
Impact of Altered Body Composition on Clinical and Oncological Outcomes in Intrahepatic Cholangiocarcinoma

 ,
,  , ,
, ,
Abstract
:
1. Introduction
2. Materials and Methods
2.1. Study Population
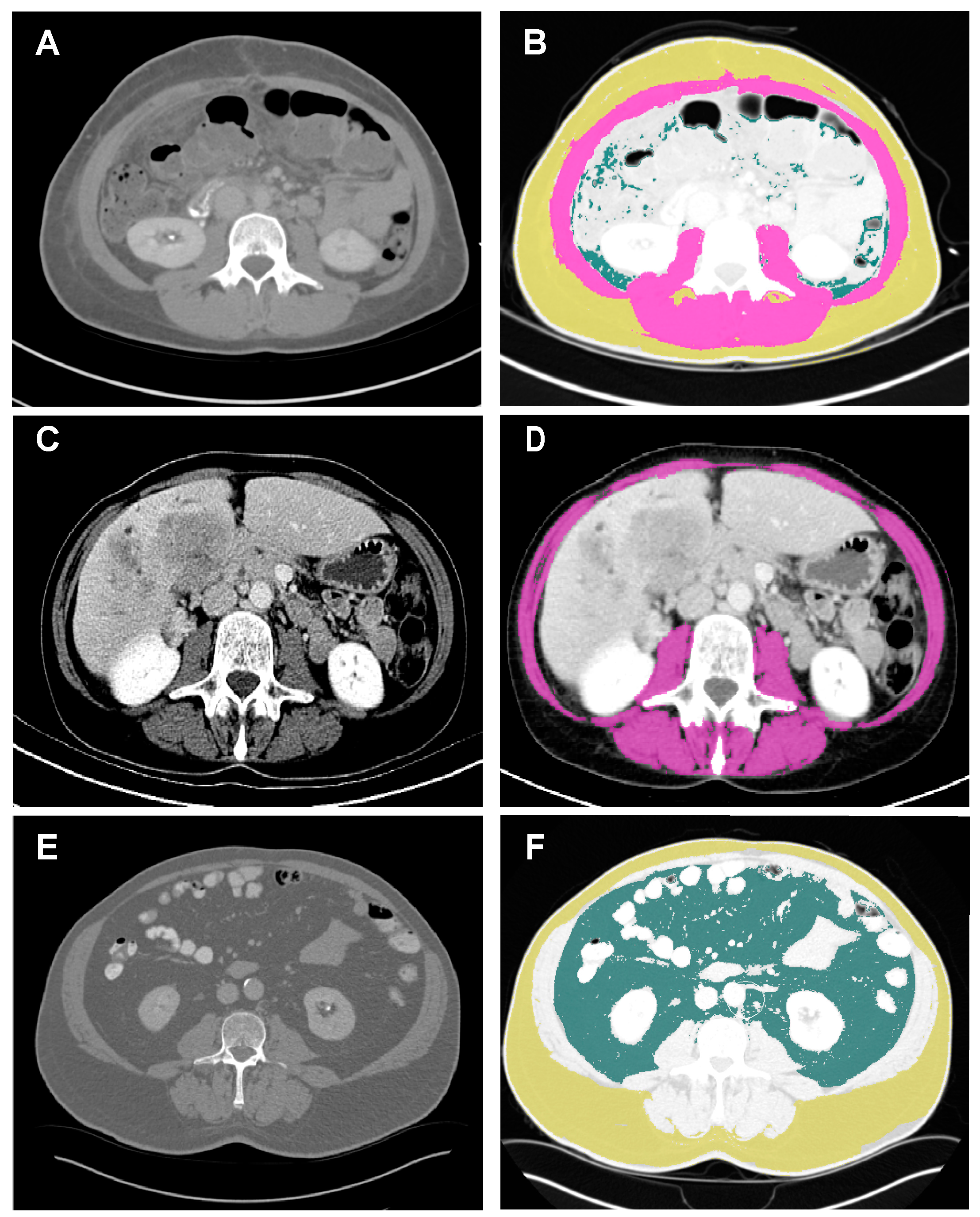
2.2. Body Composition Measurement
2.3. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Associations between Body Composition and Clinical and Laboratory Features
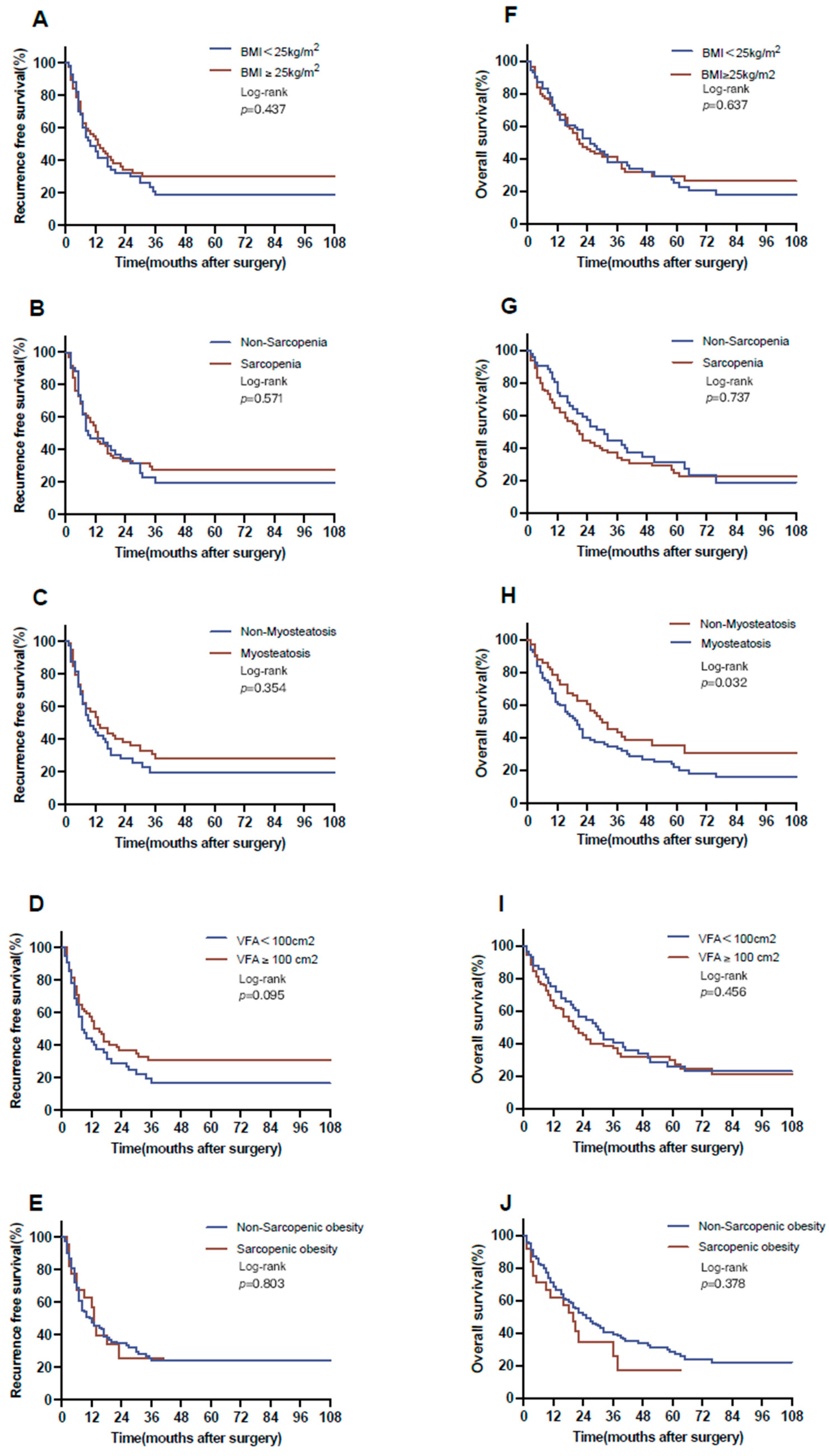
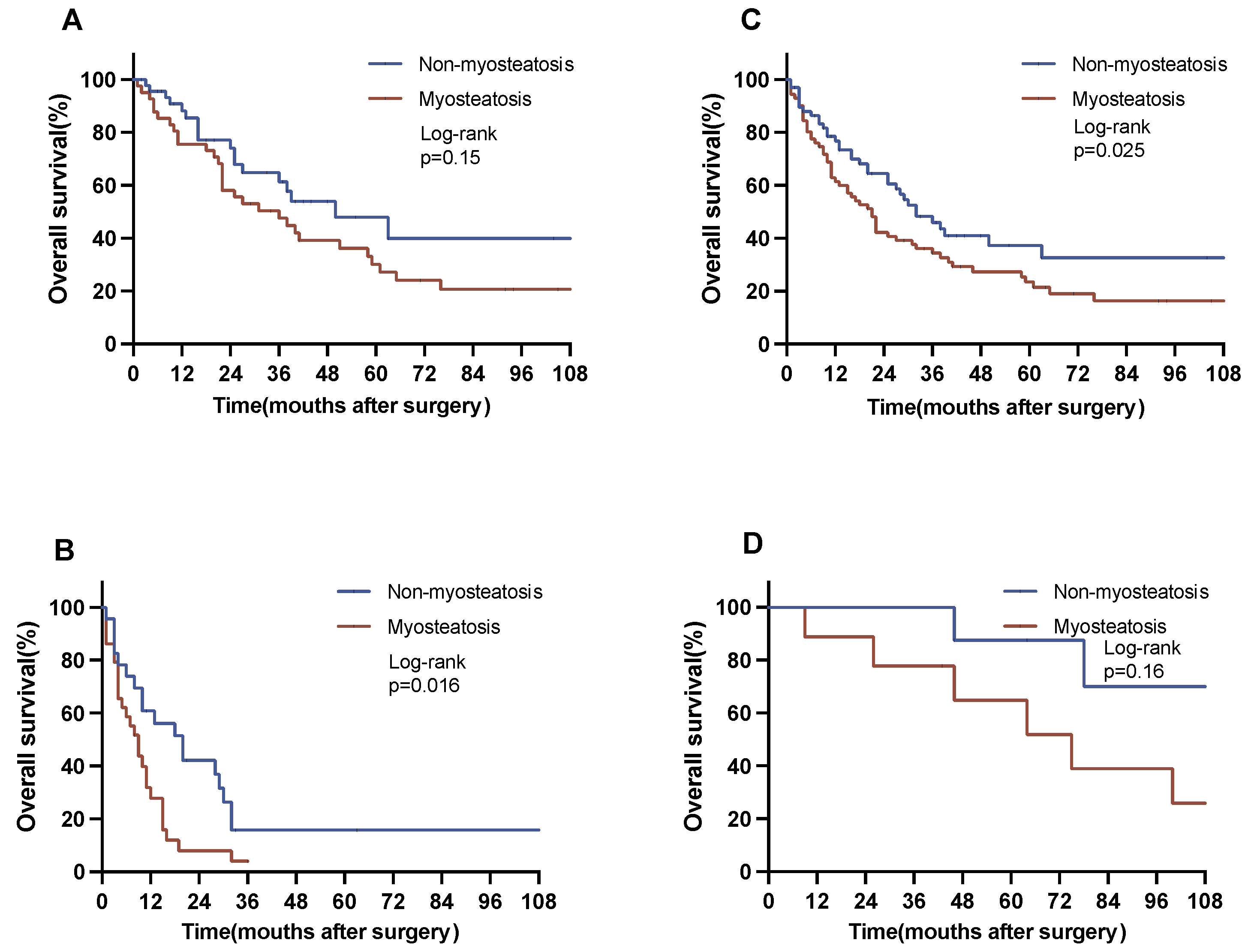
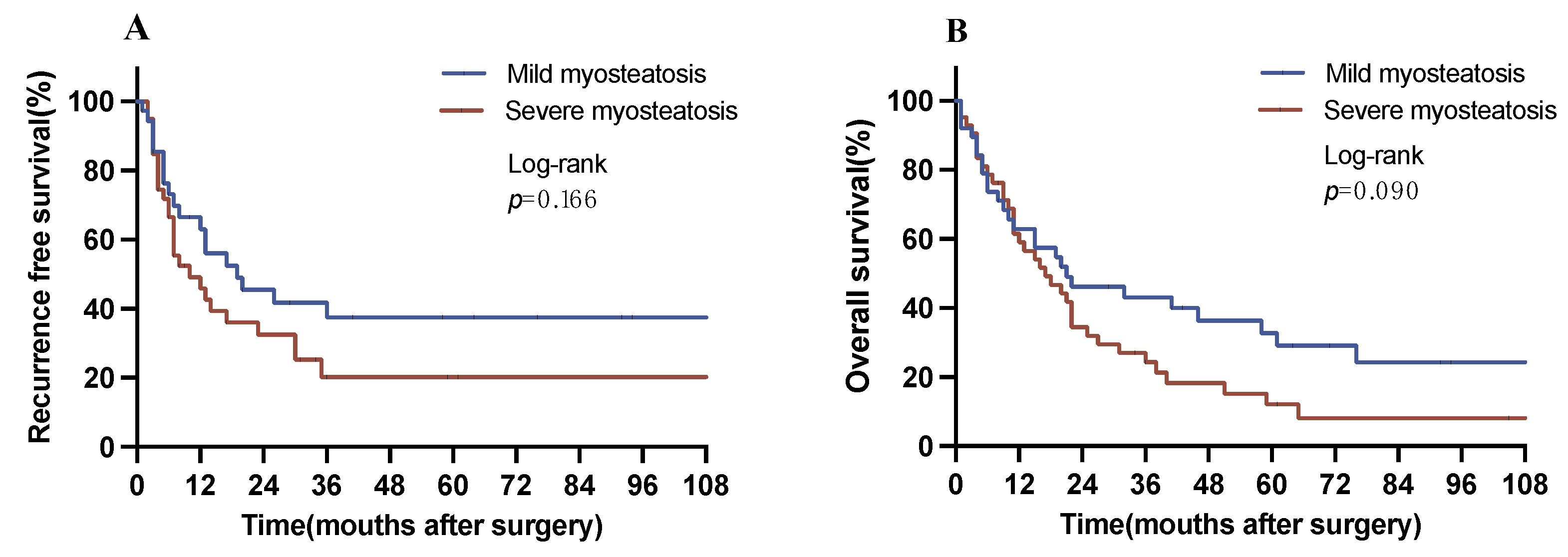
3.3. Kaplan–Meier Analysis
3.4. Oncological Outcomes in iCCA
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J. Clin. 2022, 72, 7–33. [Google Scholar] [CrossRef] [PubMed]
- Endo, I.; Gonen, M.; Yopp, A.; Dalal, K.; Zhou, Q.; Klimstra, D.; D’Angelica, M.; DeMatteo, R.; Fong, Y.; Schwartz, L.; et al. Intrahepatic cholangiocarcinoma: Rising frequency, improved survival, and determinants of outcome after resection. Ann. Surg. 2008, 248, 84–96. [Google Scholar] [CrossRef] [PubMed]
- Bednarsch, J.; Czigany, Z.; Heij, L.R.; Liu, D.; Dulk, M.D.; Wiltberger, G.; Bruners, P.; Ulmer, T.F.; Neumann, U.P.; Lang, S.A. Compelling Long-Term Results for Liver Resection in Early Cholangiocarcinoma. J. Clin. Med. 2021, 10, 2959. [Google Scholar] [CrossRef] [PubMed]
- Yao, K.J.; Jabbour, S.; Parekh, N.; Lin, Y.; Moss, R.A. Increasing mortality in the United States from cholangiocarcinoma: An analysis of the National Center for Health Statistics Database. BMC Gastroenterol. 2016, 16, 117. [Google Scholar] [CrossRef]
- Wang, J.; Tan, S.; Gianotti, L.; Wu, G. Evaluation and management of body composition changes in cancer patients. Nutrition 2023, 114, 112132. [Google Scholar] [CrossRef]
- Muscaritoli, M.; Arends, J.; Bachmann, P.; Baracos, V.; Barthelemy, N.; Bertz, H.; Bozzetti, F.; Hütterer, E.; Isenring, E.; Kaasa, S.; et al. ESPEN practical guideline: Clinical Nutrition in cancer. Clin. Nutr. 2021, 40, 2898–2913. [Google Scholar] [CrossRef]
- Iwase, T.; Wang, X.; Shrimanker, T.V.; Kolonin, M.G.; Ueno, N.T. Body composition and breast cancer risk and treatment: Mechanisms and impact. Breast Cancer Res. Treat. 2021, 186, 273–283. [Google Scholar] [CrossRef]
- Guo, Y.; Ren, Y.; Zhu, L.; Yang, L.; Zheng, C. Association between sarcopenia and clinical outcomes in patients with hepatocellular carcinoma: An updated meta-analysis. Sci. Rep. 2023, 13, 934. [Google Scholar] [CrossRef]
- Juez, L.D.; Priego, P.; Bajawi, M.; Cuadrado, M.; Blázquez, L.A.; Sánchez-Picot, S.; Galindo, J.; Blázquez, J.; Fernández-Cebrián, J.M.; Botella-Carretero, J.I. Impact of Sarcopenic Obesity on Long-Term Cancer Outcomes and Postoperative Complications After Gastrectomy for Gastric Cancer. J. Gastrointest. Surg. 2023, 27, 35–46. [Google Scholar] [CrossRef]
- Kim, H.J.; Kim, C.Y.; Hur, Y.H.; Koh, Y.S.; Kim, J.C.; Kim, H.J.; Cho, C.K. Prognostic factors for survival after curative resection of distal cholangiocarcinoma: Perineural invasion and lymphovascular invasion. Surg. Today 2014, 44, 1879–1886. [Google Scholar] [CrossRef]
- Lurje, G.; Bednarsch, J.; Czigany, Z.; Lurje, I.; Schlebusch, I.K.; Boecker, J.; Meister, F.A.; Tacke, F.; Roderburg, C.; Dulk, M.D.; et al. The prognostic role of lymphovascular invasion and lymph node metastasis in perihilar and intrahepatic cholangiocarcinoma. Eur. J. Surg. Oncol. 2019, 45, 1468–1478. [Google Scholar] [CrossRef]
- Rizvi, S.; Gores, G.J. Pathogenesis, diagnosis, and management of cholangiocarcinoma. Gastroenterology 2013, 145, 1215–1229. [Google Scholar] [CrossRef] [PubMed]
- Gu, Q.; He, M.; He, Y.; Dai, A.; Liu, J.; Chen, X.; Liu, P. CT-measured body composition radiomics predict lymph node metastasis in localized pancreatic ductal adenocarcinoma. Discov. Oncol. 2023, 14, 16. [Google Scholar] [CrossRef] [PubMed]
- Levolger, S.; A van Vugt, J.L.; de Bruin, R.W.F.; Ijzermans, J.N.M. Systematic review of sarcopenia in patients operated on for gastrointestinal and hepatopancreatobiliary malignancies. Br. J. Surg. 2015, 102, 1448–1458. [Google Scholar] [CrossRef] [PubMed]
- Cao, Q.; Xiong, Y.; Zhong, Z.; Ye, Q. Computed Tomography-Assessed Sarcopenia Indexes Predict Major Complications following Surgery for Hepatopancreatobiliary Malignancy: A Meta-Analysis. Ann. Nutr. Metab. 2019, 74, 24–34. [Google Scholar] [CrossRef] [PubMed]
- Dicken, B.J.; Graham, K.; Hamilton, S.M.; Andrews, S.; Lai, R.; Listgarten, J.; Jhangri, G.S.; Saunders, D.; Damaraju, S.; Cass, C. Lymphovascular invasion is associated with poor survival in gastric cancer: An application of gene-expression and tissue array techniques. Ann. Surg. 2006, 243, 64–73. [Google Scholar] [CrossRef] [PubMed]
- Hwang, J.-E.; Hong, J.-Y.; Kim, J.E.; Shim, H.-J.; Bae, W.-K.; Hwang, E.-C.; Jeong, O.; Park, Y.K.; Lee, K.-H.; Lee, J.-H.; et al. Prognostic significance of the concomitant existence of lymphovascular and perineural invasion in locally advanced gastric cancer patients who underwent curative gastrectomy and adjuvant chemotherapy. Jpn J. Clin. Oncol. 2015, 45, 541–546. [Google Scholar] [CrossRef]
- Wu, J.; Chen, Q.X. Prognostic and predictive significance of tumor length in patients with esophageal squamous cell carcinoma undergoing radical resection. BMC Cancer 2016, 16, 394. [Google Scholar] [CrossRef]
- Skancke, M.; Arnott, S.M.; Amdur, R.L.; Siegel, R.S.; Obias, V.J.; Umapathi, B.A. Lymphovascular Invasion and Perineural Invasion Negatively Impact Overall Survival for Stage II Adenocarcinoma of the Colon. Dis. Colon Rectum 2019, 62, 181–188. [Google Scholar] [CrossRef]
- Bagante, F.; Spolverato, G.; Weiss, M.; Alexandrescu, S.; Marques, H.P.; Aldrighetti, L.; Maithel, S.K.; Pulitano, C.; Bauer, T.W.; Shen, F.; et al. Assessment of the Lymph Node Status in Patients Undergoing Liver Resection for Intrahepatic Cholangiocarcinoma: The New Eighth Edition AJCC Staging System. J. Gastrointest. Surg. 2018, 22, 52–59. [Google Scholar] [CrossRef]
- de Jong, M.C.; Nathan, H.; Sotiropoulos, G.C.; Paul, A.; Alexandrescu, S.; Marques, H.; Pulitano, C.; Barroso, E.; Clary, B.M.; Aldrighetti, L.; et al. Intrahepatic cholangiocarcinoma: An international multi-institutional analysis of prognostic factors and lymph node assessment. J. Clin. Oncol. 2011, 29, 3140–3145. [Google Scholar] [CrossRef] [PubMed]
- Shimada, M.; Yamashita, Y.; Aishima, S.; Shirabe, K.; Takenaka, K.; Sugimachi, K. Value of lymph node dissection during resection of intrahepatic cholangiocarcinoma. Br. J. Surg. 2001, 88, 1463–1466. [Google Scholar] [CrossRef] [PubMed]
- Yamamoto, M.; Takasaki, K.; Yoshikawa, T. Lymph node metastasis in intrahepatic cholangiocarcinoma. Jpn J. Clin. Oncol. 1999, 29, 147–150. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.; Lin, L.; Lin, Z.; Chen, Y.; Huang, Q.; Ding, L.; Lou, J.; Zheng, S.; Bi, X.; Wang, J.; et al. Impact of surgical margin width on long-term outcomes for intrahepatic cholangiocarcinoma: A multicenter study. BMC Cancer 2021, 21, 840. [Google Scholar] [CrossRef] [PubMed]
- Li, M.-X.; Bi, X.-Y.; Li, Z.-Y.; Huang, Z.; Han, Y.; Zhao, J.-J.; Zhao, H.; Cai, J.-Q. Impaction of surgical margin status on the survival outcome after surgical resection of intrahepatic cholangiocarcinoma: A systematic review and meta-analysis. J. Surg. Res. 2016, 203, 163–173. [Google Scholar] [CrossRef] [PubMed]
- Tang, H.; Lu, W.; Li, B.; Meng, X.; Dong, J. Influence of surgical margins on overall survival after resection of intrahepatic cholangiocarcinoma: A meta-analysis. Medicine 2016, 95, e4621. [Google Scholar] [CrossRef] [PubMed]
- Valero, V., 3rd; Amini, N.; Spolverato, G.; Weiss, M.J.; Hirose, K.; Dagher, N.N.; Wolfgang, C.L.; Cameron, A.A.; Philosophe, B.; Kamel, I.R.; et al. Sarcopenia adversely impacts postoperative complications following resection or transplantation in patients with primary liver tumors. J. Gastrointest. Surg. 2015, 19, 272–281. [Google Scholar] [CrossRef]
- Marasco, G.; Dajti, E.; Serenari, M.; Alemanni, L.V.; Ravaioli, F.; Ravaioli, M.; Vestito, A.; Vara, G.; Festi, D.; Golfieri, R.; et al. Sarcopenia Predicts Major Complications after Resection for Primary Hepatocellular Carcinoma in Compensated Cirrhosis. Cancers 2022, 14, 1935. [Google Scholar] [CrossRef]
- Yang, J.; Chen, K.; Zheng, C.; Chen, K.; Lin, J.; Meng, Q.; Chen, Z.; Deng, L.; Yu, H.; Deng, T.; et al. Impact of sarcopenia on outcomes of patients undergoing liver resection for hepatocellular carcinoma. J. Cachexia Sarcopenia Muscle 2022, 13, 2383–2392. [Google Scholar] [CrossRef]
- Yang, J.; Wang, D.; Ma, L.; An, X.; Hu, Z.; Zhu, H.; Zhang, W.; Chen, K.; Ma, J.; Yang, Y.; et al. Sarcopenia negatively affects postoperative short-term outcomes of patients with non-cirrhosis liver cancer. BMC Cancer 2023, 23, 212. [Google Scholar] [CrossRef]
- Lutz, C.T.; Quinn, L.S. Sarcopenia, obesity, and natural killer cell immune senescence in aging: Altered cytokine levels as a common mechanism. Aging 2012, 4, 535–546. [Google Scholar] [CrossRef] [PubMed]
- Pedersen, B.K.; Febbraio, M.A. Muscles, exercise and obesity: Skeletal muscle as a secretory organ. Nat. Rev. Endocrinol. 2012, 8, 457–465. [Google Scholar] [CrossRef] [PubMed]
- Yasuta, S.; Sugimoto, M.; Kudo, M.; Kobayashi, S.; Takahashi, S.; Konishi, M.; Gotohda, N. Early postoperative decrease of skeletal muscle mass predicts recurrence and poor survival after surgical resection for perihilar cholangiocarcinoma. BMC Cancer 2022, 22, 1358. [Google Scholar] [CrossRef] [PubMed]
- Jung, H.E.; Han, D.H.; Koo, B.N.; Kim, J. Effect of sarcopenia on postoperative ICU admission and length of stay after hepatic resection for Klatskin tumor. Front. Oncol. 2023, 13, 1136376. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.-X.; Ding, Y.; Yan, H.-T.; Zhou, C.-G.; Liu, J.; Liu, S.; Zu, Q.-Q.; Shi, H.-B. Skeletal-muscle index predicts survival after percutaneous transhepatic biliary drainage for obstructive jaundice due to perihilar cholangiocarcinoma. Surg. Endosc. 2021, 35, 6073–6080. [Google Scholar] [CrossRef] [PubMed]
- Yagi, N.; Suzuki, T.; Mizuno, S.; Kojima, M.; Kudo, M.; Sugimoto, M.; Kobayashi, S.; Gotohda, N.; Ishii, G.; Nakatsura, T. Component with abundant immune-related cells in combined hepatocellular cholangiocarcinoma identified by cluster analysis. Cancer Sci. 2022, 113, 1564–1574. [Google Scholar] [CrossRef] [PubMed]
- Tantai, X.; Liu, Y.; Yeo, Y.H.; Praktiknjo, M.; Mauro, E.; Hamaguchi, Y.; Engelmann, C.; Zhang, P.; Jeong, J.Y.; van Vugt, J.L.A.; et al. Effect of sarcopenia on survival in patients with cirrhosis: A meta-analysis. J. Hepatol. 2022, 76, 588–599. [Google Scholar] [CrossRef]
- Paradis, V.; Zucman-Rossi, J. Pathogenesis of primary liver carcinomas. J. Hepatol. 2023, 78, 448–449. [Google Scholar] [CrossRef]
- Herbst, E.A.F.; Paglialunga, S.; Gerling, C.; Whitfield, J.; Mukai, K.; Chabowski, A.; Heigenhauser, G.J.F.; Spriet, L.L.; Holloway, G.P. Omega-3 supplementation alters mitochondrial membrane composition and respiration kinetics in human skeletal muscle. J. Physiol. 2014, 592, 1341–1352. [Google Scholar] [CrossRef]
- Almasud, A.A.; Giles, K.H.; Miklavcic, J.J.; Martins, K.J.B.; Baracos, V.E.; Putman, C.T.; Guan, L.L.; Mazurak, V.C. Fish oil mitigates myosteatosis and improves chemotherapy efficacy in a preclinical model of colon cancer. PLoS ONE 2017, 12, e0183576. [Google Scholar] [CrossRef]
- Mallard, J.; Hucteau, E.; Bender, L.; Charlot, A.; Debrut, L.; Pflumio, C.; Trensz, P.; Schott, R.; Favret, F.; Pivot, X.; et al. Development of skeletal muscle atrophy and intermuscular adipose tissue in patients with early breast cancer treated with chemotherapy. Am. J. Physiol. Cell Physiol. 2022, 323, C1325–C1332. [Google Scholar] [CrossRef] [PubMed]
- Lorsy, E.; Topuz, A.S.; Geisler, C.; Stahl, S.; Garczyk, S.; von Stillfried, S.; Hoss, M.; Gluz, O.; Hartmann, A.; Knüchel, R.; et al. Loss of Dickkopf 3 Promotes the Tumorigenesis of Basal Breast Cancer. PLoS ONE 2016, 11, e0160077. [Google Scholar] [CrossRef] [PubMed]
- Gauger, K.J.; Bassa, L.M.; Henchey, E.M.; Wyman, J.; Bentley, B.; Brown, M.; Shimono, A.; Schneider, S.S. Mice deficient in Sfrp1 exhibit increased adiposity, dysregulated glucose metabolism, and enhanced macrophage infiltration. PLoS ONE 2013, 8, e78320. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Li, F.; Feng, J.; Wang, J.; Liu, X. The effects of S-nitrosylation-induced PPARγ/SFRP5 pathway inhibition on the conversion of non-alcoholic fatty liver to non-alcoholic steatohepatitis. Ann. Transl. Med. 2021, 9, 684. [Google Scholar] [CrossRef]
- Dahl, E.; Villwock, S.; Habenberger, P.; Choidas, A.; Rose, M.; Klebl, B.M. White Paper: Mimetics of Class 2 Tumor Suppressor Proteins as Novel Drug Candidates for Personalized Cancer Therapy. Cancers 2022, 14, 4386. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variables | iCCA (n = 162) |
| Demographics | |
| Gender, M/F (%) | 76 (46.9)/86 (53.1) |
| Age (years) | 66 (58–74) |
| ASA, n (%) | |
| I | 4 (2.5) |
| II | 64 (39.5) |
| III | 87 (53.7) |
| IV | 7 (4.3) |
| V | 0 (0) |
| Cholangitis, n (%) | 10 (6.2) |
| Portal vein embolization, n (%) | 14 (8.6) |
| Preoperative chemotherapy, n (%) | 21 (13.0) |
| Clinical chemistry | |
| AST (U/L) | 33.0 (25.0–46.0) |
| ALT (U/L) | 27.0 (18.0–48.0) |
| Albumin (g/L) | 4.3 (4.0–4.6) |
| AP, U/L | 118.0 (85.5–217.0) |
| CA199 (U/mL) | 55.20 (20.00–274.40) |
| CRP (mg/L) | 55.20 (20.00–274.40) |
| GGT (U/L) | 109.0 (55.5–299.0) |
| Hemoglobin (g/dL) | 13.0 (12.00–14.20) |
| INR | 1.00 (0.96–1.07) |
| Platelet count (/nL) | 247 (193–306) |
| Prothrombin time (%) | 100 (89–107) |
| Total bilirubin (mg/dL) | 0.46 (0.335–0.690) |
| Operative Data | |
| Intraoperative PRBC, n (%) | 48 (29.6) |
| Intraoperative FFP, n (%) | 56 (34.6) |
| Operative time (minutes) | 300 (230–362) |
| Operative procedure, n (%) | |
| Bisegmentectomy | 23 (14.1) |
| Hemihepatectomy | 57 (35.0) |
| Extended hemihepatectomy | 31 (19.0) |
| Trisectionectomy | 20 (12.3) |
| Hepatoduodenoectomy | 0 (0) |
| ALPPS | 14 (8.6) |
| Others | 18 (11.0) |
| Time to surgery, days | 47 (30–89) |
| Pathological examination | |
| LVI, n (%) | 33 (20.4) |
| MVI, n (%) | 52 (32.1) |
| R1 resection, n (%) | 16 (9.9) |
| pT category n (%) | |
| 1 | 58 (35.8) |
| 2 | 62 (38.3) |
| 3 | 24 (14.8) |
| 4 | 17 (10.5) |
| pN category, n (%) | |
| N0 | 91 (56.2) |
| N1 | 57 (35.2) |
| Tumor grading, n (%) | |
| G1 | 2 (1.2) |
| G2 | 94 (58.0) |
| G3 | 42 (25.9) |
| G4 | 5 (3.1) |
| Postoperative Data | |
| Intensive care, days | 1 (1–1) |
| Hospitalization, days | 13 (8–26) |
| Postoperative complications, n (%) | |
| No complications | 56 (34.6) |
| Clavien–Dindo I | 8 (4.9) |
| Clavien–Dindo II | 30 (18.5) |
| Clavien–Dindo IIIa | 34 (20.9) |
| Clavien–Dindo IIIb | 13 (8.0) |
| Clavien–Dindo IVa | 8 (5.0) |
| Clavien–Dindo IVb | 1 (0.6) |
| Clavien–Dindo V | 12 (7.4) |
| Liver failure, n (%) | |
| No failure | 135 (82.8) |
| Grade A | 13 (8.0) |
| Grade B | 8 (4.9) |
| Grade C | 7 (4.3) |
| Infection Clavien–Dindo | |
| No complications | 89 (54.6) |
| Clavien–Dindo I | 0 (0) |
| Clavien–Dindo II | 30 (18.4) |
| Clavien–Dindo IIIa | 30 (18.4) |
| Clavien–Dindo IIIb | 4 (2.5) |
| Clavien–Dindo IVa | 0 (0) |
| Clavien–Dindo IVb | 1 (0.6) |
| Clavien–Dindo V | 8 (4.9) |
| Bile leak, n (%) | |
| No | 134 (82.2) |
| Grade A | 3 (1.8) |
| Grade B | 20 (12.3) |
| Grade C | 6 (3.7) |
| Hemorrhage, n (%) | |
| No | 150 (92.0) |
| Grade A | 2 (1.2) |
| Grade B | 2 (1.2) |
| Grade C | 9 (5.5) |
| Oncologic Data | |
| Adjuvant chemotherapy, n (%) | 56 (34.6) |
| Recurrence, n (%) | 95 (58.6) |
| Median RFS, months (95% CI) | 12 (8–16) |
| Median OS, months (95% CI) | 22 (17–28) |
| Body composition | |
| BMI (kg/m2) | 25.35 (22.61–29.27) |
| Visceral_fat area (cm2) | 131.82 (64.67–216.76) |
| SMI (cm2/m2) | 43.27 (38.93–50.24) |
| SM-RA (HU) | 37.06 (28.97–41.72) |
| Obesity, n (%) | 86 (53.1) |
| Sarcopenia, n (%) | 103 (63.2) |
| Myosteatosis, n (%) | 86 (52.8) |
| Visceral obesity, n (%) | 101 (62.3) |
| Sarcopenic_obesity, n (%) | 25 (15.3) |
| Outcome | Descriptives | Univariate Analysis | Multivariate Analysis | |||
|---|---|---|---|---|---|---|
| BMI (kg/m2) | <25 (n = 77) | ≥25 (n = 85) | OR (95% CI) | p= | OR (95% CI) | p= |
| Sex (male/female (%); ref = male) | 30 (39.0)/47 (61.0) | 46 (54.1)/39 (45.9) | 0.541 (0.289–1.012) | 0.055 | 0.431 (0.177–1.046) | 0.063 |
| ASA ((I/II)/(III/IV) (%); ref = I/II) | 38 (49.4)/39 (50.6) | 30 (35.3)/55 (64.7) | 1.786 (0.951–3.356) | 0.071 | 2.029 (0.785–5.243) | 0.144 |
| Cholangitis (no/yes (%); ref = no) | 69 (89.6)/8 (10.4) | 83 (97.6)/2 (2.4) | 0.208 (0.043–1.011) | 0.052 | 0.244 (0.017–3.406) | 0.294 |
| Albumin, g/L (≤4.2/>4.2 (%); ref = ≤4.2) | 34 (44.2)/25 (32.5) | 27 (31.8)/43 (50.6) | 2.166 (1.069–4.387) | 0.032 | 2.075 (0.937–4.595) | 0.072 |
| AP, U/L (≤100/>100 (%); ref = ≤100) | 20 (26.0)/53 (68.8) | 38 (44.7)/45 (52.9) | 0.447 (0.228–0.875) | 0.019 | 0.598 (0.249–1.437) | 0.251 |
| Hemoglobin, g/L (≤13/>13 (%); ref = ≤13) | 51 (66.2)/25 (32.5) | 25 (29.4)/59 (69.4) | 4.814 (2.466–9.40) | 0.001 | 6.443 (2.538–16.359) | <0.001 |
| Platelet count (≤300/>300 (%); ref = ≤300) | 50 (64.9)/26 (33.8) | 67 (78.8)/17 (20.0) | 0.488 (0.239–0.995) | 0.048 | 0.517 (0.172–1.552) | 0.240 |
| Prothrombin time (≤110/>110 (%); ref = ≤110) | 56 (72.7)/20 (26.0) | 73 (85.9)/10 (11.8) | 0.384 (0.166–0.884) | 0.025 | 0.229 (0.072–0.733) | 0.013 |
| Intraoperative PRBC (no/yes (%); ref = no) | 49 (63.6)/28 (36.4) | 65 (76.5)/20 (23.5) | 0.538 (0.272–1.066) | 0.076 | 1.479 (0.396–5.525) | 0.561 |
| R1 resection ((R0/R2)/R1) (%); ref = R0/R2) | 66 (85.7)/11 (14.3) | 79 (92.9)/5 (5.9) | 0.380 (0.126–1.148) | 0.086 | 0.477 (0.095–2.400) | 0.369 |
| pT category (T1–2/T3–4 (%); ref = T1–T2) | 50 (64.9)/26 (33.8) | 70 (82.4)/15 (17.6) | 0.412 (0.198–0.857) | 0.018 | 0.296 (0.101–0.864) | 0.026 |
| Hospitalization, days (≤14/>14 (%); ref = ≤14) | 32 (41.6)/45 (58.4) | 55 (64.7)/30 (35.3) | 0.388 (0.206–0.732) | 0.003 | 0.925 (0.274–3.122) | 0.900 |
| Postoperative complications Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 57 (74.0)/20 (26.0) | 71 (83.5)/14 (16.5) | 0.409 (0.216–0.775) | 0.006 | 0.663 (0.145–3.037) | 0.596 |
| Liver failure (no/yes (%); ref = no) | 58 (75.3)/19 (24.7) | 76 (89.4)/9 (10.6) | 0.361 (0.152–0.857) | 0.021 | 0.548 (0.158–1.893) | 0.341 |
| Bile leak (no/yes (%); ref = no) | 56 (72.7)/21 (27.3) | 77 (90.6)/8 (9.4) | 0.277 (0.114–0.671) | 0.004 | 0.426 (0.123–1.467) | 0.176 |
| Hemorrhage (no/yes (%); ref = no) | 70 (90.9)/7 (9.1) | 79 (92.9)/6 (7.1) | 0.759 (0.244–2.367) | 0.635 | ||
| Infection Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 66 (85.7)/10 (13.0) | 82 (96.5)/3 (3.5) | 0.421 (0.205–0.863) | 0.018 | 0.896 (0.754–14.397) | 0.113 |
| Sarcopenia | No (n = 59) | Yes (n = 103) | OR (95% CI) | p= | OR (95% CI) | p= |
| Sex (male/female (%); ref = male) | 40 (67.8)/19 (32.2) | 36 (35.0)/67 (65.0) | 3.918 (1.985–7.733) | <0.001 | 2.263 (0.898–5.701) | <0.001 |
| Hemoglobin, g/L (≤13/>13 (%); ref = ≤13) | 22 (37.3)/36 (61.0) | 54 (52.4)/48 (46.6) | 0.543 (0.281–1.049) | 0.069 | 0.560 (0.270–1.160) | 0.119 |
| LVI (no/yes (%); ref = no) | 49 (83.1)/8 (13.6) | 70 (68.0)/25 (24.3) | 2.187 (0.911–5.252) | 0.080 | 2.307 (0.906–5.874) | 0.080 |
| Postoperative complications Clavien–Dindo ((0/I/II )/(III/IV/V) (%); ref = 0/I/II) | 47 (79.7)/12 (20.3) | 81 (78.6)/22 (21.4) | 0.874 (0.458–1.669) | 0.683 | ||
| Liver failure (no/yes (%); ref = no) | 47 (79.7)/12 (20.3) | 87 (84.5)/16 (15.5) | 0.720 (0.315–1.649) | 0.438 | ||
| Bile leak (no/yes (%); ref = no) | 46 (78.0)/13 (22.0) | 87 (84.5)/16 (15.5) | 0.651 (0.288–1.469) | 0.301 | ||
| Hemorrhage (no/yes (%); ref = no) | 55 (93.2)/4 (6.8) | 94 (91.3)/9 (8.7) | 1.316 (0.387–4.477) | 0.660 | ||
| Infection Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 54 (91.5)/5 (8.5) | 94 (91.3)/8 (7.8) | 0.740 (0.362–1.511) | 0.408 | ||
| Myosteatosis | No (n = 76) | Yes (n = 86) | OR (95% CI) | p= | OR (95% CI) | p= |
| Sex (male/female (%); ref = male) | 43 (56.6)/33 (43.4) | 33 (38.4)/53 (61.6) | 2.093 (1.117–3.922) | 0.021 | 3.636 (1.447–9.132) | 0.006 |
| Age (≤65/>65 years (%); ref = ≤65) | 50 (65.8)/26 (34.2) | 30 (34.9)/56 (65.1) | 3.590 (1.876–6.870) | <0.001 | 4.989 (1.904–13.068) | 0.001 |
| Albumin, g/L (≤4.2/>4.2 (%); ref = ≤4.2) | 22 (28.9)/40 (52.6) | 39 (45.3)/28 (32.6) | 0.395 (0.194–804) | 0.010 | 0.817 (0.318–2.096) | 0.674 |
| Hemoglobin, g/L (≤13/>13 (%); ref = ≤13) | 25 (32.9)/50 (65.8) | 51 (59.3)/34 (39.5) | 0.333 (0.175–0.637) | 0.001 | 0.535 (0.230–1.242) | 0.145 |
| Total bilirubin, mg/dL (≤1/>1 (%); ref = ≤1) | 69 (90.8)/6 (7.9) | 69 (80.2)/16 (18.6) | 2.667 (0.985–7.219) | 0.054 | 2.141 (0.637–7.196) | 0.218 |
| Intraoperative PRBC (no/yes (%); ref = no) | 62 (81.6)/14 (18.4) | 52 (60.5)/34 (39.5) | 2.896 (1.405–5.969) | 0.004 | 1.594 (0.594–4.277) | 0.354 |
| LVI (no/yes (%); ref = no) | 60 (78.9)/10 (13.2) | 59 (68.6)/23 (26.7) | 2.339 (1.025–5.336) | 0.043 | 2.942 (1.047–8.268) | 0.041 |
| Postoperative complications Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 47 (61.8)/29 (38.2) | 47 (54.7)/39 (45.3) | 1.345 (0.718–2.520) | 0.355 | ||
| Liver failure (no/yes (%); ref = no) | 66 (86.8)/10 (13.2) | 68 (79.1)/18 (20.9) | 1.747 (0.751–4.063) | 0.195 | ||
| Bile leak (no/yes (%); ref = no) | 62 (81.6)/14 (18.4) | 71 (82.6)/15 (17.4) | 0.936 (0.419–2.091) | 0.871 | ||
| Hemorrhage (no/yes (%); ref = no) | 72 (94.7)/4 (5.3) | 77 (89.5)/9 (10.5) | 2.104 (0.621–7.132) | 0.232 | ||
| Infection Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 72 (94.7)/3 (3.9) | 76 (88.4)/10 (11.6) | 1.004 (0.499–2.022) | 0.991 | ||
| Adjuvant therapy (no/yes (%); ref = no) | 39 (51.3)/33 (43.4) | 62 (72.1)/23 (26.7) | 0.438 (0.225–0.854) | 0.015 | 0.485 (0.205–1.146) | 0.099 |
| VFA (cm2) | <100 (n = 61) | ≥100 (n = 101) | OR (95% CI) | p= | OR (95% CI) | p= |
| Sex (male/female (%); ref = male) | 13 (21.3)/48 (78.7) | 63 (62.4)/38 (37.6) | 0.163 (0.078–0.340) | <0.001 | 0.247 (0.114–0.536) | <0.001 |
| Age (≤65/>65 years (%); ref = ≤65) | 39 (63.9)/22 (36.1) | 41 (40.6)/60 (59.4) | 2.594 (1.346–5.001) | 0.004 | 3.577 (1.592–8.035) | 0.002 |
| Hemoglobin, g/L (≤13/>13 (%); ref = ≤13) | 37 (60.7)/22 (36.1) | 39 (38.6)/62 (61.4) | 2.674 (1.378–5.186) | 0.004 | 3.265 (1.455–7.325) | 0.004 |
| INR (≤1/>1 (%); ref = ≤1) | 36 (59.0)/23 (37.7) | 47 (46.5)/53 (52.5) | 1.765 (0.918–3.395) | 0.089 | 1.310 (0.603–2.844) | 0.495 |
| Hospitalization, days (≤14/>14 (%); ref = ≤14) | 26 (42.6)/35 (57.4) | 61 (60.4)/40 (39.6) | 0.487 (0.255–0.929) | 0.029 | 0.570 (0.260–1.251) | 0.161 |
| Postoperative complications Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 45 (73.8)/16 (26.2) | 63 (62.4)/38 (37.6) | 0.614 (0.323–1.167) | 0.136 | ||
| Liver failure (no/yes (%); ref = no) | 47 (77.0)/14 (23.0) | 87 (86.1)/14 (13.9) | 0.540 (0.238–1.228) | 0.142 | ||
| Bile leak (no/yes (%); ref = no) | 46 (75.4)/15 (24.6) | 87 (86.1)/14 (13.9) | 0.493 (0.219–1.111) | 0.088 | 0.636 (0.229–1.765) | 0.385 |
| Hemorrhage (no/yes (%); ref = no) | 55 (90.2)/6 (9.8) | 94 (93.1)/7 (6.9) | 0.683 (0.218–2.135) | 0.512 | ||
| Infection Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 42 (68.9)/18 (29.5) | 76 (75.2)/25 (24.8) | 0.758 (0.371–1.546) | 0.445 | ||
| Sarcopenic_obesity | No (n = 137) | Yes (n = 25) | OR (95% CI) | p= | OR (95% CI) | p= |
| Sex (male/female (%); ref = male) | 55 (40.1)/82 (59.9) | 21 (84.0)/4 (16.0) | 0.128 (0.042–0.393) | <0.001 | 0.180 (0.056–0.582) | 0.004 |
| Age (≤65/>65 years (%); ref = ≤65) | 74 (54.0)/63 (46.0) | 6 (24.0)/19 (76.0) | 3.720 (1.400–9.885) | 0.008 | 4.007 (1.375–11.674) | 0.011 |
| AP, U/L (≤100/>100 (%); ref = ≤100) | 45 (32.8)/86 (62.8) | 13 (52.0)/12 (48.0) | 0.483 (0.204–1.145) | 0.099 | 1.009 (0.292–3.479) | 0.989 |
| GGT,U/L (≤100/>100 (%); ref = ≤100) | 59 (43.1)/72 (52.6) | 17 (68.0)/8 (32.0) | 0.386 (0.156–0.956) | 0.040 | 0.405 (0.134–1.225) | 0.110 |
| INR (≤1/>1 (%); ref = ≤1) | 75 (54.7)/60 (43.8) | 8 (32.0)/16 (64.0) | 2.500 (1.002–6.236) | 0.049 | 1.247 (0.419–3.714) | 0.691 |
| Platelet count (≤300/>300 (%); ref = ≤300) | 95 (69.3)/40 (29.2) | 22 (88.0)/3 (12.0) | 0.324 (0.092–1.144) | 0.080 | 0.779 (0.184–3.299) | 0.735 |
| MVI (no/yes (%); ref = no) | 82 (59.9)/48 (35.0) | 21 (84.0)/4 (16.0) | 0.325 (0.105–1.004) | 0.051 | 0.438 (0.128–1.498) | 0.188 |
| Hospitalization, days (≤14/>14 (%); ref = ≤14) | 69 (50.4)/68 (49.6) | 18 (72.0)/7 (28.0) | 0.395 (0.155–1.005) | 0.051 | 2.382 (0.453–12.525) | 0.306 |
| Postoperative complications Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 74 (54.0)/63 (46.0) | 20 (80.0)/5 (20.0) | 0.294 (0.104–0.827) | 0.020 | 0.246 (0.080–0.760) | 0.015 |
| Liver failure (no/yes (%); ref = no) | 111 (81.0)/26 (19.0) | 23 (92.0)/2 (8.0) | 0.371 (0.082–1.675) | 0.197 | ||
| Bile leak (no/yes (%); ref = no) | 109 (79.6)/28 (20.4) | 24 (96.0)/1 (4.0) | 0.162 (0.021–1.251) | 0.081 | 0.363 (0.036–3.718) | 0.394 |
| Hemorrhage (no/yes (%); ref = no) | 124 (90.5)/13 (9.5) | 130 (81.3)/30 (18.8) | 0 (0–0) | 0.999 | ||
| Infection Clavien–Dindo ((0/I/II)/(III/IV/V) (%); ref = 0/I/II) | 96 (70.1)/40 (29.2) | 22 (88.0)/3 (12.0) | 0.327 (0.093–1.155) | 0.083 | 0.894 (0.096–8.339) | 0.921 |
| RFS | OS | |||||||
|---|---|---|---|---|---|---|---|---|
| Univariable | Multivariable | Univariable | Multivariable | |||||
| Variables | HR (95%Cl) | p | HR (95%Cl) | p | HR (95%Cl) | p | HR (95%CI) | p |
| Sex (male = 1) | 1.034 (0.688–1.554) | 0.871 | 0.730 (0.502–1.602) | 0.100 | ||||
| Age, years (≤65 = 1) | 0.769 (0.510–1.159) | 0.209 | 1.544 (1.061–2.247) | 0.023 | 1.564 (0.894–2.736) | 0.117 | ||
| ASA (I/II = 1) | 1.131 (0.753–1.699) | 0.554 | 0.730 (0.502–1.602) | 0.100 | ||||
| Cholangitis (no = 1) | 0.266 (0.065–1.085) | 0.065 | 0.238 (0.057–1.044) | 0.049 | 1.544 (1.061–2.247) | 0.023 | 1.077 (0.414–2.804) | 0.879 |
| PVE (no = 1) | 1.496 (0.750–2.987) | 0.253 | 1.714 (0.937–3.135) | 0.080 | 1.878 (0.746–4.727) | 0.181 | ||
| Neoadjuvant therapy (no = 1) | 2.271 (1.270–4.061) | 0.006 | 3.607 (1.758–7.402) | <0.001 | 1.907 (1.112–3.270) | 0.019 | 1.771 (0.554–5.659) | 0.575 |
| AST, U/L (≤40 = 1) | 1.264 (0.829–1.927) | 0.277 | 1.108 (0.751–1.633) | 0.606 | ||||
| ALT, U/L (≤40 = 1) | 1.186 (0.743–1.892) | 0.474 | 1.090 (0.705–1.685) | 0.697 | ||||
| AP, U/L (≤100 = 1) | 1.829 (1.177–2.842) | 0.007 | 1.218 (0.652–2.278) | 0.536 | 1.958 (1.276–3.005) | 0.002 | 1.193 (0.589–2.416) | 0.624 |
| CRP, mg/L (≤8.2 = 1) | 2.319 (1.513–3.555) | <0.001 | 2.190 (1.232–3.894) | 0.008 | 2.308 (1.379–3.012) | <0.001 | 1.747 (0.815–3.746) | 0.152 |
| GGT, U/L (≤100 = 1) | 1.751 (1.155–2.654) | 0.008 | 1.124 (0.620–2.039) | 0.700 | 1.691 (1.147–2.493) | 0.008 | 1.189 (0.612–2.308) | 0.610 |
| Hemoglobin, g/dL (≤13 = 1) | 0.637 (0.423–0.960) | 0.031 | 0.901 (0.515–1.576) | 0.715 | 0.595 (0.409–0.868) | 0.007 | 0.410 (0.243–0.693) | 0.001 |
| INR (≤1 = 1) | 1.497 (0.990–2.265) | 0.056 | 1.603 (0.970–2.648) | 0.065 | 1.380 (0.946–2.013) | 0.095 | 1.030 (0.573–1.851) | 0.921 |
| Platelet count, L/nL (≤300 = 1) | 1.499 (0.965–2.330) | 0.072 | 1.008 (0.587–1.731) | 0.977 | 0.901 (0.591–1.374) | 0.629 | ||
| Prothrombin time (≤110 = 1) | 0.761 (0.448–1.292) | 0.312 | 0.643 (0.386–1.070) | 0.089 | 0.804 (0.348–1.855) | 0.609 | ||
| Bilirubin, mg/dL (≤1 = 1) | 0.789 (0.420–1.483) | 0.462 | 1.229 (0.740–2.041) | 0.425 | ||||
| Intraoperative PRBC (No = 1) | 1.906 (1.235–2.942) | 0.004 | 1.379 (0.756–2.515) | 0.295 | 2.001 (1.366–2.930) | <0.001 | 0.726 (0.307–1.714) | 0.465 |
| Intraoperative FFP (No = 1) | 1.687 (1.104–2.578) | 0.016 | 1.274 (0.785–2.066) | 0.327 | 1.986 (1.365–2.890) | <0.001 | 2.546 (1.449–4.473) | 0.001 |
| Operative time, min (≤360 = 1) | 1.562 (0.993–2.459) | 0.054 | 1.028 (0.574–1.839) | 0.926 | 1.988 (1.324–2.986) | 0.001 | 1.680 (0.883–3.199) | 0.114 |
| Time to surgery, days (≤30 = 1) | 0.704 (0.451–1.097) | 0.120 | 1.022 (0.698–1.497) | 0.911 | ||||
| LVI (no = 1) | 2.600 (1.569–4.309) | <0.001 | 2.399 (1.316–4.373) | 0.004 | 3.416 (2.208–5.285) | <0.001 | 3.920 (2.197–6.992) | < 0.001 |
| MVI (no = 1) | 1.027 (0.956–1.103) | 0.470 | 1.038 (1.016–1.061) | 0.001 | 1.034 (1.006–1.062) | 0.015 | ||
| R1 resection (R0/Rx = 1) | 1.992 (1.045–3.764) | 0.036 | 1.290 (0.524–3.174) | 0.579 | 1.768 (0.984–3.176) | 0.056 | 1.290 (0.455–3.659) | 0.632 |
| pT category (T1/T2 = 1) | 1.341 (0.836–2.152) | 0.224 | 1.674 (1.099–2.550) | 0.016 | 1.291 (0.684–2.435) | 0.431 | ||
| pN category (N0 = 1) | 2.871 (1.828–4.511) | <0.001 | 1.525 (0.809–2.878) | 0.192 | 3.320 (2.198–5.015) | <0.001 | 1.195 (0.487–2.934) | 0.697 |
| Tumor grading (G1/G2 = 1) | 1.441 (0.895–2.318) | 0.133 | 2.118 (1.389–3.230) | <0.001 | 2.138 (1.272–3.594) | 0.004 | ||
| ICU time, days (≤1 = 1) | 1.122 (0.669–1.879) | 0.663 | 1.579 (1.013–2.459) | 0.044 | 1.052 (0.502–2.203) | 0.894 | ||
| Hospitalization, days (≤14 = 1) | 1.023 (2.308–) | 0.038 | 1.036 (0.541–1.985) | 0.915 | 1.567 (1.079–2.277) | 0.018 | 1.024 (0.520–2.019) | 0.944 |
| Perioperative complications (Clavien–Dindo 0/I/II = 1) | 1.7533 (1.159–2.653) | 0.008 | 1.631 (0.900–2.957) | 0.107 | 2.230 (1.532–3.247) | <0.001 | 3.776 (1.617–8.817) | 0.002 |
| Liver failure (no = 1) | 1.597 (0.902–2.830) | 0.108 | 1.815 (1.153–2.858) | 0.010 | 1.144 (0.611–2.142) | 0.674 | ||
| Bile leak (no = 1) | 1.377 (0.811–2.338) | 0.236 | 1.809 (1.135–2.883) | 0.013 | 1.082 (0.483–2.420) | 0.849 | ||
| Hemorrhage (No = 1) | 0.928 (0.377–2.286) | 0.871 | 2.304 (1.055–3.919) | 0.034 | 1.850 (0.668–5.122) | 0.236 | ||
| Infection complications (Clavien–Dindo 0/I/II = 1) | 2.256 (1.421–3.580) | 0.001 | 1.658 (0.955–2.878) | 0.073 | 2.438 (1.624–3.660) | <0.001 | 1.545 (0.655–3.641) | 0.320 |
| Adjuvant therapy (no = 1) | 1.145 (0.759–1.728) | 0.518 | 0.620 (0.406–0.948) | 0.010 | 0.273 (0.149–0.500) | <0.001 | ||
| BMI, kg/m2 (≤25 = 1) | 0.855 (0.571–1.282) | 0.450 | 0.913 (0.629–1.326) | 0.632 | ||||
| Visceral_fat area (≤100 = 1) | 0.731 (0.487–1.098) | 0.131 | 1.067 (0.726–1.568) | 0.741 | ||||
| Sarcopenia (no = 1) | 0.890 (0.587–1.349) | 0.586 | 1.509 (1.027–2.217) | 0.036 | 1.293 (0.640–2.613) | 0.474 | ||
| Myosteatosis (no = 1) | 0.829 (0.553–1.245) | 0.367 | 1.200 (0.817–1.762) | 0.352 | ||||
| Sarcopenic_obesity (no = 1) | 0.932 (0.528–1.646) | 0.808 | 1.267 (0.742–2.165) | 0.386 | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wang, G.; Otto, C.C.; Heij, L.R.; Al-Masri, T.M.; Dahl, E.; Heise, D.; Olde Damink, S.W.M.; Luedde, T.; Lang, S.A.; Ulmer, T.F.; et al. Impact of Altered Body Composition on Clinical and Oncological Outcomes in Intrahepatic Cholangiocarcinoma. J. Clin. Med. 2023, 12, 7747. https://doi.org/10.3390/jcm12247747
Wang G, Otto CC, Heij LR, Al-Masri TM, Dahl E, Heise D, Olde Damink SWM, Luedde T, Lang SA, Ulmer TF, et al. Impact of Altered Body Composition on Clinical and Oncological Outcomes in Intrahepatic Cholangiocarcinoma. Journal of Clinical Medicine. 2023; 12(24):7747. https://doi.org/10.3390/jcm12247747
Chicago/Turabian StyleWang, Guanwu, Carlos C. Otto, Lara R. Heij, Tarick M. Al-Masri, Edgar Dahl, Daniel Heise, Steven W. M. Olde Damink, Tom Luedde, Sven A. Lang, Tom F. Ulmer, and et al. 2023. "Impact of Altered Body Composition on Clinical and Oncological Outcomes in Intrahepatic Cholangiocarcinoma" Journal of Clinical Medicine 12, no. 24: 7747. https://doi.org/10.3390/jcm12247747
APA StyleWang, G., Otto, C. C., Heij, L. R., Al-Masri, T. M., Dahl, E., Heise, D., Olde Damink, S. W. M., Luedde, T., Lang, S. A., Ulmer, T. F., Neumann, U. P., & Bednarsch, J. (2023). Impact of Altered Body Composition on Clinical and Oncological Outcomes in Intrahepatic Cholangiocarcinoma. Journal of Clinical Medicine, 12(24), 7747. https://doi.org/10.3390/jcm12247747