Lateral Humeral Condyle Fracture in Childhood: Results of a New Surgical Technique

 , ,
, ,  and
and
Abstract
1. Introduction
2. Materials and Methods
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Ganeshalingam, R.; Donnan, A.; Evans, O.; Hoq, M.; Camp, M.; Donnan, L. Lateral condylar fractures of the humerus in children: Does the type of fixation matter? Bone Jt. J. 2018, 100, 387–395. [Google Scholar] [CrossRef]
- Liu, T.J.; Wang, E.B.; Dai, Q.; Zhang, L.J.; Li, Q.W.; Zhao, Q. Open reduction and internal fixation for the treatment of fractures of the lateral humeral condyle with an early delayed presentation in children: A radiological and clinical prospective study. Bone Jt. J. 2016, 98, 244–248. [Google Scholar] [CrossRef]
- Franks, D.; Shatrov, J.; Symes, M.; Little, D.G.; Cheng, T.L. Cannulated screw versus Kirschner-wire fixation for Milch II lateral condyle fractures in a paediatric sawbone model: A biomechanical comparison. J. Child. Orthop. 2018, 12, 29–35. [Google Scholar] [CrossRef]
- Abzug, J.M.; Dua, K.; Kozin, S.H.; Herman, M.J. Current Concepts in the Treatment of Lateral Condyle Fractures in Children. J. Am. Acad. Orthop. Surg. 2020, 28, e9–e19. [Google Scholar] [CrossRef]
- Shaerf, D.A.; Vanhegan, I.S.; Dattani, R. Diagnosis, management and complications of distal humerus lateral condyle fractures in children. Shoulder Elb. 2018, 10, 114–120. [Google Scholar] [CrossRef]
- Tan, S.H.S.; Dartnell, J.; Lim, A.K.S.; Hui, J.H. Paediatric lateral condyle fractures: A systematic review. Arch. Orthop. Trauma Surg. 2018, 138, 809–817. [Google Scholar] [CrossRef]
- Flynn, J.C. Nonunion of slightly displaced fractures of the lateral humeral condyle in children: An update. J. Pediatr. Orthop. 1989, 9, 691–696. [Google Scholar] [CrossRef]
- Akar, M.S.; Ulus, S.A.; Durgut, F.; Dönmez, S. Complications and difficulties due to bonesetter in the treatment of pediatric distal humerus fractures. J. Clin. Trials Exp. Investig. 2023, 2, 38–44. [Google Scholar]
- Milch, H. Fractures and fracture dislocations of the humeral condyles. J. Trauma 1964, 4, 592–607. [Google Scholar] [CrossRef] [PubMed]
- Jakob, R.; Fowles, J.V.; Rang, M.; Kassab, M.T. Observations concerning fractures of the lateral humeral condyle in children. J. Bone Jt. Surg. Br. 1975, 57, 430–436. [Google Scholar] [CrossRef]
- Margalit, A.; Stein, B.E.; Hassanzadeh, H.; Ain, M.C.; Sponseller, P.D. Percutaneous Screw Fixation of Lateral Condylar Humeral Fractures. JBJS Essent. Surg. Tech. 2016, 6, e15. [Google Scholar] [CrossRef] [PubMed]
- Justus, C.; Haruno, L.S.; Riordan, M.K.; Wilsford, L.; Smith, T.; Antekeier, S.; McKay, S.D. Closed and Open Reduction of Displaced Pediatric Lateral Condyle Humeral Fractures, a Study of Short-Term Complications and Postoperative Protocols. Iowa Orthop. J. 2017, 37, 163–169. [Google Scholar] [PubMed]
- Gilbert, S.R.; MacLennan, P.A.; Schlitz, R.S.; Estes, A.R. Screw versus pin fixation with open reduction of pediatric lateral condyle fractures. J. Pediatr. Orthop. B 2016, 25, 148–152. [Google Scholar] [CrossRef]
- Stein, B.E.; Ramji, A.F.; Hassanzadeh, H.; Wohlgemut, J.M.; Ain, M.C.; Sponseller, P.D. Cannulated Lag Screw Fixation of Displaced Lateral Humeral Condyle Fractures Is Associated with Lower Rates of Open Reduction and Infection than Pin Fixation. J. Pediatr. Orthop. 2017, 37, 7–13. [Google Scholar] [CrossRef] [PubMed]
- Wirmer, J.; Kruppa, C.; Fitze, G. Operative treatment of lateral humeral condyle fractures in children. Eur. J. Pediatr. Surg. 2012, 22, 289–294. [Google Scholar] [CrossRef]
- Sharma, H.; Chirputkar, K.; Duncan, R.D.D. Management of lateral humeral condylar mass fractures in children. Curr. Orthop. 2007, 21, 145–149. [Google Scholar] [CrossRef]
- Singh, A.; Kushwaha, N.S.; Kumar, S.; Kumar, R.; Mohan, R.; Roy, S.; Singh, U.; Abbas, Z. A Comparative Study of the Modified Baumann’s Angle Between the Dominant and Non-Dominant Sides in a North Indian Pediatric Population. Cureus 2023, 15, e47687. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.H.; Seo, S.W.; Kim, K.M.; Shim, J.S. Clinical and radiographic results of lateral condylar fracture of distal humerus in children. J. Pediatr. Orthop. 2010, 30, 425–429. [Google Scholar] [CrossRef] [PubMed]
- Stevenson, R.A.; Perry, D.C. Paediatric lateral condyle fractures of the distal humerus. Orthop. Trauma 2018, 32, 352–359. [Google Scholar] [CrossRef]
- Song, K.S.; Kang, C.H.; Min, B.W.; Bae, K.C.; Cho, C.H.; Lee, J.H. Closed reduction and internal fixation of displaced unstable lateral condylar fractures of the humerus in children. J. Bone Jt. Surg. Am. 2008, 90, 2673–2681. [Google Scholar] [CrossRef]
- Launay, F.; Leet, A.I.; Jacopin, S.; Jouve, J.L.; Bollini, G.; Sponseller, P.D. Lateral humeral condyle fractures in children: A comparison of two approaches to treatment. J. Pediatr. Orthop. 2004, 24, 385–391. [Google Scholar] [CrossRef]
- Li, W.C.; Xu, R.J. Comparison of Kirschner wires and AO cannulated screw internal fixation for displaced lateral humeral condyle fracture in children. Int. Orthop. 2012, 36, 1261–1266. [Google Scholar] [CrossRef]
- Wormald, J.C.R.; Park, C.Y.; Eastwood, D.M. A systematic review and meta-analysis of adverse outcomes following non-buried versus buried Kirschner wires for paediatric lateral condyle elbow fractures. J. Child. Orthop. 2017, 11, 465–471. [Google Scholar] [CrossRef]
- Raghavan, R.; Jones, A.; Dwyer, A.J. Should Kirschner wires for fixation of lateral humeral condyle fractures in children be buried or left exposed? A systematic review. Orthop. Traumatol. Surg. Res. 2019, 105, 739–745. [Google Scholar] [CrossRef]
- Pennock, A.T.; Salgueiro, L.; Upasani, V.V.; Bastrom, T.P.; Newton, P.O.; Yaszay, B. Closed Reduction and Percutaneous Pinning Versus Open Reduction and Internal Fixation for Type II Lateral Condyle Humerus Fractures in Children Displaced >2 mm. J. Pediatr. Orthop. 2016, 36, 780–786. [Google Scholar] [CrossRef]
- Andrey, V.; Tercier, S.; Vauclair, F.; Bregou-Bourgeois, A.; Lutz, N.; Zambelli, P.Y. Lateral Condyle Fracture of the Humerus in Children Treated with Bioabsorbable Materials. Sci. World J. 2013, 2013, 869418. [Google Scholar] [CrossRef]
- Su, Y.; Chen, K.; Qin, J. Retrospective study of open reduction and internal fixation of lateral humeral condyle fractures with absorbable screws and absorbable sutures in children. Medicine 2019, 98, e17850. [Google Scholar] [CrossRef]
- Huang, X.; Liu, C.; Jia, G.; Yao, J.; Xu, J. Criteria of ultrasound-guided closed reduction with percutaneous pinning in unstable humeral lateral condylar fractures: A three-center retrospective cohort study. Front. Pediatr. 2024, 12, 1373913. [Google Scholar] [CrossRef]
- Sinikumpu, J.J.; Pokka, T.; Victorzon, S.; Lindholm, E.L.; Serlo, W. Paediatric lateral humeral condylar fracture outcomes at twelve years follow-up as compared with age and sex matched paired controls. Int. Orthop. 2017, 41, 1453–1461. [Google Scholar] [CrossRef]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Mean | |
|---|---|
| Age | 6.06 |
| Follow-up (months) | 42.00 |
| VAS score | 0.17 |
| MAYO Score | 99.58 |
| Healing (days) | 33.00 |
| Surgery time (min) | 55.42 |
| Nr | |
| Patients | 36 |
| Male | 21 [58.3%] |
| Female | 15 [41.7%] |
| Mean | SD | Range | |
|---|---|---|---|
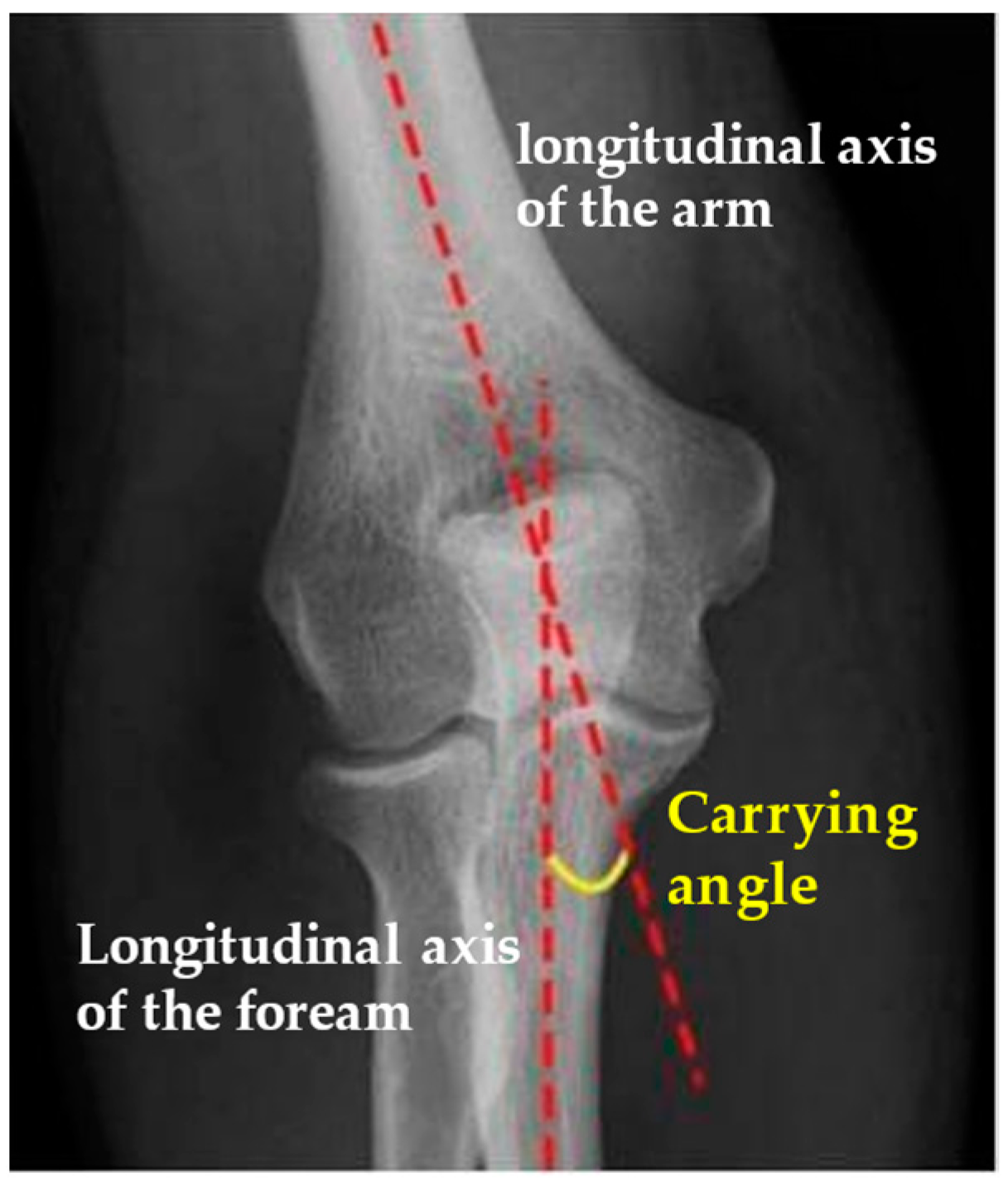
| Carrying Angle | 12.3° | 4.28 | 5–22° |
| Contralateral Carrying Angle | 12.3° | 3.87 | 5.9–20° |
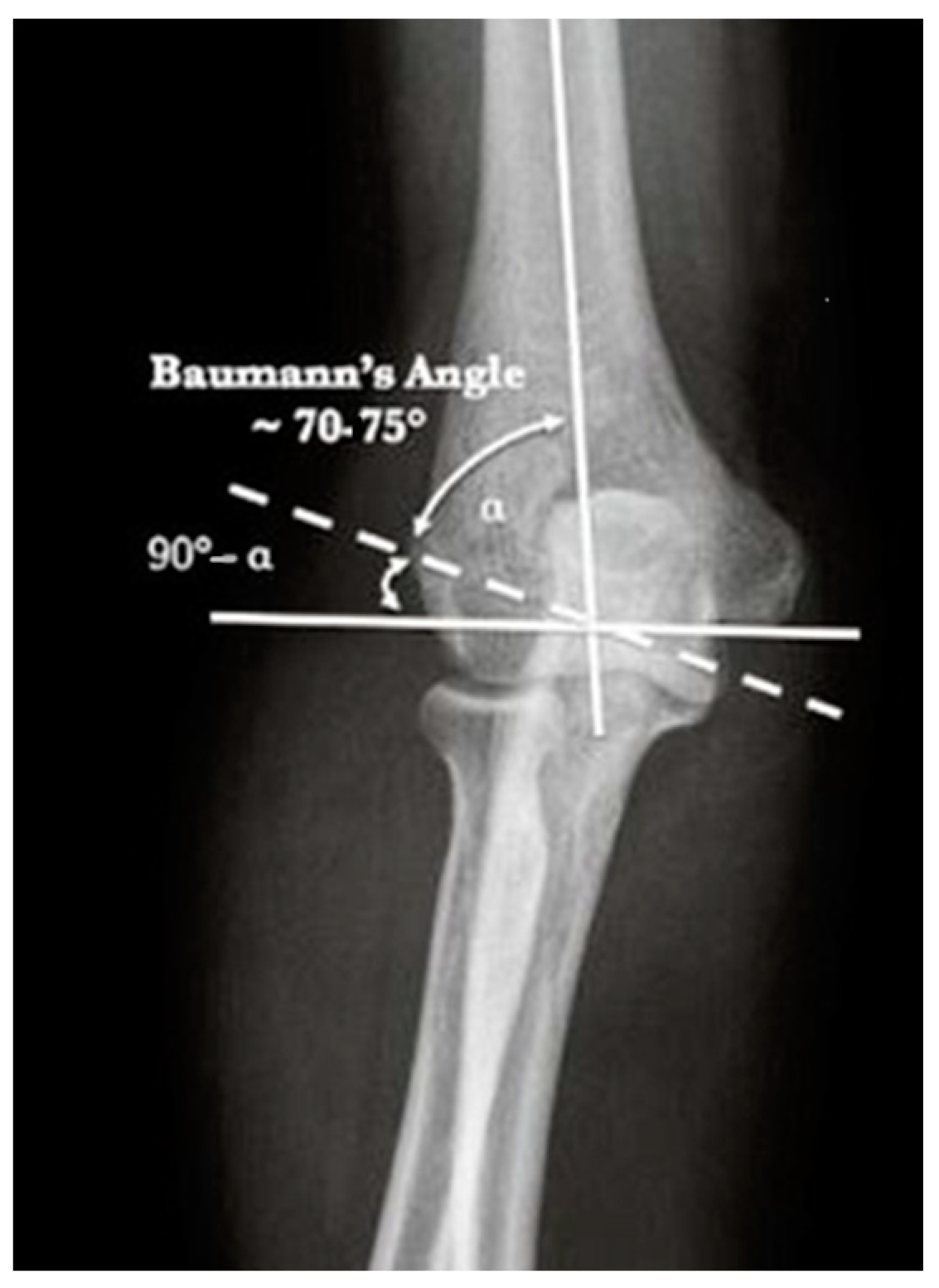
| Baumann Angle | 78.9° | 13.5 | 60.4–112° |
| Contralateral Baumann Angle | 79.1° | 12.7 | 63–118.8° |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Masci, G.; Basiglini, L.; Giusti, C.; Aulisa, A.G.; Falciglia, F. Lateral Humeral Condyle Fracture in Childhood: Results of a New Surgical Technique. J. Clin. Med. 2024, 13, 2830. https://doi.org/10.3390/jcm13102830
Masci G, Basiglini L, Giusti C, Aulisa AG, Falciglia F. Lateral Humeral Condyle Fracture in Childhood: Results of a New Surgical Technique. Journal of Clinical Medicine. 2024; 13(10):2830. https://doi.org/10.3390/jcm13102830
Chicago/Turabian StyleMasci, Giulia, Luca Basiglini, Carlotta Giusti, Angelo Gabriele Aulisa, and Francesco Falciglia. 2024. "Lateral Humeral Condyle Fracture in Childhood: Results of a New Surgical Technique" Journal of Clinical Medicine 13, no. 10: 2830. https://doi.org/10.3390/jcm13102830
APA StyleMasci, G., Basiglini, L., Giusti, C., Aulisa, A. G., & Falciglia, F. (2024). Lateral Humeral Condyle Fracture in Childhood: Results of a New Surgical Technique. Journal of Clinical Medicine, 13(10), 2830. https://doi.org/10.3390/jcm13102830