
Risk Factor Analysis for Developing Major Complications Following Esophageal Surgery—A Two-Center Study

 , ,
, ,  ,
,
Abstract
1. Introduction
2. Methods
2.1. Data Collection
2.2. Statistical Analysis
3. Results
3.1. Baseline Demographics, Comorbidities
3.2. Univariate Analysis
3.3. Outcomes
3.4. Multivariate Analysis
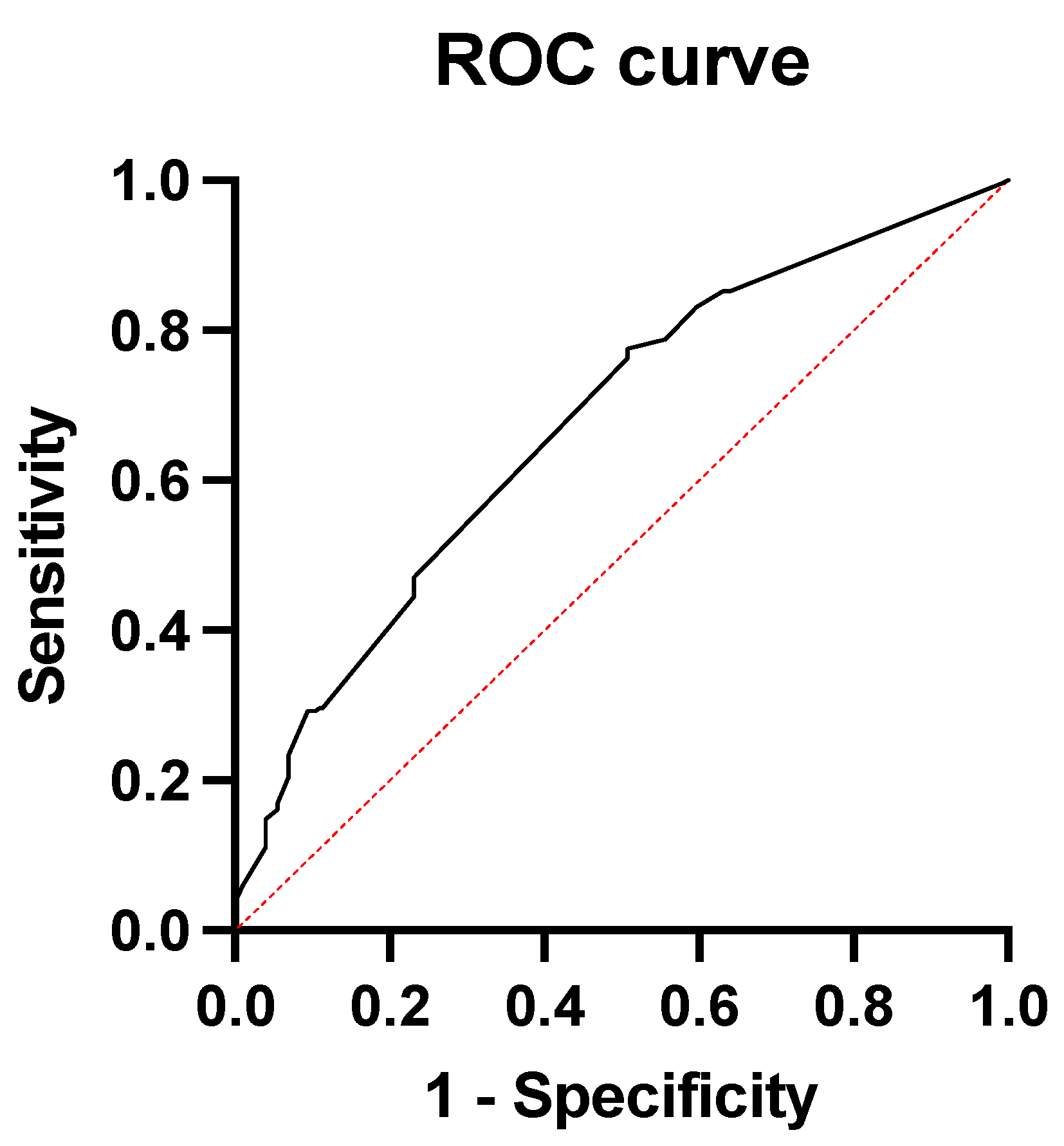
3.5. Predictive Value of Comorbidities for Major Complications
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lepage, C.; Rachet, B.; Jooste, V.; Faivre, J.; Coleman, M.P. Continuing rapid increase in esophageal adenocarcinoma in England and Wales. Am. J. Gastroenterol. 2008, 103, 2694–2699. [Google Scholar] [CrossRef]
- Rubenstein, J.H.; Taylor, J.B. Meta-analysis: The association of oesophageal adenocarcinoma with symptoms of gastro-oesophageal reflux. Aliment. Pharmacol. Ther. 2010, 32, 1222–1227. [Google Scholar] [CrossRef]
- Turati, F.; Tramacere, I.; La Vecchia, C.; Negri, E. A meta-analysis of body mass index and esophageal and gastric cardia adenocarcinoma. Ann. Oncol. 2013, 24, 609–617. [Google Scholar] [CrossRef]
- Tramacere, I.; La Vecchia, C.; Negri, E. Tobacco smoking and esophageal and gastric cardia adenocarcinoma: A meta-analysis. Epidemiology 2011, 22, 344–349. [Google Scholar] [CrossRef]
- Sun, F.; Yuan, P.; Chen, T.; Hu, J. Efficacy and complication of endoscopic submucosal dissection for superficial esophageal carcinoma: A systematic review and meta-analysis. J. Cardiothorac. Surg. 2014, 9, 78. [Google Scholar] [CrossRef]
- Wright, C.D. Esophageal cancer surgery in 2005. Minerva Chir. 2005, 60, 431–444. [Google Scholar] [PubMed]
- Rentz, J.; Bull, D.; Harpole, D.; Bailey, S.; Neumayer, L.; Pappas, T.; Krasnicka, B.; Henderson, W.; Daley, J.; Khuri, S. Transthoracic versus transhiatal esophagectomy: A prospective study of 945 patients. J. Thorac. Cardiovasc. Surg. 2003, 125, 1114–1120. [Google Scholar] [CrossRef] [PubMed]
- Finks, J.F.; Osborne, N.H.; Birkmeyer, J.D. Trends in hospital volume and operative mortality for high-risk surgery. N. Engl. J. Med. 2011, 364, 2128–2137. [Google Scholar] [CrossRef] [PubMed]
- Busweiler, L.A.; Henneman, D.; Dikken, J.L.; Fiocco, M.; van Berge Henegouwen, M.I.; Wijnhoven, B.P.; van Hillegersberg, R.; Rosman, C.; Wouters, M.W.; van Sandick, J.W. Failure-to-rescue in patients undergoing surgery for esophageal or gastric cancer. Eur. J. Surg. Oncol. 2017, 43, 1962–1969. [Google Scholar] [CrossRef] [PubMed]
- Abdelsattar, Z.M.; Habermann, E.; Borah, B.J.; Moriarty, J.P.; Rojas, R.L.; Blackmon, S.H. Understanding Failure to Rescue After Esophagectomy in the United States. Ann. Thorac. Surg. 2020, 109, 865–871. [Google Scholar] [CrossRef] [PubMed]
- Dunst, C.M.; Swanström, L.L. Minimally invasive esophagectomy. J. Gastrointest. Surg. 2010, 14 (Suppl. 1), S108–S114. [Google Scholar] [CrossRef] [PubMed]
- Courrech Staal, E.F.; Aleman, B.M.; Boot, H.; van Velthuysen, M.L.; van Tinteren, H.; van Sandick, J.W. Systematic review of the benefits and risks of neoadjuvant chemoradiation for oesophageal cancer. Br. J. Surg. 2010, 97, 1482–1496. [Google Scholar] [CrossRef] [PubMed]
- Guo, W.; Ma, X.; Yang, S.; Zhu, X.; Qin, W.; Xiang, J.; Lerut, T.; Li, H. Combined thoracoscopic-laparoscopic esophagectomy versus open esophagectomy: A meta-analysis of outcomes. Surg. Endosc. 2016, 30, 3873–3881. [Google Scholar] [CrossRef] [PubMed]
- Ashok, A.; Niyogi, D.; Ranganathan, P.; Tandon, S.; Bhaskar, M.; Karimundackal, G.; Jiwnani, S.; Shetmahajan, M.; Pramesh, C.S. The enhanced recovery after surgery (ERAS) protocol to promote recovery following esophageal cancer resection. Surg. Today 2020, 50, 323–334. [Google Scholar] [CrossRef]
- Low, D.E.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.E.; D'Journo, X.B.; Griffin, S.M.; Hölscher, A.H.; Hofstetter, W.L.; Jobe, B.A.; et al. International Consensus on Standardization of Data Collection for Complications Associated With Esophagectomy: Esophagectomy Complications Consensus Group (ECCG). Ann. Surg. 2015, 262, 286–294. [Google Scholar] [CrossRef]
- Low, D.E.; Kuppusamy, M.K.; Alderson, D.; Cecconello, I.; Chang, A.C.; Darling, G.; Davies, A.; D’Journo, X.B.; Gisbertz, S.S.; Griffin, S.M.; et al. Benchmarking Complications Associated with Esophagectomy. Ann. Surg. 2019, 269, 291–298. [Google Scholar] [CrossRef]
- Ljungqvist, O.; Scott, M.; Fearon, K.C. Enhanced Recovery After Surgery: A Review. JAMA Surg. 2017, 152, 292–298. [Google Scholar] [CrossRef]
- Stone, A.B.; Grant, M.C.; Pio Roda, C.; Hobson, D.; Pawlik, T.; Wu, C.L.; Wick, E.C. Implementation Costs of an Enhanced Recovery After Surgery Program in the United States: A Financial Model and Sensitivity Analysis Based on Experiences at a Quaternary Academic Medical Center. J. Am. Coll. Surg. 2016, 222, 219–225. [Google Scholar] [CrossRef]
- Bolger, J.C.; Loughney, L.; Tully, R.; Cunningham, M.; Keogh, S.; McCaffrey, N.; Hickey, W.; Robb, W.B. Perioperative prehabilitation and rehabilitation in esophagogastric malignancies: A systematic review. Dis. Esophagus 2019, 32, doz058. [Google Scholar] [CrossRef]
- van Kooten, R.T.; Voeten, D.M.; Steyerberg, E.W.; Hartgrink, H.H.; van Berge Henegouwen, M.I.; van Hillegersberg, R.; Tollenaar, R.; Wouters, M. Patient-Related Prognostic Factors for Anastomotic Leakage, Major Complications, and Short-Term Mortality Following Esophagectomy for Cancer: A Systematic Review and Meta-Analyses. Ann. Surg. Oncol. 2022, 29, 1358–1373. [Google Scholar] [CrossRef]
- Low, D.E.; Allum, W.; De Manzoni, G.; Ferri, L.; Immanuel, A.; Kuppusamy, M.; Law, S.; Lindblad, M.; Maynard, N.; Neal, J.; et al. Guidelines for Perioperative Care in Esophagectomy: Enhanced Recovery After Surgery (ERAS(®)) Society Recommendations. World J. Surg. 2019, 43, 299–330. [Google Scholar] [CrossRef] [PubMed]
- Mortensen, K.; Nilsson, M.; Slim, K.; Schäfer, M.; Mariette, C.; Braga, M.; Carli, F.; Demartines, N.; Griffin, S.M.; Lassen, K. Consensus guidelines for enhanced recovery after gastrectomy: Enhanced Recovery After Surgery (ERAS®) Society recommendations. Br. J. Surg. 2014, 101, 1209–1229. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
| Postoperative Complication | n (%) |
|---|---|
| Pneumonia | 160 (36%) |
| Sepsis | 94 (21%) |
| PE | 26 (5.9%) |
| Bleeding | 13 (3.0%) |
| Anastomotic leakage | 111 (25%) |
| ≥1 Major Complication | 236 (54%) |
| Variable | Anastomotic Insufficiency | Surgical Site Infection | Bleeding | ||||||
| No | Yes | No | Yes | No | Yes | ||||
| n = 328 | n = 112 | p-Value | n = 404 | n = 35 | p-Value | n = 426 | n = 13 | p-Value | |
| Age (years) | 63 (56, 71) | 62 (57, 70) | 0.8 | 63 (56, 71) | 60 (54, 70) | 0.6 | 63 (56, 71) | 59 (57, 64) | 0.5 |
| Male sex | 266 (81%) | 92 (82%) | 0.8 | 326 (81%) | 31 (89%) | 0.3 | 345 (81%) | 12 (92%) | 0.5 |
| Diabetes | 50 (15%) | 11 (9.9%) | 0.2 | 57 (14%) | 4 (11%) | 0.8 | 59 (13%) | 2 (15%) | 0.7 |
| CHD | 44 (13%) | 15 (14%) | >0.9 | 57 (14%) | 2 (5.7%) | 0.2 | 55 (13%) | 4 (31%) | 0.083 |
| Stroke | 17 (5.2%) | 2 (1.8%) | 0.2 | 17 (4.2%) | 2 (5.7%) | 0.7 | 19 (4.5%) | 0 (0%) | >0.9 |
| COPD | 37 (11%) | 14 (13%) | 0.7 | 49 (12%) | 2 (5.7%) | 0.4 | 50 (12%) | 1 (7.7%) | >0.9 |
| Alcohol | 25 (7.6%) | 22 (20%) | <0.001 | 42 (10%) | 5 (14%) | 0.4 | 43 (10%) | 4 (31%) | 0.040 |
| Tobacco use | 88 (27%) | 43 (39%) | 0.018 | 117 (29%) | 14 (40%) | 0.2 | 125 (29%) | 6 (46%) | 0.2 |
| CTx | 142 (43%) | 24 (21%) | <0.001 | 153 (38%) | 13 (37%) | >0.9 | 164 (38%) | 2 (15%) | 0.14 |
| Open surgery | 260 (79%) | 85 (76%) | 0.5 | 312 (77%) | 32 (91%) | 0.05 | 335 (79%) | 9 (69%) | 0.5 |
| UICC stage | 0.6 | 0.3 | 0.9 | ||||||
| 0 | 25 (8%) | 11 (10%) | 35 (8.7%) | 1 (2.9%) | 34 (8.0%) | 2 (15%) | |||
| 1 | 99 (30%) | 29 (26%) | 121 (30%) | 7 (20%) | 125 (29%) | 3 (23%) | |||
| 2 | 53 (16%) | 25 (22%) | 71 (18%) | 7 (20%) | 76 (18%) | 2 (15%) | |||
| 3 | 128 (39%) | 35 (31%) | 147 (36%) | 15 (43%) | 157 (37%) | 5 (38%) | |||
| 4 | 23 (7%) | 12 (11%) | 30 (7.4%) | 5 (14%) | 34 (8.0%) | 1 (7.7%) | |||
| Type of Cancer | <0.001 | 0.3 | 0.5 | ||||||
| EAC | 251 (77%) | 67 (60%) | 290 (72%) | 27 (77%) | 309 (73%) | 8 (62%) | |||
| ESC | 71 (22%) | 45 (40%) | 109 (27%) | 7 (20%) | 111 (26%) | 5 (38%) | |||
| Other | 6 (1.8%) | 0 (0%) | 5 (1.2%) | 1 (2.9%) | 6 (1.4%) | 0 (0%) | |||
| Variable | Pneumonia | Sepsis | PE | ||||||
| No | Yes | No | Yes | No | Yes | ||||
| n = 279 | n = 160 | p-Value | n = 345 | n = 95 | p-Value | n = 413 | n = 26 | p-Value | |
| Age (years) | 63 (56, 71) | 64 (57, 71) | 0.7 | 63 (56, 71) | 64 (57, 71) | 0.5 | 63 (56, 71) | 58 (56, 64) | 0.11 |
| Male sex | 223 (80%) | 134 (84%) | 0.3 | 281 (81%) | 77 (81%) | >0.9 | 335 (81%) | 22 (85%) | 0.8 |
| Diabetes | 40 (14%) | 21 (13%) | 0.7 | 48 (14%) | 13 (14%) | >0.9 | 58 (14%) | 3 (12%) | >0.9 |
| CHD | 35 (13%) | 24 (15%) | 0.5 | 38 (11%) | 21 (22%) | 0.004 | 55 (13%) | 4 (15%) | 0.8 |
| Stroke | 15 (5.4%) | 4 (2.5%) | 0.2 | 16 (4.6%) | 3 (3.2%) | 0.8 | 19 (4.6%) | 0 (0%) | 0.6 |
| COPD | 23 (8.2%) | 28 (18%) | 0.004 | 38 (11%) | 13 (14%) | 0.5 | 50 (12%) | 1 (3.8%) | 0.3 |
| Alcohol | 22 (7.9%) | 25 (16%) | 0.012 | 32 (9.3%) | 15 (16%) | 0.063 | 46 (11%) | 1 (3.8%) | 0.3 |
| Tobacco use | 78 (28%) | 53 (33%) | 0.3 | 101 (29%) | 30 (32%) | 0.6 | 124 (30%) | 7 (27%) | 0.7 |
| CTx | 126 (45%) | 40 (25%) | <0.001 | 145 (42%) | 22 (23%) | <0.001 | 155 (38%) | 11 (42%) | 0.6 |
| Open surgery | 216 (77%) | 132 (82%) | 0.2 | 265 (77%) | 80 (84%) | 0.12 | 324 (78%) | 20 (77%) | 0.9 |
| UICC stage | 0.4 | 0.6 | 0.015 | ||||||
| 0 | 29 (10%) | 7 (4.4%) | 30 (8.7%) | 7 (7.4%) | 33 (8.0%) | 3 (12%) | |||
| 1 | 80 (29%) | 48 (30%) | 102 (30%) | 26 (27%) | 121 (29%) | 7 (27%) | |||
| 2 | 48 (17%) | 30 (18%) | 64 (19%) | 14 (15%) | 78 (19%) | 0 (0%) | |||
| 3 | 98 (35%) | 64 (40%) | 122 (35%) | 40 (42%) | 151 (37%) | 11 (42%) | |||
| 4 | 24 (9%) | 11 (6.9%) | 27 (7.8%) | 8 (8.4%) | 30 (7.3%) | 5 (19%) | |||
| Type of Cancer | 0.4 | 0.3 | |||||||
| EAC | 206 (74%) | 111 (69%) | 252 (73%) | 65 (68%) | 295 (71%) | 22 (85%) | 0.5 | ||
| ESC | 68 (24%) | 48 (30%) | 87 (25%) | 30 (32%) | 112 (27%) | 4 (15%) | |||
| Other | 5 (1.8%) | 1 (0.6%) | 6 (1.7%) | 0 (0%) | 6 (1.5%) | 0 (0%) | |||
| Variable | Total | ≥1 Major Complication | ||
|---|---|---|---|---|
| No | Yes | |||
| n = 441 | n = 203 | n = 238 | p-Value | |
| Age (years) | 63 (56, 71) | 63 (56, 71) | 63 (57, 71) | >0.9 |
| Male sex | 359 (81%) | 161 (79%) | 198 (83%) | 0.3 |
| Diabetes | 61 (14%) | 31 (15%) | 30 (13%) | 0.4 |
| CHD | 59 (13%) | 20 (9.9%) | 39 (17%) | 0.041 |
| Stroke | 19 (4%) | 11 (5.4%) | 8 (3.4%) | 0.3 |
| COPD | 51 (12%) | 15 (7.4%) | 36 (15%) | 0.010 |
| Alcohol | 47 (11%) | 12 (5.9%) | 35 (15%) | 0.003 |
| Tobacco use | 131 (30%) | 57 (28%) | 74 (31%) | 0.5 |
| CTx | 167 (38%) | 102 (50%) | 65 (27%) | <0.001 |
| Open surgery | 346 (78%) | 161 (79%) | 185 (78%) | 0.700 |
| UICC stage | 0.6 | |||
| 0 | 37 (8%) | 20 (9.9%) | 17 (7.1%) | |
| 1 | 128 (29%) | 62 (31%) | 66 (28%) | |
| 2 | 78 (18%) | 35 (17%) | 43 (18%) | |
| 3 | 163 (37%) | 68 (33%) | 95 (40%) | |
| 4 | 35 (8%) | 18 (8.9%) | 17 (7.1%) | |
| Type of Cancer | 0.005 | |||
| EAC | 318 (72%) | 159 (78%) | 159 (67%) | |
| ESC | 117 (27%) | 40 (20%) | 77 (32%) | |
| Other | 6 (1.4%) | 4 (2.0%) | 2 (0.8%) | |
| Variable | Odds Ratios (CI 95%) | p Value |
|---|---|---|
| CHD | 1.91 (1.05–3.54) | 0.0367 |
| COPD | 2.13 (1.11–4.26) | 0.0264 |
| Alcohol | 2.16 (1.09–4.56) | 0.0341 |
| CTx | 0.40 (0.26–0.61) | <0.0001 |
| Type of Cancer | 1.39 (0.86–2.25) | 0.1786 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Stüben, B.-O.; Plitzko, G.A.; Stern, L.; Schmeding, R.; Karstens, K.-F.; Reeh, M.; Treckmann, J.W.; Izbicki, J.R.; Saner, F.H.; Neuhaus, J.P.; et al. Risk Factor Analysis for Developing Major Complications Following Esophageal Surgery—A Two-Center Study. J. Clin. Med. 2024, 13, 1137. https://doi.org/10.3390/jcm13041137
Stüben B-O, Plitzko GA, Stern L, Schmeding R, Karstens K-F, Reeh M, Treckmann JW, Izbicki JR, Saner FH, Neuhaus JP, et al. Risk Factor Analysis for Developing Major Complications Following Esophageal Surgery—A Two-Center Study. Journal of Clinical Medicine. 2024; 13(4):1137. https://doi.org/10.3390/jcm13041137
Chicago/Turabian StyleStüben, Björn-Ole, Gabriel Andreas Plitzko, Louisa Stern, Rainer Schmeding, Karl-Frederick Karstens, Matthias Reeh, Jürgen Walter Treckmann, Jakob Robert Izbicki, Fuat Hakan Saner, Jan Peter Neuhaus, and et al. 2024. "Risk Factor Analysis for Developing Major Complications Following Esophageal Surgery—A Two-Center Study" Journal of Clinical Medicine 13, no. 4: 1137. https://doi.org/10.3390/jcm13041137
APA StyleStüben, B.-O., Plitzko, G. A., Stern, L., Schmeding, R., Karstens, K.-F., Reeh, M., Treckmann, J. W., Izbicki, J. R., Saner, F. H., Neuhaus, J. P., Tachezy, M., & Hoyer, D. P. (2024). Risk Factor Analysis for Developing Major Complications Following Esophageal Surgery—A Two-Center Study. Journal of Clinical Medicine, 13(4), 1137. https://doi.org/10.3390/jcm13041137