and outcomes in cervical deformity: A practical guide to aid the spine surgeon. Clin. Neurol. Neurosurg. 2019, 185, 105496. [Google Scholar] [CrossRef] [PubMed]
- Scheer, J.K.; Tang, J.A.; Smith, J.S.; Acosta, F.L., Jr.; Protopsaltis, T.S.; Blondel, B.; Bess, S.; Shaffrey, C.I.; Deviren, V.; Lafage, V.; et al. Cervical spine alignment, sagittal deformity, and clinical implications: A review. J. Neurosurg. Spine 2013, 19, 141–159. [Google Scholar] [CrossRef] [PubMed]
- Buell, T.J.; Buchholz, A.L.; Quinn, J.C.; Shaffrey, C.I.; Smith, J.S. Importance of Sagittal Alignment of the Cervical Spine in the Management of Degenerative Cervical Myelopathy. Neurosurg. Clin. N. Am. 2018, 29, 69–82. [Google Scholar] [CrossRef]
- Dru, A.B.; Lockney, D.T.; Vaziri, S.; Decker, M.; Polifka, A.J.; Fox, W.C.; Hoh, D.J. Cervical Spine Deformity Correction Techniques. Neurospine 2019, 16, 470–482. [Google Scholar] [CrossRef]
- Funaba, M.; Imajo, Y.; Suzuki, H.; Nishida, N.; Nagao, Y.; Sakamoto, T.; Sakai, T. The radiological characteristics associated with the development of myelopathy due to ossification of the posterior longitudinal ligaments at each responsible level based on spinal cord evoked potentials. Clin. Neurol. Neurosurg. 2020, 194, 105814. [Google Scholar] [CrossRef]
- Funaba, M.; Kanchiku, T.; Yoshida, G.; Imagama, S.; Kawabata, S.; Fujiwara, Y.; Ando, M.; Yamada, K.; Taniguchi, S.; Iwasaki, H.; et al. Efficacy of Intraoperative Neuromonitoring Using Transcranial Motor-Evoked Potentials for Degenerative Cervical Myelopathy: A Prospective Multicenter Study by the Monitoring Committee of the Japanese Society for Spine Surgery and Related Research. Spine 2022, 47, E27–E37. [Google Scholar] [CrossRef]
- Kato, S.; Fehlings, M. Degenerative cervical myelopathy. Curr. Rev. Musculoskelet. Med. 2016, 9, 263–271. [Google Scholar] [CrossRef] [PubMed]
- Ames, C.P.; Smith, J.S.; Eastlack, R.; Blaskiewicz, D.J.; Shaffrey, C.I.; Schwab, F.; Bess, S.; Kim, H.J.; Mundis, G.M., Jr.; Klineberg, E.; et al. Reliability assessment of a novel cervical spine deformity classification system. J. Neurosurg. Spine 2015, 23, 673–683. [Google Scholar] [CrossRef]
- Koller, H.; Ames, C.; Mehdian, H.; Bartels, R.; Ferch, R.; Deriven, V.; Toyone, H.; Shaffrey, C.; Smith, J.; Hitzl, W.; et al. Characteristics of deformity surgery in patients with severe and rigid cervical kyphosis (CK): Results of the CSRS-Europe multi-centre study project. Eur. Spine J. 2019, 28, 324–344. [Google Scholar] [CrossRef]
- Kim, H.J.; Virk, S.; Elysee, J.; Passias, P.; Ames, C.; Shaffrey, C.I.; Mundis, G.; Protopsaltis, T.; Gupta, M.; Klineberg, E.; et al. The morphology of cervical deformities: A two-step cluster analysis to identify cervical deformity patterns. J. Neurosurg. Spine 2019, 15, 353–359. [Google Scholar] [CrossRef]
- Funaba, M.; Imajo, Y.; Suzuki, H.; Nishida, N.; Nagao, Y.; Sakamoto, T.; Fujimoto, K.; Sakai, T. The associations between radiological and neurological findings of degenerative cervical myelopathy: Radiological analysis based on kinematic CT myelography and evoked potentials of the spinal cord. J. Neurosurg. Spine 2021, 35, 308–319. [Google Scholar] [CrossRef] [PubMed]
- Funaba, M.; Imajo, Y.; Suzuki, H.; Nishida, N.; Nagao, Y.; Sakamoto, T.; Fujimoto, K.; Sakai, T. Impact of various MRI signal intensity changes on radiological parameters, the neurological status, and surgical outcomes in degenerative cervical myelopathy. Clin. Neurol. Neurosurg. 2021, 207, 106802. [Google Scholar] [CrossRef] [PubMed]
- Funaba, M.; Suzuki, H.; Imajo, Y.; Nishida, N.; Fujimoto, K.; Ikeda, H.; Sakai, T. Laminoplasty is relevant for degenerative cervical spondylolisthesis when there is little risk of postoperative excessive kyphosis during neck flexion. J. Clin. Neurosci. 2023, 111, 26–31. [Google Scholar] [CrossRef] [PubMed]
- Gibson, J.; Nouri, A.; Krueger, B.; Lakomkin, N.; Nasser, R.; Gimbel, D.; Cheng, J. Degenerative Cervical Myelopathy: A Clinical Review. Yale J. Biol. Med. 2018, 91, 43–48. [Google Scholar] [PubMed]
- Nouri, A.; Tetreault, L.; Singh, A.; Karadimas, S.K.; Fehlings, M.G. Degenerative Cervical Myelopathy: Epidemiology, Genetics, and Pathogenesis. Spine 2015, 40, E675–E693. [Google Scholar] [CrossRef] [PubMed]
- Badhiwala, J.H.; Ahuja, C.S.; Akbar, M.A.; Witiw, C.D.; Nassiri, F.; Furlan, J.C.; Curt, A.; Wilson, J.R.; Fehlings, M.G. Degenerative cervical myelopathy—Update and future directions. Nat. Rev. Neurol. 2020, 16, 108–124. [Google Scholar] [CrossRef]
- Davies, B.M.; Mowforth, O.D.; Smith, E.K.; Kotter, M.R. Degenerative cervical myelopathy. BMJ 2018, 360, k186. [Google Scholar] [CrossRef] [PubMed]
- Lannon, M.; Kachur, E. Degenerative Cervical Myelopathy: Clinical Presentation, Assessment, and Natural History. J. Clin. Med. 2021, 10, 3626. [Google Scholar] [CrossRef]
- Heller, J.G.; Edwards, C.C., II; Murakami, H.; Rodts, G.E. Laminoplasty versus laminectomy and fusion for multilevel cervical myelopathy: An independent matched cohort analysis. Spine 2001, 26, 1330–1336. [Google Scholar] [CrossRef]
- Sakai, K.; Hirai, T.; Arai, Y.; Maehara, H.; Torigoe, I.; Inose, H.; Tomori, M.; Sakaki, K.; Yuasa, M.; Matsukura, Y.; et al. Laminar Closure in Double-door Laminoplasty for Cervical Spondylotic Myelopathy with Nonkyphotic Alignment. Spine 2021, 46, 999–1006. [Google Scholar] [CrossRef]
- Lee, S.H.; Hyun, S.J.; Jain, A. Cervical Sagittal Alignment: Literature Review and Future Directions. Neurospine 2020, 17, 478–496. [Google Scholar] [CrossRef]
- Scheer, J.K.; Lau, D.; Ames, C.P. Sagittal balance of the cervical spine. J. Orthop. Surg. 2021, 29, 23094990211024454. [Google Scholar] [CrossRef]
- Martini, M.L.; Neifert, S.N.; Chapman, E.K.; Mroz, T.E.; Rasouli, J.J. Cervical Spine Alignment in the Sagittal Axis: A Review of the Best Validated Measures in Clinical Practice. Glob. Spine J. 2021, 11, 1307–1312. [Google Scholar] [CrossRef] [PubMed]
- Baker, J.F. Analysis of Sagittal Thoracic Inlet Measures in Relation to Anterior Access to the Cervicothoracic Junction. Glob. Spine J. 2023, 13, 705–712. [Google Scholar] [CrossRef] [PubMed]
- Le Huec, J.C.; Demezon, H.; Aunoble, S. Sagittal parameters of global cervical balance using EOS imaging: Normative values from a prospective cohort of asymptomatic volunteers. Eur. Spine J. 2015, 24, 63–71. [Google Scholar] [CrossRef] [PubMed]
- Weng, C.; Wang, J.; Tuchman, A.; Wang, J.; Fu, C.; Hsieh, P.C.; Buser, Z.; Wang, J.C. Influence of T1 Slope on the Cervical Sagittal Balance in Degenerative Cervical Spine: An Analysis Using Kinematic MRI. Spine 2016, 41, 185–190. [Google Scholar] [CrossRef] [PubMed]
- Le Huec, J.C.; Thompson, W.; Mohsinaly, Y.; Barrey, C.; Faundez, A. Sagittal balance of the spine. Eur. Spine J. 2019, 28, 1889–1905. [Google Scholar] [CrossRef] [PubMed]
- Protopsaltis, T.S.; Lafage, R.; Vira, S.; Sciubba, D.; Soroceanu, A.; Hamilton, K.; Smith, J.; Passias, P.G.; Mundis, G.; Hart, R.; et al. Novel Angular Measures of Cervical Deformity Account for Upper Cervical Compensation and Sagittal Alignment. Clin. Spine Surg. 2017, 30, E959–E967. [Google Scholar] [CrossRef] [PubMed]
- Yoon, S.D.; Lee, C.H.; Lee, J.; Choi, J.Y.; Min, W.K. Occipitocervical inclination: New radiographic parameter of neutral occipitocervical position. Eur. Spine J. 2017, 26, 2297–2302. [Google Scholar] [CrossRef]
- Hashimoto, K.; Miyamoto, H.; Ikeda, T.; Akagi, M. Radiologic features of dropped head syndrome in the overall sagittal alignment of the spine. Eur. Spine J. 2018, 27, 467–474. [Google Scholar] [CrossRef]
- Kim, H.S.; Kim, T.H.; Park, M.S.; Kim, S.W.; Chang, H.G.; Kim, J.H.; Ahn, J.H.; Chang, I.B.; Song, J.H.; Oh, J.K. K-line tilt as a novel radiographic parameter in cervical sagittal alignment. Eur. Spine J. 2018, 27, 2023–2028. [Google Scholar] [CrossRef] [PubMed]
- Choi, S.H.; Lee, D.H.; Hwang, C.J.; Son, S.M.; Woo, Y.; Goh, T.S.; Kang, S.W.; Lee, J.S. Effectiveness of C2 Incidence Angle for Evaluating Global Spinopelvic Alignment in Patients with Mild Degenerative Spondylosis. World Neurosurg. 2019, 127, e826–e834. [Google Scholar] [CrossRef] [PubMed]
- Protopsaltis, T.S.; Stekas, N.; Smith, J.S.; Soroceanu, A.; Lafage, R.; Daniels, A.H.; Kim, H.J.; Passias, P.G.; Mundis, G.M.; Klineberg, E.O.; et al. Surgical outcomes in rigid versus flexible cervical deformities. J. Neurosurg. Spine 2021, 34, 716–724. [Google Scholar] [CrossRef] [PubMed]
- Kawai, S.; Sunago, K.; Doi, K.; Saika, M.; Taguchi, T. Cervical laminoplasty (Hattori’s method). Procedure and follow-up results. Spine (Phila Pa 1976) 1988, 13, 1245–1250. [Google Scholar] [CrossRef] [PubMed]
- Kurokawa, R.; Kim, P. Cervical Laminoplasty: The History and the Future. Neurol. Med. Chir. 2015, 55, 529–539. [Google Scholar] [CrossRef]
- Hirabayashi, K.; Watanabe, K. A Review of My Invention of Expansive Laminoplasty. Neurospine 2019, 16, 379–382. [Google Scholar] [CrossRef]
- Sakai, K.; Yoshii, T.; Hirai, T.; Arai, Y.; Torigoe, I.; Tomori, M.; Sato, H.; Okawa, A. Cervical Sagittal Imbalance is a Predictor of Kyphotic Deformity After Laminoplasty in Cervical Spondylotic Myelopathy Patients Without Preoperative Kyphotic Alignment. Spine 2016, 41, 299–305. [Google Scholar] [CrossRef]
- Oe, S.; Kurosu, K.; Hasegawa, T.; Shimizu, S.; Yoshida, G.; Fujita, T.; Kobayashi, S.; Yamada, T.; Ide, K.; Nakai, K.; et al. Risk Factors for Cervical Deformity After Posterior Cervical Decompression Surgery: A Multicenter Study. Glob. Spine J. 2023, 13, 1457–1466. [Google Scholar] [CrossRef]
- Kim, B.J.; Cho, S.M.; Hur, J.W.; Cha, J.; Kim, S.H. Kinematics after cervical laminoplasty: Risk factors for cervical kyphotic deformity after laminoplasty. Spine J. 2021, 21, 1822–1829. [Google Scholar] [CrossRef] [PubMed]
- Abe, T.; Miyazaki, M.; Ishihara, T.; Kanezaki, S.; Notani, N.; Kataoka, M.; Tsumura, H. Analysis of the risk factors for increasing cervical sagittal vertical axis after cervical laminoplasty for cervical spondylotic myelopathy. Arch. Orthop. Trauma Surg. 2022, 142, 553–560. [Google Scholar] [CrossRef] [PubMed]
- Ninomiya, K.; Yamane, J.; Aoyama, R.; Suzuki, S.; Shiono, Y.; Takahashi, Y.; Fujita, N.; Okada, E.; Tsuji, O.; Yagi, M.; et al. Clinical Effects of Anterior Cervical Spondylolisthesis on Cervical Spondylotic Myelopathy After Posterior Decompression Surgery: A Retrospective Multicenter Study of 732 Cases. Glob. Spine J. 2022, 12, 820–828. [Google Scholar] [CrossRef]
- Zhang, H.; Lu, S.; Sun, T.; Yadav, S.K. Effect of lamina open angles in expansion open-door laminoplasty on the clinical results in treating cervical spondylotic myelopathy. J. Spinal Disord. Tech. 2015, 28, 89–94. [Google Scholar] [CrossRef] [PubMed]
- Nurboja, B.; Kachramanoglou, C.; Choi, D. Cervical laminectomy vs laminoplasty: Is there a difference in outcome and postoperative pain? Neurosurgery 2012, 70, 965–970, discussion 970. [Google Scholar] [CrossRef] [PubMed]
- Guo, Q.; Xu, Y.; Fang, Z.; Guan, H.; Xiong, W.; Li, F. Clinical and Radiological Outcomes of Two Modified Open-door Laminoplasties Based on a Novel Paraspinal Approach for Treatment of Multilevel Cervical Spondylotic Myelopathy. Spine 2022, 47, E222–E232. [Google Scholar] [CrossRef] [PubMed]
- Lee, D.G.; Lee, S.H.; Park, S.J.; Kim, E.S.; Chung, S.S.; Lee, C.S.; Eoh, W. Comparison of surgical outcomes after cervical laminoplasty: Open-door technique versus French-door technique. J. Spinal Disord. Tech. 2013, 26, E198–E203. [Google Scholar] [CrossRef] [PubMed]
- Nori, S.; Aoyama, R.; Ninomiya, K.; Suzuki, S.; Anazawa, U.; Shiraishi, T. Does K-line (-) in the Neck-flexed Position Predict Surgical Outcome of Cervical Spondylotic Myelopathy?: Results of a Multivariate Analysis After Muscle-preserving Selective Laminectomy. Spine 2020, 45, E1225–E1231. [Google Scholar] [CrossRef] [PubMed]
- Jain, A.; Rustagi, T.; Prasad, G.; Deore, T.; Bhojraj, S.Y. Does Segmental Kyphosis Affect Surgical Outcome after a Posterior Decompressive Laminectomy in Multisegmental Cervical Spondylotic Myelopathy? Asian Spine J. 2017, 11, 24–30. [Google Scholar] [CrossRef]
- Liu, C.; Shi, B.; Wang, W.; Li, X.; Lu, S. Effect of preoperative dynamic cervical sagittal alignment on the loss of cervical lordosis after laminoplasty. BMC Musculoskelet. Disord. 2023, 24, 233. [Google Scholar] [CrossRef]
- Fujishiro, T.; Hayama, S.; Obo, T.; Nakaya, Y.; Nakano, A.; Usami, Y.; Nozawa, S.; Baba, I.; Neo, M. Gap between flexion and extension ranges of motion: A novel indicator to predict the loss of cervical lordosis after laminoplasty in patients with cervical spondylotic myelopathy. J. Neurosurg. Spine 2021, 35, 8–17. [Google Scholar] [CrossRef]
- Lin, B.J.; Lin, M.C.; Lin, C.; Lee, M.S.; Feng, S.W.; Ju, D.T.; Ma, H.I.; Liu, M.Y.; Hueng, D.Y. Image analysis of open-door laminoplasty for cervical spondylotic myelopathy: Comparing the influence of cord morphology and spine alignment. Clin. Neurol. Neurosurg. 2015, 137, 72–78. [Google Scholar] [CrossRef]
- Chen, H.Y.; Yang, M.H.; Lin, Y.P.; Lin, F.H.; Chen, P.Q.; Hu, M.H.; Yang, S.H. Impact of cervical sagittal parameters and spinal cord morphology in cervical spondylotic myelopathy status post spinous process-splitting laminoplasty. Eur. Spine J. 2020, 29, 1052–1060. [Google Scholar] [CrossRef]
- Takasawa, E.; Iizuka, Y.; Ishiwata, S.; Kakuta, Y.; Inomata, K.; Tomomatsu, Y.; Ito, S.; Honda, A.; Mieda, T.; Chikuda, H. Impact of the preoperative nutritional status on postoperative kyphosis in geriatric patients undergoing cervical laminoplasty. Eur. Spine J. 2023, 32, 374–381. [Google Scholar] [CrossRef]
- Wang, Z.; Wang, Z.W.; Fan, X.W.; Liu, Z.; Sun, J.Y.; Ding, W.Y.; Yang, D.L. Influence of SCA on clinical outcomes and cervical alignment after laminoplasty in patients with multilevel cervical spondylotic myelopathy. J. Orthop. Surg. Res. 2021, 16, 49. [Google Scholar] [CrossRef]
- Ikeda, T.; Miyamoto, H.; Akagi, M. Usefulness of K-line in predicting prognosis of laminoplasty for cervical spondylotic myelopathy. BMC Musculoskelet. Disord. 2023, 24, 118. [Google Scholar] [CrossRef]
- Nori, S.; Nagoshi, N.; Suzuki, S.; Tsuji, O.; Okada, E.; Yagi, M.; Nakamura, M.; Matsumoto, M.; Watanabe, K. K-line (-) in the neck-flexed position negatively affects surgical outcome of expansive open-door laminoplasty for cervical spondylotic myelopathy. J. Orthop. Sci. 2022, 27, 551–557. [Google Scholar] [CrossRef]
- Cao, J.; Zhang, J.; Yang, D.; Yang, L.; Shen, Y. Multivariate analysis of factors associated with kyphotic deformity after laminoplasty in cervical spondylotic myelopathy patients without preoperative kyphotic alignment. Sci. Rep. 2017, 7, 43443. [Google Scholar] [CrossRef]
- Kurihara, K.; Iba, K.; Teramoto, A.; Emori, M.; Hirota, R.; Oshigiri, T.; Ogon, I.; Iesato, N.; Terashima, Y.; Takashima, H.; et al. Effect of Minimally Invasive Selective Laminectomy for Cervical Spondylotic Myelopathy on Degenerative Spondylolisthesis. Clin. Spine Surg. 2022, 35, E242–E247. [Google Scholar] [CrossRef]
- Laiginhas, A.R.; Silva, P.A.; Pereira, P.; Vaz, R. Long-term clinical and radiological follow-up after laminectomy for cervical spondylotic myelopathy. Surg. Neurol. Int. 2015, 6, 162. [Google Scholar] [CrossRef]
- Minamide, A.; Yoshida, M.; Simpson, A.K.; Yamada, H.; Hashizume, H.; Nakagawa, Y.; Iwasaki, H.; Tsutsui, S.; Okada, M.; Takami, M.; et al. Microendoscopic laminotomy versus conventional laminoplasty for cervical spondylotic myelopathy: 5-year follow-up study. J. Neurosurg. Spine 2017, 27, 403–409. [Google Scholar] [CrossRef]
- Taniyama, T.; Hirai, T.; Yoshii, T.; Yamada, T.; Yasuda, H.; Saito, M.; Inose, H.; Kato, T.; Kawabata, S.; Okawa, A. Modified K-line in magnetic resonance imaging predicts clinical outcome in patients with nonlordotic alignment after laminoplasty for cervical spondylotic myelopathy. Spine 2014, 39, E1261–E1268. [Google Scholar] [CrossRef]
- Ninomiya, K.; Okuyama, K.; Aoyama, R.; Nori, S.; Yamane, J.; Suzuki, S.; Kitamura, K.; Anazawa, U.; Furukawa, M.; Shiraishi, T.; et al. Surgical Outcomes of Selective Laminectomy for Patients with Cervical Kyphosis: A Retrospective Study of 379 Cases. Glob. Spine J. 2023, 13, 1777–1786. [Google Scholar] [CrossRef]
- Chen, G.; Jia, M.; Connel, R.K.; Sheng, Y.; Lin, C.; Huang, K.; Ying, J.; Teng, H. Nomogram for predicting kyphotic deformity after laminoplasty in cervical spondylotic myelopathy patients without preoperative kyphotic alignment. Clin. Neurol. Neurosurg. 2020, 199, 106284. [Google Scholar] [CrossRef]
- Machino, M.; Ando, K.; Kobayashi, K.; Morozumi, M.; Tanaka, S.; Kanbara, S.; Ito, S.; Inoue, T.; Ito, K.; Kato, F.; et al. Postoperative Kyphosis in Cervical Spondylotic Myelopathy: Cut-off Preoperative Angle for Predicting the Postlaminoplasty Kyphosis. Spine 2020, 45, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Yang, Y.; Qu, R.; Liu, Z.; Chen, Z.; Wu, Y.; Chu, H.; Liu, Z.; Liu, X.; Jiang, L. Predicting post-laminoplasty kyphosis in cervical spondylotic myelopathy patients without preoperative kyphosis: A retrospective study. BMC Musculoskelet. Disord. 2023, 24, 526. [Google Scholar] [CrossRef]
- Zhang, J.T.; Li, J.Q.; Niu, R.J.; Liu, Z.; Tong, T.; Shen, Y. Predictors of cervical lordosis loss after laminoplasty in patients with cervical spondylotic myelopathy. Eur. Spine J. 2017, 26, 1205–1210. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, T.; Fujibayashi, S.; Otsuki, B.; Murata, K.; Masuda, S.; Matsuda, S. Residual anterior cord compression after laminoplasty for cervical spondylotic myelopathy: Evaluation of risk factors according to the most severely stenotic vertebral segment. J. Neurosurg. Spine 2022, 37, 794–801. [Google Scholar] [CrossRef] [PubMed]
- Obo, T.; Fujishiro, T.; Mizutani, M.; Nakano, A.; Nakaya, Y.; Hayama, S.; Usami, Y.; Neo, M. Segmental cervical instability does not drive the loss of cervical lordosis after laminoplasty in patients with cervical spondylotic myelopathy. Spine J. 2022, 22, 1837–1847. [Google Scholar] [CrossRef]
- Chang, H.; Kim, C.; Choi, B.W. Selective laminectomy for cervical spondylotic myelopathy: A comparative analysis with laminoplasty technique. Arch. Orthop. Trauma Surg. 2017, 137, 611–616. [Google Scholar] [CrossRef]
- Sivaraman, A.; Bhadra, A.K.; Altaf, F.; Singh, A.; Rai, A.; Casey, A.T.; Crawford, R.J. Skip laminectomy and laminoplasty for cervical spondylotic myelopathy: A prospective study of clinical and radiologic outcomes. J. Spinal Disord. Tech. 2010, 23, 96–100. [Google Scholar] [CrossRef]
- Nagoshi, N.; Nori, S.; Tsuji, O.; Suzuki, S.; Okada, E.; Yagi, M.; Nakamura, M.; Matsumoto, M.; Watanabe, K. Surgical and Functional Outcomes of Expansive Open-Door Laminoplasty for Patients with Mild Kyphotic Cervical Alignment. Neurospine 2021, 18, 749–757. [Google Scholar] [CrossRef]
- Rao, H.; Huang, Y.; Lan, Z.; Xu, Z.; Li, G.; Xu, W. Does Preoperative T1 Slope and Cervical Lordosis Mismatching Affect Surgical Outcomes After Laminoplasty in Patients with Cervical Spondylotic Myelopathy? World Neurosurg. 2019, 130, e687–e693. [Google Scholar] [CrossRef]
- Machino, M.; Ando, K.; Kobayashi, K.; Ito, K.; Tsushima, M.; Matsumoto, A.; Morozumi, M.; Tanaka, S.; Ito, K.; Kato, F.; et al. The Feature of Clinical and Radiographic Outcomes in Elderly Patients with Cervical Spondylotic Myelopathy: A Prospective Cohort Study on 1025 Patients. Spine 2018, 43, 817–823. [Google Scholar] [CrossRef]
- Yeh, K.T.; Lee, R.P.; Chen, I.H.; Yu, T.C.; Peng, C.H.; Liu, K.L.; Wang, J.H.; Wu, W.T. The Midterm Surgical Outcome of Modified Expansive Open-Door Laminoplasty. Biomed. Res. Int. 2016, 2016, 8069354. [Google Scholar] [CrossRef]
- Kanbara, S.; Imagama, S.; Ito, K.; Ito, K.; Ishiguro, N.; Kato, F. A retrospective imaging study of surgical outcomes and range of motion in patients with cervical ossification of the posterior longitudinal ligament. Eur. Spine J. 2018, 27, 1416–1422. [Google Scholar] [CrossRef]
- Kawaguchi, Y.; Nakano, M.; Yasuda, T.; Seki, S.; Suzuki, K.; Yahara, Y.; Makino, H.; Kobayashi, K.; Kanamori, M.; Kimura, T. Clinical Impact of Ossification of the Posterior Longitudinal Ligament Progression after Cervical Laminoplasty. Clin. Spine Surg. 2019, 32, E133–E139. [Google Scholar] [CrossRef]
- Chen, Z.; Liu, B.; Dong, J.; Feng, F.; Chen, R.; Xie, P.; Zhang, L.; Rong, L. Comparison of anterior corpectomy and fusion versus laminoplasty for the treatment of cervical ossification of posterior longitudinal ligament: A meta-analysis. Neurosurg. Focus 2016, 40, E8. [Google Scholar] [CrossRef]
- Kim, B.; Yoon, D.H.; Ha, Y.; Yi, S.; Shin, D.A.; Lee, C.K.; Lee, N.; Kim, K.N. Relationship between T1 slope and loss of lordosis after laminoplasty in patients with cervical ossification of the posterior longitudinal ligament. Spine J. 2016, 16, 219–225. [Google Scholar] [CrossRef]
- Liu, X.; Li, T.; Shi, L.; Luo, Y.; Chen, D.; Xu, B.; Chen, Y. Extended Laminoplasty for Ossification of Posterior Longitudinal Ligament Involving the C2 Segment. World Neurosurg. 2019, 130, 317–323. [Google Scholar] [CrossRef]
- Nakashima, H.; Imagama, S.; Yoshii, T.; Egawa, S.; Sakai, K.; Kusano, K.; Tsutsui, S.; Hirai, T.; Matsukura, Y.; Wada, K.; et al. Factors Associated with Loss of Cervical Lordosis After Laminoplasty for Patients with Cervical Ossification of the Posterior Longitudinal Ligament: Data From a Prospective Multicenter Study. Spine 2023, 48, 1047–1056. [Google Scholar] [CrossRef]
- Li, C.; Zha, G.; Yang, Z.; Pang, Y.; Qiu, S.; Fan, W.; Liu, Y.; Jiang, W. K-line in patients with cervical ossification of the posterior longitudinal ligament: Relationship with change in sagittal cervical curvature and laminoplasty outcomes. Arch. Orthop. Trauma Surg. 2022, 142, 1743–1751. [Google Scholar] [CrossRef]
- Sakai, K.; Yoshii, T.; Arai, Y.; Hirai, T.; Torigoe, I.; Inose, H.; Tomori, M.; Sakaki, K.; Yuasa, M.; Yamada, T.; et al. K-Line Tilt is a Predictor of Postoperative Kyphotic Deformity After Laminoplasty for Cervical Myelopathy Caused by Ossification of the Posterior Longitudinal Ligament. Glob. Spine J. 2023, 13, 1005–1010. [Google Scholar] [CrossRef]
- Yoo, S.; Ryu, D.; Choi, H.J.; Kuh, S.U.; Chin, D.K.; Kim, K.S.; Cho, Y.E. Ossification foci act as stabilizers in continuous-type ossification of the posterior longitudinal ligament: A comparative study between laminectomy and laminoplasty. Acta Neurochir. 2017, 159, 1783–1790. [Google Scholar] [CrossRef]
- Saito, J.; Koda, M.; Furuya, T.; Maki, S.; Ijima, Y.; Kitamura, M.; Miyamoto, T.; Orita, S.; Inage, K.; Hasue, F.; et al. Segmental motion at the peak of the ossification foci is independent risk factor except for mal-alignment and thick ossification foci for poor outcome after laminoplasty for cervical ossification of the posterior longitudinal ligament: Analyses in patients with positive K-line, lordotic alignment, and lower canal occupying ratio. J. Orthop. Surg. Res. 2020, 15, 407. [Google Scholar] [CrossRef]
- Xu, C.; Zhang, Y.; Dong, M.; Wu, H.; Yu, W.; Tian, Y.; Cao, P.; Chen, H.; Wang, X.; Shen, X.; et al. The relationship between preoperative cervical sagittal balance and clinical outcome of laminoplasty treated cervical ossification of the posterior longitudinal ligament patients. Spine J. 2020, 20, 1422–1429. [Google Scholar] [CrossRef]
- Kim, S.W.; Jang, S.B.; Lee, H.M.; Lee, J.H.; Lee, M.U.; Kim, J.W.; Yee, J.S. Analysis of Cervical Spine Alignment and its Relationship with Other Spinopelvic Parameters After Laminoplasty in Patients with Degenerative Cervical Myelopathy. J. Clin. Med. 2020, 9, 713. [Google Scholar] [CrossRef] [PubMed]
- Shimizu, K.; Mitsuhara, T.; Takeda, M.; Kurisu, K.; Yamaguchi, S. Effects of Preservation of the Semispinalis Cervicis Inserted into C2 on Craniocervical Alignment after Laminoplasty. World Neurosurg. 2021, 146, e1367–e1376. [Google Scholar] [CrossRef]
- Chen, H.; Deng, Y.; Li, T.; Gong, Q.; Song, Y.; Liu, H. Clinical and radiography results of mini-plate fixation compared to suture suspensory fixation in cervical laminoplasty: A five-year follow-up study. Clin. Neurol. Neurosurg. 2015, 138, 188–195. [Google Scholar] [CrossRef] [PubMed]
- Sakamoto, R.; Nakamoto, H.; Yoshida, Y.; Ohtomo, N.; Nagata, K.; Kato, S.; Doi, T.; Matsubayashi, Y.; Taniguchi, Y.; Tanaka, S.; et al. Does T1 slope minus cervical lordosis mismatch affect surgical outcomes of cervical laminoplasty in the absence of preoperative severe kyphosis? BMC Musculoskelet. Disord. 2022, 23, 810. [Google Scholar] [CrossRef]
- Qian, S.; Wang, Z.; Jiang, G.; Xu, Z.; Chen, W. Efficacy of Laminoplasty in Patients with Cervical Kyphosis. Med. Sci. Monit. 2018, 24, 1188–1195. [Google Scholar] [CrossRef]
- Fujiwara, H.; Oda, T.; Makino, T.; Moriguchi, Y.; Yonenobu, K.; Kaito, T. Impact of Cervical Sagittal Alignment on Axial Neck Pain and Health-related Quality of Life After Cervical Laminoplasty in Patients with Cervical Spondylotic Myelopathy or Ossification of the Posterior Longitudinal Ligament: A Prospective Comparative Study. Clin. Spine Surg. 2018, 31, E245–E251. [Google Scholar] [CrossRef]
- Kato, S.; Mihara, H.; Niimura, T.; Watanabe, K.; Kawai, T.; Choe, H.; Inaba, Y. Impact of focal apex angle on postoperative decompression status of the spinal cord and neurological recovery after cervical laminoplasty. J. Neurosurg. Spine 2021, 35, 410–418. [Google Scholar] [CrossRef]
- Kim, S.W.; Hai, D.M.; Sundaram, S.; Kim, Y.C.; Park, M.S.; Paik, S.H.; Kwak, Y.H.; Kim, T.H. Is cervical lordosis relevant in laminoplasty? Spine J. 2013, 13, 914–921. [Google Scholar] [CrossRef] [PubMed]
- Sakaura, H.; Hosono, N.; Mukai, Y.; Iwasaki, M.; Yoshikawa, H. Medium-term outcomes of C3-6 laminoplasty for cervical myelopathy: A prospective study with a minimum 5-year follow-up. Eur. Spine J. 2011, 20, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Ebata, S.; Sato, H.; Ohba, T.; Ando, T.; Haro, H. Postoperative intervertebral stabilizing effect after cervical laminoplasty. J. Back Musculoskelet. Rehabil. 2015, 28, 303–309. [Google Scholar] [CrossRef] [PubMed]
- Matsuoka, Y.; Suzuki, H.; Endo, K.; Sawaji, Y.; Murata, K.; Nishimura, H.; Tanaka, H.; Yamamoto, K. Small sagittal vertical axis accompanied with lumbar hyperlordosis as a risk factor for developing postoperative cervical kyphosis after expansive open-door laminoplasty. J. Neurosurg. Spine 2018, 29, 176–181. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Xu, J.X.; Liu, Z.; Li, R.Y.; Wang, Z.W.; Chang, H.R.; Ding, W.Y.; Yang, D.L. Spino cranial angle as a predictor of loss of cervical lordosis after laminoplasty in patients with cervical myelopathy. BMC Surg. 2021, 21, 291. [Google Scholar] [CrossRef] [PubMed]
- Kire, N.; Jain, S.; Merchant, Z.A.; Kundnani, V. The Efficacy of Posterior Cervical Laminectomy for Multilevel Degenerative Cervical Spondylotic Myelopathy in Long Term Period. Asian J. Neurosurg. 2019, 14, 848–852. [Google Scholar] [CrossRef]
- Kong, Q.; Zhang, L.; Liu, L.; Li, T.; Gong, Q.; Zeng, J.; Song, Y.; Liu, H.; Wang, S.; Sun, Y.; et al. Effect of the decompressive extent on the magnitude of the spinal cord shift after expansive open-door laminoplasty. Spine 2011, 36, 1030–1036. [Google Scholar] [CrossRef]
- Funaba, M.; Imajo, Y.; Suzuki, H.; Nishida, N.; Sakamoto, T.; Sakai, T. The Deterioration of Cervical Kyphosis During Neck Flexion after Laminoplasty Affects the Surgical Outcome of Cervical Spondylotic Myelopathy. Glob. Spine J. 2023, 13, 2497–2507. [Google Scholar] [CrossRef]
- Sakamoto, T.; Funaba, M.; Imajo, Y.; Nagao, Y.; Suzuki, H.; Nishida, N.; Fujimoto, K.; Sakai, T. The Impact of Anterior Spondylolisthesis and Kyphotic Alignment on Dynamic Changes in Spinal Cord Compression and Neurological Status in Cervical Spondylotic Myelopathy: A Radiological Analysis Involving Kinematic CT Myelography and Multimodal Spinal Cord Evoked Potentials. Spine 2021, 46, 72–79. [Google Scholar] [CrossRef]
- Du, W.; Wang, H.X.; Zhang, J.T.; Wang, F.; Zhang, X.; Shen, Y.; Chen, R.; Zhang, L. Cervical alignment and clinical outcome of anterior decompression with fusion vs. posterior decompression with fixation in kyphotic cervical spondylotic myelopathy. Front. Neurosci. 2022, 16, 1029327. [Google Scholar] [CrossRef]
- Li, X.Y.; Wang, Y.; Zhu, W.G.; Liu, C.X.; Kong, C.; Lu, S.B. Cervical sagittal alignment changes following anterior cervical discectomy and fusion, laminectomy with fusion, and laminoplasty for multisegmental cervical spondylotic myelopathy. J. Orthop. Surg. Res. 2023, 18, 190. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Li, X.; Wang, J.; Li, Z.; Li, Z.; Chen, S.; Wang, H.; Zheng, Z. Comparison study of clinical outcomes and sagittal alignment improvement between anterior and posterior fusion techniques for multilevel cervical spondylotic myelopathy. J. Orthop. Surg. 2021, 29, 2309499020988177. [Google Scholar] [CrossRef]
- Lau, D.; Winkler, E.A.; Than, K.D.; Chou, D.; Mummaneni, P.V. Laminoplasty versus laminectomy with posterior spinal fusion for multilevel cervical spondylotic myelopathy: Influence of cervical alignment on outcomes. J. Neurosurg. Spine 2017, 27, 508–517. [Google Scholar] [CrossRef]
- Miyamoto, H.; Maeno, K.; Uno, K.; Kakutani, K.; Nishida, K.; Sumi, M. Outcomes of surgical intervention for cervical spondylotic myelopathy accompanying local kyphosis (comparison between laminoplasty alone and posterior reconstruction surgery using the screw-rod system). Eur. Spine J. 2014, 23, 341–346. [Google Scholar] [CrossRef]
- Ashana, A.O.; Ajiboye, R.M.; Sheppard, W.L.; Ishmael, C.R.; Cohen, J.Y.; Beckett, J.S.; Holly, L.T. Spinal Cord Drift Following Laminoplasty Versus Laminectomy and Fusion for Cervical Spondylotic Myelopathy. Int. J. Spine Surg. 2021, 15, 205–212. [Google Scholar] [CrossRef]
- Lee, J.J.; Park, J.H.; Oh, Y.G.; Shin, H.K.; Jung, S.K. Should cervicothoracic junctions be avoided in long cervical posterior fusion surgery? Analysis of clinical and radiologic outcomes over two years. J. Orthop. Surg. 2022, 30, 10225536221137751. [Google Scholar] [CrossRef]
- Koda, M.; Mochizuki, M.; Konishi, H.; Aiba, A.; Kadota, R.; Inada, T.; Kamiya, K.; Ota, M.; Maki, S.; Takahashi, K.; et al. Comparison of clinical outcomes between laminoplasty, posterior decompression with instrumented fusion, and anterior decompression with fusion for K-line (-) cervical ossification of the posterior longitudinal ligament. Eur. Spine J. 2016, 25, 2294–2301. [Google Scholar] [CrossRef]
- Nakashima, H.; Imagama, S.; Yoshii, T.; Egawa, S.; Sakai, K.; Kusano, K.; Nakagawa, Y.; Hirai, T.; Wada, K.; Katsumi, K.; et al. Comparison of laminoplasty and posterior fusion surgery for cervical ossification of posterior longitudinal ligament. Sci. Rep. 2022, 12, 748. [Google Scholar] [CrossRef]
- Lee, C.H.; Jahng, T.A.; Hyun, S.J.; Kim, K.J.; Kim, H.J. Expansive Laminoplasty Versus Laminectomy Alone Versus Laminectomy and Fusion for Cervical Ossification of the Posterior Longitudinal Ligament: Is There a Difference in the Clinical Outcome and Sagittal Alignment? Clin. Spine Surg. 2016, 29, E9–E15. [Google Scholar] [CrossRef]
- Liu, X.; Chen, Y.; Yang, H.; Li, T.; Xu, B.; Chen, D. Expansive open-door laminoplasty versus laminectomy and instrumented fusion for cases with cervical ossification of the posterior longitudinal ligament and straight lordosis. Eur. Spine J. 2017, 26, 1173–1180. [Google Scholar] [CrossRef]
- Moon, B.J.; Kim, D.; Shin, D.A.; Yi, S.; Kim, K.N.; Yoon, D.H.; Ha, Y. Patterns of short-term and long-term surgical outcomes and prognostic factors for cervical ossification of the posterior longitudinal ligament between anterior cervical corpectomy and fusion and posterior laminoplasty. Neurosurg. Rev. 2019, 42, 907–913. [Google Scholar] [CrossRef] [PubMed]
- Perez, E.A.; Woodroffe, R.W.; Park, B.; Gold, C.; Helland, L.C.; Seaman, S.C.; Hitchon, P.W. Cervical alignment in the obese population following posterior cervical fusion for cervical myelopathy. Clin. Neurol. Neurosurg. 2022, 212, 107059. [Google Scholar] [CrossRef]
- Schroeder, G.D.; Kepler, C.K.; Kurd, M.F.; Mead, L.; Millhouse, P.W.; Kumar, P.; Nicholson, K.; Stawicki, C.; Helber, A.; Fasciano, D.; et al. Is It Necessary to Extend a Multilevel Posterior Cervical Decompression and Fusion to the Upper Thoracic Spine? Spine 2016, 41, 1845–1849. [Google Scholar] [CrossRef]
- Hirano, Y.; Ohara, Y.; Mizuno, J.; Itoh, Y. History and Evolution of Laminoplasty. Neurosurg. Clin. N. Am. 2018, 29, 107–113. [Google Scholar] [CrossRef]
- Kato, S.; Nouri, A.; Wu, D.; Nori, S.; Tetreault, L.; Fehlings, M.G. Impact of Cervical Spine Deformity on Preoperative Disease Severity and Postoperative Outcomes Following Fusion Surgery for Degenerative Cervical Myelopathy: Sub-analysis of AOSpine North America and International Studies. Spine 2018, 43, 248–254. [Google Scholar] [CrossRef]
- Zhou, X.; Cai, P.; Li, Y.; Wang, H.; Xia, S.; Wang, X. Posterior or Single-stage Combined Anterior and Posterior Approach Decompression for Treating Complex Cervical Spondylotic Myelopathy Coincident Multilevel Anterior and Posterior Compression. Clin. Spine Surg. 2017, 30, E1343–E1351. [Google Scholar] [CrossRef]
- Yeh, K.T.; Lee, R.P.; Chen, I.H.; Yu, T.C.; Peng, C.H.; Liu, K.L.; Wang, J.H.; Wu, W.T. Laminoplasty with adjunct anterior short segment fusion for multilevel cervical myelopathy associated with local kyphosis. J. Chin. Med. Assoc. 2015, 78, 364–369. [Google Scholar] [CrossRef]
- Sun, K.; Wang, S.; Huan, L.; Sun, J.; Xu, X.; Sun, X.; Shi, J.; Guo, Y. Analysis of the spinal cord angle for severe cervical ossification of the posterior longitudinal ligament: Comparison between anterior controllable antedisplacement and fusion (ACAF) and posterior laminectomy. Eur. Spine J. 2020, 29, 1001–1012. [Google Scholar] [CrossRef]
- Li, Y.C.; Liu, Z.H.; Li, Y.S.; Yeap, M.C.; Liu, Y.T.; Huang, Y.C.; Chen, C.C.; Tu, P.H. The surgical strategy for multilevel massive ossification of the posterior longitudinal ligaments. Front. Surg. 2022, 9, 1066120. [Google Scholar] [CrossRef]
- Shin, J.J.; Jeon, H.; Lee, J.J.; Kim, H.C.; Kim, T.W.; An, S.B.; Shin, D.A.; Yi, S.; Kim, K.N.; Yoon, D.H.; et al. Predictors of neurologic outcome after surgery for cervical ossification of the posterior longitudinal ligament differ based on myelopathy severity: A multicenter study. J. Neurosurg. Spine 2021, 34, 749–758. [Google Scholar] [CrossRef]
- Yagi, M.; Ninomiya, K.; Kihara, M.; Horiuchi, Y. Long-term surgical outcome and risk factors in patients with cervical myelopathy and a change in signal intensity of intramedullary spinal cord on Magnetic Resonance imaging. J. Neurosurg. Spine 2010, 12, 59–65. [Google Scholar] [CrossRef]
- Nishida, N.; Kanchiku, T.; Imajo, Y.; Suzuki, H.; Yoshida, Y.; Kato, Y.; Nakashima, D.; Taguchi, T. Stress analysis of the cervical spinal cord: Impact of the morphology of spinal cord segments on stress. J. Spinal Cord Med. 2016, 39, 327–334. [Google Scholar] [CrossRef]
- Nishida, N.; Jiang, F.; Asano, T.; Tome, R.; Kumaran, Y.; Imajo, Y.; Suzuki, H.; Funaba, M.; Ohgi, J.; Chen, X.; et al. Effect of posterior decompression with and without fixation on a kyphotic cervical spine with ossification of the posterior longitudinal ligament. Spinal Cord 2023, 61, 133–138. [Google Scholar] [CrossRef]
- Oshima, Y.; Kato, S.; Doi, T.; Matsubayashi, Y.; Taniguchi, Y.; Tanaka, S. Comparison of microendoscopic selective laminectomy versus conventional laminoplasty in patients with degenerative cervcical myelopathy: A minimum 2-year follow-up study. BMC Musculoskelet. Disord. 2019, 20, 471. [Google Scholar] [CrossRef]
- Chavanne, A.; Pettigrew, D.B.; Holtz, J.R.; Dollin, N.; Kuntz, C., IV. Spinal cord intramedullary pressure in cervical kyphotic deformity: A cadaveric study. Spine 2011, 36, 1619–1626. [Google Scholar] [CrossRef]
- Kato, S.; Nouri, A.; Wu, D.; Nori, S.; Tetreault, L.; Fehlings, M.G. Comparison of Anterior and Posterior Surgery for Degenerative Cervical Myelopathy: An MRI-Based Propensity-Score-Matched Analysis Using Data from the Prospective Multicenter AOSpine CSM North America and International Studies. J. Bone Jt. Surg. Am. 2017, 99, 1013–1021. [Google Scholar] [CrossRef]
- Ghogawala, Z.; Terrin, N.; Dunbar, M.R.; Breeze, J.L.; Freund, K.M.; Kanter, A.S.; Mummaneni, P.V.; Bisson, E.F.; Barker, F.G., II; Schwartz, J.S.; et al. Effect of Ventral vs Dorsal Spinal Surgery on Patient-Reported Physical Functioning in Patients with Cervical Spondylotic Myelopathy: A Randomized Clinical Trial. JAMA 2021, 325, 942–951. [Google Scholar] [CrossRef]
- Hasegawa, K.; Dubousset, J.F. Cone of Economy with the Chain of Balance-Historical Perspective and Proof of Concept. Spine Surg. Relat. Res. 2022, 6, 337–349. [Google Scholar] [CrossRef]
- Hasegawa, K.; Okamoto, M.; Hatsushikano, S.; Shimoda, H.; Ono, M.; Homma, T.; Watanabe, K. Standing sagittal alignment of the whole axial skeleton with reference to the gravity line in humans. J. Anat. 2017, 230, 619–630. [Google Scholar] [CrossRef]
- Hasegawa, K.; Hatsushikano, S.; Watanabe, K.; Ohashi, M.; Dubousset, J. Scoliosis Research Society-22r score is affected by standing whole body sagittal alignment, age, and sex, but not by standing balance or skeletal muscle mass in healthy volunteers. Eur. Spine J. 2022, 31, 3000–3012. [Google Scholar] [CrossRef] [PubMed]
- Hasegawa, K.; Okamoto, M.; Hatsushikano, S.; Watanabe, K.; Ohashi, M.; Vital, J.M.; Dubousset, J. Compensation for standing posture by whole-body sagittal alignment in relation to health-related quality of life. Bone Jt. J. 2020, 102-B, 1359–1367. [Google Scholar] [CrossRef] [PubMed]
- Oakley, P.A.; Ehsani, N.N.; Moustafa, I.M.; Harrison, D.E. Restoring cervical lordosis by cervical extension traction methods in the treatment of cervical spine disorders: A systematic review of controlled trials. J. Phys. Ther. Sci. 2021, 33, 784–794. [Google Scholar] [CrossRef] [PubMed]


| Parameter | Measurement Description | Reference |
|---|---|---|
| Neck tilt | The angle formed by a line drawn from the upper end of the sternum and a line connecting the center of the T1 upper endplate (UEP) | [21] |
| Thoracic inlet angle | The angle formed by a line from the center of the T1UEP vertical to the T1UEP and a line connecting the center of the T1UEP and the upper end of the sternum. | [24] |
| Cranial incidence | The angle between the center of the line perpendicular to the McGregor line and the line that joins the middle of the McGregor line to the sella turcica | [25] |
| Cranial slope | The angle between the horizontal line and the McGregor line | [21] |
| Cranial tilt | The angle between the vertical line and the line joining the center of the McGregor line and the sella turcica | [26] |
| Spino-cranial angle | The angle between the C7 slope and the straight line joining the middle of the C7 end plate and the middle of the sella turcica | [27] |
| C2-pelvic angle | The angle of a line from the C2 centroid to the femoral head (FH) and a line from the FH to the middle of the S1 endplate | [28] |
| Cervicothoracic pelvic angle | The angle of a line from the center of C2 to the FH and a line from the FH to center of T1 | [28] |
| Craniocervical angle | The angle of the line from the center of C7 to the posterior corner of the hard palate and McGregor’s line | [28] |
| Occipitocervical inclination | The angle formed by the line connecting McGregor’s line and the posterior border of the C4 vertebral body | [29] |
| Clivo-axial angle | The angle subtended by lines drawn parallel to the dorsal surfaces of the clivus and dens | [30] |
| K-line tilt | The angle between the K-line and a line perpendicular to the horizon | [31] |
| C2 incidence angle | The angle between a line from the center of the FH through the midpoint of the sacral superior endplate and a line extended perpendicular to the C2 inferior endplate | [32] |
| C2 slope | The angle between the lower endplate of C2 and the horizontal plane | [33] |
| 1st Author | Year | Number of Patients (CSM/OPLL) | Definition of Cervical Deformity | Surgical Techniques (vs. Other Surgical Approach) | Risk Factors of Postoperative Malalignment | Prediction Factors of Postoperative Malalignment before Surgery | Risk Factors of Poor HRQOL Outcome |
|---|---|---|---|---|---|---|---|
| Zhou X [117] | 2017 | CSM: 67 | - | ADF and LAMP (vs. LAMP only) | No difference | No difference | No difference |
| Yeh KT [118] | 2015 | DCM: 109 | -- | ADF and LAMP | - | - | - |
| Sun K [119] | 2020 | OPLL: 71 | - | ADF (vs. laminectomy) | Laminectomy | - | Laminectomy |
| Li YC [120] | 2022 | OPLL: 55 | - | ADF and laminectomy (vs. P-F) | - | - | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Suzuki, H.; Funaba, M.; Fujimoto, K.; Ichihara, Y.; Nishida, N.; Sakai, T. Current Concepts of Cervical Spine Alignment, Sagittal Deformity, and Cervical Spine Surgery. J. Clin. Med. 2024, 13, 1196. https://doi.org/10.3390/jcm13051196
Suzuki H, Funaba M, Fujimoto K, Ichihara Y, Nishida N, Sakai T. Current Concepts of Cervical Spine Alignment, Sagittal Deformity, and Cervical Spine Surgery. Journal of Clinical Medicine. 2024; 13(5):1196. https://doi.org/10.3390/jcm13051196
Chicago/Turabian StyleSuzuki, Hidenori, Masahiro Funaba, Kazuhiro Fujimoto, Yusuke Ichihara, Norihiro Nishida, and Takashi Sakai. 2024. "Current Concepts of Cervical Spine Alignment, Sagittal Deformity, and Cervical Spine Surgery" Journal of Clinical Medicine 13, no. 5: 1196. https://doi.org/10.3390/jcm13051196
APA StyleSuzuki, H., Funaba, M., Fujimoto, K., Ichihara, Y., Nishida, N., & Sakai, T. (2024). Current Concepts of Cervical Spine Alignment, Sagittal Deformity, and Cervical Spine Surgery. Journal of Clinical Medicine, 13(5), 1196. https://doi.org/10.3390/jcm13051196