
Impact on Endovascular Thrombectomy for Acute Ischemic Stroke of Aortic Arch Calcification on Chest X-ray

 , ,
, ,
Abstract
:1. Introduction
2. Materials and Methods
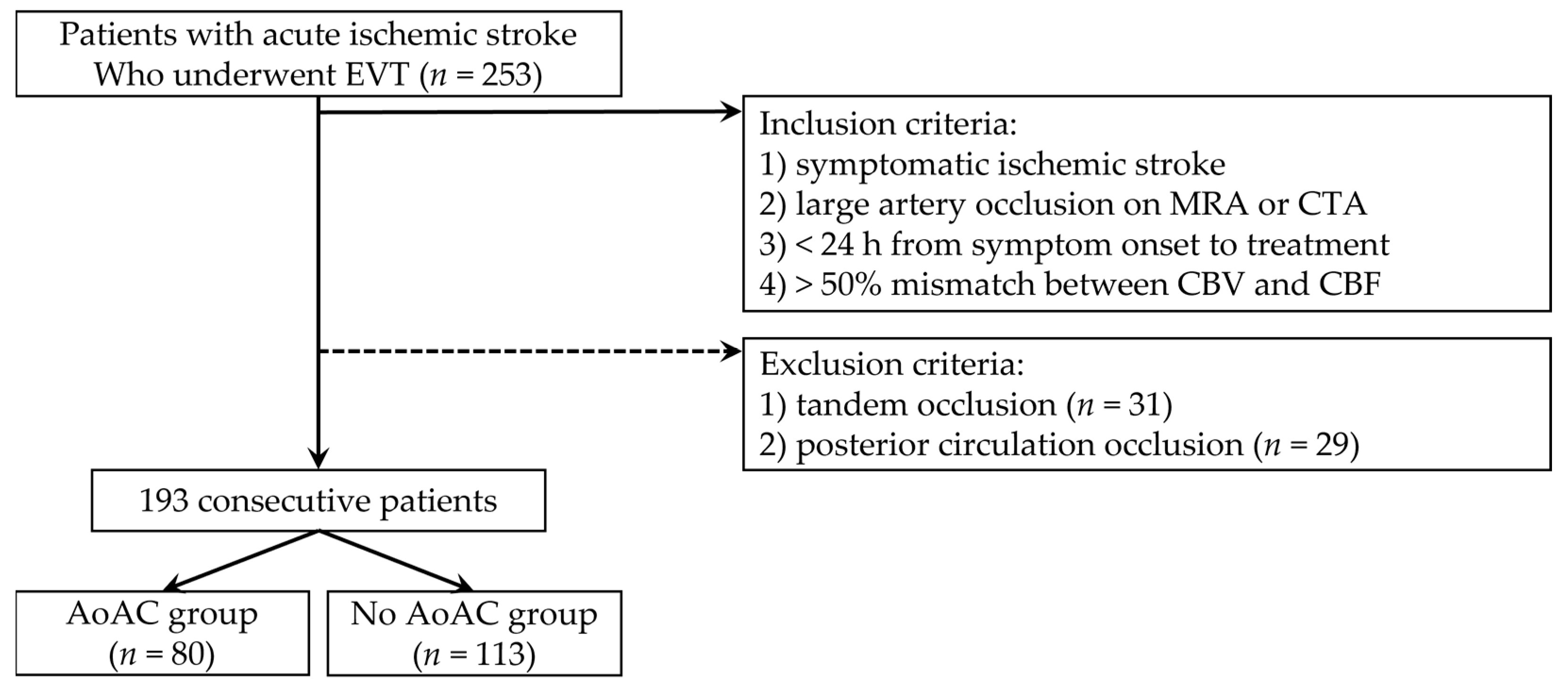
2.1. Study Population
2.2. Data Collection
2.3. EVT for AIS
2.4. Statistical Analysis
3. Results
4. Discussion
Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Berkhemer, O.A.; Fransen, P.S.; Beumer, D.; van den Berg, L.A.; Lingsma, H.F.; Yoo, A.J.; Schonewille, W.J.; Vos, J.A.; Nederkoorn, P.J.; Wermer, M.J.; et al. A randomized trial of intraarterial treatment for acute ischemic stroke. N. Engl. J. Med. 2015, 372, 11–20. [Google Scholar] [CrossRef] [PubMed]
- Campbell, B.C.; Mitchell, P.J.; Kleinig, T.J.; Dewey, H.M.; Churilov, L.; Yassi, N.; Yan, B.; Dowling, R.J.; Parsons, M.W.; Oxley, T.J.; et al. Endovascular therapy for ischemic stroke with perfusion-imaging selection. N. Engl. J. Med. 2015, 372, 1009–1018. [Google Scholar] [CrossRef] [PubMed]
- Goyal, M.; Demchuk, A.M.; Menon, B.K.; Eesa, M.; Rempel, J.L.; Thornton, J.; Roy, D.; Jovin, T.G.; Willinsky, R.A.; Sapkota, B.L.; et al. Randomized assessment of rapid endovascular treatment of ischemic stroke. N. Engl. J. Med. 2015, 372, 1019–1030. [Google Scholar] [CrossRef] [PubMed]
- Jovin, T.G.; Chamorro, A.; Cobo, E.; de Miquel, M.A.; Molina, C.A.; Rovira, A.; San Román, L.; Serena, J.; Abilleira, S.; Ribó, M.; et al. Thrombectomy within 8 hours after symptom onset in ischemic stroke. N. Engl. J. Med. 2015, 372, 2296–2306. [Google Scholar] [CrossRef] [PubMed]
- Saver, J.L.; Goyal, M.; Bonafe, A.; Diener, H.C.; Levy, E.I.; Pereira, V.M.; Albers, G.W.; Cognard, C.; Cohen, D.J.; Hacke, W.; et al. Stent-retriever thrombectomy after intravenous t-PA vs. t-PA alone in stroke. N. Engl. J. Med. 2015, 372, 2285–2295. [Google Scholar] [CrossRef] [PubMed]
- Anadani, M.; Alawieh, A.; Vargas, J.; Chatterjee, A.R.; Turk, A.; Spiotta, A. First attempt recanalization with ADAPT: Rate, predictors, and outcome. J. Neurointerv. Surg. 2019, 11, 641–645. [Google Scholar] [CrossRef]
- LeCouffe, N.E.; Kappelhof, M.; Treurniet, K.M.; Lingsma, H.F.; Zhang, G.; van den Wijngaard, I.R.; van Es, A.; Emmer, B.J.; Majoie, C.; Roos, Y.; et al. 2B, 2C, or 3: What Should Be the Angiographic Target for Endovascular Treatment in Ischemic Stroke? Stroke 2020, 51, 1790–1796. [Google Scholar] [CrossRef]
- Kim, S.H.; Lee, H.; Kim, S.B.; Kim, S.T.; Baek, J.W.; Heo, Y.J.; Jeong, H.W.; Kim, H.J.; Park, J.H.; Kim, J.S.; et al. Hybrid mechanical thrombectomy for acute ischemic stroke using an intermediate aspiration catheter and Trevo stent simultaneously. J. Clin. Neurosci. 2020, 76, 9–14. [Google Scholar] [CrossRef]
- Maus, V.; Henkel, S.; Riabikin, A.; Riedel, C.; Behme, D.; Tsogkas, I.; Hesse, A.C.; Abdullayev, N.; Jansen, O.; Wiesmann, M.; et al. The SAVE Technique: Large-Scale Experience for Treatment of Intracranial Large Vessel Occlusions. Clin. Neuroradiol. 2019, 29, 669–676. [Google Scholar] [CrossRef]
- Baek, J.H.; Kim, B.M.; Heo, J.H.; Nam, H.S.; Kim, Y.D.; Park, H.; Bang, O.Y.; Yoo, J.; Kim, D.J.; Jeon, P.; et al. Number of Stent Retriever Passes Associated with Futile Recanalization in Acute Stroke. Stroke 2018, 49, 2088–2095. [Google Scholar] [CrossRef]
- Flottmann, F.; Brekenfeld, C.; Broocks, G.; Leischner, H.; McDonough, R.; Faizy, T.D.; Deb-Chatterji, M.; Alegiani, A.; Thomalla, G.; Mpotsaris, A.; et al. Good Clinical Outcome Decreases With Number of Retrieval Attempts in Stroke Thrombectomy: Beyond the First-Pass Effect. Stroke 2021, 52, 482–490. [Google Scholar] [CrossRef] [PubMed]
- Flottmann, F.; Leischner, H.; Broocks, G.; Nawabi, J.; Bernhardt, M.; Faizy, T.D.; Deb-Chatterji, M.; Thomalla, G.; Fiehler, J.; Brekenfeld, C. Recanalization Rate per Retrieval Attempt in Mechanical Thrombectomy for Acute Ischemic Stroke. Stroke 2018, 49, 2523–2525. [Google Scholar] [CrossRef]
- Jindal, G.; Carvalho, H.P.; Wessell, A.; Le, E.; Naragum, V.; Miller, T.R.; Wozniak, M.; Shivashankar, R.; Cronin, C.A.; Schrier, C.; et al. Beyond the first pass: Revascularization remains critical in stroke thrombectomy. J. Neurointerv. Surg. 2019, 11, 1095–1099. [Google Scholar] [CrossRef]
- Maros, M.E.; Brekenfeld, C.; Broocks, G.; Leischner, H.; McDonough, R.; Deb-Chatterji, M.; Alegiani, A.; Thomalla, G.; Fiehler, J.; Flottmann, F. Number of Retrieval Attempts Rather Than Procedure Time Is Associated With Risk of Symptomatic Intracranial Hemorrhage. Stroke 2021, 52, 1580–1588. [Google Scholar] [CrossRef] [PubMed]
- Zaidat, O.O.; Castonguay, A.C.; Linfante, I.; Gupta, R.; Martin, C.O.; Holloway, W.E.; Mueller-Kronast, N.; English, J.D.; Dabus, G.; Malisch, T.W.; et al. First Pass Effect: A New Measure for Stroke Thrombectomy Devices. Stroke 2018, 49, 660–666. [Google Scholar] [CrossRef] [PubMed]
- Bourcier, R.; Saleme, S.; Labreuche, J.; Mazighi, M.; Fahed, R.; Blanc, R.; Gory, B.; Kyheng, M.; Marnat, G.; Bracard, S.; et al. More than three passes of stent retriever is an independent predictor of parenchymal hematoma in acute ischemic stroke. J. Neurointerv. Surg. 2019, 11, 625–629. [Google Scholar] [CrossRef]
- Kim, B.M. Causes and Solutions of Endovascular Treatment Failure. J. Stroke 2017, 19, 131–142. [Google Scholar] [CrossRef]
- Koge, J.; Tanaka, K.; Yoshimoto, T.; Shiozawa, M.; Kushi, Y.; Ohta, T.; Satow, T.; Kataoka, H.; Ihara, M.; Koga, M.; et al. Internal Carotid Artery Tortuosity: Impact on Mechanical Thrombectomy. Stroke 2022, 53, 2458–2467. [Google Scholar] [CrossRef]
- Leischner, H.; Flottmann, F.; Hanning, U.; Broocks, G.; Faizy, T.D.; Deb-Chatterji, M.; Bernhardt, M.; Brekenfeld, C.; Buhk, J.H.; Gellissen, S.; et al. Reasons for failed endovascular recanalization attempts in stroke patients. J. Neurointerv. Surg. 2019, 11, 439–442. [Google Scholar] [CrossRef]
- Kim, H.G.; Lee, S.H.; Nam, T.M.; Jang, J.H.; Kim, Y.Z.; Kim, K.H.; Kim, D.H.; Kim, S.H. Association of Aortic Arch Calcification on Chest X-ray with Procedural Thromboembolism after Mechanical Thrombectomy for Acute Ischemic Stroke. Medicina 2021, 57, 859. [Google Scholar] [CrossRef]
- Kim, S.H.; Nam, T.M.; Lee, S.H.; Jang, J.H.; Kim, Y.Z.; Kim, K.H.; Kim, D.H.; Lee, C.H. Association of aortic arch calcification on chest X-ray with procedural thromboembolism after coil embolization of cerebral aneurysm. J. Clin. Neurosci. 2022, 99, 373–378. [Google Scholar] [CrossRef] [PubMed]
- Woo, J.S.; Kim, W.; Kwon, S.H.; Youn, H.C.; Kim, H.S.; Kim, J.B.; Kim, S.J.; Kim, W.S.; Kim, K.S. Aortic arch calcification on chest X-ray combined with coronary calcium score show additional benefit for diagnosis and outcome in patients with angina. J. Geriatr. Cardiol. 2016, 13, 218–225. [Google Scholar] [CrossRef] [PubMed]
- Kotelis, D.; Bischoff, M.S.; Jobst, B.; von Tengg-Kobligk, H.; Hinz, U.; Geisbüsch, P.; Böckler, D. Morphological risk factors of stroke during thoracic endovascular aortic repair. Langenbecks Arch. Surg. 2012, 397, 1267–1273. [Google Scholar] [CrossRef] [PubMed]
- Ritz, K.; Denswil, N.P.; Stam, O.C.; van Lieshout, J.J.; Daemen, M.J. Cause and mechanisms of intracranial atherosclerosis. Circulation 2014, 130, 1407–1414. [Google Scholar] [CrossRef] [PubMed]
- Landis, J.R.; Koch, G.G. The measurement of observer agreement for categorical data. Biometrics 1977, 33, 159–174. [Google Scholar] [CrossRef]
- Alkan, O.; Kizilkilic, O.; Yildirim, T.; Atalay, H. Intracranial cerebral artery stenosis with associated coronary artery and extracranial carotid artery stenosis in Turkish patients. Eur. J. Radiol. 2009, 71, 450–455. [Google Scholar] [CrossRef]
- Powers, W.J.; Rabinstein, A.A.; Ackerson, T.; Adeoye, O.M.; Bambakidis, N.C.; Becker, K.; Biller, J.; Brown, M.; Demaerschalk, B.M.; Hoh, B.; et al. Guidelines for the Early Management of Patients With Acute Ischemic Stroke: 2019 Update to the 2018 Guidelines for the Early Management of Acute Ischemic Stroke: A Guideline for Healthcare Professionals from the American Heart Association/American Stroke Association. Stroke 2019, 50, e344–e418. [Google Scholar] [CrossRef]
- Bayar, N.; Erkal, Z.; Köklü, E.; Güven, R.; Arslan, Ş. Increased Intima-Media Thickness of the Ascending Aorta May Predict Neurological Complications Associated with TAVI. J. Stroke Cerebrovasc. Dis. 2021, 30, 105665. [Google Scholar] [CrossRef]
- Melissano, G.; Tshomba, Y.; Bertoglio, L.; Rinaldi, E.; Chiesa, R. Analysis of stroke after TEVAR involving the aortic arch. Eur. J. Vasc. Endovasc. Surg. 2012, 43, 269–275. [Google Scholar] [CrossRef]
- Lee, D.H.; Kim, S.H.; Lee, H.; Kim, S.B.; Lee, D.; Heo, Y.J.; Baek, J.W.; Kim, H.J.; Kim, J.S.; Park, J.H.; et al. Thrombectomy in acute vertebrobasilar occlusion: A single-centre experience. Neuroradiology 2020, 62, 723–731. [Google Scholar] [CrossRef]
- Park, H.; Baek, J.H.; Kim, B.M. Endovascular Treatment of Acute Stroke Due to Intracranial Atherosclerotic Stenosis-Related Large Vessel Occlusion. Front. Neurol. 2019, 10, 308. [Google Scholar] [CrossRef] [PubMed]
- Tsang, A.C.O.; Orru, E.; Klostranec, J.M.; Yang, I.H.; Lau, K.K.; Tsang, F.C.P.; Lui, W.M.; Pereira, V.M.; Krings, T. Thrombectomy Outcomes of Intracranial Atherosclerosis-Related Occlusions. Stroke 2019, 50, 1460–1466. [Google Scholar] [CrossRef] [PubMed]
- Di Maria, F.; Kyheng, M.; Consoli, A.; Desilles, J.P.; Gory, B.; Richard, S.; Rodesch, G.; Labreuche, J.; Girot, J.B.; Dargazanli, C.; et al. Identifying the predictors of first-pass effect and its influence on clinical outcome in the setting of endovascular thrombectomy for acute ischemic stroke: Results from a multicentric prospective registry. Int. J. Stroke 2021, 16, 20–28. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Zhang, T.; Xu, Y.; Xu, X.; Xu, J.; Yang, K.; Yuan, L.; Yang, Q.; Huang, X.; Zhou, Z. Predictors of First-Pass Effect in Endovascular Thrombectomy with Stent-Retriever Devices for Acute Large Vessel Occlusion Stroke. Front. Neurol. 2022, 13, 664140. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| Aortic Arch Calcification | p-Value | |||
|---|---|---|---|---|
| Present (n = 80) | Absent (n = 113) | |||
| Baseline characteristics | Age (years) * | 74.5 ± 7.78 | 63.9 ± 12.4 | <0.001 |
| Sex, male (%) | 41 (51.2) | 71 (62.8) | 0.139 | |
| Hypertension (%) | 52 (65.0) | 43 (38.1) | <0.001 | |
| Diabetes mellitus (%) | 17 (21.3) | 20 (17.7) | 0.580 | |
| Atrial fibrillation (%) | 45 (56.3) | 39 (34.5) | 0.003 | |
| Occlusion side, left (%) | 40 (50.0) | 48 (42.5) | 0.309 | |
| Occlusion site | 0.198 | |||
| ICA | 21 | 20 | ||
| M1 | 49 | 70 | ||
| M2 | 10 | 23 | ||
| Etiology | 0.267 | |||
| Atherosclerotic | 12 | 25 | ||
| Non-atherosclerotic | 68 | 88 | ||
| Type of aortic arch | <0.001 | |||
| Type I or Type II | 46 | 99 | ||
| Type III | 34 | 14 | ||
| Intracranial atherosclerotic stenosis (%) | 21 (26.3) | 28 (24.8%) | 0.867 | |
| NIHSS at admission * | 12.8 ± 5.79 | 11.4 ± 6.13 | 0.104 | |
| Onset-to-door time in min * | 176.1 ± 186.1 | 209.8 ± 222.9 | 0.270 | |
| Onset-to-puncture time in min * | 323.9 ± 209.3 | 352.8 ± 231.4 | 0.375 | |
| Treatment characteristics | Intravenous thrombolysis (%) | 33 (41.3) | 45 (39.8) | 0.882 |
| Balloon guide catheter (%) | 14 (17.5) | 20 (17.7) | 1.000 | |
| Technique | 0.122 | |||
| Combination | 56 | 91 | ||
| Non-combination | 24 | 22 | ||
| Total number of EVT attempts * | 3.04 ± 1.95 | 2.01 ± 1.34 | <0.001 | |
| Procedural time in min * | 71.7 ± 31.2 | 48.7 ± 23.1 | <0.001 | |
| Radiological and clinical outcomes | Successful recanalization (%) | 60 (75.0) | 102 (90.3) | 0.005 |
| First-pass successful recanalization (%) | 15 (18.8) | 54 (47.8) | <0.001 | |
| Postprocedural hemorrhage (%) | 36 (45.0) | 31 (27.7) | 0.015 | |
| Subarachnoid hemorrhage (%) | 14 (17.5) | 13 (11.5) | 0.293 | |
| Intracerebral hematoma (%) | 22 (27.5) | 17 (15.0) | 0.045 | |
| Good clinical outcome (%) | 37 (46.3) | 73 (64.6) | 0.013 | |
| Factors | Adjusted OR | Adjusted 95% CI | p-Value |
|---|---|---|---|
| Age | 1.106 | 1.063–1.151 | <0.001 |
| Hypertension | 2.044 | 1.049–3.981 | 0.036 |
| First-Pass Successful Recanalization | p-Value | |||
|---|---|---|---|---|
| Yes (n = 69) | No (n = 124) | |||
| Baseline characteristics | Age (years) * | 67.7 ± 12.7 | 68.6 ± 11.5 | 0.591 |
| Sex, male (%) | 46 (66.7) | 66 (53.2) | 0.094 | |
| Hypertension (%) | 29 (42.0) | 66 (53.2) | 0.176 | |
| Diabetes mellitus (%) | 11 (15.9) | 26 (21.0) | 0.449 | |
| Atrial fibrillation (%) | 29 (42.0) | 55 (44.4) | 0.765 | |
| Occlusion side, left (%) | 35 (50.7) | 53 (42.7) | 0.296 | |
| Occlusion site | 0.032 | |||
| ICA | 8 | 33 | ||
| M1 | 50 | 69 | ||
| M2 | 11 | 22 | ||
| Etiology | 0.449 | |||
| Atherosclerotic | 11 | 26 | ||
| Non-atherosclerotic | 58 | 98 | ||
| Aortic arch calcification (%) | 15 (21.7) | 65 (52.4) | <0.001 | |
| Type of aortic arch | 0.862 | |||
| Type I or Type II | 51 | 94 | ||
| Type III | 18 | 30 | ||
| Intracranial atherosclerotic stenosis (%) | 16 (23.2) | 33 (26.6%) | 0.730 | |
| NIHSS at admission * | 11.8 ± 5.57 | 12.1 ± 6.28 | 0.800 | |
| Onset-to-door time in min * | 190.7 ± 192.7 | 198.7 ± 217.6 | 0.800 | |
| Onset-to-puncture time in min * | 328.5 ± 215.4 | 347.6 ± 226.8 | 0.569 | |
| Treatment characteristics | Intravenous thrombolysis (%) | 35 (50.7) | 43 (34.7) | 0.033 |
| Balloon guide catheter (%) | 15 (21.7) | 19 (15.3) | 0.324 | |
| Technique | 0.725 | |||
| Combination | 54 | 93 | ||
| Non-combination | 15 | 31 | ||
| Procedural time in min * | 37.0 ± 16.7 | 70.0 ± 27.7 | <0.001 | |
| Radiological and clinical outcomes | Postprocedural hemorrhage (%) | 11 (15.9) | 56 (45.5) | <0.001 |
| Subarachnoid hemorrhage (%) | 4 (5.8) | 23 (18.5) | 0.016 | |
| Intracerebral hematoma (%) | 7 (10.1) | 32 (25.8) | 0.009 | |
| Good clinical outcome (%) | 53 (76.8) | 57 (46.0) | <0.001 | |
| Factors | Adjusted OR | Adjusted 95% CI | p-Value |
|---|---|---|---|
| AoAC | 0.239 | 0.121–0.475 | <0.001 |
| Intravenous thrombolysis | 2.126 | 1.126–4.014 | 0.020 |
| Good Clinical Outcomes | p-Value | |||
|---|---|---|---|---|
| Yes (n = 110) | No (n = 83) | |||
| Baseline characteristics | Age (years) * | 66.2 ± 12.6 | 71.1 ± 10.4 | 0.003 |
| Sex, male (%) | 69 (62.7) | 43 (51.8) | 0.142 | |
| Hypertension (%) | 47 (42.7) | 48 (57.8) | 0.043 | |
| Diabetes mellitus (%) | 16 (14.5) | 21 (25.3) | 0.067 | |
| Atrial fibrillation (%) | 43 (39.1) | 41 (49.4) | 0.187 | |
| Occlusion side, left (%) | 42 (38.2) | 46 (55.4) | 0.020 | |
| Occlusion site | 0.020 | |||
| ICA | 16 | 25 | ||
| M1 | 71 | 48 | ||
| M2 | 23 | 10 | ||
| Etiology | 1.000 | |||
| Atherosclerotic | 21 | 16 | ||
| Non-atherosclerotic | 89 | 67 | ||
| Aortic arch calcification (%) | 37 (33.6) | 43 (51.3) | 0.013 | |
| Type of aortic arch | 0.179 | |||
| Type I or Type II | 87 | 58 | ||
| Type III | 23 | 25 | ||
| Intracranial atherosclerotic stenosis (%) | 30 (27.3) | 19 (22.9%) | 0.509 | |
| NIHSS at admission * | 11.8 ± 5.57 | 12.1 ± 6.28 | 0.800 | |
| Onset-to-door time in min * | 201.5 ± 212.8 | 188.3 ± 203.9 | 0.662 | |
| Onset-to-puncture time in min * | 348.4 ± 230.7 | 330.7 ± 211.9 | 0.582 | |
| Treatment characteristics | Intravenous thrombolysis (%) | 50 (45.5) | 28 (33.7) | 0.106 |
| Balloon guide catheter (%) | 21 (19.1) | 13 (15.7) | 0.572 | |
| Technique | 1.000 | |||
| Combination | 84 | 63 | ||
| Non-combination | 20 | 26 | ||
| Total number of EVT attempts * | 2.14 ± 1.47 | 2.83 ± 1.89 | 0.006 | |
| Procedural time in min * | 51.8 ± 24.5 | 66.7 ± 32.3 | <0.001 | |
| Radiological and clinical outcomes | Successful recanalization (%) | 103 (93.6) | 59 (71.1) | <0.001 |
| First-pass successful recanalization (%) | 53 (48.2) | 16 (19.3) | <0.001 | |
| Postprocedural hemorrhage (%) | 26 (23.9) | 41 (49.4) | <0.001 | |
| Subarachnoid hemorrhage (%) | 13 (11.8) | 14 (16.9) | 0.402 | |
| Intracerebral hematoma (%) | 13 (11.8) | 26 (31.3) | 0.001 | |
| Factors | Adjusted OR | Adjusted 95% CI | p-Value |
|---|---|---|---|
| Age | 0.975 | 0.947–1.005 | 0.105 |
| Occlusion side, left | 0.381 | 0.193–0.754 | 0.006 |
| First-pass successful recanalization | 2.827 | 1.329–6.018 | 0.007 |
| Successful recanalization | 4.088 | 1.465–11.403 | 0.007 |
| Intracerebral hematoma | 0.344 | 0.150–0.791 | 0.012 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Jeong, H.Y.; Nam, T.M.; Lee, S.H.; Jang, J.H.; Kim, Y.Z.; Kim, K.H.; Ryu, K.H.; Kim, D.-H.; Kwan, B.S.; Bak, H.; et al. Impact on Endovascular Thrombectomy for Acute Ischemic Stroke of Aortic Arch Calcification on Chest X-ray. J. Clin. Med. 2023, 12, 6115. https://doi.org/10.3390/jcm12196115
Jeong HY, Nam TM, Lee SH, Jang JH, Kim YZ, Kim KH, Ryu KH, Kim D-H, Kwan BS, Bak H, et al. Impact on Endovascular Thrombectomy for Acute Ischemic Stroke of Aortic Arch Calcification on Chest X-ray. Journal of Clinical Medicine. 2023; 12(19):6115. https://doi.org/10.3390/jcm12196115
Chicago/Turabian StyleJeong, Hyeon Yeong, Taek Min Nam, Sang Hyuk Lee, Ji Hwan Jang, Young Zoon Kim, Kyu Hong Kim, Kyeong Hwa Ryu, Do-Hyung Kim, Byung Soo Kwan, Hyerang Bak, and et al. 2023. "Impact on Endovascular Thrombectomy for Acute Ischemic Stroke of Aortic Arch Calcification on Chest X-ray" Journal of Clinical Medicine 12, no. 19: 6115. https://doi.org/10.3390/jcm12196115
APA StyleJeong, H. Y., Nam, T. M., Lee, S. H., Jang, J. H., Kim, Y. Z., Kim, K. H., Ryu, K. H., Kim, D.-H., Kwan, B. S., Bak, H., & Kim, S. H. (2023). Impact on Endovascular Thrombectomy for Acute Ischemic Stroke of Aortic Arch Calcification on Chest X-ray. Journal of Clinical Medicine, 12(19), 6115. https://doi.org/10.3390/jcm12196115