
“Under the Bridge”: Looking for Ischemia in a Patient with Intramyocardial Coronary Artery Course—The Role of the Cardiopulmonary Exercise Test

 , , ,
, , ,
Abstract
:1. Introduction
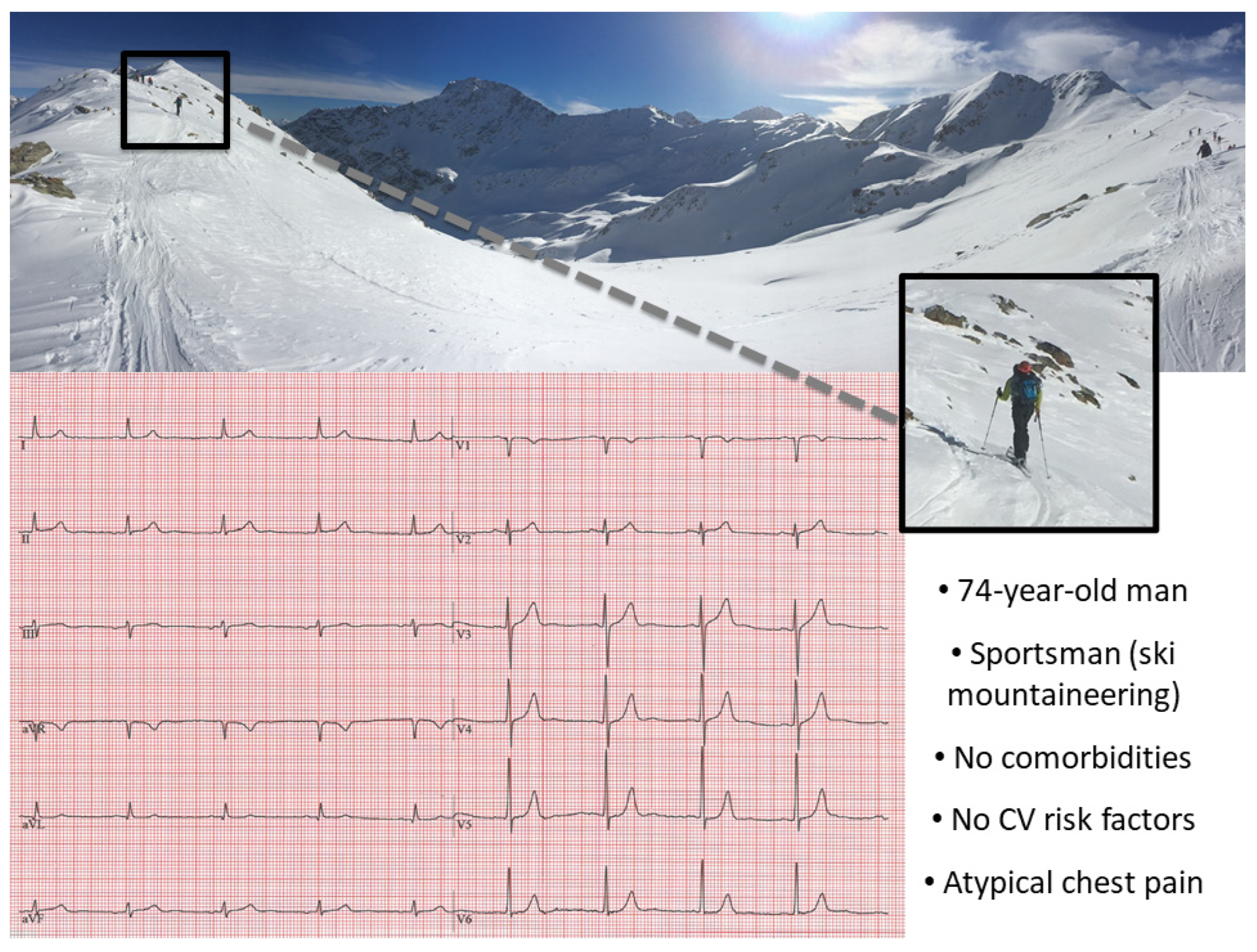
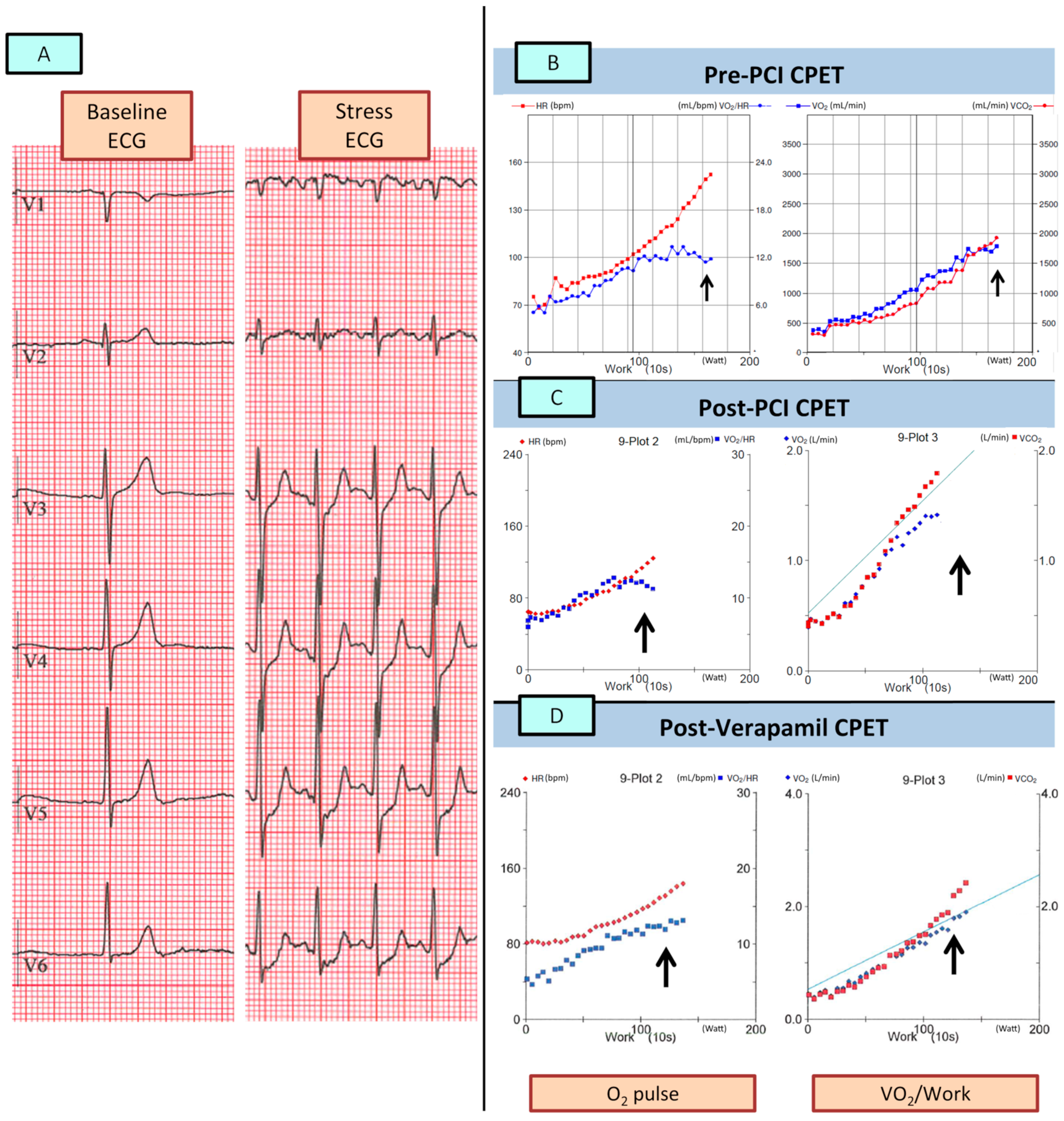
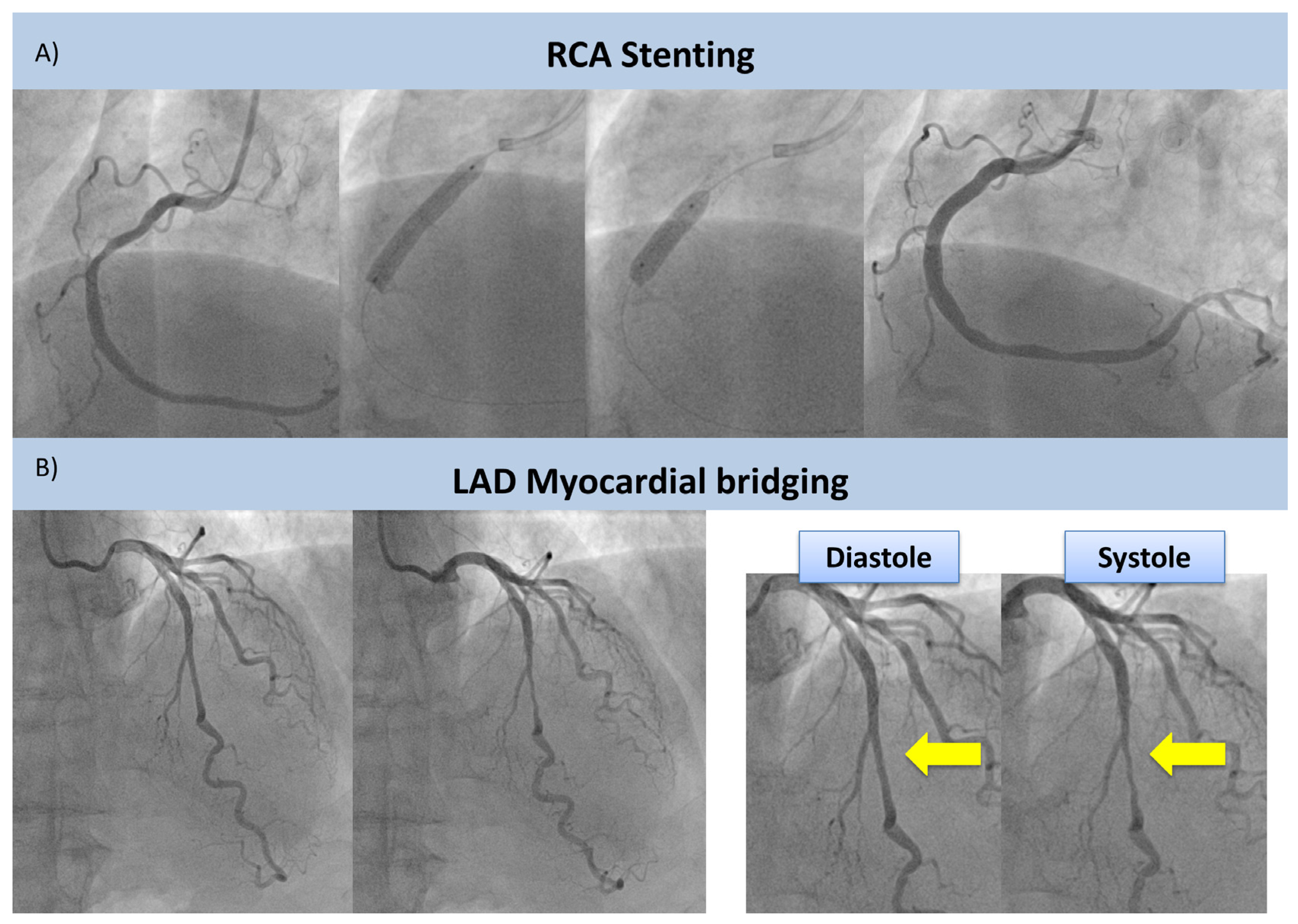
2. Case Description
3. Discussion
4. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Belardinelli, R.; Lacalaprice, F.; Carle, F.; Minnucci, A.; Cianci, G.; Perna, G.; D’Eusanio, G. Exercise-induced myocardial ischaemia detected by cardiopulmonary exercise testing. Eur. Heart J. 2003, 24, 1304–1313. [Google Scholar] [CrossRef] [PubMed]
- Belardinelli, R.; Lacalaprice, F.; Tiano, L.; Muçai, A.; Perna, G.P. Cardiopulmonary exercise testing is more accurate than ECG-stress testing in diagnosing myocardial ischemia in subjects with chest pain. Int. J. Cardiol. 2014, 174, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Stringer, W.W.; Hansen, J.E.; Wasserman, K. Cardiac output estimated noninvasively from oxygen uptake during exercise. J. Appl. Physiol. 1997, 82, 908–912. [Google Scholar] [CrossRef] [PubMed]
- Sullivan, M.J.; Knight, J.D.; Higginbotham, M.B.; Cobb, F.R. Relation between central and peripheral hemodynamics during exercise in patients with chronic heart failure. Muscle blood flow is reduced with maintenance of arterial perfusion pressure. Circulation 1989, 80, 769–781. [Google Scholar] [CrossRef] [PubMed]
- Accalai, E.; Vignati, C.; Salvioni, E.; Pezzuto, B.; Contini, M.; Cadeddu, C.; Meloni, L.; Agostoni, P. Non-invasive estimation of stroke volume during exercise from oxygen in heart failure patients. Eur. J. Prev. Cardiol. 2021, 28, 280–286. [Google Scholar] [CrossRef] [PubMed]
- Bhambhani, Y.; Norris, S.; Bell, G. Prediction of Stroke Volume from Oxygen Pulse Measurements in Untrained and Trained Men. Can. J. Appl. Physiol. 1994, 19, 49–59. [Google Scholar] [CrossRef] [PubMed]
- Crisafulli, A.; Piras, F.; Chiappori, P.; Vitelli, S.; Caria, M.A.; Lobina, A.; Milia, R.; Tocco, F.; Concu, A.; Melis, F. Estimating stroke volume from oxygen pulse during exercise. Physiol. Meas. 2007, 28, 1201–1212. [Google Scholar] [CrossRef] [PubMed]
- Mapelli, M.; Romani, S.; Magrì, D.; Merlo, M.; Cittar, M.; Masè, M.; Muratori, M.; Gallo, G.; Sclafani, M.; Carriere, C.; et al. Exercise oxygen pulse kinetics in patients with hypertrophic cardiomyopathy. Heart 2022, 108, 1629–1636. [Google Scholar] [CrossRef] [PubMed]
- Bussotti, M.; Apostolo, A.; Andreini, D.; Palermo, P.; Contini, M.; Agostoni, P. Cardiopulmonary evidence of exercise-induced silent ischaemia. Eur. J. Prev. Cardiol. 2006, 13, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Danek, B.A.; Kearney, K.; Steinberg, Z.L. Clinically significant myocardial bridging. Heart, 2023; online ahead of print. [Google Scholar] [CrossRef]
- Patel, A.R.; Salerno, M.; Kwong, R.Y.; Singh, A.; Heydari, B.; Kramer, C.M. Stress Cardiac Magnetic Resonance Myocardial Perfusion Imaging: JACC Review Topic of the Week. J. Am. Coll. Cardiol. 2021, 78, 1655–1668. [Google Scholar] [CrossRef] [PubMed]
- Pargaonkar, V.S.; Kimura, T.; Kameda, R.; Tanaka, S.; Yamada, R.; Schwartz, J.G.; Perl, L.; Rogers, I.S.; Honda, Y.; Fitzgerald, P.; et al. Invasive assessment of myocardial bridging in patients with angina and no obstructive coronary artery disease. EuroIntervention 2021, 16, 1070–1078. [Google Scholar] [CrossRef] [PubMed]
- Tarantini, G.; Barioli, A.; Fovino, L.N.; Fraccaro, C.; Masiero, G.; Iliceto, S.; Napodano, M. Unmasking Myocardial Bridge–Related Ischemia by Intracoronary Functional Evaluation. Circ. Cardiovasc. Interv. 2018, 11, e006247. [Google Scholar] [CrossRef] [PubMed]
- Kelle, S.; Thouet, T.; Tangcharoen, T.; Fleck, E.; Nagel, E. Anatomical and Functional Evaluation of Myocardial Bridging on the Left Anterior Descending Artery by Cardiovascular Magnetic Resonance Imaging. J. Cardiovasc. Magn. Reson. 2006, 8, 755–757. [Google Scholar] [CrossRef] [PubMed]
- Sternheim, D.; Power, D.A.; Samtani, R.; Kini, A.; Fuster, V.; Sharma, S. Myocardial Bridging: Diagnosis, Functional Assessment, and Management: JACC State-of-the-Art Review. J. Am. Coll. Cardiol. 2021, 78, 2196–2212. [Google Scholar] [CrossRef] [PubMed]
- Thomson, V.; Botnar, R.; Croisille, P. Usefulness of MRI to Demonstrate the Mechanisms of Myocardial Ischemia in Hypertrophic Cardiomyopathy with Myocardial Bridge. Cardiology 2006, 107, 159–164. [Google Scholar] [CrossRef] [PubMed]
- Mandapaka, S.; Hundley, W.G. Dobutamine cardiovascular magnetic resonance: A review. J. Magn. Reson. Imaging 2006, 24, 499–512. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Pre-PCI | Post-PCI | Post-Verapamil | |
|---|---|---|---|
| Ramp protocol (Watt/min) | 15 | 15 | 15 |
| VO2 at AT (mL/min) | 1050 | 884 | 1089 |
| HR at AT (bpm) | 102 | 83 | 102 |
| Work rate at AT (watt) | 72 | 60 | 73 |
| Peak VO2 (mL/min) | 1770 | 1431 | 1881 |
| Peak VO2 predicted (%) | 112 | 96 | 127 |
| Peak HR (bpm) | 154 | 123 | 145 |
| Peak work rate (watt) | 148 | 111 | 137 |
| VE/VCO2 slope | 25.7 | 25.0 | 24.6 |
| VO2 work slope (mL/min/Watt) | 11.3 | 11.5 | 11.9 |
| RR (bpm) | 27.5 | 24 | 32 |
| Peak VE (L/min) | 60.8 | 57.3 | 72.4 |
| Peak RER | 1.08 | 1.24 | 1.27 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Mapelli, M.; Cattadori, G.; Salvioni, E.; Mattavelli, I.; Pestrin, E.; Attanasio, U.; Magrì, D.; Palermo, P.; Agostoni, P. “Under the Bridge”: Looking for Ischemia in a Patient with Intramyocardial Coronary Artery Course—The Role of the Cardiopulmonary Exercise Test. J. Clin. Med. 2023, 12, 5764. https://doi.org/10.3390/jcm12175764
Mapelli M, Cattadori G, Salvioni E, Mattavelli I, Pestrin E, Attanasio U, Magrì D, Palermo P, Agostoni P. “Under the Bridge”: Looking for Ischemia in a Patient with Intramyocardial Coronary Artery Course—The Role of the Cardiopulmonary Exercise Test. Journal of Clinical Medicine. 2023; 12(17):5764. https://doi.org/10.3390/jcm12175764
Chicago/Turabian StyleMapelli, Massimo, Gaia Cattadori, Elisabetta Salvioni, Irene Mattavelli, Emanuele Pestrin, Umberto Attanasio, Damiano Magrì, Pietro Palermo, and Piergiuseppe Agostoni. 2023. "“Under the Bridge”: Looking for Ischemia in a Patient with Intramyocardial Coronary Artery Course—The Role of the Cardiopulmonary Exercise Test" Journal of Clinical Medicine 12, no. 17: 5764. https://doi.org/10.3390/jcm12175764
APA StyleMapelli, M., Cattadori, G., Salvioni, E., Mattavelli, I., Pestrin, E., Attanasio, U., Magrì, D., Palermo, P., & Agostoni, P. (2023). “Under the Bridge”: Looking for Ischemia in a Patient with Intramyocardial Coronary Artery Course—The Role of the Cardiopulmonary Exercise Test. Journal of Clinical Medicine, 12(17), 5764. https://doi.org/10.3390/jcm12175764