
Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women

 ,
,  ,
,  ,
,  ,
,  and
and 
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Description of the Questionnaire
- The first section collected general demographic and obstetric data, such as age, number of pregnancies, and the gestational month of the current pregnancy.
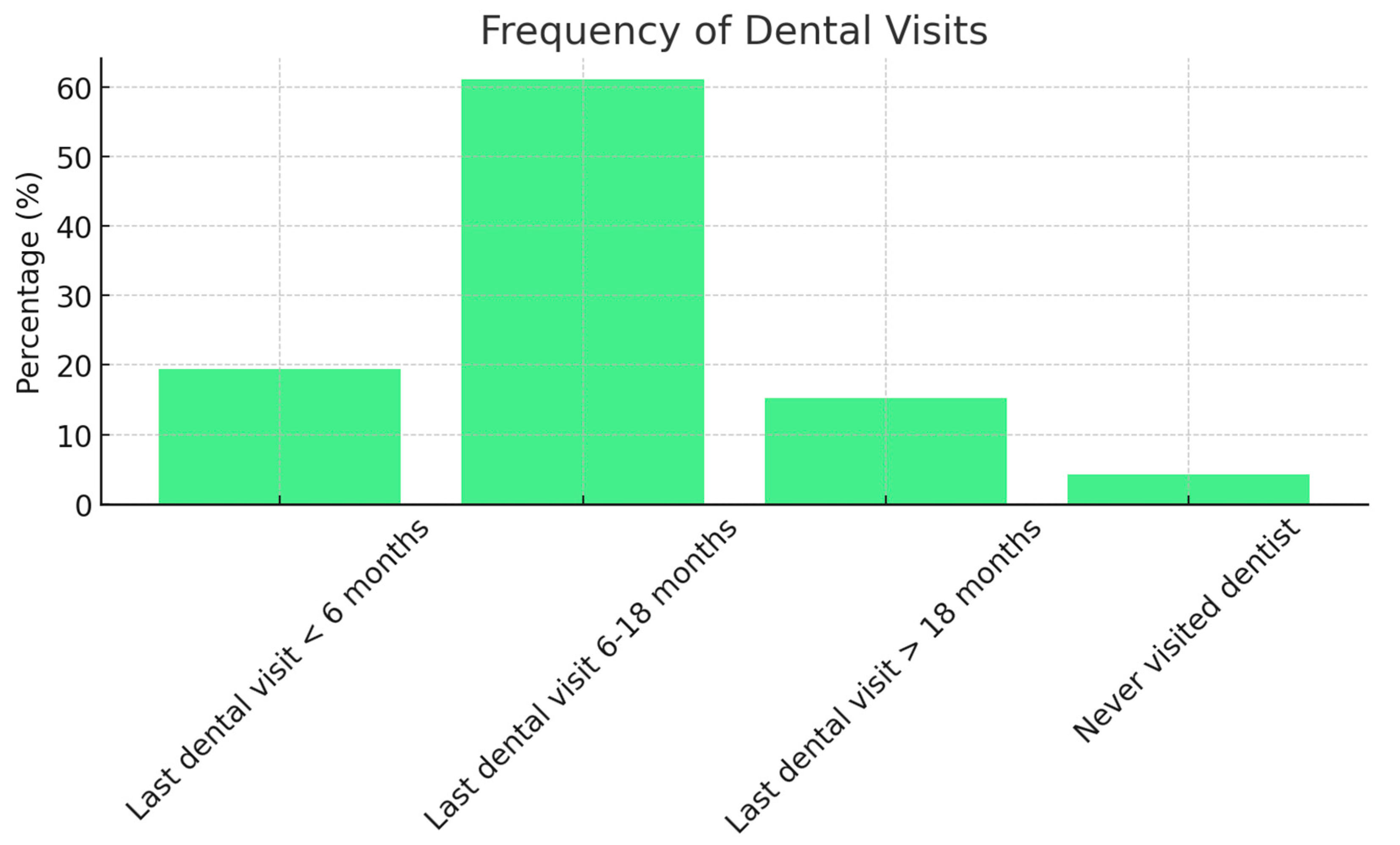
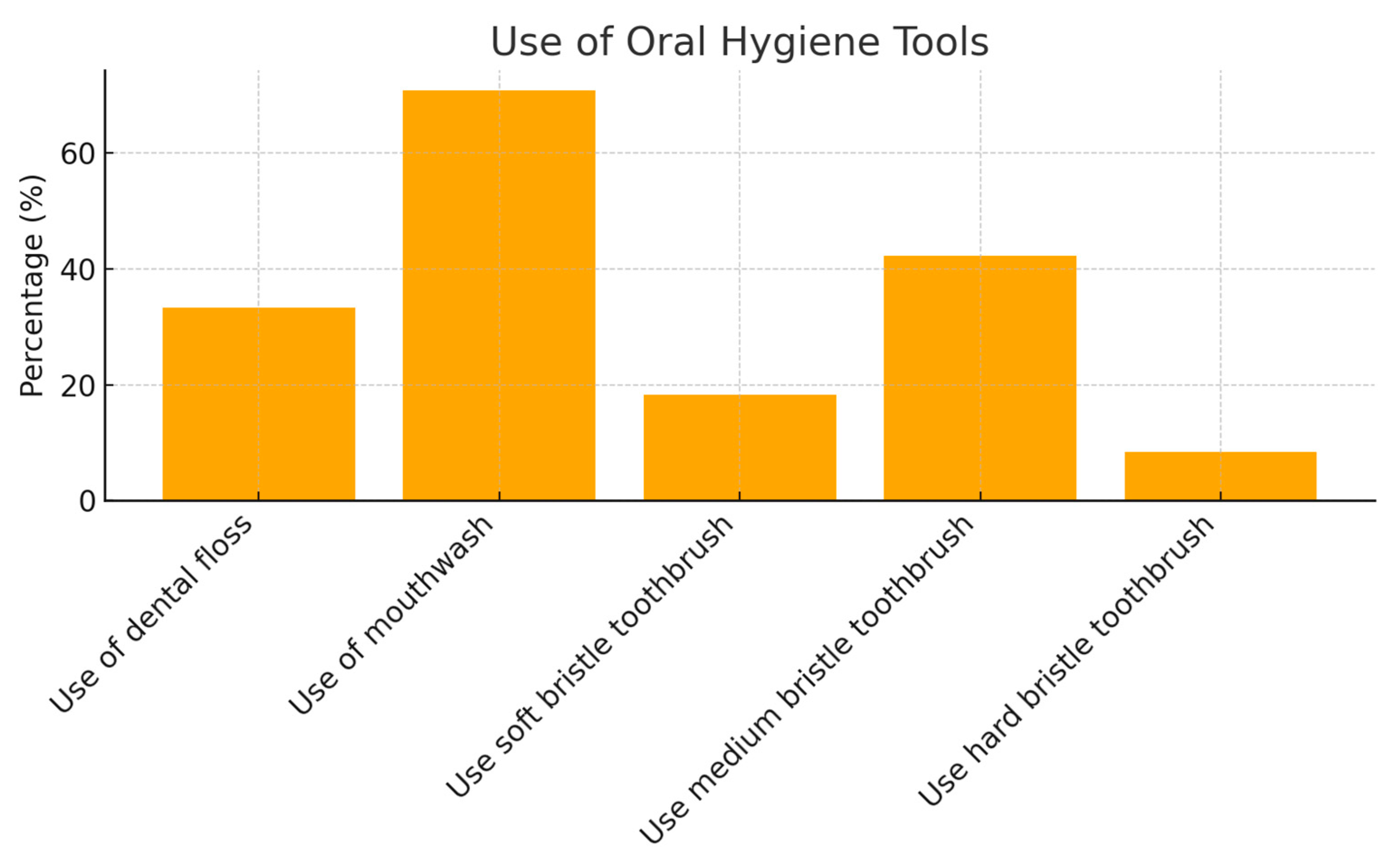
- The second section assessed oral hygiene habits before and during pregnancy, including the timing of the last dental visit, daily brushing frequency, type of toothbrush bristles used (soft, medium, or hard), and the use of dental floss and mouthwash.
- The third section explored oral pathologies, including gingival bleeding (spontaneous or induced), its onset (before or during pregnancy), and whether it worsened during pregnancy. It also addressed dental sensitivity, its onset, and progression during pregnancy. Additional questions examined vomiting episodes and oral hygiene practices afterward, as well as changes in carbohydrate consumption during the day and at night, including subsequent toothbrushing habits. Additionally, this section asked the patient to describe their toothbrushing technique to assess whether it was performed correctly.
- The fourth section focused on the following behavioral changes related to pregnancy: presence of vomiting and whether the patient brushed their teeth afterward; increased carbohydrate intake; night-time carbohydrate intake and whether the patient brushed their teeth afterward.
- Last dental visit:
- <6 months = 1 point
- 6 months = 0 points
- 18 months = −1 point;
- Number of times the patient brushes their teeth daily:
- 0 times = −1 point
- 1 time = 0 points
- 2 times = 1 point
- 3 or more times = 2 points;
- Correct/incorrect brushing technique:
- Correct = 1 point
- Incorrect = −1 point;
- Toothbrush bristle type:
- Soft = 1 point
- Medium = 0 points
- Hard = −1 point;
- Use of dental floss:
- Yes = 1 point
- No = 0 points
- Use of mouthwash:
- Yes = 1 point
- No = 0 points;
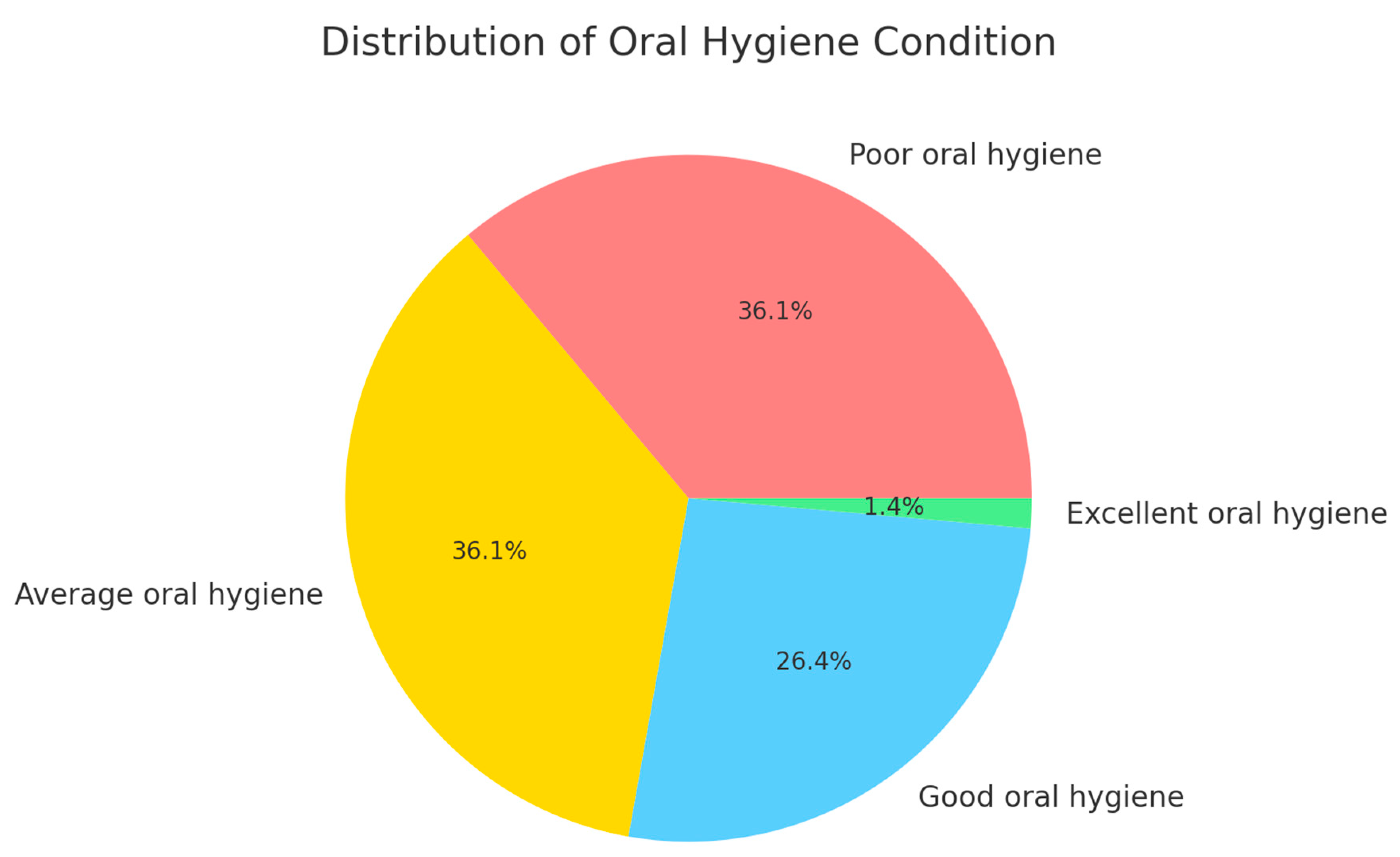
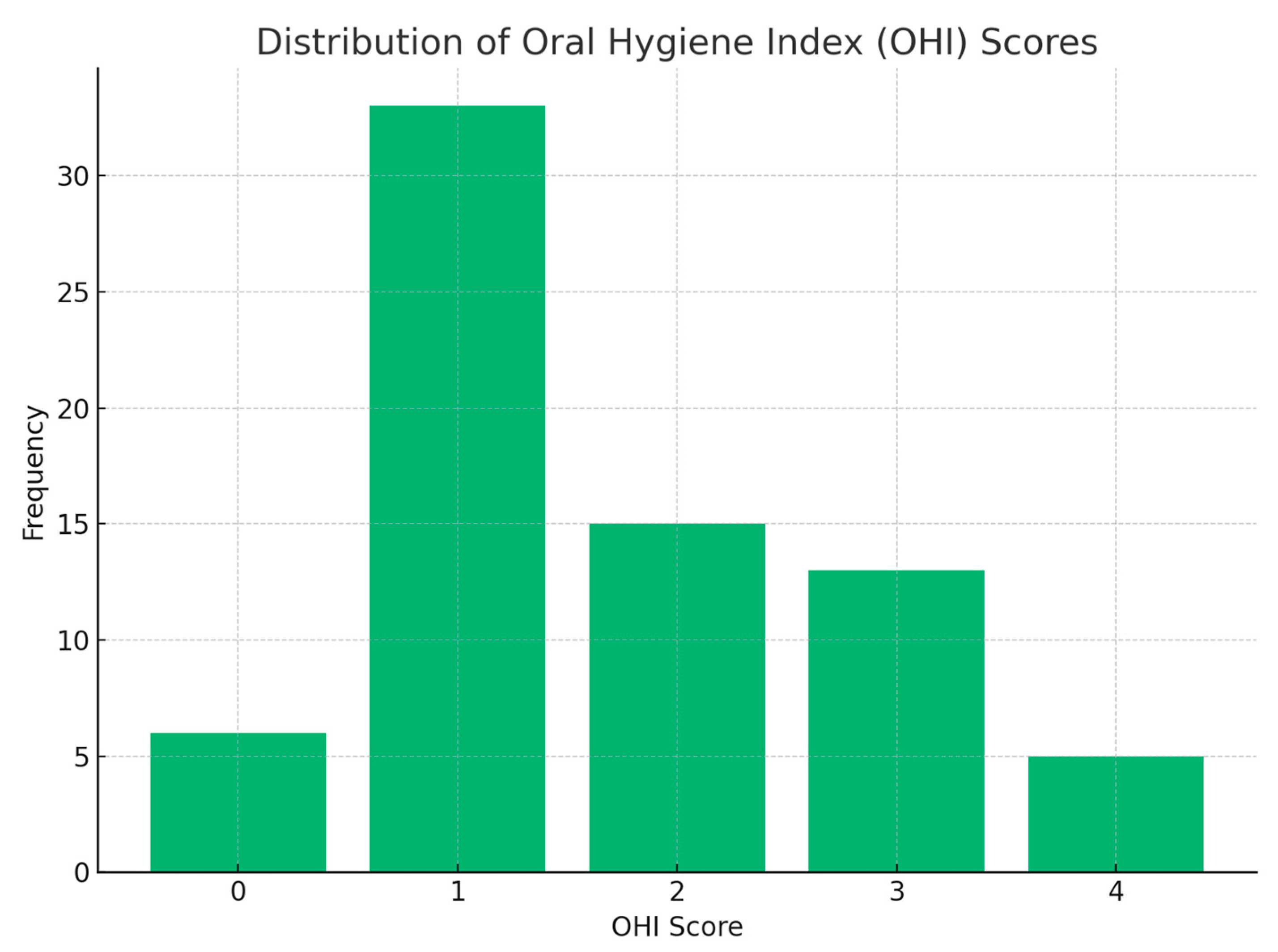
- The OHI score was then categorized as follows:
- Score ≥5: Excellent oral hygiene
- Score 3–4: Good oral hygiene
- Score 0–2: Average oral hygiene
- Score ≤−1: Poor oral hygiene.
2.3. Statistical Analysis
- Age;
- Number of pregnancies;
- Date of the last dental visit: less than 6 months, more than 6 months, more than 1 year, or never;
- Number of times the teeth are brushed daily;
- Brushing technique: correct or incorrect;
- Toothbrush bristle type: soft, medium, or hard;
- Presence of gingival bleeding: spontaneous or induced, onset before or during pregnancy, and whether it increased during pregnancy;
- Presence of dental sensitivity: onset before or during pregnancy, and whether it increased during pregnancy;
- Use of dental floss;
- Use of mouthwash;
- Presence of vomiting;
- Brushing teeth after vomiting;
- Carbohydrate intake: increased, decreased, or unchanged;
- Night-time carbohydrate intake and whether teeth are brushed afterward;
- DMFT and OHI.
3. Results
3.1. Descriptive Analysis of the Sample
3.2. Statistical Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Piccinni, M.P.; Raghupathy, R.; Saito, S.; Szekeres-Bartho, J. Cytokines, Hormones and Cellular Regulatory Mechanisms Favoring Successful Reproduction. Front. Immunol. 2021, 12, 717808. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Stanczyk, F.Z. Metabolism of endogenous and exogenous estrogens in women. J. Steroid Biochem. Mol. Biol. 2024, 242, 106539. [Google Scholar] [CrossRef] [PubMed]
- Mulac-Jericevic, B.; Mullinax, R.A.; DeMayo, F.J.; Lydon, J.P.; Conneely, O.M. Subgroup of Reproductive Functions of Progesterone Mediated by Progesterone Receptor-B Isoform. Science 2000, 289, 1751–1754. [Google Scholar] [CrossRef] [PubMed]
- Levi-Setti, P.E.; Cavagna, M.; Baggiani, A.; Zannoni, E.; Colombo, G.V.; Liprandi, V. FSH and LH together in ovarian stimulation. Eur. J. Obstet. Gynecol. Reprod. Biol. 2004, 115 (Suppl. S1), S34–S39. [Google Scholar] [CrossRef] [PubMed]
- de Ziegler, D.; Pirtea, P.; Andersen, C.Y.; Ayoubi, J.M. Role of gonadotropin-releasing hormone agonists, human chorionic gonadotropin (hCG), progesterone, and estrogen in luteal phase support after hCG triggering, and when in pregnancy hormonal support can be stopped. Fertil. Steril. 2018, 109, 749–755. [Google Scholar] [CrossRef] [PubMed]
- Fournier, T. Human chorionic gonadotropin: Different glycoforms and biological activity depending on its source of production. Ann. Endocrinol. 2016, 77, 75–81. [Google Scholar] [CrossRef]
- Dean, E. Morning sickness. Nurs. Stand. 2016, 30, 15. [Google Scholar] [CrossRef] [PubMed]
- Togoo, R.A.; Al-Almai, B.; Al-Hamdi, F.; Huaylah, S.H.; Althobati, M.; Alqarni, S. Knowledge of Pregnant Women about Pregnancy Gingivitis and Children Oral Health. Eur. J. Dent. 2019, 13, 261–270. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Hartnett, E.; Haber, J.; Krainovich-Miller, B.; Bella, A.; Vasilyeva, A.; Lange Kessler, J. Oral Health in Pregnancy. Gynecol. Neonatal Nurs. 2016, 45, 565–573. [Google Scholar] [CrossRef] [PubMed]
- Tenenbaum, A.; Azogui-Levy, S. Oral Health Knowledge, Attitudes, Practices, and Literacy of Pregnant Women: A Scoping Review. Oral Health Prev. Dent. 2023, 21, 185–198. [Google Scholar] [CrossRef] [PubMed]
- Raju, K.; Berens, L. Periodontology and pregnancy: An overview of biomedical and epidemiological evidence. Periodontology 2000 2021, 87, 132–142. [Google Scholar] [CrossRef] [PubMed]
- Holmstrup, P.; Plemons, J.; Meyle, J. Non-plaque-induced gingival diseases. J. Clin. Periodontol. 2018, 45 (Suppl. S20), S28–S43. [Google Scholar] [CrossRef] [PubMed]
- Jafarzadeh, H.; Sanatkhani, M.; Mohtasham, N. Oral pyogenic granuloma: A review. J. Oral Sci. 2006, 48, 167–175. [Google Scholar] [CrossRef] [PubMed]
- Dodds, M.W.; Johnson, D.A.; Yeh, C.K. Health benefits of saliva: A review. J. Dent. 2005, 33, 223–233. [Google Scholar] [CrossRef] [PubMed]
- Collins, M.K.; McCutcheon, C.R.; Petroff, M.G. Impact of Estrogen and Progesterone on Immune Cells and Host–Pathogen Interactions in the Lower Female Reproductive Tract. J. Immunol. 2022, 209, 1437–1449. [Google Scholar] [CrossRef]
- Al-Harthi, L.; Wright, D.J.; Anderson, D.; Cohen, M.; Matity Ahu, D.; Cohn, J.; Cu-Unvin, S.; Burns, D.; Reichelderfer, P.; Lewis, S.; et al. The impact of the ovulatory cycle on cytokine production: Evaluation of systemic, cervicovaginal, and salivary compartments. J. Interferon Cytokine Res. 2000, 20, 719–724. [Google Scholar] [CrossRef] [PubMed]
- Laine, M.A. Effect of pregnancy on periodontal and dental health. Acta Odontol. Scand. 2002, 60, 257–264. [Google Scholar] [CrossRef] [PubMed]
- Dosedělová, V.; Ďurč, P.; Dolina, J.; Konečný, Š.; Foret, F.; Kubáň, P. Analysis of bicarbonate, phosphate and other anions in saliva by capillary electrophoresis with capacitively coupled contactless conductivity detection in diagnostics of gastroesophageal reflux disease. Electrophoresis 2020, 41, 116–122. [Google Scholar] [CrossRef] [PubMed]
- Lasisi, T.J.; Ugwuadu, P.N. Pregnancy related changes in human salivary secretion and composition in a Nigerian population. Afr. J. Med. Med. Sci. 2014, 43, 347–351. [Google Scholar] [PubMed]
- Festin, M. Nausea and vomiting in early pregnancy. BMJ Clin. Evid. 2014, 2014, 1405. [Google Scholar] [PubMed] [PubMed Central]
- Fejzo, M.S.; Trovik, J.; Grooten, I.J.; Sridharan, K.; Roseboom, T.J.; Vikanes, Å.; Painter, R.C.; Mullin, P.M. Nausea and vomiting of pregnancy and hyperemesis gravidarum. Nat. Rev. Dis. Primers 2019, 5, 62. [Google Scholar] [CrossRef] [PubMed]
- Evans, R.D.; Briggs, P.F. Tooth-surface loss related to pregnancy-induced vomiting. Prim. Dent. Care 1994, 1, 24–26. [Google Scholar] [PubMed]
- Steinberg, B.J.; Hilton, I.V.; Iida, H.; Samelson, R. Oral health and dental care during pregnancy. Dent. Clin. N. Am. 2013, 57, 195–210, Erratum in Dent. Clin. N. Am. 2013, 57, 195–210. [Google Scholar] [CrossRef] [PubMed]
- Puleio, F.; Lo Giudice, G.; Molica Colella, A.; Cannarozzo, M.G.; Polosa, R.; Alibrandi, A.; Lo Giudice, R. Fibromyalgia and Orofacial Health: Administration of a Dental Disease Assessment Questionnaire. Appl. Sci. 2024, 14, 6908. [Google Scholar] [CrossRef]
- Aranza, D.; Nota, A.; Galić, T.; Kozina, S.; Tecco, S.; Poklepović Peričić, T.; Milavić, B. Development and Initial Validation of the Oral Health Activities Questionnaire. Int. J. Environ. Res. Public Health 2022, 19, 5556. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Radwan-Oczko, M.; Hirnle, L.; Szczepaniak, M.; Duś-Ilnicka, I. How much do pregnant women know about the importance of oral health in pregnancy? Questionnaire-based survey. BMC Pregnancy Childbirth 2023, 23, 348. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Silk, H.; Douglass, A.B.; Douglass, J.M.; Silk, L. Oral health during pregnancy. Am. Fam. Physician 2008, 77, 1139–1144. [Google Scholar] [PubMed]
- Kumar, S.; Priyaranjan Gautam, A.; Quazi, S.S.N.; Singh, A.; Ranjan, R. Pregnant Women’s Oral Health-Related Quality of Life and Lifestyle Factors. J. Pharm. Bioallied. Sci. 2023, 15 (Suppl. S1), S546–S549. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Gharehghani, M.A.M.; Bayani, A.; Bayat, A.H.; Hemmat, M.; Karimy, M.; Ahounbar, E.; Armoon, B.; Fakhri, Y.; Schroth, R.J. Poor oral health-related quality of life among pregnant women: A systematic review and meta-analysis. Int. J. Dent. Hyg. 2021, 19, 39–49. [Google Scholar] [CrossRef] [PubMed]
- Aimée, N.R.; van Wijk, A.J.; Maltz, M.; Varjão, M.; Mestrinho, H.D.; Carvalho, J.C. Dental caries, fluorosis, oral health determinants, and quality oflife in adolescents. Clin. Oral Investig. 2017, 21, 1811–1820. [Google Scholar] [CrossRef]
- Jamieson, L.M.; Parker, E.J.; Roberts-Thomson, K.F.; Lawrence, H.P.; Broughton, J. Self-efficacy and self-rated oral health among preg-nant aboriginal Australian women. BMC Oral Health 2014, 14, 29. [Google Scholar] [CrossRef] [PubMed]
- Vitiello, F.; Monterubbianesi, R.; Sparabombe, S.; Bourgeois, D.; Tosco, V.; Alshehri, F.A.; Carrouel, F.; Putignano, A.; Orsini, G. Use of over-the-counter mouthwashes as an additional measure in individual oral prophylaxis on adults with plaque-induced gingivitis: A double-blind, parallel, randomized controlled trial. BMC Oral Health 2024, 24, 83. [Google Scholar] [CrossRef] [PubMed]
- Shamsoddin, E. Dental floss as an adjuvant of the toothbrush helps gingival health. Evid. Based Dent. 2022, 23, 94–96. [Google Scholar] [CrossRef] [PubMed]
- Ausenda, F.; Jeong, N.; Arsenault, P.; Gyurko, R.; Finkelman, M.; Dragan, I.F.; Levi, P.A., Jr. The Effect of the Bass Intrasulcular Toothbrushing Technique on the Reduction of Gingival Inflammation: A Randomized Clinical Trial. J. Evid. Based Dent. Pract. 2019, 19, 106–114. [Google Scholar] [CrossRef] [PubMed]
- Greggianin, B.F.; Oliveira, S.C.; Haas, A.N.; Oppermann, R.V. The incidence of gingival fissures associated with toothbrushing: Crossover 28-day randomized trial. J. Clin. Periodontol. 2013, 40, 319–326. [Google Scholar] [CrossRef] [PubMed]
- Niederman, R. Pregnancy gingivitis and causal inference. Evid. Based Dent. 2013, 14, 107–108. [Google Scholar] [CrossRef] [PubMed]
- Abraham-Inpijn, L.; Polsacheva, O.V.; Raber-Durlacher, J.E. The significance of endocrine factors and microorganisms in the development of gingivitis in pregnant women. Stomatologiia 1996, 75, 15–18. [Google Scholar] [PubMed]
- Puleio, F.; Di Spirito, F.; Lo Giudice, G.; Pantaleo, G.; Rizzo, D.; Lo Giudice, R. Long-Term Chromatic Durability of White Spot Lesions through Employment of Infiltration Resin Treatment. Medicina 2023, 59, 749. [Google Scholar] [CrossRef]
- Scheutzel, P. Etiology of dental erosion-intrinsic factors. Eur. J. Oral Sci. 1996, 104 Pt 2, 178–190. [Google Scholar] [CrossRef] [PubMed]
- Ten Cate, J.M.; Imfeld, T. Dental erosion, summary. Eur. J. Oral Sci. 1996, 104 Pt 2, 241–244. [Google Scholar] [CrossRef] [PubMed]
- Rangé, H.; Colon, P.; Godart, N.; Kapila, Y.; Bouchard, P. Eating disorders through the periodontal lens. Periodontology 2000 2021, 87, 17–31. [Google Scholar] [CrossRef] [PubMed] [PubMed Central]
- Lussi, A.; Buzalaf MA, R.; Duangthip, D.; Anttonen, V.; Ganss, C.; João-Souza, S.H.; Baumann, T.; Carvalho, T.S. The use of fluoride for the prevention of dental erosion and erosive tooth wear in children and adolescents. Eur. Arch. Paediatr. Dent. 2019, 20, 517–527. [Google Scholar] [CrossRef] [PubMed]
- Burkhart, N.; Roberts, M.; Alexander, M.; Dodds, A. Communicating effectively with patients suspected of having bulimia nervosa. J. Am. Dent. Assoc. 2005, 136, 1130–1137. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, J.D.; Smith, B.M.; Spresser, C.; Harkins, P.; Zolton, L.; Williams, K. The relationship of night eating to oral health and obesity in community dental clinic patients. Gen. Dent. 2010, 58, e134–e139. [Google Scholar] [PubMed]
- Foglio-Bonda, P.L.; Rocchetti, V.; Nardella, A.; Fantinato, M.; Sandhu, K.K.; Foglio-Bonda, A. Salivary pH and flow rate in menopausal women. Eur. Rev. Med. Pharmacol. Sci. 2019, 23, 918–922. [Google Scholar]
- Villa, A.; Abati, S.; Pileri, P.; Calabrese, S.; Capobianco, G.; Strohmenger, L.; Ottolenghi, L.; Cetin, I.; Campus, G.G. Oral health and oral diseases in pregnancy: A multicentre survey of Italian postpartum women. Aust. Dent. J. 2013, 58, 224–229. [Google Scholar] [CrossRef]
- Wagle, M.; D’Antonio, F.; Reierth, E.; Basnet, P.; Trovik, T.A.; Orsini, G.; Manzoli, L.; Acharya, G. Dental caries and preterm birth: A systematic review and meta-analysis. BMJ Open 2018, 8, e018556. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lo Giudice, R.; Martinelli, C.; Alibrandi, A.; Mondo, A.; Venezia, R.; Cannarozzo, M.G.; Puleio, F.; Pollicino, R.; Lo Giudice, G.; Laganà, A.S. Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. J. Clin. Med. 2024, 13, 7315. https://doi.org/10.3390/jcm13237315
Lo Giudice R, Martinelli C, Alibrandi A, Mondo A, Venezia R, Cannarozzo MG, Puleio F, Pollicino R, Lo Giudice G, Laganà AS. Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. Journal of Clinical Medicine. 2024; 13(23):7315. https://doi.org/10.3390/jcm13237315
Chicago/Turabian StyleLo Giudice, Roberto, Canio Martinelli, Angela Alibrandi, Alessandro Mondo, Renato Venezia, Maria Grazia Cannarozzo, Francesco Puleio, Raffaella Pollicino, Giuseppe Lo Giudice, and Antonio Simone Laganà. 2024. "Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women" Journal of Clinical Medicine 13, no. 23: 7315. https://doi.org/10.3390/jcm13237315
APA StyleLo Giudice, R., Martinelli, C., Alibrandi, A., Mondo, A., Venezia, R., Cannarozzo, M. G., Puleio, F., Pollicino, R., Lo Giudice, G., & Laganà, A. S. (2024). Multicenter Cross-Sectional Study of Oral Health and Hygiene Practices Among Pregnant Women. Journal of Clinical Medicine, 13(23), 7315. https://doi.org/10.3390/jcm13237315