


Intramedullary Nail vs. Plate Fixation for Pathological Humeral Shaft Fracture: An Updated Narrative Review and Meta-Analysis of Surgery-Related Factors
 ,
, 
Abstract
1. Introduction
2. Materials and Methods
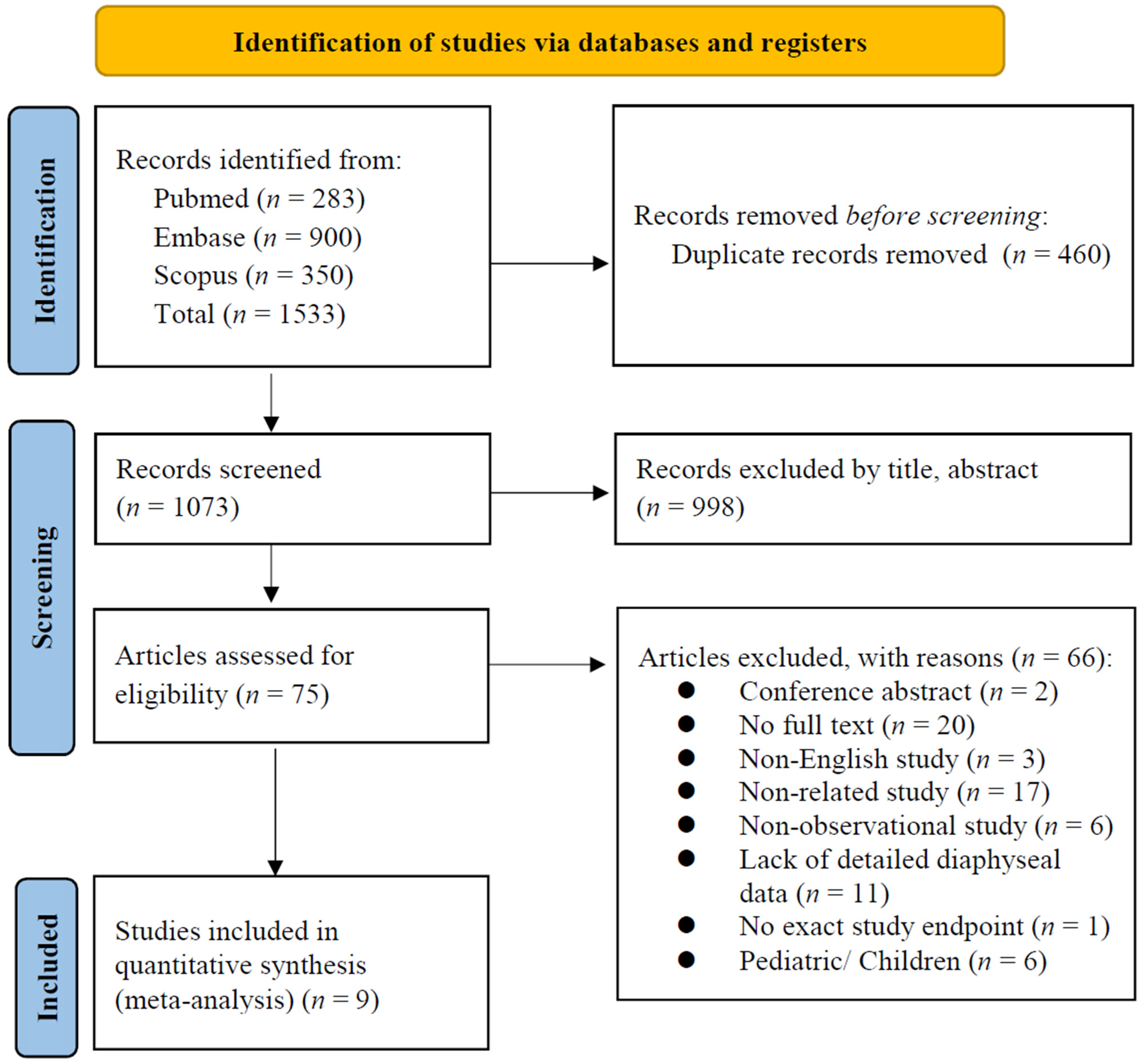
2.1. Study Design and Identification of Eligible Studies
2.2. Inclusion and Exclusion Criteria
2.3. Data Extraction
2.4. Methodological Quality Appraisal
2.5. Outcomes
2.6. Statistical Analyses
3. Results
3.1. Quantitative Data Synthesis (Meta-Analysis)
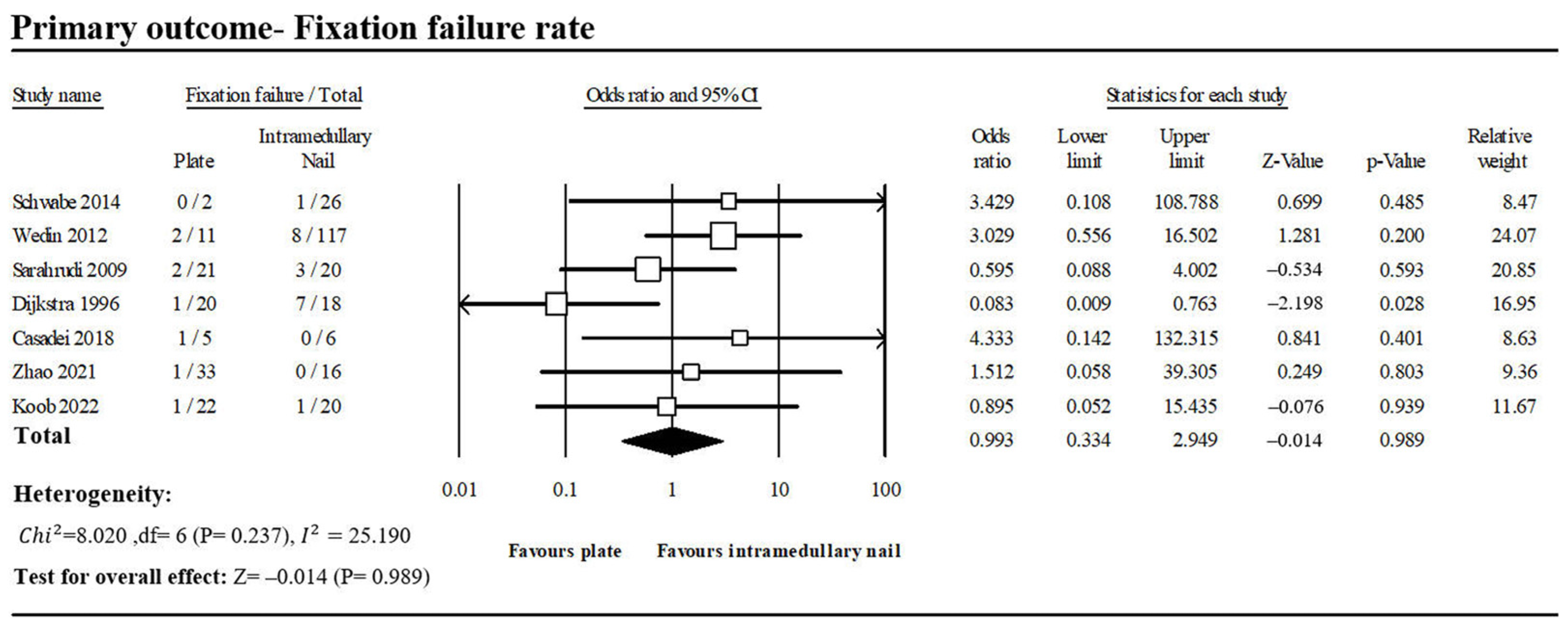
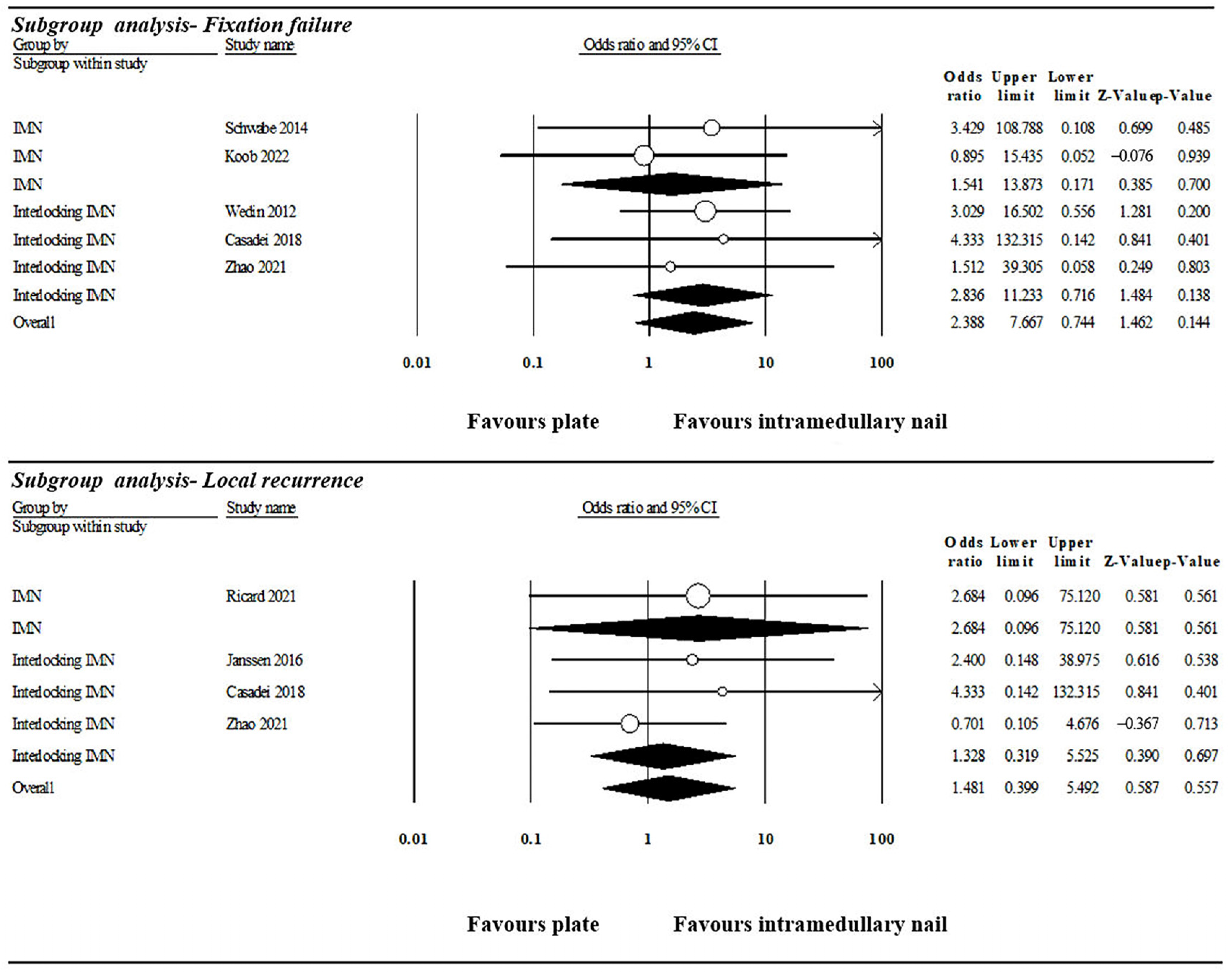
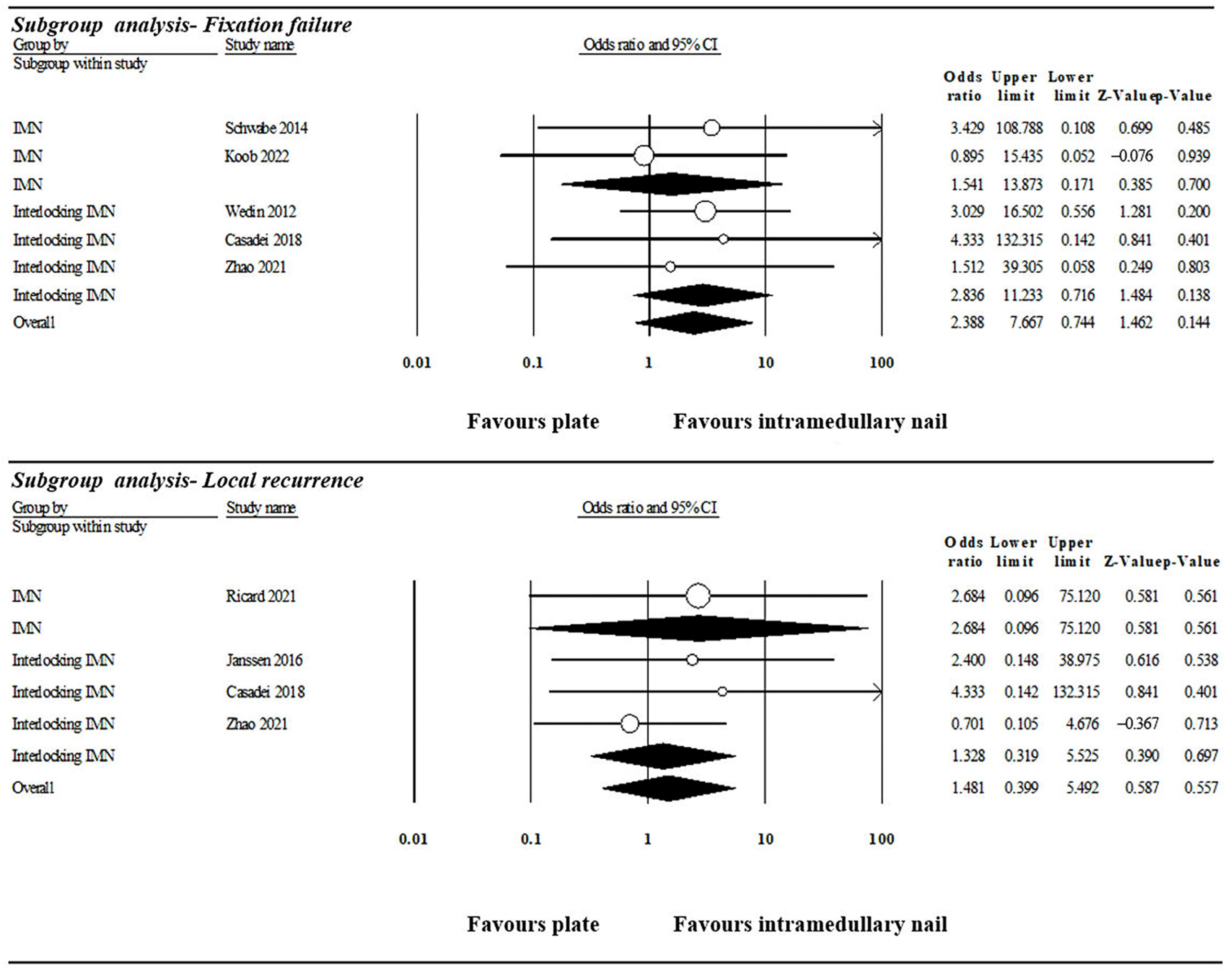
3.1.1. Fixation Failure Rate
3.1.2. Local Recurrence Rate
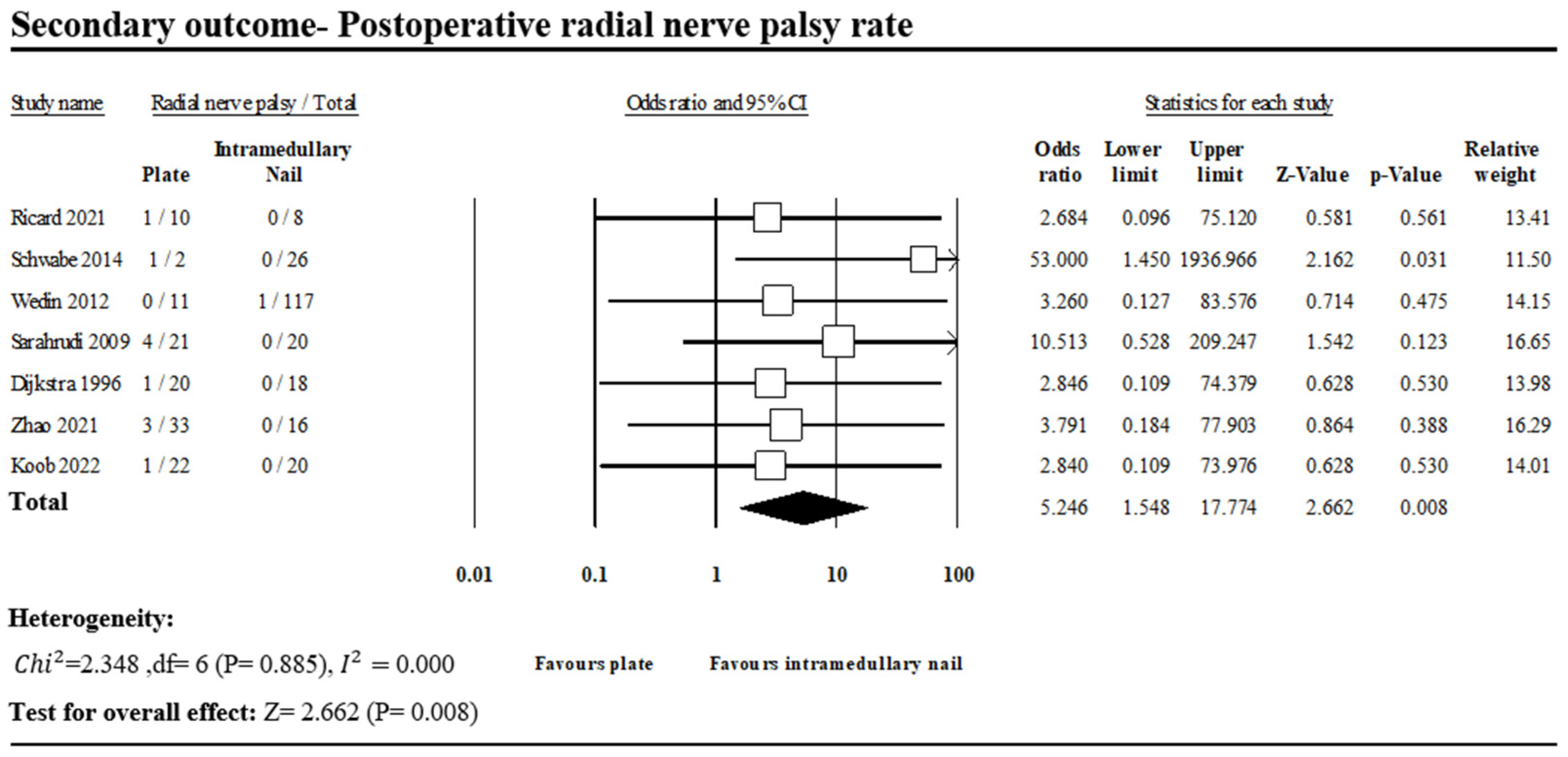
3.1.3. Postoperative Radial Nerve Palsy
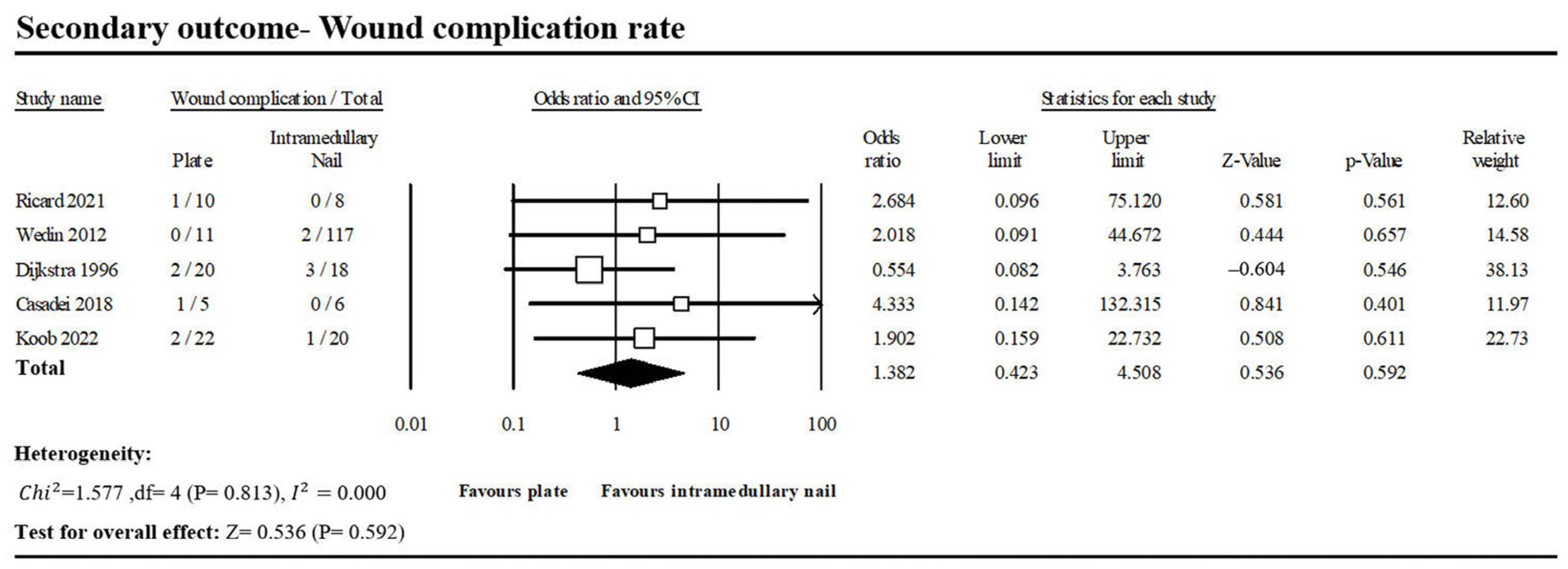
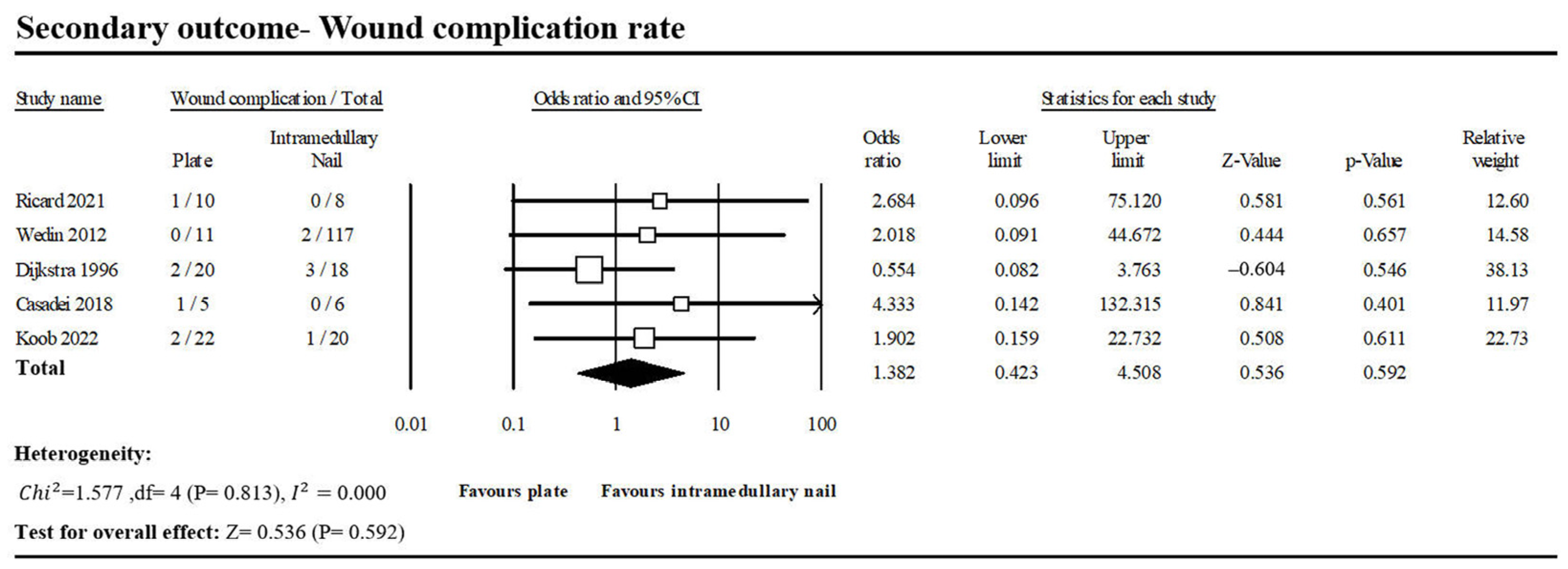
3.1.4. Wound Complication Rate
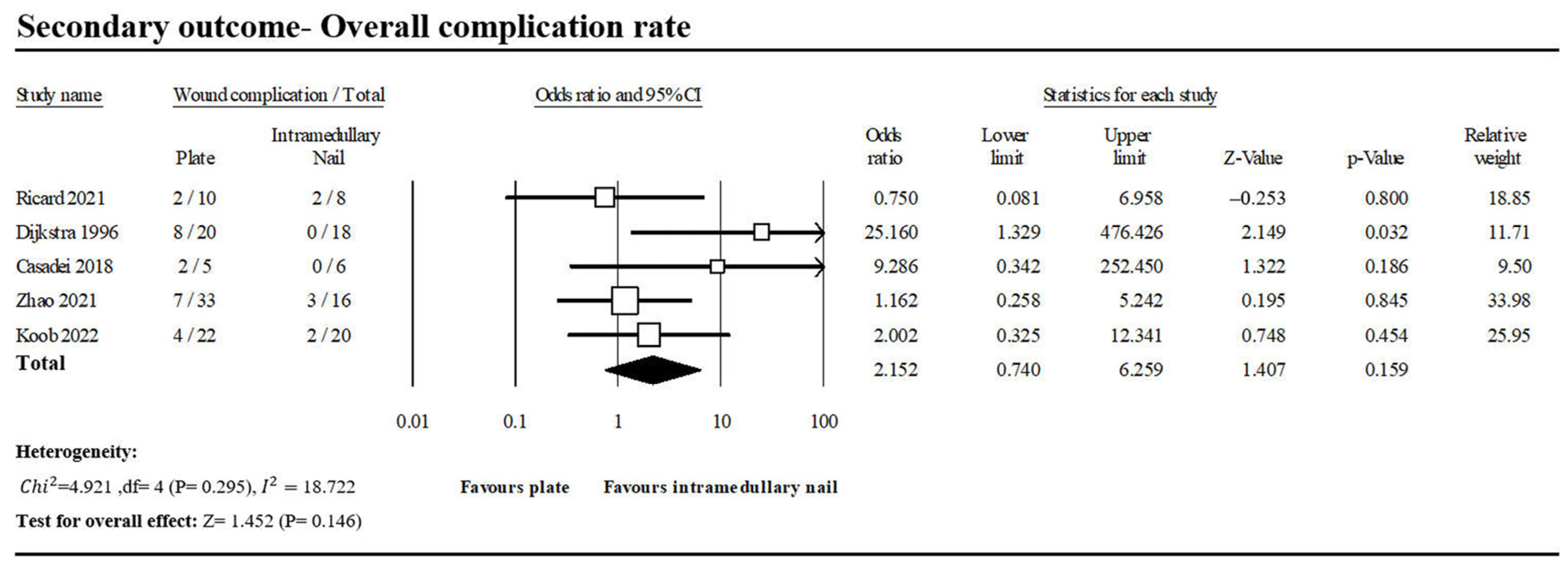
3.1.5. Overall Complication Rate
3.2. Interlocking Intramedullary Nail Subgroup Analysis
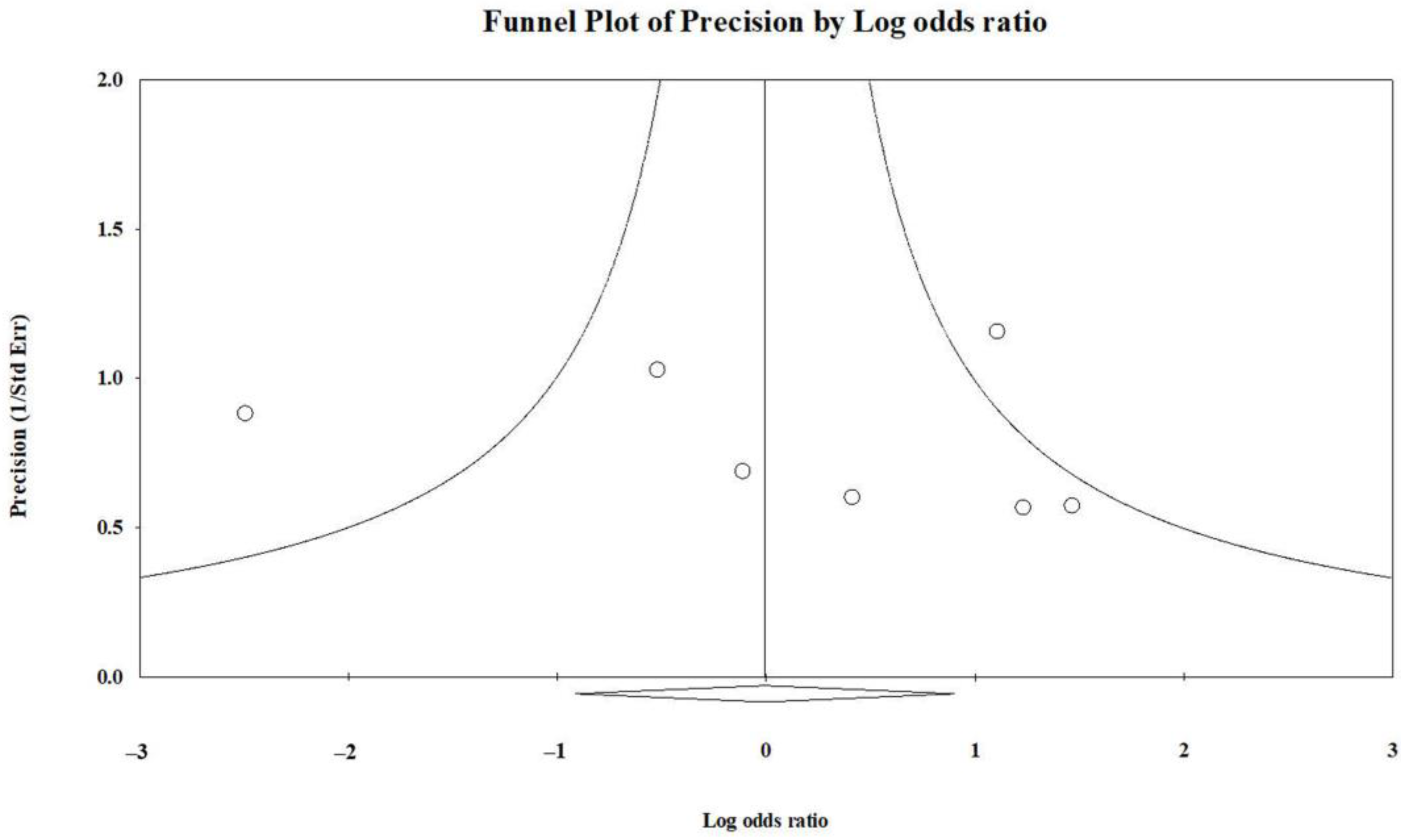
3.3. Publication Bias
4. Discussion
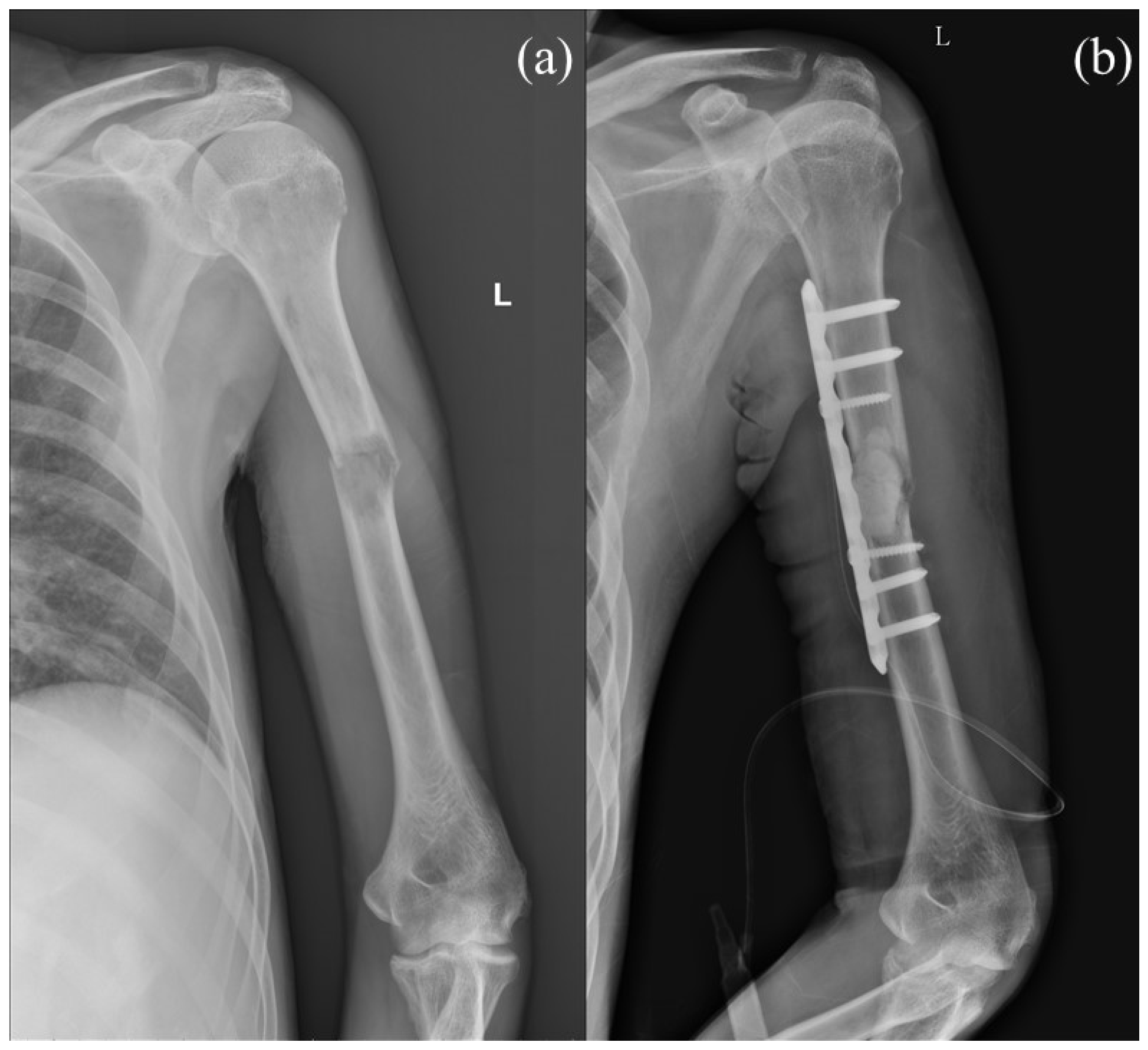
4.1. Surgical and Clinical Features of Plate Fixation
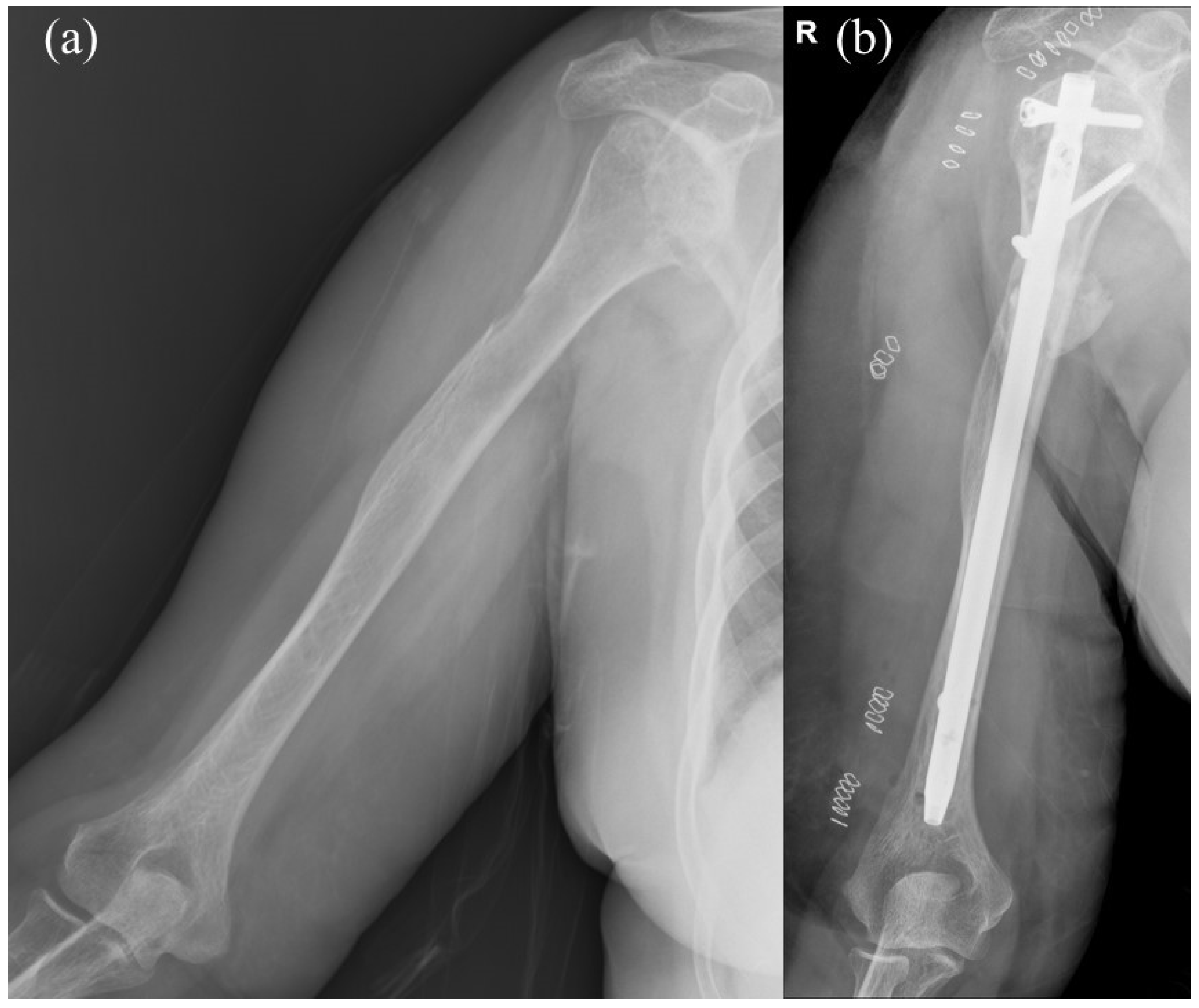
4.2. Surgical and Clinical Features of Intramedullary Nail Fixation
4.3. Applications of Postoperative Radiotherapy
4.4. Shoulder Complications for INF
4.5. Surgical Costs for Both Methods
4.6. Similar Studies
4.7. Recommended Surgical Approach Based on Different Conditions
5. Limitations
6. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Dijkstra, S.; Stapert, J.; Boxma, H.; Wiggers, T. Treatment of Pathological Fractures of the Humeral Shaft due to Bone Metastases: A Comparison of Intramedullary Locking Nail and Plate Osteosynthesis with Adjunctive Bone Cement. Eur. J. Surg. Oncol. 1996, 22, 621–626. [Google Scholar] [CrossRef]
- Dutka, J.; Sosin, P. Time of Survival and Quality of Life of the Patients Operatively Treated due to Pathological Fractures due to Bone Metastases. Ortop. Traumatol. Rehabil. 2003, 5, 276–283. [Google Scholar]
- Sarahrudi, K.; Wolf, H.; Funovics, P.; Pajenda, G.; Hausmann, J.T.; Vécsei, V. Surgical Treatment of Pathological Fractures of the Shaft of the Humerus. J. Trauma 2009, 66, 789–794. [Google Scholar] [CrossRef]
- Frassica, F.J.; Frassica, D.A. Metastatic Bone Disease of the Humerus. J. Am. Acad. Orthop. Surg. 2003, 11, 282–288. [Google Scholar] [CrossRef]
- Piccioli, A.; Maccauro, G.; Rossi, B.; Scaramuzzo, L.; Frenos, F.; Capanna, R. Surgical Treatment of Pathologic Fractures of Humerus. Injury 2010, 41, 1112–1116. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.J.; van der Linden, Y.M.; van de Sande, M.A.J.; Dijkstra, P.D.S. Treatment of Pathological Fractures of the Long Bones. EFORT Open Rev. 2016, 1, 136–145. [Google Scholar] [CrossRef] [PubMed]
- Weiss, K.R.; Bhumbra, R.; Biau, D.J.; Griffin, A.M.; Deheshi, B.; Wunder, J.S.; Ferguson, P.C. Fixation of Pathological Humeral Fractures by the Cemented Plate Technique. J. Bone Jt. Surg. Br. 2011, 93, 1093–1097. [Google Scholar] [CrossRef] [PubMed]
- Zheng, K.; Yu, X.C.; Hu, Y.C.; Shao, Z.W.; Xu, M.; Wang, B.C.; Wang, F. Outcome of Segmental Prosthesis Reconstruction for Diaphyseal Bone Tumors: A Multi-Center Retrospective Study. BMC Cancer 2019, 19, 638. [Google Scholar] [CrossRef] [PubMed]
- Zhao, Z.; Ye, Z.; Yan, T.; Tang, X.; Guo, W.; Yang, R. Intercalary Prosthetic Replacement Is a Reliable Solution for Metastatic Humeral Shaft Fractures: Retrospective, Observational Study of a Single Center Series. World J. Surg. Oncol. 2021, 19, 140. [Google Scholar] [CrossRef] [PubMed]
- Bickels, J.; Kollender, Y.; Wittig, J.C.; Meller, I.; Malawer, M.M. Function after Resection of Humeral Metastases: Analysis of 59 Consecutive Patients. Clin. Orthop. Relat. Res. 2005, 437, 201–208. [Google Scholar] [CrossRef]
- Frassica, F.J.; Frassica, D.A. Evaluation and Treatment of Metastases to the Humerus. Clin. Orthop. Relat. Res. 2003, 415, S212–S218. [Google Scholar] [CrossRef] [PubMed]
- Janssen, S.J.; van Dijke, M.; Lozano-Calderón, S.A.; Ready, J.E.; Raskin, K.A.; Ferrone, M.L.; Hornicek, F.J.; Schwab, J.H. Complications after Surgery for Metastatic Humeral Lesions. J. Shoulder Elb. Surg. 2016, 25, 207–215. [Google Scholar] [CrossRef] [PubMed]
- Wedin, R.; Hansen, B.H.; Laitinen, M.; Trovik, C.; Zaikova, O.; Bergh, P.; Kalén, A.; Schwarz-Lausten, G.; Vult von Steyern, F.; Walloe, A.; et al. Complications and Survival after Surgical Treatment of 214 Metastatic Lesions of the Humerus. J. Shoulder Elb. Surg. 2012, 21, 1049–1055. [Google Scholar] [CrossRef] [PubMed]
- Casadei, R.; Drago, G.; Di Pressa, F.; Donati, D. Humeral Metastasis of Renal Cancer: Surgical Options and Review of Literature. Orthop. Traumatol. Surg. Res. 2018, 104, 533–538. [Google Scholar] [CrossRef] [PubMed]
- Koob, S.; Plöger, M.M.; Bornemann, R.; Lehmann, R.P.; Alex, D.; Placzek, R. Intramedullary Nailing versus Compound Plate Osteosynthesis in Pathologic Diaphyseal Humerus Fractures: A Retrospective Cohort Study. Am. J. Clin. Oncol. 2022, 45, 379–380. [Google Scholar] [CrossRef] [PubMed]
- Ricard, M.M.; Stavropoulos, N.A.; Nooh, A.; Ste-Marie, N.; Goulding, K.; Turcotte, R. Intramedullary Nailing versus Plate Osteosynthesis for Humeral Shaft Metastatic Lesions. Cureus 2021, 13, e13788. [Google Scholar] [CrossRef] [PubMed]
- Schwabe, P.; Ruppert, M.; Tsitsilonis, S.; Melcher, I.; Schaser, K.D.; Märdian, S. Surgical Management and Outcome of Skeletal Metastatic Disease of the Humerus. Acta Chir. Orthop. Traumatol. Cech. 2014, 81, 365–370. [Google Scholar] [CrossRef]
- Aboulafia, A.J.; Levine, A.M.; Schmidt, D.; Aboulafia, D. Surgical Therapy of Bone Metastases. Semin. Oncol. 2007, 34, 206–214. [Google Scholar] [CrossRef]
- Soeharno, H.; Povegliano, L.; Choong, P.F. Multimodal Treatment of Bone Metastasis–A Surgical Perspective. Front. Endocrinol. 2018, 9, 518. [Google Scholar] [CrossRef]
- Pretell, J.; Rodriguez, J.; Blanco, D.; Zafra, A.; Resines, C. Treatment of Pathological Humeral Shaft Fractures with Intramedullary Nailing. A Retrospective Study. Int. Orthop. 2010, 34, 559–563. [Google Scholar] [CrossRef]
- Schwab, T.R.; Stillhard, P.F.; Schibli, S.; Furrer, M.; Sommer, C. Radial Nerve Palsy in Humeral Shaft Fractures with Internal Fixation: Analysis of Management and Outcome. Eur. J. Trauma Emerg. Surg. 2018, 44, 235–243. [Google Scholar] [CrossRef]
- Wang, Y.; Kayastha, Y.; Cao, Y.; Guo, Z.; Yuan, Y.; Bi, Y. Outcome of Humeral Shaft Fracture Treated with Intramedullary Nail and Plate Fixation. J. Coll. Physicians Surg. Pak. 2020, 30, 73–78. [Google Scholar] [CrossRef]
- Voskuil, R.T.; Mayerson, J.L.; Scharschmidt, T.J. Management of Metastatic Disease of the Upper Extremity. J. Am. Acad. Orthop. Surg. 2021, 29, e116–e125. [Google Scholar] [CrossRef]
- Kulkarni, S.G.; Varshneya, A.; Jain, M.; Kulkarni, V.S.; Kulkarni, G.S.; Kulkarni, M.G.; Kulkarni, R.M. Antegrade Interlocking Nailing versus Dynamic Compression Plating for Humeral Shaft Fractures. J. Orthop. Surg. 2012, 20, 288–291. [Google Scholar] [CrossRef] [PubMed]
- Thai, D.M.; Katigawa, Y.; Choong, P.F.M. Outcome of Surgical Management of Bony Metastases to the Humerus and Shoulder Girdle: A Retrospective Analysis of 93 Patients. Int. Semin. Surg. Oncol. 2006, 3, 5. [Google Scholar] [CrossRef] [PubMed]
- Willeumier, J.J.; van der Linden, Y.M.; Dijkstra, P.D.S. Lack of Clinical Evidence for Postoperative Radiotherapy after Surgical Fixation of Impending or Actual Pathologic Fractures in the Long Bones in Patients with Cancer; a Systematic Review. Radiother. Oncol. 2016, 121, 138–142. [Google Scholar] [CrossRef] [PubMed]
- Epstein-Peterson, Z.D.; Sullivan, A.; Krishnan, M.; Chen, J.T.; Ferrone, M.; Ready, J.; Baldini, E.H.; Balboni, T. Postoperative Radiation Therapy for Osseous Metastasis: Outcomes and Predictors of Local Failure. Pract. Radiat. Oncol. 2015, 5, e531–e536. [Google Scholar] [CrossRef] [PubMed]
- Dijkstra, S.; Wiggers, T.; Geel, B.; Boxma, H. Impending and Actual Pathological Fractures in Patients with Bone Metastases of the Long Bones. A Retrospective Study of 233 Surgically Treated Fractures. Eur. J. Surg. Acta Chir. 1994, 160, 535–542. [Google Scholar]
- Ofluoglu, O.; Erol, B.; Ozgen, Z.; Yildiz, M. Minimally Invasive Treatment of Pathological Fractures of the Humeral Shaft. Int. Orthop. 2009, 33, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Wali, M.G.; Baba, A.N.; Latoo, I.A.; Bhat, N.A.; Baba, O.K.; Sharma, S. Internal Fixation of Shaft Humerus Fractures by Dynamic Compression Plate or Interlocking Intramedullary Nail: A Prospective, Randomised Study. Strateg. Trauma Limb Reconstr. 2014, 9, 133–140. [Google Scholar] [CrossRef]
- Baltov, A.; Mihail, R.; Dian, E. Complications after Interlocking Intramedullary Nailing of Humeral Shaft Fractures. Injury 2014, 45 (Suppl. S1), S9–S15. [Google Scholar] [CrossRef] [PubMed]
- Heinsen, J.; Hempel, D. Präoperative Sonographische Untersuchung der Rotatorenmanschette vor Anterograder Nagelung von Humerusschaftfrakturen. Osteosynth. Int. 2001, 9, S85–S87. [Google Scholar] [CrossRef]
- El Ghazoui, A.; Haddaoui, J.; Zahar, E.M.; Sekkach, N. Humeral Shaft Fracture: Outcomes of Percutaneous Antegrade Intramedullary Nailing Using the Long Telegraph® Nail with Dynamic Distal Locking. Orthop. Traumatol. Surg. Res. 2022, 108, 103286. [Google Scholar] [CrossRef]
- Kachare, S.D.; Liner, K.R.; Vohra, N.A.; Zervos, E.E.; Hickey, T.; Fitzgerald, T.L. Assessment of Health Care Cost for Complex Surgical Patients: Review of Cost, Re-Imbursement and Revenue Involved in Pancreatic Surgery at a High-Volume Academic Medical Centre. HPB 2015, 17, 311–317. [Google Scholar] [CrossRef]
- Stephens, A.R.; Presson, A.P.; Zhang, C.; Orleans, B.; Martin, M.; Tyser, A.R.; Kazmers, N.H. Comparison of Direct Surgical Cost for Humeral Shaft Fracture Fixation: Open Reduction Internal Fixation versus Intramedullary Nailing. JSES Int. 2021, 5, 734–738. [Google Scholar] [CrossRef]
- Wu, K.; Lin, T.; Lee, C.-H. Intramedullary Nailing versus Cemented Plate for Treating Metastatic Pathological Fracture of the Proximal Humerus: A Comparison Study and Literature Review. J. Orthop. Traumatol. 2023, 24, 45. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Tai, T.; Tu, T.; Liaw, C.; Chiu, Y. Modified Hackethal’s Technique with Bone Grafting and Plate Fixation: A Case Report of Treatment for Pathological Humeral Shaft Fracture. Clin. Case Rep. Int. 2023, 7, 1548. [Google Scholar]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author (Year) | Country | Design | Sample Size (n) | Mean Age (Years) | Female (n (%)) | Endpoint | Follow-Up Duration (Months) (Mean ± SD) (Median, Range) | Outcome |
|---|---|---|---|---|---|---|---|---|
| Dijkstra et al. (1996) [1] | Netherlands | Retrospective cohort study | PF: 20 INF: 18 | PF: 63 INF: 68 | 26 (70%) | At least six months/Death | 4.8 (mean) | (1) (3) (4) (5) |
| Sarahrudi et al. (2009) [3] | Austria | Retrospective cohort study | PF: 21 INF: 20 | PF: 70.2 INF: 66.3 | 26 (63.4%) | Implant failure/Death | Not-mentioned | (1) (3) |
| Wedin et al. (2012) [13] | Sweden, Denmark, Norway | Prospective cohort study | PF: 11 INF: 117 | No diaphysis-limited data | No diaphysis-limited data | Implant failure/Death | 8, 0–97 (No diaphysis-limited data) | (1) (3) (4) |
| Schwabe et al. (2014) [17] | Germany | Retrospective cohort study | PF: 2 INF: 26 | No diaphysis-limited data | No diaphysis-limited data | Implant failure/Death | Not-mentioned | (1) (3) |
| Janssen et al. (2016) [12] | America | Retrospective cohort study | PF: 39 INF: 91 | No diaphysis-limited data | No diaphysis-limited data | Implant failure/Death | 4, 0–120 (Not diaphysis-limited data) | (2) |
| Casadei et al. (2018) [14] | Italy | Retrospective cohort study | PF: 5 INF: 6 | Total: 66.6 | 3 (25%) | At least 2 months from surgery | 22 (mean) (Not diaphysis-limited data) | (1) (2) (4) (5) |
| Ricard et al. (2021) [16] | Canada | Prospective cohort study | PF: 10 INF: 8 | PF: 61.2 INF: 70.25 | 8 (44.4%) | At least 52 weeks of follow-up or/Death | Not-mentioned | (2) (3) (4) (5) |
| Zhao et al. (2021) [9] | China | Retrospective cohort study | PF: 33 INF: 16 | PF: 62.1 INF: 61.9 | 30 (48%) | Implant failure/Death | 20.83 ± 18.4 | (1) (2) (3) (5) |
| Koob et al. (2022) [15] | Germany | Retrospective cohort study | PF: 22 INF: 20 | Total: 64.2 | 16 (38.09) | Implant failure/Death | 8.5 ± 15.4 | (1) (3) (4) (5) |
| Author (Year) | Implant Details | Preoperative Radiotherapy | Postoperative Radiotherapy | From Diagnosis of Primary Tumor to Humeral Metastasis (Months) (Mean ± SD) (Median/Mean, Range) | From Diagnosis of Primary Tumor to Surgery (Months) (Mean ± SD) (Median, Range) |
|---|---|---|---|---|---|
| Dijkstra et al. (1996) [1] | PF: Plate with bone cement INF: Antegrade nail without bipolar static locking for 2 cases; Interlocking nail with antegrade procedure for 9 cases, Retrograde operation in 7 cases | 33% of the patient cohort (17 Gy) | 25% of the PF group, and all the INF groups | Not-mentioned | Not-mentioned |
| Sarahrudi et al. (2009) [3] | PF: Dynamic compression plate in 18 patients, locking compression plate in 2 patients and Y-plate in 1 patient. All augmented with cement INF: Unreamed humeral nail in 15, a Seidel nail in 3, and an AR-Nail in 1 patient. | Not-mentioned | Not-mentioned | Not-mentioned | Not-mentioned |
| Wedin et al. (2012) [13] | PF: Plate without bone cement INF: Interlocked intramedullary nail | No diaphysis-limited data | Routinely | 10, 0–288 (median, range) (Not diaphysis-limited) | 23, 0–289 (median, range) (Not diaphysis-limited) |
| Schwabe et al. (2014) [17] | PF: Locking-compression plate with bone cement INF: Intramedullary nail | No diaphysis-limited data | No diaphysis-limited data | 14.5, 0–173 (mean, range) | 21.4, 0–173 (median, range) |
| Janssen et al. (2016) [12] | PF: Plate-screw fixation with bone cement in 19 cases; Plate-screw fixation without bone cement in 20 cases INF: Interlocked intramedullary nail | No diaphysis-limited data | Not-mentioned | Not-mentioned | Not-mentioned |
| Casadei et al. (2018) [14] | PF: Plate with bone cement INF: Interlocked intramedullary nail | Not-mentioned | 33% of the patient cohort | Not-mentioned | Not-mentioned |
| Ricard et al. (2021) [16] | PF: Plate with bone cement in 9 cases; plate without bone cement in 1 case INF: Intramedullary nail with cement in 2 cases, without cement in 6 cases | 16.7% of the patient cohort received | 5.6% of the patient cohort received | Not-mentioned | Not-mentioned |
| Zhao et al. (2021) [9] | PF: Plate with bone cement INF: Interlocked intramedullary nail | 31.7% of the patient cohort received | 4 weeks postoperatively | 13.5 ± 25.6 | Not-mentioned |
| Koob et al. (2022) [15] | PF: Plate with bone cement INF: Intramedullary nail with bone cement | Not-mentioned | Not-mentioned | Not-mentioned | Not-mentioned |
| Features of PHSF | Short-Term Care | Long-Term Care |
|---|---|---|
| Large solitary lesion | PF | PF |
| Impending fracture or multiple lesions | INF | INF |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Chen, B.-K.; Tai, T.-H.; Lin, S.-H.; Chen, K.-H.; Huang, Y.-M.; Chen, C.-Y. Intramedullary Nail vs. Plate Fixation for Pathological Humeral Shaft Fracture: An Updated Narrative Review and Meta-Analysis of Surgery-Related Factors. J. Clin. Med. 2024, 13, 755. https://doi.org/10.3390/jcm13030755
Chen B-K, Tai T-H, Lin S-H, Chen K-H, Huang Y-M, Chen C-Y. Intramedullary Nail vs. Plate Fixation for Pathological Humeral Shaft Fracture: An Updated Narrative Review and Meta-Analysis of Surgery-Related Factors. Journal of Clinical Medicine. 2024; 13(3):755. https://doi.org/10.3390/jcm13030755
Chicago/Turabian StyleChen, Bing-Kuan, Ting-Han Tai, Shu-Hsuan Lin, Kuan-Hao Chen, Yu-Min Huang, and Chih-Yu Chen. 2024. "Intramedullary Nail vs. Plate Fixation for Pathological Humeral Shaft Fracture: An Updated Narrative Review and Meta-Analysis of Surgery-Related Factors" Journal of Clinical Medicine 13, no. 3: 755. https://doi.org/10.3390/jcm13030755
APA StyleChen, B.-K., Tai, T.-H., Lin, S.-H., Chen, K.-H., Huang, Y.-M., & Chen, C.-Y. (2024). Intramedullary Nail vs. Plate Fixation for Pathological Humeral Shaft Fracture: An Updated Narrative Review and Meta-Analysis of Surgery-Related Factors. Journal of Clinical Medicine, 13(3), 755. https://doi.org/10.3390/jcm13030755