

Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis

 , ,
, , 
 , and
, and 
Abstract
1. Introduction
2. Materials and Methods
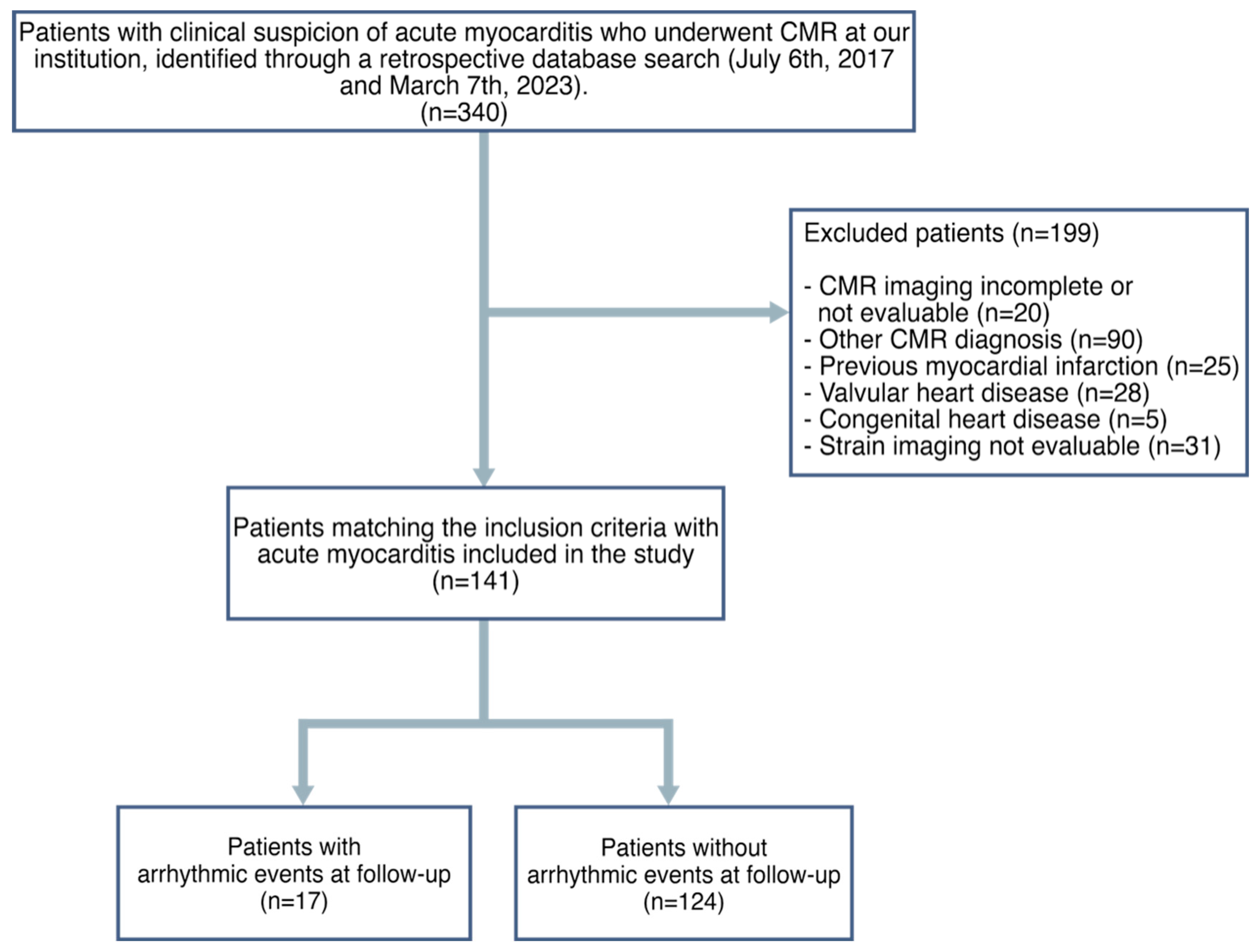
2.1. Study Population
2.2. CMR Acquisition
2.3. CMR Image Post-Processing
2.4. Study End Points
2.5. Statistical Analysis
3. Results
3.1. Patient Population
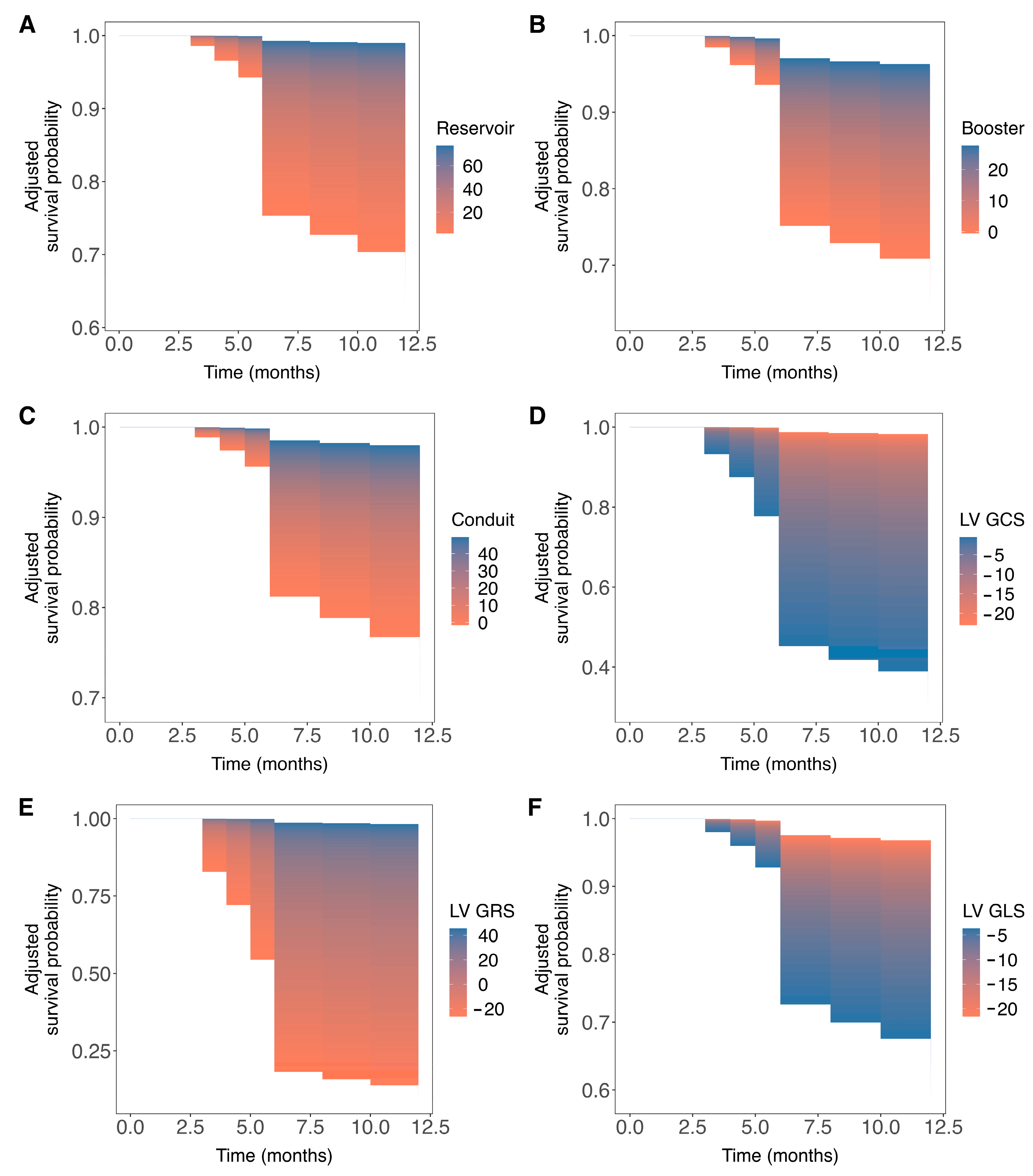
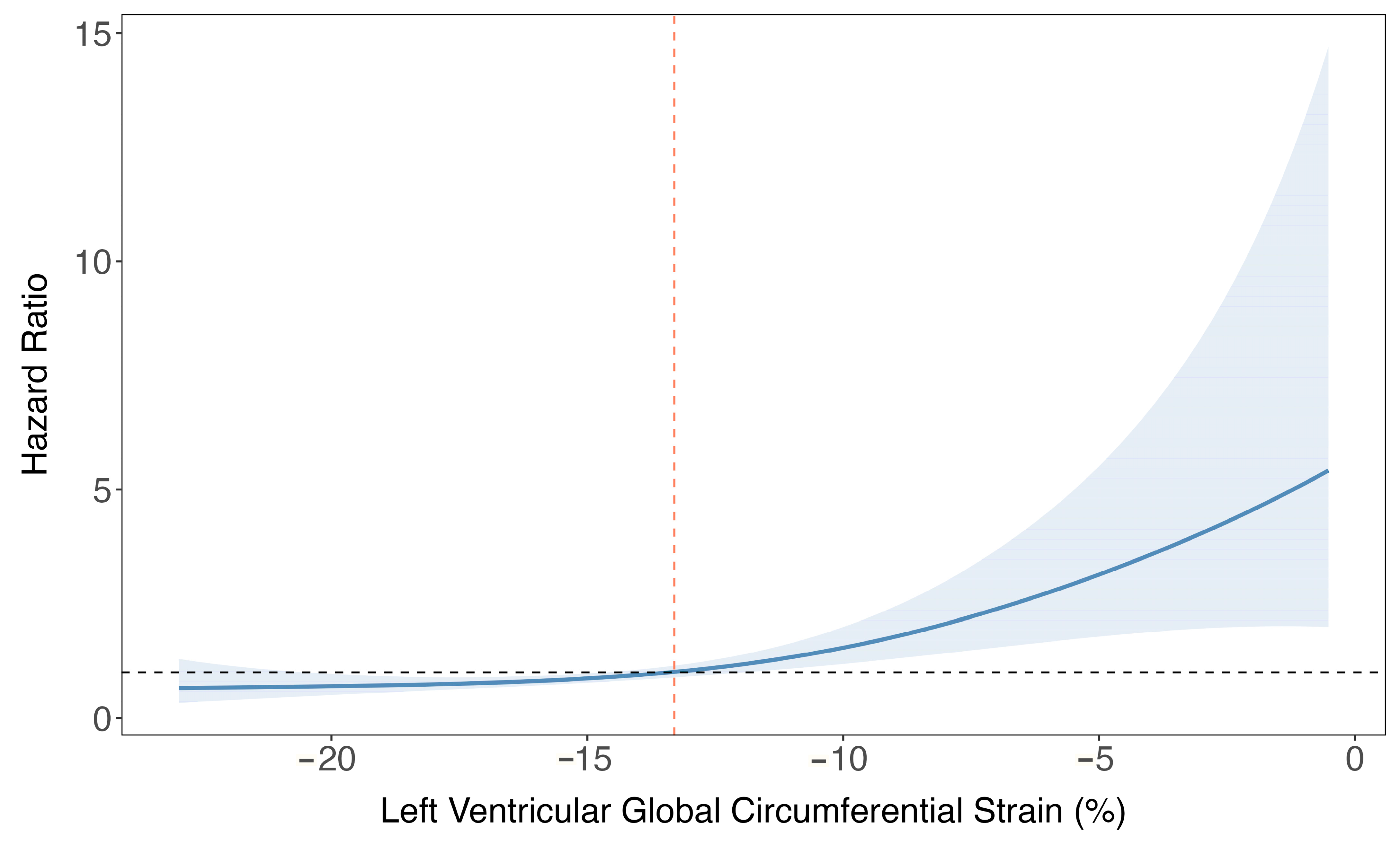
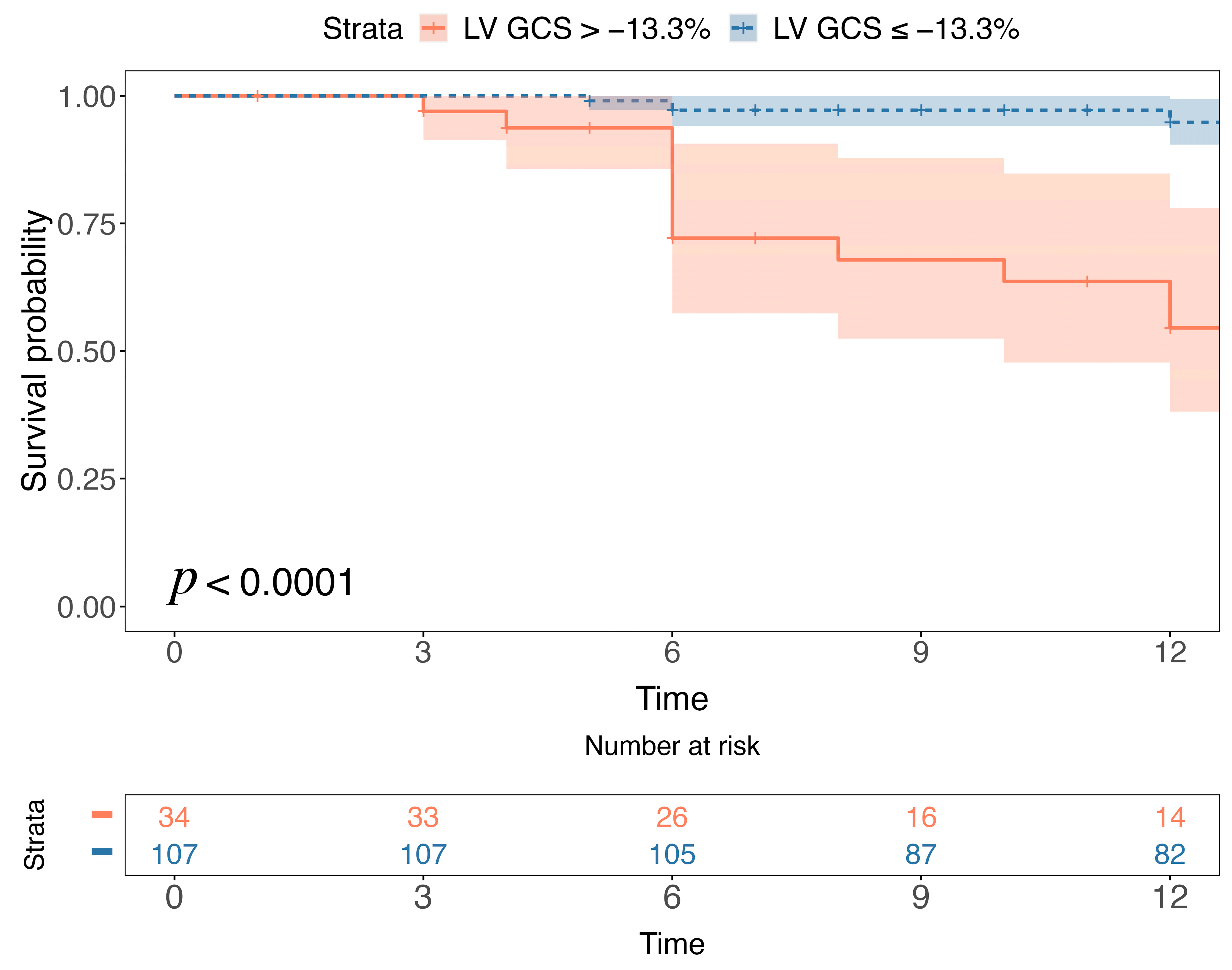
3.2. Associations of Ventricular and Atrial Strain Measures with Ventricular Arrhythmia Risk
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Tschöpe, C.; Ammirati, E.; Bozkurt, B.; Caforio, A.L.P.; Cooper, L.T.; Felix, S.B.; Hare, J.M.; et al. Myocarditis and inflammatory cardiomyopathy: Current evidence and future directions. Nat. Rev. Cardiol. 2021, 18, 169–193. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Frigerio, M.; Adler, E.D.; Basso, C.; Birnie, D.H.; Brambatti, M.; Friedrich, M.G.; Klingel, K.; Lehtonen, J.; Moslehi, J.J.; et al. Management of Acute Myocarditis and Chronic Inflammatory Cardiomyopathy: An Expert Consensus Document. Circ. Heart Fail. 2020, 13, e007405. [Google Scholar] [CrossRef] [PubMed]
- Ammirati, E.; Cipriani, M.; Moro, C.; Raineri, C.; Pini, D.; Sormani, P.; Mantovani, R.; Varrenti, M.; Pedrotti, P.; Conca, C.; et al. Clinical Presentation and Outcome in a Contemporary Cohort of Patients with Acute Myocarditis: Multicenter Lombardy Registry. Circulation 2018, 138, 1088–1099. [Google Scholar] [CrossRef] [PubMed]
- Caforio, A.L.P.; Marcolongo, R.; Basso, C.; Iliceto, S. Clinical presentation and diagnosis of myocarditis. Heart 2015, 101, 1332–1344. [Google Scholar] [CrossRef] [PubMed]
- Fung, G.; Luo, H.; Qiu, Y.; Yang, D.; McManus, B. Myocarditis. Circ. Res. 2016, 118, 496–514. [Google Scholar] [CrossRef] [PubMed]
- Al-Khatib, S.M.; Stevenson, W.G.; Ackerman, M.J.; Bryant, W.J.; Callans, D.J.; Curtis, A.B.; Deal, B.J.; Dickfeld, T.; Field, M.E.; Fonarow, G.C.; et al. 2017 AHA/ACC/HRS Guideline for Management of Patients with Ventricular Arrhythmias and the Prevention of Sudden Cardiac Death: Executive Summary: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Gu. Circulation 2018, 138, e210–e271. [Google Scholar] [CrossRef]
- Caforio, A.L.; Pankuweit, S.; Arbustini, E.; Basso, C.; Gimeno-Blanes, J.; Felix, S.B.; Fu, M.; Heliö, T.; Heymans, S.; Jahns, R.; et al. Current state of knowledge on aetiology, diagnosis, management, and therapy of myocarditis: A position statement of the European Society of Cardiology Working Group on Myocardial and Pericardial Diseases. Eur. Heart J. 2013, 34, 2636–2648. [Google Scholar] [CrossRef]
- Cau, R.; Muscogiuri, G.; Pisu, F.; Mannelli, L.; Sironi, S.; Suri, J.S.; Pontone, G.; Saba, L. Effect of late gadolinium enhancement on left atrial impairment in myocarditis patients. Eur. Radiol. 2023, 0123456789. [Google Scholar] [CrossRef]
- Cau, R.; Pisu, F.; Suri, J.S.; Montisci, R.; Bastarrika, G.; Esposito, A.; Saba, L. Sex-based differences in late gadolinium enhancement among patients with acute myocarditis. Eur. J. Radiol. 2023, 166, 110980. [Google Scholar] [CrossRef] [PubMed]
- Ferreira, V.M.; Schulz-Menger, J.; Holmvang, G.; Kramer, C.M.; Carbone, I.; Sechtem, U.; Kindermann, I.; Gutberlet, M.; Cooper, L.T.; Liu, P.; et al. Cardiovascular Magnetic Resonance in Nonischemic Myocardial Inflammation: Expert Recommendations. J. Am. Coll. Cardiol. 2018, 72, 3158–3176. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Perfetti, M.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Pepe, A.; Todiere, G.; Lanzillo, C.; Scatteia, A.; et al. Cardiac MR With Late Gadolinium Enhancement in Acute Myocarditis with Preserved Systolic Function: ITAMY Study. J. Am. Coll. Cardiol. 2017, 70, 1977–1987. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Ghebru Habtemicael, Y.; Camastra, G.; Monti, L.; Dellegrottaglie, S.; Moro, C.; Lanzillo, C.; Scatteia, A.; Di Roma, M.; Pontone, G.; et al. Prognostic Value of Repeating Cardiac Magnetic Resonance in Patients with Acute Myocarditis. J. Am. Coll. Cardiol. 2019, 74, 2439–2448. [Google Scholar] [CrossRef] [PubMed]
- Gräni, C.; Eichhorn, C.; Bière, L.; Murthy, V.L.; Agarwal, V.; Kaneko, K.; Cuddy, S.; Aghayev, A.; Steigner, M.; Blankstein, R.; et al. Prognostic Value of Cardiac Magnetic Resonance Tissue Characterization in Risk Stratifying Patients with Suspected Myocarditis. J. Am. Coll. Cardiol. 2017, 70, 1964–1976. [Google Scholar] [CrossRef] [PubMed]
- Casella, M.; Bergonti, M.; Narducci, M.L.; Persampieri, S.; Gasperetti, A.; Conte, E.; Catto, V.; Carbucicchio, C.; Guerra, F.; Pontone, G.; et al. Prior myocarditis and ventricular arrhythmias: The importance of scar pattern. Heart Rhythm 2021, 18, 589–596. [Google Scholar] [CrossRef] [PubMed]
- Georgiopoulos, G.; Figliozzi, S.; Sanguineti, F.; Aquaro, G.D.; di Bella, G.; Stamatelopoulos, K.; Chiribiri, A.; Garot, J.; Masci, P.G.; Ismail, T.F. Prognostic Impact of Late Gadolinium Enhancement by Cardiovascular Magnetic Resonance in Myocarditis. Circ. Cardiovasc. Imaging 2021, 14, e011492. [Google Scholar] [CrossRef] [PubMed]
- Scatteia, A.; Baritussio, A.; Bucciarelli-Ducci, C. Strain imaging using cardiac magnetic resonance. Heart Fail. Rev. 2017, 22, 465–476. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Bassareo, P.; Suri, J.S.; Pontone, G.; Saba, L. The emerging role of atrial strain assessed by cardiac MRI in different cardiovascular settings: An up-to-date review. Eur. Radiol. 2022, 32, 4384–4394. [Google Scholar] [CrossRef]
- Muscogiuri, G.; Guglielmo, M.; Serra, A.; Gatti, M.; Volpato, V.; Schoepf, U.J.; Saba, L.; Cau, R.; Faletti, R.; McGill, L.J.; et al. Multimodality Imaging in Ischemic Chronic Cardiomyopathy. J. Imaging 2022, 8, 35. [Google Scholar] [CrossRef]
- Doerner, J.; Bunck, A.C.; Michels, G.; Maintz, D.; Baeßler, B. Incremental value of cardiovascular magnetic resonance feature tracking derived atrial and ventricular strain parameters in a comprehensive approach for the diagnosis of acute myocarditis. Eur. J. Radiol. 2018, 104, 120–128. [Google Scholar] [CrossRef]
- Secchi, F.; Monti, C.B.; Alì, M.; Carbone, F.S.; Cannaò, P.M.; Sardanelli, F. Diagnostic Value of Global Cardiac Strain in Patients with Myocarditis. J. Comput. Assist. Tomogr. 2020, 44, 591–598. [Google Scholar] [CrossRef]
- Luetkens, J.A.; Schlesinger-Irsch, U.; Kuetting, D.L.; Dabir, D.; Homsi, R.; Doerner, J.; Schmeel, F.C.; Fimmers, R.; Sprinkart, A.M.; Naehle, C.P.; et al. Feature-tracking myocardial strain analysis in acute myocarditis: Diagnostic value and association with myocardial oedema. Eur. Radiol. 2017, 27, 4661–4671. [Google Scholar] [CrossRef] [PubMed]
- Bernhard, B.; Tanner, G.; Garachemani, D.; Schnyder, A.; Fischer, K.; Huber, A.T.; Safarkhanlo, Y.; Stark, A.W.; Guensch, D.P.; Schütze, J.; et al. Predictive value of cardiac magnetic resonance right ventricular longitudinal strain in patients with suspected myocarditis. J. Cardiovasc. Magn. Reson. 2023, 25, 49. [Google Scholar] [CrossRef] [PubMed]
- Vos, J.L.; Raafs, A.G.; van der Velde, N.; Germans, T.; Biesbroek, P.S.; Roes, K.; Hirsch, A.; Heymans, S.R.B.; Nijveldt, R. Comprehensive Cardiovascular Magnetic Resonance-Derived Myocardial Strain Analysis Provides Independent Prognostic Value in Acute Myocarditis. J. Am. Heart Assoc. 2022, 11, e025106. [Google Scholar] [CrossRef] [PubMed]
- Porcari, A.; Merlo, M.; Baggio, C.; Gagno, G.; Cittar, M.; Barbati, G.; Paldino, A.; Castrichini, M.; Vitrella, G.; Pagnan, L.; et al. Global longitudinal strain by CMR improves prognostic stratification in acute myocarditis presenting with normal LVEF. Eur. J. Clin. Investig. 2022, 52, e13815. [Google Scholar] [CrossRef] [PubMed]
- Fischer, K.; Obrist, S.J.; Erne, S.A.; Stark, A.W.; Marggraf, M.; Kaneko, K.; Guensch, D.P.; Huber, A.T.; Greulich, S.; Aghayev, A.; et al. Feature Tracking Myocardial Strain Incrementally Improves Prognostication in Myocarditis Beyond Traditional CMR Imaging Features. JACC Cardiovasc. Imaging 2020, 13, 1891–1901. [Google Scholar] [CrossRef] [PubMed]
- Bulluck, H.; Carberry, J.; Carrick, D.; McCartney, P.J.; Maznyczka, A.M.; Greenwood, J.P.; Maredia, N.; Chowdhary, S.; Gershlick, A.H.; Appleby, C.; et al. A Noncontrast CMR Risk Score for Long-Term Risk Stratification in Reperfused ST-Segment Elevation Myocardial Infarction. JACC Cardiovasc. Imaging 2022, 15, 431–440. [Google Scholar] [CrossRef]
- Baggiano, A.; Boldrini, M.; Martinez-Naharro, A.; Kotecha, T.; Petrie, A.; Rezk, T.; Gritti, M.; Quarta, C.; Knight, D.S.; Wechalekar, A.D.; et al. Noncontrast Magnetic Resonance for the Diagnosis of Cardiac Amyloidosis. JACC Cardiovasc. Imaging 2020, 13 Pt 1, 69–80. [Google Scholar] [CrossRef]
- Raucci, F.J., Jr.; Xu, M.; George-Durrett, K.; Crum, K.; Slaughter, J.C.; Parra, D.A.; Markham, L.W.; Soslow, J.H. Non-contrast cardiovascular magnetic resonance detection of myocardial fibrosis in Duchenne muscular dystrophy. J. Cardiovasc. Magn. Reson. 2021, 23, 48. [Google Scholar] [CrossRef]
- Salehi Ravesh, M.; Eden, M.; Langguth, P.; Piesch, T.C.; Lehmann, J.K.; Lebenatus, A.; Hauttemann, D.; Graessner, J.; Frey, N.; Jansen, O.; et al. Non-contrast enhanced diagnosis of acute myocarditis based on the 17-segment heart model using 2D-feature tracking magnetic resonance imaging. Magn. Reson. Imaging 2020, 65, 155–165. [Google Scholar] [CrossRef]
- Abdel-Gadir, A.; Vorasettakarnkij, Y.; Ngamkasem, H.; Nordin, S.; Ako, E.A.; Tumkosit, M.; Sucharitchan, P.; Uaprasert, N.; Kellman, P.; Piechnik, S.K.; et al. Ultrafast magnetic resonance imaging for iron quantification in thalassemia participants in the developing world: The TIC-TOC Study (Thailand and UK International Collaboration in Thalassaemia Optimising Ultrafast CMR). Circulation 2016, 134, 432–434. [Google Scholar] [CrossRef]
- Raman, S.V.; Markl, M.; Patel, A.R.; Bryant, J.; Allen, B.D.; Plein, S.; Seiberlich, N. 30-minute CMR for common clinical indications: A Society for Cardiovascular Magnetic Resonance white paper. J. Cardiovasc. Magn. Reson. 2022, 24, 13. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Pisu, F.; Suri, J.S.; Mannelli, L.; Scaglione, M.; Masala, S.; Saba, L. Artificial Intelligence Applications in Cardiovascular Magnetic Resonance Imaging: Are We on the Path to Avoiding the Administration of Contrast Media? Diagnostics 2023, 13, 2061. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Pisu, F.; Porcu, M.; Cademartiri, F.; Montisci, R.; Bassareo, P.; Muscogiuri, G.; Amadu, A.; Sironi, S.; Esposito, A.; et al. Machine learning approach in diagnosing Takotsubo cardiomyopathy: The role of the combined evaluation of atrial and ventricular strain, and parametric mapping. Int. J. Cardiol. 2022, 373, 124–133. [Google Scholar] [CrossRef] [PubMed]
- Unger, T.; Borghi, C.; Charchar, F.; Khan, N.A.; Poulter, N.R.; Prabhakaran, D.; Ramirez, A.; Schlaich, M.; Stergiou, G.S.; Tomaszewski, M.; et al. 2020 International Society of Hypertension Global Hypertension Practice Guidelines. Hypertension 2020, 75, 1334–1357. [Google Scholar] [CrossRef]
- World Health Organization. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycaemia: Report of a WHO/IDF Consultation; WHO: Geneva, Switzerland, 2006. [Google Scholar]
- Flegal, K.M.; Carroll, M.D.; Kuczmarski, R.J.; Johnson, C.L. Overweight and obesity in the United States: Prevalence and trends, 1960–1994. Int. J. Obes. 1998, 22, 39–47. [Google Scholar] [CrossRef] [PubMed]
- Robins, J. A new approach to causal inference in mortality studies with a sustained exposure period—Application to control of the healthy worker survivor effect. Math. Model. 1986, 7, 1393–1512. [Google Scholar] [CrossRef]
- Peretto, G.; Sala, S.; Lazzeroni, D.; Palmisano, A.; Gigli, L.; Esposito, A.; De Cobelli, F.; Camici, P.G.; Mazzone, P.; Basso, C.; et al. Septal Late Gadolinium Enhancement and Arrhythmic Risk in Genetic and Acquired Non-Ischaemic Cardiomyopathies. Heart Lung Circ. 2020, 29, 1356–1365. [Google Scholar] [CrossRef]
- Peretto, G.; Sala, S.; Rizzo, S.; Palmisano, A.; Esposito, A.; De Cobelli, F.; Campochiaro, C.; De Luca, G.; Foppoli, L.; Dagna, L.; et al. Ventricular Arrhythmias in Myocarditis: Characterization and Relationships with Myocardial Inflammation. J. Am. Coll. Cardiol. 2020, 75, 1046–1057. [Google Scholar] [CrossRef]
- Cau, R.; Bassareo, P.; Caredda, G.; Suri, J.S.; Esposito, A.; Saba, L. Atrial Strain by Feature-Tracking Cardiac Magnetic Resonance Imaging in Takotsubo Cardiomyopathy. Features, Feasibility, and Reproducibility. Can. Assoc. Radiol. J. 2021, 73, 8465371211042497. [Google Scholar] [CrossRef]
- Cau, R.; Bassareo, P.; Deidda, M.; Caredda, G.; Suri, J.S.; Pontone, G.; Saba, L. Could CMR Tissue-Tracking and Parametric Mapping Distinguish between Takotsubo Syndrome and Acute Myocarditis? A Pilot Study. Acad. Radiol. 2021, 29, S33–S39. [Google Scholar] [CrossRef]
- Hinojar, R.; Zamorano, J.L.; Fernández-Méndez, M.; Esteban, A.; Plaza-Martin, M.; González-Gómez, A.; Carbonell, A.; Rincón, L.M.; Nácher, J.J.J.; Fernández-Golfín, C. Prognostic value of left atrial function by cardiovascular magnetic resonance feature tracking in hypertrophic cardiomyopathy. Int. J. Cardiovasc. Imaging 2019, 35, 1055–1065. [Google Scholar] [CrossRef] [PubMed]
- Schuster, A.; Backhaus, S.J.; Stiermaier, T.; Navarra, J.L.; Uhlig, J.; Rommel, K.P.; Koschalka, A.; Kowallick, J.T.; Bigalke, B.; Kutty, S.; et al. Impact of Right Atrial Physiology on Heart Failure and Adverse Events after Myocardial Infarction. J. Clin. Med. 2020, 9, 210. [Google Scholar] [CrossRef] [PubMed]
- Fong, L.C.W.; Lee, N.H.C.; Poon, J.W.L.; Chin, C.W.L.; He, B.; Luo, L.; Chen, C.; Wan, E.Y.F.; Pennell, D.J.; Mohiaddin, R.; et al. Prognostic value of cardiac magnetic resonance derived global longitudinal strain analysis in patients with ischaemic and non-ischaemic dilated cardiomyopathy: A systematic review and meta-analysis. Int. J. Cardiovasc. Imaging 2022, 38, 2707–2721. [Google Scholar] [CrossRef] [PubMed]
- Ersbøll, M.; Valeur, N.; Andersen, M.J.; Mogensen, U.M.; Vinther, M.; Svendsen, J.H.; Møller, J.E.; Kisslo, J.; Velazquez, E.J.; Hassager, C.; et al. Early echocardiographic deformation analysis for the prediction of sudden cardiac death and life-threatening arrhythmias after myocardial infarction. JACC Cardiovasc. Imaging 2013, 6, 851–860. [Google Scholar] [CrossRef] [PubMed]
- Bjerregaard, C.L.; Skaarup, K.G.; Lassen, M.C.; Biering-Sørensen, T.; Olsen, F.J. Strain Imaging and Ventricular Arrhythmia. Diagnostics 2023, 13, 1778. [Google Scholar] [CrossRef] [PubMed]
- Tang, X.; Yu, S.; Yu, Y.; Ren, H.; Li, S.; Zhou, L.; Yang, Z.; Wu, H.; Zhou, W.; Gong, L. Left ventricular myocardial strain in ventricular arrhythmia without structural heart disease using cardiac magnetic resonance. Am. J. Transl. Res. 2017, 9, 3006–3016. [Google Scholar] [PubMed]
- Candan, Ö.; Geçmen, Ç.; Kahyaoğlu, M.; Çelik, M.; Şimşek, Z.; Dindaş, F.; Doğduş, M.; Zehir, R.; Kırma, C. Left Atrial Dysfunction as Marker of Arrhythmic Events in Patients with Hypertrophic Cardiomyopathy. Anatol. J. Cardiol. 2022, 26, 771–777. [Google Scholar] [CrossRef]
- Pu, C.; Fei, J.; Lv, S.; Wu, Y.; He, C.; Guo, D.; Mabombo, P.U.; Chooah, O.; Hu, H. Global Circumferential Strain by Cardiac Magnetic Resonance Tissue Tracking Associated with Ventricular Arrhythmias in Hypertrophic Cardiomyopathy Patients. Front. Cardiovasc. Med. 2021, 8, 670361. [Google Scholar] [CrossRef]
- Paiman, E.H.M.; Androulakis, A.F.A.; Shahzad, R.; Tao, Q.; Zeppenfeld, K.; Lamb, H.J.; van der Geest, R.J. Association of cardiovascular magnetic resonance-derived circumferential strain parameters with the risk of ventricular arrhythmia and all-cause mortality in patients with prior myocardial infarction and primary prevention implantable cardioverter defibri. J. Cardiovasc. Magn. Reson. 2019, 21, 28. [Google Scholar] [CrossRef]
- Dello Russo, A.; Casella, M.; Pieroni, M.; Pelargonio, G.; Bartoletti, S.; Santangeli, P.; Zucchetti, M.; Innocenti, E.; Di Biase, L.; Carbucicchio, C.; et al. Drug-Refractory Ventricular Tachycardias after Myocarditis. Circ. Arrhythmia Electrophysiol. 2012, 5, 492–498. [Google Scholar] [CrossRef]
- Chaumont, C.; Suffee, N.; Gandjbakhch, E.; Balse, E.; Anselme, F.; Hatem, S.N. Epicardial origin of cardiac arrhythmias: Clinical evidences and pathophysiology. Cardiovasc. Res. 2022, 118, 1693–1702. [Google Scholar] [CrossRef] [PubMed]
- Cau, R.; Loewe, C.; Cherchi, V.; Porcu, M.; Ciet, P.; Suri, J.S.; Saba, L. Atrial Impairment as a Marker in Discriminating between Takotsubo and Acute Myocarditis Using Cardiac Magnetic Resonance. J. Thorac. Imaging 2022, 37, W78–W84. [Google Scholar] [CrossRef] [PubMed]
- Wu, L.; Fiet, M.D.; Raaijmakers, D.R.; Woudstra, L.; van Rossum, A.C.; Niessen, H.W.M.; Krijnen, P.A.J. Transient atrial inflammation in a murine model of Coxsackievirus B3-induced myocarditis. Int. J. Exp. Pathol. 2022, 103, 149–155. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | Overall, n = 141 1 | Event, n = 17 1 | No Event, n = 124 1 | p-Value 2 |
|---|---|---|---|---|
| Gender (male) | 112 (79%) | 14 (82%) | 98 (79%) | >0.99 |
| Age, years | 40 (22, 56) | 56 (50, 70) | 37 (21, 52) | <0.001 |
| Height, cm | 170 (170, 175) | 170 (168, 175) | 170 (170, 175) | 0.89 |
| Weight, kg | 72 (63, 82) | 80 (72, 90) | 70 (60, 79) | 0.020 |
| BSA, m2 | 1.86 (1.72, 1.98) | 1.88 (1.76, 2.05) | 1.82 (1.69, 1.94) | 0.25 |
| Hypertension | 26 (18%) | 7 (41%) | 19 (15%) | 0.018 |
| Dyslipidemia | 16 (11%) | 5 (29%) | 11 (8.9%) | 0.027 |
| Obesity | 16 (11%) | 5 (29%) | 11 (8.9%) | 0.027 |
| Current or previous smoking | 20 (14%) | 2 (12%) | 18 (15%) | >0.99 |
| Diabetes mellitus | 6 (4.3%) | 3 (18%) | 3 (2.4%) | 0.023 |
| Family history of coronary disease | 30 (21%) | 4 (24%) | 26 (21%) | 0.76 |
| Chest pain | 125 (89%) | 9 (53%) | 116 (94%) | <0.001 |
| Heart failure | 11 (7.8%) | 4 (24%) | 7 (5.6%) | 0.029 |
| Arrhythmias | 14 (9.9%) | 10 (59%) | 4 (3.2%) | <0.001 |
| Reservoir, % | 30 (24, 38) | 20 (10, 29) | 30 (25, 39) | <0.001 |
| Conduit, % | 18 (12, 23) | 8 (5, 15) | 18 (14, 23) | <0.001 |
| Booster, % | 12.2 (9.8, 16.0) | 11.2 (7.2, 14.3) | 12.8 (10.1, 16.0) | 0.10 |
| LVEF, % | 56 (50, 61) | 49 (41, 58) | 57 (52, 61) | 0.022 |
| LV EDV/BSA, mL/m2 | 92 (80, 103) | 96 (84, 129) | 91 (80, 102) | 0.054 |
| LV ESV/BSA, mL/m2 | 40 (32, 48) | 51 (41, 75) | 39 (32, 45) | 0.023 |
| LV SV/BSA, mL/m2 | 51 (45, 57) | 47 (42, 52) | 52 (46, 57) | 0.22 |
| RVEF, % | 55.7 (52.0, 58.7) | 51.3 (49.2, 58.9) | 55.9 (52.4, 58.6) | 0.17 |
| RV EDV/BSA, mL/m2 | 82 (71, 95) | 81 (72, 88) | 82 (71, 96) | 0.68 |
| RV ESV/BSA, mL/m2 | 35 (30, 43) | 36 (29, 44) | 35 (30, 43) | 0.73 |
| RV SV, mL/m2 | 46 (38, 53) | 39 (37, 47) | 46 (40, 53) | 0.082 |
| LV GRS, % | 22 (18, 29) | 16 (13, 20) | 23 (19, 29) | <0.001 |
| LV GCS, % | −14.4 (−17.0, −12.2) | −11.1 (−13.6, −9.3) | −14.9 (−17.3, −12.5) | <0.001 |
| LV GLS, % | −13.9 (−15.5, −12.1) | −9.3 (−12.2, −8.3) | −14.3 (−15.5, −12.6) | <0.001 |
| LGE, number of AHA segments | 69 (49%) | 8 (47%) | 61 (49%) | 0.87 |
| LGE septal | 32 (23%) | 9 (53%) | 23 (19%) | 0.004 |
| LGE mass, % | 9 (4, 13) | 11 (5, 16) | 8 (4, 13) | 0.35 |
| LGE mass, g | 7 (3, 11) | 8 (5, 12) | 6 (3, 11) | 0.24 |
| Pericardial involvement | 34 (24%) | 3 (18%) | 31 (25%) | 0.76 |
| T2 total, ms | 59.3 (55.8, 63.1) | 61.4 (59.5, 63.9) | 59.0 (55.6, 62.6) | 0.047 |
| Variable | Hazard Ratio (95% CI) | p-Value |
|---|---|---|
| Gender | 1.4 (0.39–4.7) | 0.63 |
| Age | 1.1 (1–1.1) | <0.001 |
| Height | 1 (0.94–1.1) | 0.89 |
| Weight | 1 (1–1.1) | 0.017 |
| BSA | 3 (0.32–29) | 0.33 |
| Hypertension | 3.5 (1.3–9.3) | 0.01 |
| Dyslipidemia | 4.2 (1.5–12) | 0.0072 |
| Obesity | 4 (1.4–11) | 0.0096 |
| Current or previous smoking | 0.8 (0.18–3.5) | 0.77 |
| Diabetes mellitus | 7.2 (2.1–25) | 0.0021 |
| Family history of coronary disease | 1.1 (0.35–3.3) | 0.9 |
| Chest pain | 0.1 (0.039–0.26) | <0.001 |
| Heart failure | 6 (1.9–18) | 0.002 |
| Arrhythmias | 23 (8.8–63) | <0.001 |
| Reservoir | 0.9 (0.86–0.94) | <0.001 |
| Conduit | 0.87 (0.82–0.93) | <0.001 |
| Booster | 0.88 (0.79–0.97) | 0.012 |
| LVEF | 0.93 (0.89–0.96) | <0.001 |
| LV EDV/BSA | 1 (1–1) | <0.001 |
| LV ESV/BSA | 1 (1–1) | 0.0025 |
| LV SV/BSA | 0.96 (0.91–1) | 0.12 |
| RVEF | 0.96 (0.89–1) | 0.19 |
| RV EDV/BSA | 0.99 (0.97–1) | 0.54 |
| RV ESV/BSA | 0.98 (0.93–1) | 0.33 |
| RV SV | 0.96 (0.92–1) | 0.093 |
| LV GRS | 0.95 (0.92–0.98) | 0.0012 |
| LV GCS | 1.2 (1.1–1.3) | <0.001 |
| LV GLS | 1.4 (1.2–1.6) | <0.001 |
| LGE, number of AHA segments | 1.1 (0.41–2.8) | 0.88 |
| LGE septal | 5.1 (2–13) | <0.001 |
| LGE mass, % | 1 (0.98–1.1) | 0.24 |
| LGE mass, g | 1 (0.99–1.1) | 0.11 |
| Pericardial involvement | 0.64 (0.18–2.2) | 0.48 |
| T2 total | 1.1 (0.99–1.2) | 0.083 |
| Multivariable Analysis | ||
|---|---|---|
| Hazard Ratio (95% CI) | p-Value | |
| Adjusted for sex and age 1 | ||
| Reservoir | 0.92 (0.87–0.97) | 0.002 |
| Booster | 0.85 (0.77–0.94) | 0.002 |
| Conduit | 0.91 (0.84–0.99) | 0.03 |
| LV GCS | 1.25 (1.11–1.40) | <0.001 |
| LV GRS | 0.93 (0.89–0.97) | <0.001 |
| LV GLS | 1.25 (1.08–1.43) | 0.002 |
| + cardiovascular risk factors 2 | ||
| Reservoir | 0.91 (0.87–0.96) | <0.001 |
| Booster | 0.84 (0.75–0.93) | 0.001 |
| Conduit | 0.89 (0.82–0.97) | 0.007 |
| LV GCS | 1.44 (1.20–1.72) | <0.001 |
| LV GRS | 0.87 (0.81–0.94) | <0.001 |
| LV GLS | 1.37 (1.16–1.61) | <0.001 |
| + LVEF 3 | ||
| Reservoir | 0.93 (0.88–0.99) | 0.03 |
| Booster | 0.89 (0.78–1.00) | 0.049 |
| Conduit | 0.93 (0.85–1.01) | 0.1 |
| LV GCS | 1.39 (1.12–1.73) | 0.003 |
| LV GRS | 0.89 (0.82–0.97) | 0.006 |
| LV GLS | 1.27 (1.03–1.56) | <0.001 |
| + LGE septal 4 | ||
| Reservoir | 0.93 (0.87–0.99) | 0.02 |
| Booster | 0.87 (0.76–0.99) | 0.04 |
| Conduit | 0.92 (0.84–1.02) | 0.1 |
| LV GCS | 1.37 (1.08–1.73) | 0.008 |
| LV GRS | 0.89 (0.80–0.98) | 0.01 |
| LV GLS | 1.26 (1.02–1.55) | 0.03 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cau, R.; Pisu, F.; Suri, J.S.; Pontone, G.; D’Angelo, T.; Zha, Y.; Salgado, R.; Saba, L. Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis. J. Clin. Med. 2024, 13, 662. https://doi.org/10.3390/jcm13030662
Cau R, Pisu F, Suri JS, Pontone G, D’Angelo T, Zha Y, Salgado R, Saba L. Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis. Journal of Clinical Medicine. 2024; 13(3):662. https://doi.org/10.3390/jcm13030662
Chicago/Turabian StyleCau, Riccardo, Francesco Pisu, Jasjit S. Suri, Gianluca Pontone, Tommaso D’Angelo, Yunfei Zha, Rodrigo Salgado, and Luca Saba. 2024. "Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis" Journal of Clinical Medicine 13, no. 3: 662. https://doi.org/10.3390/jcm13030662
APA StyleCau, R., Pisu, F., Suri, J. S., Pontone, G., D’Angelo, T., Zha, Y., Salgado, R., & Saba, L. (2024). Atrial and Ventricular Strain Imaging Using CMR in the Prediction of Ventricular Arrhythmia in Patients with Myocarditis. Journal of Clinical Medicine, 13(3), 662. https://doi.org/10.3390/jcm13030662