
Characterization and Management of Stable Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation
 , , ,
, , ,  , , ,
, , ,  , , , , , , , , ,
, , , , , , , , ,  ,
,  , , , , , and add
Show full author list
, , , , , and add
Show full author list
Abstract
1. Introduction
2. Materials and Methods
3. Results
3.1. Baseline Characteristics
3.2. TAVI Procedure Details
3.3. Coronary Artery Disease Details
3.4. Percutaneous Coronary Intervention Details
3.5. Clinical Outcomes
3.6. Predictors and Outcomes of Percutaneous Coronary Intervention
4. Discussion
- (1)
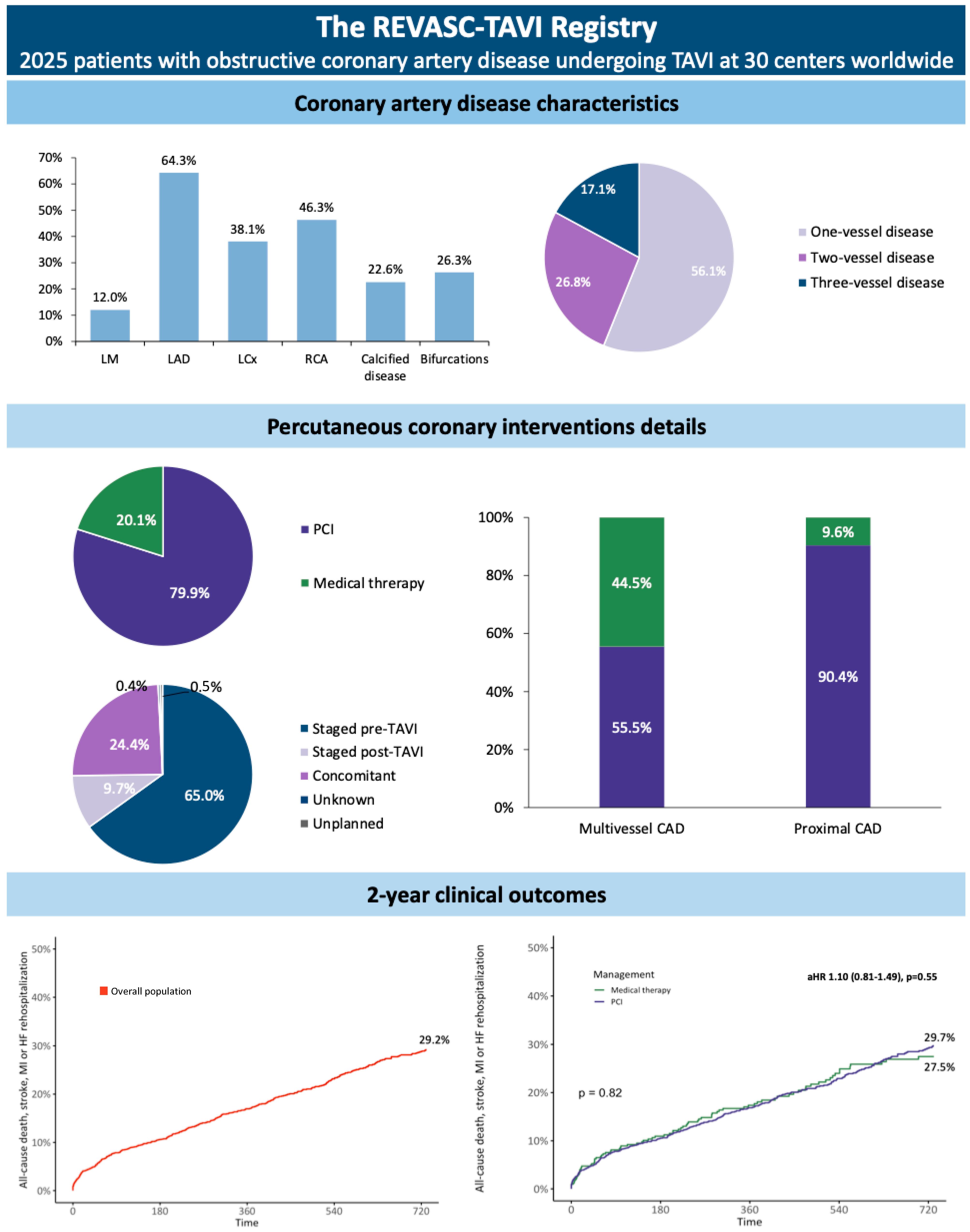
- Most of patients had one-vessel CAD, with proximal coronary segments involved in about 60% of cases.
- (2)
- About 80% of patients underwent PCI, most frequently performed before the TAVI procedure, with disease in proximal coronary segments being treated in about 90% of cases.
- (3)
- Angina at baseline, lesions involving main tracts of coronary arteries, or coronary bifurcations led operators to perform PCI while patients with an involvement of distal or secondary vessels (i.e., diagonal or posterolateral branches) had a lower probability of receiving PCI.
- (4)
- Physiologic assessment of coronary lesions was quite uncommon.
- (5)
- The balloon-expandable SAPIEN 3 was the most used TAVI platform in patients treated with PCI.
- (6)
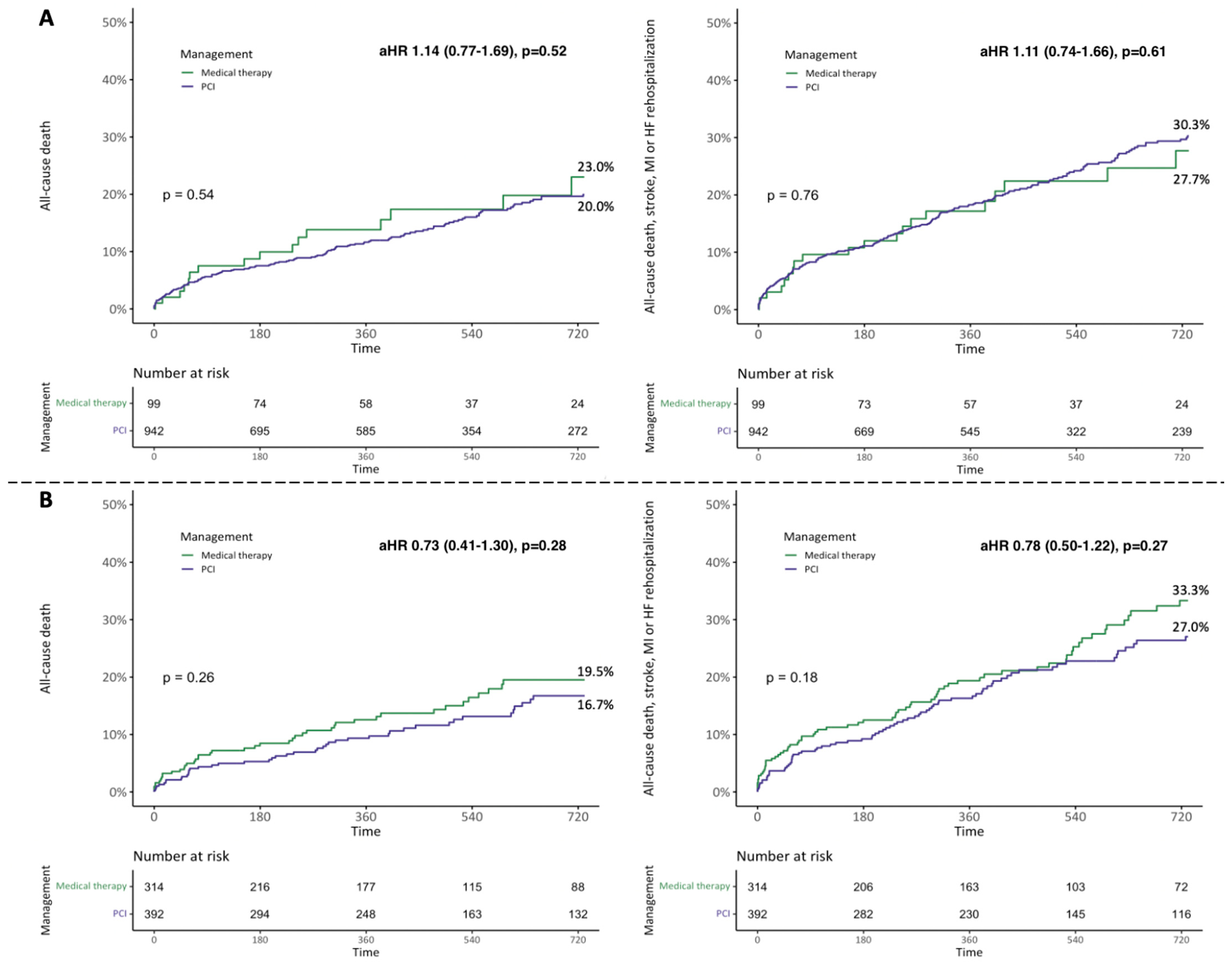
- Patients receiving PCI had similar mid-term clinical outcomes compared to those treated conservatively.
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Faroux, L.; Guimaraes, L.; Wintzer-Wehekind, J.; Junquera, L.; Ferreira-Neto, A.N.; del Val, D.; Muntané-Carol, G.; Mohammadi, S.; Paradis, J.-M.; Rodés-Cabau, J. Coronary Artery Disease and Transcatheter Aortic Valve Replacement. J. Am. Coll. Cardiol. 2019, 74, 362–372. [Google Scholar] [CrossRef] [PubMed]
- Vahanian, A.; Beyersdorf, F.; Praz, F.; Milojevic, M.; Baldus, S.; Bauersachs, J.; Capodanno, D.; Conradi, L.; De Bonis, M.; De Paulis, R.; et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur. Heart J. 2021, 43, 561–632. [Google Scholar] [CrossRef] [PubMed]
- Otto, C.M.; Otto, C.M.; Nishimura, R.A.; Nishimura, R.A.; Bonow, R.O.; Bonow, R.O.; Carabello, B.A.; Carabello, B.A.; Erwin, J.P.; Erwin, J.P.; et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation 2021, 143, e35–e71. [Google Scholar] [CrossRef] [PubMed]
- Patterson, T.; Clayton, T.; Dodd, M.; Khawaja, Z.; Morice, M.C.; Wilson, K.; Kim, W.-K.; Meneveau, N.; Hambrecht, R.; Byrne, J.; et al. ACTIVATION (PercutAneous Coronary inTervention prIor to transcatheter aortic VAlve implantaTION). JACC Cardiovasc. Interv. 2021, 14, 1965–1974. [Google Scholar] [CrossRef] [PubMed]
- Kappetein, A.P.; Head, S.J.; Généreux, P.; Piazza, N.; Van Mieghem, N.M.; Blackstone, E.H.; Brott, T.G.; Cohen, D.J.; Cutlip, D.E.; van Es, G.A.; et al. Updated standardized endpoint definitions for transcatheter aortic valve implantation: The Valve Academic Research Consortium-2 consensus document. J. Am. Coll. Cardiol. 2012, 60, 1438–1454. [Google Scholar] [CrossRef] [PubMed]
- De Silva, K.; Morton, G.; Sicard, P.; Chong, E.; Indermuehle, A.; Clapp, B.; Thomas, M.; Redwood, S.; Perera, D. Prognostic Utility of BCIS Myocardial Jeopardy Score for Classification of Coronary Disease Burden and Completeness of Revascularization. Am. J. Cardiol. 2013, 111, 172–177. [Google Scholar] [CrossRef] [PubMed]
- Lateef, N.; Khan, M.S.; Deo, S.V.; Yamani, N.; Riaz, H.; Virk, H.U.H.; Khan, S.U.; Hedrick, D.P.; Kanaan, A.; Reed, G.W.; et al. Meta-Analysis Comparing Outcomes in Patients Undergoing Transcatheter Aortic Valve Implantation with Versus Without Percutaneous Coronary Intervention. Am. J. Cardiol. 2019, 124, 1757–1764. [Google Scholar] [CrossRef] [PubMed]
- Masson, J.; Lee, M.; Boone, R.H.; Al Ali, A.; Al Bugami, S.; Hamburger, J.; Mancini, G.J.; Ye, J.; Cheung, A.; Humphries, K.H.; et al. Impact of coronary artery disease on outcomes after transcatheter aortic valve implantation. Catheter. Cardiovasc. Interv. 2010, 76, 165–173. [Google Scholar] [CrossRef] [PubMed]
- D’Ascenzo, F.; Conrotto, F.; Giordana, F.; Moretti, C.; D’Amico, M.; Salizzoni, S.; Omedè, P.; La Torre, M.; Thomas, M.; Khawaja, Z.; et al. Mid-term prognostic value of coronary artery disease in patients undergoing transcatheter aortic valve implantation: A meta-analysis of adjusted observational results. Int. J. Cardiol. 2013, 168, 2528–2532. [Google Scholar] [CrossRef] [PubMed]
- Ussia, G.P.; Barbanti, M.; Colombo, A.; Tarantini, G.; Petronio, A.S.; Ettori, F.; Ramondo, A.; Santoro, G.; Klugmann, S.; Bedogni, F.; et al. Impact of coronary artery disease in elderly patients undergoing transcatheter aortic valve implantation: Insight from the Italian CoreValve Registry. Int. J. Cardiol. 2012, 167, 943–950. [Google Scholar] [CrossRef] [PubMed]
- Van Mieghem, N.M.; van der Boon, R.M.; Faqiri, E.; Diletti, R.; Schultz, C.; van Geuns, R.-J.; Serruys, P.W.; Kappetein, A.-P.; van Domburg, R.T.; de Jaegere, P.P. Complete Revascularization Is Not a Prerequisite for Success in Current Transcatheter Aortic Valve Implantation Practice. JACC Cardiovasc. Interv. 2013, 6, 867–875. [Google Scholar] [CrossRef] [PubMed]
- Neumann, F.-J.; Sousa-Uva, M.; Ahlsson, A.; Alfonso, F.; Banning, A.P.; Benedetto, U.; Byrne, R.A.; Collet, J.-P.; Falk, V.; Head, S.J.; et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. EuroIntervention 2019, 14, 1435–1534. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Tang, G.; Fovino, L.N.; Blackman, D.; Van Mieghem, N.M.; Kim, W.-K.; Karam, N.; Carrilho-Ferreira, P.; Fournier, S.; Pręgowski, J.; et al. Management of coronary artery disease in patients undergoing transcatheter aortic valve implantation. A clinical consensus statement from the European Association of Percutaneous Cardiovascular Interventions in collaboration with the ESC Working Group on Cardiovascular Surgery. EuroIntervention 2023, 19, 37–52. [Google Scholar] [CrossRef] [PubMed]
- Barbanti, M.; Costa, G.; Picci, A.; Criscione, E.; Reddavid, C.; Valvo, R.; Todaro, D.; Deste, W.; Condorelli, A.; Scalia, M.; et al. Coronary Cannulation After Transcatheter Aortic Valve Replacement. JACC Cardiovasc. Interv. 2020, 13, 2542–2555. [Google Scholar] [CrossRef] [PubMed]
- Valvo, R.; Costa, G.; Tamburino, C.; Barbanti, M. Coronary artery cannulation after transcatheter aortic valve implantation. EuroIntervention 2021, 17, 835–847. [Google Scholar] [CrossRef] [PubMed]
- Costa, G.; Sammartino, S.; Strazzieri, O.; Motta, S.; Frittitta, V.; Dipietro, E.; Comis, A.; Calì, M.; Garretto, V.; Inserra, C.; et al. Coronary Cannulation Following TAVR Using Self-Expanding Devices With Commissural Alignment: The RE-ACCESS 2 Study. JACC Cardiovasc. Interv. 2024, 17, 727–737. [Google Scholar] [CrossRef] [PubMed]
- Van Belle, E.; Vincent, F.; Labreuche, J.; Auffret, V.; Debry, N.; Lefèvre, T.; Eltchaninoff, H.; Manigold, T.; Gilard, M.; Verhoye, J.-P.; et al. Balloon-Expandable Versus Self-Expanding Transcatheter Aortic Valve Replacement A Propensity-Matched Comparison From the FRANCE-TAVI Registry. Circulation 2020, 141, 243–259. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Overall (n = 2025) | No PCI (n = 408) | PCI (n = 1617) | p-Value | |
|---|---|---|---|---|
| Sex, male n (%) | 1188 (58.7) | 250 (61.3) | 938 (58.0) | 0.40 |
| Age, median [IQR] | 82.4 [78.0, 85.8] | 83.0 [79.0, 86.0] | 82.2 [78.0, 85.3] | 0.12 |
| Body mass index, median [IQR] | 26.5 [23.8, 29.4] | 26.7 [23.9, 29.8] | 26.5 [23.7, 29.1] | 0.29 |
| Hypertension, n (%) | 1719 (84.9) | 341 (83.6) | 1378 (85.2) | 0.51 |
| Diabetes, n (%) | 648 (32.0) | 132 (32.4) | 516 (31.9) | 0.26 |
| Peripheric artery disease, n (%) | 338 (16.7) | 68 (16.7) | 270 (16.7) | 0.12 |
| COPD, n (%) | 319 (15.8) | 67 (16.4) | 252 (15.6) | 0.06 |
| eGFR, ml/min median [IQR] | 55.1 [43.0, 64.5] | 53.5 [39.6, 67.1] | 55.1 [44.0, 64.0] | 0.04 |
| Prior CABG, n (%) | 195 (9.6) | 61 (15.0) | 134 (8.3) | <0.01 |
| Prior PCI, n (%) | 963 (47.6) | 107 (26.2) | 856 (52.9) | <0.01 |
| Prior myocardial infarction, n (%) | 405 (20.0) | 93 (22.8) | 312 (19.3) | 0.04 |
| Prior stroke, n (%) | 169 (8.3) | 22 (5.4) | 147 (9.1) | <0.01 |
| Prior pacemaker, n (%) | 178 (8.8) | 45 (11.0) | 133 (8.2) | 0.01 |
| Prior SAVR, n (%) | 39 (1.9) | 7 (1.7) | 32 (2.0) | <0.01 |
| Bicuspid aortic valve, n (%) | 80 (4.0) | 11 (2.7) | 69 (4.3) | <0.01 |
| CCS class > 1, n (%) | 444 (28.1) | 73 (19.2) | 371 (30.9) | <0.01 |
| NYHA class > 2, n (%) | 1274 (63.1) | 262 (64.2) | 1012 (62.8) | 0.61 |
| Atrial fibrillation, n (%) | 541 (26.7) | 102 (25.0) | 439 (27.1) | 0.04 |
| STS mortality score, % median [IQR] | 5.0 [3.1, 5.1] | 4.3 [2.8, 5.4] | 5.0 [3.2, 5.1] | 0.01 |
| LVEF, % median [IQR] | 55.0 [45.0, 61.0] | 55.0 [43.8, 60.0] | 56.0 [47.0, 62.0] | <0.01 |
| LVEF < 40%, n (%) | 300 (14.8) | 73 (17.9) | 227 (14.0) | 0.05 |
| Aortic mean gradient, mmHg, median [IQR] | 44.0 [36.0, 51.0] | 44.4 [38.0, 51.0] | 44.0 [36.0, 51.0] | 0.22 |
| Aortic valve area, cm2 median [IQR] | 0.7 [0.6, 0.8] | 0.7 [0.6, 0.8] | 0.7 [0.6, 0.8] | 0.23 |
| Dual antiplatelet therapy, n (%) | 745 (36.8) | 23 (5.6) | 722 (44.7) | <0.01 |
| Dual anti-thrombotic therapy, n (%) | 145 (7.2) | 23 (5.6) | 122 (7.5) | <0.01 |
| Triple anti-thrombotic therapy, n (%) | 107 (5.3) | 0 (0.0) | 107 (6.6) | <0.01 |
| Overall (n = 2025) | No PCI (n = 408) | PCI (n = 1617) | p-Value | |
|---|---|---|---|---|
| Diseased vessels, n (%) | 0.81 | |||
| One | 1137 (56.1) | 227 (55.6) | 910 (56.3) | |
| Two | 542 (26.8) | 107 (26.2) | 435 (26.9) | |
| Three or more | 346 (17.1) | 74 (18.1) | 272 (16.8) | |
| Right dominance, n (%) | 1634 (83.7) | 328 (81.8) | 1306 (84.2) | 0.26 |
| Multivessel CAD, n (%) | 403 (22.6) | 181 (44.4) | 707 (43.7) | 0.82 |
| Proximal CAD, n (%) | 432 (26.3) | 223 (54.7) | 1043 (64.5) | <0.01 |
| Calcific disease, n (%) | 888 (43.9) | 73 (19.8) | 330 (23.3) | 0.18 |
| Bifurcation involved, n (%) | 1266 (62.5) | 44 (12.0) | 388 (30.4) | <0.01 |
| Syntax score, median [IQR] | 8 [5, 13] | 7 [4, 11] | 8 [5, 14] | <0.01 |
| BCIS jeopardy score, median [IQR] | 4 [2, 6] | 4 [2, 6] | 4 [2, 8] | <0.01 |
| Residual BCIS jeopardy score, median [IQR] | 0 [0, 2] | 4 [2, 6] | 0 [0, 0] | <0.01 |
| Coronary segments involved | ||||
| LM, n (%) | 242 (12.0) | 21 (5.1) | 221 (13.7) | <0.01 |
| LAD, n (%) | 1302 (64.3) | 265 (65.0) | 1037 (64.1) | 0.77 |
| Proximal LAD, n (%) | 615 (30.4) | 103 (25.2) | 512 (31.7) | 0.01 |
| Mid LAD, n (%) | 768 (37.9) | 133 (32.6) | 635 (39.3) | 0.01 |
| Distal LAD, n (%) | 146 (7.2) | 30 (7.4) | 116 (7.2) | 0.92 |
| Diagonal, n (%) | 298 (14.7) | 87 (21.3) | 211 (13.0) | <0.01 |
| LCx, n (%) | 771 (38.1) | 184 (45.1) | 587 (36.3) | 0.00 |
| Proximal LCx, n (%) | 357 (17.6) | 84 (20.6) | 273 (16.9) | 0.08 |
| Mid LCx, n (%) | 232 (11.5) | 45 (11.0) | 187 (11.6) | 0.80 |
| Distal LCx/PDA, n (%) | 96 (4.7) | 25 (6.1) | 71 (4.4) | 0.15 |
| Obtuse marginal, n (%) | 288 (14.2) | 78 (19.1) | 210 (13.0) | 0.00 |
| RCA, n (%) | 937 (46.3) | 188 (46.1) | 749 (46.3) | 0.96 |
| Proximal RCA, n (%) | 551 (27.2) | 90 (22.1) | 461 (28.5) | 0.01 |
| Mid RCA, n (%) | 404 (20.0) | 82 (20.1) | 322 (19.9) | 0.95 |
| Distal RCA/PL/PDA, n (%) | 254 (12.5) | 71 (17.4) | 183 (11.3) | 0.00 |
| Venous/arterial graft, n (%) | 76 (3.8) | 17 (4.2) | 59 (3.6) | 0.66 |
| Overall Lesions (n = 2014) | |
|---|---|
| Target vessel stenosis, n (%) | |
| NA | 9 (0.5) |
| > 70% | 1587 (81.3) |
| > 90% | 306 (15.7) |
| CTO | 49 (2.5) |
| PCI access (%) | |
| Right radial | 938 (48.8) |
| Left radial | 75 (3.9) |
| Femoral | 910 (47.3) |
| NA | 1 (0.1) |
| iFR/FFR use, n (%) | 159 (9.5) |
| IVUS/OCT use, n (%) | 117 (7.0) |
| Hemodynamic support, n (%) | 22 (1.1) |
| Atherectomy, n (%) | 87 (4.5) |
| LM, n (%) | 229 (11.4) |
| LAD, n (%) | 912 (45.3) |
| Proximal LAD, n (%) | 465 (23.1) |
| Mid LAD, n (%) | 560 (27.8) |
| Distal LAD, n (%) | 77 (3.8) |
| Diagonal, n (%) | 107 (5.3) |
| LCx, n (%) | 342 (17.0) |
| Proximal LCx, n (%) | 198 (9.8) |
| Mid LCx, n (%) | 133 (6.6) |
| Distal LCx, n (%) | 48 (2.4) |
| Obtuse marginal, n (%) | 127 (6.3) |
| RCA, n (%) | 585 (29.0) |
| Proximal RCA, n (%) | 358 (17.8) |
| Mid RCA, n (%) | 246 (12.2) |
| Distal RCA/PL/PDA, n (%) | 123 (6.1) |
| Venous arterial graft, n (%) | 41 (2.0) |
| Procedural success, n (%) | 1924 (97.4) |
| Crossing difficulty, n (%) | 49 (2.6) |
| Baseline Characteristics | OR (95% CI) | p-Value |
|---|---|---|
| Female | 1.17 (0.91–1.50) | 0.22 |
| Age, year | 0.99 (0.97–1.01) | 0.34 |
| Diabetes | 0.86 (0.66–1.11) | 0.24 |
| eGFR, mL/min | 1.00 (1.00–1.01) | 0.43 |
| Prior CABG | 0.40 (0.28–0.59) | <0.01 |
| Prior PCI | 2.53 (1.95–3.30) | <0.01 |
| CCS > 1 | 1.86 (1.39–2.50) | <0.01 |
| NYHA > 2 | 0.96 (0.74–1.24) | 0.75 |
| Atrial fibrillation | 1.06 (0.80–1.40) | 0.70 |
| LVEF < 40% | 0.76 (0.55–1.05) | 0.09 |
| CAD Characteristics | OR (95% CI) | p-Value |
|---|---|---|
| LM | 2.95 (1.73–5.31) | <0.01 |
| Proximal LAD | 1.30 (0.97–1.75) | 0.08 |
| Mid LAD | 1.55 (1.17–2.07) | <0.01 |
| Distal LAD | 1.08 (0.69–1.76) | 0.74 |
| Diagonal | 0.45 (0.32–0.64) | <0.01 |
| Proximal LCx | 0.61 (0.43–0.87) | 0.01 |
| Mid LCx | 1.27 (0.84–1.97) | 0.31 |
| Distal LCx/PDA | 0.75 (0.43–1.32) | 0.30 |
| Obtuse marginal | 0.73 (0.51–1.05) | 0.09 |
| Proximal RCA | 1.55 (1.14–2.12) | 0.01 |
| Mid RCA | 1.30 (0.94–1.81) | 0.11 |
| Distal RCA/PL/PDA | 0.66 (0.46–0.95) | 0.03 |
| Calcific disease | 1.12 (0.82–1.54) | 0.47 |
| Bifurcation | 3.41 (2.36–5.02) | <0.01 |
| Multivessel CAD | 0.90 (0.63–1.30) | 0.59 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Sammartino, S.; Laterra, G.; Pilgrim, T.; Amat Santos, I.J.; De Backer, O.; Kim, W.-K.; Ribeiro, H.B.; Saia, F.; Bunc, M.; Tchetche, D.; et al. Characterization and Management of Stable Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation. J. Clin. Med. 2024, 13, 3497. https://doi.org/10.3390/jcm13123497
Sammartino S, Laterra G, Pilgrim T, Amat Santos IJ, De Backer O, Kim W-K, Ribeiro HB, Saia F, Bunc M, Tchetche D, et al. Characterization and Management of Stable Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine. 2024; 13(12):3497. https://doi.org/10.3390/jcm13123497
Chicago/Turabian StyleSammartino, Sofia, Giulia Laterra, Thomas Pilgrim, Ignacio J. Amat Santos, Ole De Backer, Won-Keun Kim, Henrique Barbosa Ribeiro, Francesco Saia, Matjaz Bunc, Didier Tchetche, and et al. 2024. "Characterization and Management of Stable Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation" Journal of Clinical Medicine 13, no. 12: 3497. https://doi.org/10.3390/jcm13123497
APA StyleSammartino, S., Laterra, G., Pilgrim, T., Amat Santos, I. J., De Backer, O., Kim, W.-K., Ribeiro, H. B., Saia, F., Bunc, M., Tchetche, D., Garot, P., Ribichini, F. L., Mylotte, D., Burzotta, F., Watanabe, Y., Bedogni, F., Tesorio, T., Rheude, T., Sardella, G., ... Costa, G. (2024). Characterization and Management of Stable Coronary Artery Disease in Patients Undergoing Transcatheter Aortic Valve Implantation. Journal of Clinical Medicine, 13(12), 3497. https://doi.org/10.3390/jcm13123497