

Impact of Sarcopenia on Spinal Spondylosis: A Literature Review

 , , , and
, , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Database Search
2.2. Study Eligibility
2.3. Data Collection
3. Results
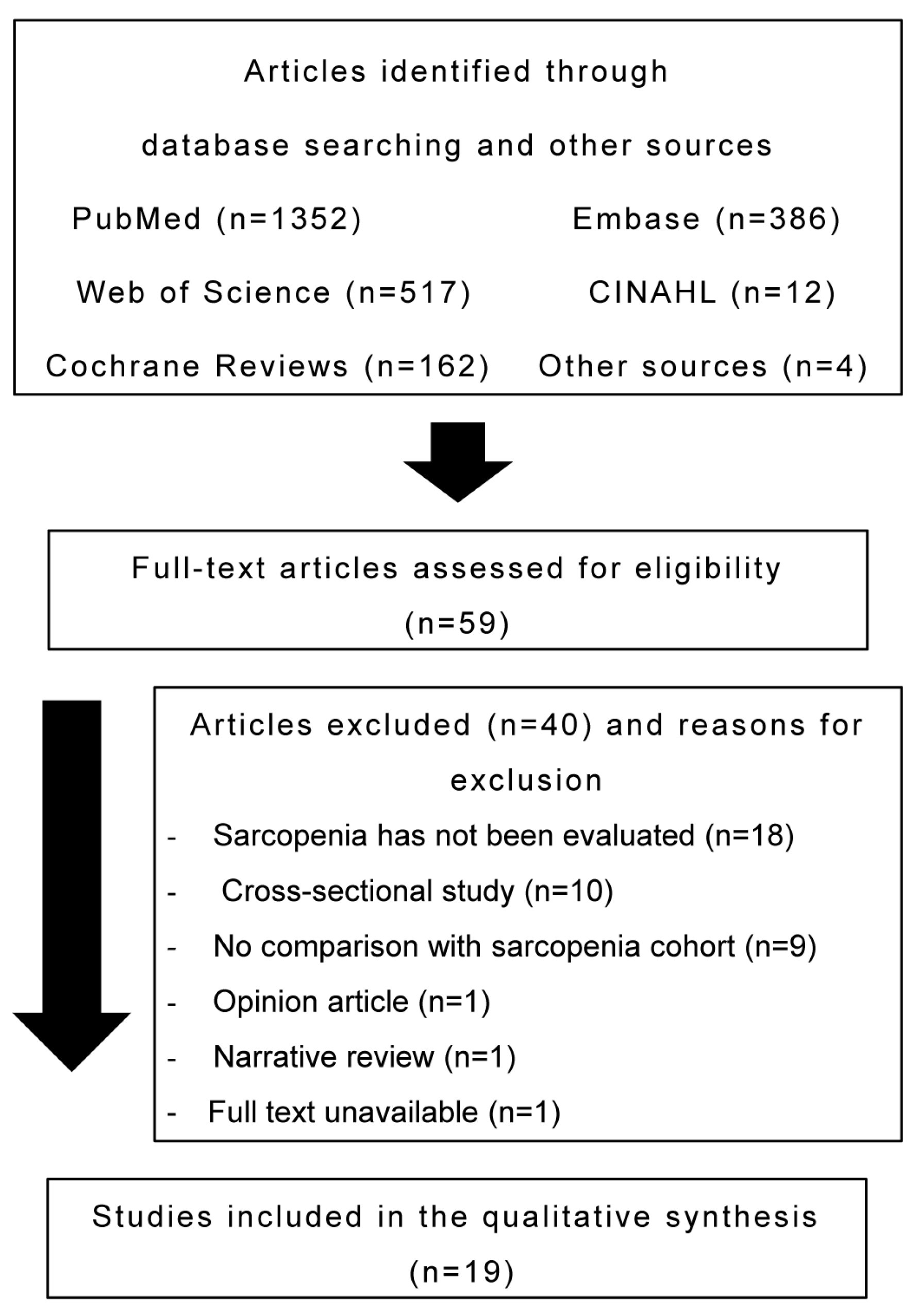
3.1. Search Results
3.2. Characteristics of Included Studies
3.2.1. Participant Characteristics
3.2.2. Study Characteristics
3.2.3. Sarcopenia Definition and Assessment Methods
3.2.4. Study Outcomes
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cruz-Jentoft, A.J.; Bahat, G.; Bauer, J.; Boirie, Y.; Bruyère, O.; Cederholm, T.; Cooper, C.; Landi, F.; Rolland, Y.; Sayer, A.A.; et al. Sarcopenia: Revised European consensus on definition and diagnosis. Age Ageing 2019, 48, 16–31. [Google Scholar] [CrossRef]
- Hida, T.; Shimokata, H.; Sakai, Y.; Ito, S.; Matsui, Y.; Takemura, M.; Kasai, T.; Ishiguro, N.; Harada, A. Sarcopenia and sarcopenic leg as potential risk factors for acute osteoporotic vertebral fracture among older women. Eur. Spine J. 2016, 25, 3424–3431. [Google Scholar] [CrossRef] [PubMed]
- Chiang, M.H.; Kuo, Y.J.; Chen, Y.P. The association between sarcopenia and postoperative outcomes among older adults with hip fracture: A systematic review. J. Appl. Gerontol. 2021, 40, 1903–1913. [Google Scholar] [CrossRef]
- Bo, J.; Zhao, X.; Hua, Z.; Li, J.; Qi, X.; Shen, Y. Impact of sarcopenia and sagittal parameters on the residual back pain after percutaneous vertebroplasty in patients with osteoporotic vertebral compression fracture. J. Orthop. Surg. Res. 2022, 17, 111. [Google Scholar] [CrossRef]
- Kemmler, W.; Teschler, M.; Goisser, S.; Bebenek, M.; von Stengel, S.; Bollheimer, L.C.; Sieber, C.C.; Freiberger, E. Prevalence of sarcopenia in Germany and the corresponding effect of osteoarthritis in females 70 years and older living in the community: Results of the FORMoSA study. Clin. Interv. Aging 2015, 10, 1565–1573. [Google Scholar] [CrossRef]
- Babu, J.M.; Kalagara, S.; Durand, W.; Antoci, V.; Deren, M.E.; Cohen, E. Sarcopenia as a risk factor for prosthetic infection after total hip or knee arthroplasty. J. Arthroplast. 2019, 34, 116–122. [Google Scholar] [CrossRef]
- Liao, C.D.; Chen, H.C.; Liou, T.H.; Lin, C.L.; Huang, S.W. Impact of sarcopenia and obesity on gait speed after total knee replacement. J. Am. Med. Dir. Assoc. 2022, 23, 631–637. [Google Scholar] [CrossRef]
- Wu, W.T.; Lee, T.M.; Han, D.S.; Chang, K.V. The prevalence of sarcopenia and its impact on clinical outcomes in lumbar degenerative spine disease—A systematic review and meta-analysis. J. Clin. Med. 2021, 10, 773. [Google Scholar] [CrossRef] [PubMed]
- Tricco, A.C.; Lillie, E.; Zarin, W.; O’Brien, K.K.; Colquhoun, H.; Levac, D.; Moher, D.; Peters, M.D.J.; Horsley, T.; Weeks, L.; et al. PRISMA-S: An extension to the PRISMA Statement for Reporting Literature Searches in Systematic Reviews. Syst. Rev. 2021, 10, 39. [Google Scholar] [CrossRef]
- Eguchi, Y.; Suzuki, M.; Yamanaka, H.; Tamai, H.; Kobayashi, T.; Orita, S.; Yamauchi, K.; Suzuki, M.; Inage, K.; Fujimoto, K.; et al. Influence of skeletal muscle mass and spinal alignment on surgical outcomes for lumbar spinal stenosis. Asian Spine J. 2018, 12, 556–562. [Google Scholar] [CrossRef] [PubMed]
- Koshimizu, H.; Sakai, Y.; Harada, A.; Ito, S.; Ito, K.; Hida, T. The impact of sarcopenia on cervical spine sagittal alignment after cervical laminoplasty. Clin. Spine Surg. 2018, 31, E342–E346. [Google Scholar] [CrossRef] [PubMed]
- Inose, H.; Yamada, T.; Hirai, T.; Yoshii, T.; Abe, Y.; Okawa, A. The impact of sarcopenia on the results of lumbar spinal surgery. Osteoporos. Sarcopenia 2018, 4, 33–36. [Google Scholar] [CrossRef] [PubMed]
- Toyoda, H.; Hoshino, M.; Ohyama, S.; Terai, H.; Suzuki, A.; Yamada, K.; Takahashi, S.; Hayashi, K.; Tamai, K.; Hori, Y.; et al. Impact of sarcopenia on clinical outcomes of minimally invasive lumbar decompression surgery. Sci. Rep. 2019, 9, 16619. [Google Scholar] [CrossRef]
- Sakai, Y.; Wakao, N.; Matsui, H.; Tomita, K.; Watanabe, T.; Iida, H. Surgical results in older patients with lumbar spinal stenosis according to gait speed in relation to the diagnosis for sarcopenia. J. Orthop. Surg. 2020, 28, 2309499020918422. [Google Scholar] [CrossRef]
- Wada, T.; Tanishima, S.; Kitsuda, Y.; Osaki, M.; Nagashima, H.; Hagino, H. Preoperative low muscle mass is a predictor of falls within 12 months of surgery in patients with lumbar spinal stenosis. BMC Geriatr. 2020, 20, 516. [Google Scholar] [CrossRef]
- Wada, T.; Tanishima, S.; Kitsuda, Y.; Osaki, M.; Nagashima, H.; Hagino, H. Association between preoperative low muscle mass and psychological factors after surgery among patients with lumbar spinal stenosis: A longitudinal study. J. Clin. Neurosci. 2021, 89, 8–14. [Google Scholar] [CrossRef]
- Bokshan, S.L.; Han, A.; Depasse, J.M.; Marcaccio, S.E.; Eltorai, A.E.M.; Daniels, A.H. Inpatient costs and blood transfusion rates of sarcopenic patients following thoracolumbar spine surgery. J. Neurosurg. Spine 2017, 27, 676–680. [Google Scholar] [CrossRef] [PubMed]
- McKenzie, J.C.; Wagner, S.C.; Sebastian, A.; Casper, D.S.; Mangan, J.; Stull, J.; Hilibrand, A.S.; Vaccaro, A.R.; Kepler, C. Sarcopenia does not affect clinical outcomes following lumbar fusion. J. Clin. Neurosci. 2019, 64, 150–154. [Google Scholar] [CrossRef]
- Akbik, O.S.; Al-Adli, N.; Pernik, M.N.; Hicks, W.H.; Hall, K.; Aoun, S.G.; Bagley, C.A. A comparative analysis of frailty, disability, and sarcopenia with patient characteristics and outcomes in adult spinal deformity surgery. Glob. Spine J. 2022, 21925682221082053. [Google Scholar] [CrossRef]
- Pinter, Z.W.; Salmons, H.I.t.; Townsley, S.; Omar, A.; Freedman, B.A.; Currier, B.L.; Elder, B.D.; Nassr, A.N.; Bydon, M.; Wagner, S.C.; et al. Multifidus sarcopenia is associated with worse patient-reported outcomes following posterior cervical decompression and fusion. Spine 2022, 47, 1426–1434. [Google Scholar] [CrossRef]
- Albright, J.A.; Chang, K.; Alsoof, D.; McDonald, C.L.; Diebo, B.G.; Daniels, A.H. Sarcopenia and postoperative complications, cost of care, and all-cause hospital readmission following lumbar spine arthrodesis: A propensity matched cohort study. World Neurosurg. 2023, 169, e131–e140. [Google Scholar] [CrossRef] [PubMed]
- Kwon, J.W.; Lee, B.H.; Lee, S.B.; Sung, S.; Lee, C.U.; Yang, J.H.; Park, M.S.; Byun, J.; Lee, H.M.; Moon, S.H. Hand grip strength can predict clinical outcomes and risk of falls after decompression and instrumented posterolateral fusion for lumbar spinal stenosis. Spine J. 2020, 20, 1960–1967. [Google Scholar] [CrossRef] [PubMed]
- Ko, S.H.; Park, S.J.; Kim, N.Y.; Jeon, W.; Shin, D.A.; Kim, S.H. Influence of preoperative handgrip strength on length of stay after lumbar fusion surgery. J. Clin. Med. 2022, 11, 3928. [Google Scholar] [CrossRef]
- Li, H.; Li, J.; Ma, Y.; Li, F.; Xu, Z.; Chen, Q. The effect of sarcopenia in the clinical outcomes following stand-alone lateral lumbar interbody fusion. J. Back Musculoskelet. Rehabil. 2021, 34, 469–476. [Google Scholar] [CrossRef]
- Li, Z.; Zhang, C.; Wang, H.; Yu, K.; Zhang, J.; Wang, Y. Impact of sarcopenia on effectiveness of lumbar decompression surgery in patients with lumbar spinal stenosis. Zhongguo Xiu Fu Chong Jian Wai Ke Za Zhi 2022, 36, 745–750. [Google Scholar] [CrossRef] [PubMed]
- Ruffilli, A.; Manzetti, M.; Cerasoli, T.; Barile, F.; Viroli, G.; Traversari, M.; Salamanna, F.; Fini, M.; Faldini, C. Osteopenia and sarcopenia as potential risk factors for surgical site infection after posterior lumbar fusion: A retrospective study. Microorganisms 2022, 10, 1905. [Google Scholar] [CrossRef]
- Barile, F.; Ruffilli, A.; Fiore, M.; Manzetti, M.; Geraci, G.; Viroli, G.; Faldini, C. Is sarcopenia a risk factor for postoperative surgical site infection after posterior lumbar spinal fusion? Int. J. Spine Surg. 2022, 16, 735–739. [Google Scholar] [CrossRef]
- Cruz-Jentoft, A.J.; Sayer, A.A. Sarcopenia. Lancet 2019, 393, 2636–2646. [Google Scholar] [CrossRef]
- Petermann-Rocha, F.; Balntzi, V.; Gray, S.R.; Lara, J.; Ho, F.K.; Pell, J.P.; Celis-Morales, C. Global prevalence of sarcopenia and severe sarcopenia: A systematic review and meta-analysis. J. Cachexia Sarcopenia Muscle 2022, 13, 86–99. [Google Scholar] [CrossRef]
- Jermy, J.E.; Copley, P.C.; Poon, M.T.C.; Demetriades, A.K. Does pre-operative multifidus morphology on MRI predict clinical outcomes in adults following surgical treatment for degenerative lumbar spine disease? A systematic review. Eur. Spine J. 2020, 29, 1318–1327. [Google Scholar] [CrossRef]
- Khalooeifard, R.; Shariatpanahi, Z.V.; Ahani, A.; Keykhaee, M.; Oraee-Yazdani, M.; Zali, A.; Oraee-Yazdani, S. Effect of protein supplement on paraspinal muscles in spine fusion surgery: A randomized, double-blind, placebo-controlled trial. Int. J. Spine Surg. 2021, 15, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Kernc, D.; Strojnik, V.; Vengust, R. Early initiation of a strength training based rehabilitation after lumbar spine fusion improves core muscle strength: A randomized controlled trial. J. Orthop. Surg. Res. 2018, 19, 151. [Google Scholar] [CrossRef] [PubMed]
- Zaina, F.; Tomkins-Lane, C.; Carragee, E.; Negrini, S. Surgical versus non-surgical treatment for lumbar spinal stenosis. Cochrane Database Syst. Rev. 2016, 2016, Cd010264. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| # | Search Formula | Number of Hits |
|---|---|---|
| 1 | “Cervical spondylosis” OR “cervical myelopathy” OR “cervical spondylosis myelopathy” OR “cervical disc herniation” OR “cervical vertebrae” OR “cervical stenosis” OR “ossification of the posterior longitudinal ligament” OR “radiculopathy” | 17,785 |
| 2 | “Thoracic spine” OR “ankylosing spinal hyperostosis” OR “ossification of ligamentum flavum” OR “thoracic spondylotic myelopathy” | 6770 |
| 3 | “Lumbar spine” OR “lumbar spinal stenosis” OR “lumbar spinal canal stenosis” OR “lumbar spondylolisthesis” OR “spondylolisthesis” OR “lumbar degenerative disc disease” OR “degenerative lumbar spondylosis” OR “lumbar disc herniation” | 45,851 |
| 4 | “Adult spinal deformity” OR “scoliosis” OR “kyphoscoliosis” OR “kyphosis” | 34,131 |
| 5 | “Arthroscopy” OR “arthroplasty” OR “decompression” OR “fusion” OR “laminectomy” OR “laminoplasty” OR “lumbar surgery” | 374,711 |
| 6 | “Sarcopenia” OR “sarcopenic” OR “muscle mass” OR “muscle atrophy” OR “appendicular lean mass” | 40,787 |
| 7 | #1 OR #2 OR #3 OR #4 OR #5 AND #6 | 1352 |
| Author, Year of Publication | Study Design | Population (Including Nationality, Disease, and Sex) | Definition and Assessment Methods of Sarcopenia | Subject Details | Outcomes | Key Findings of Results |
|---|---|---|---|---|---|---|
| Ko et al. (2022) [23] | Retrospective | Korea; patients who underwent elective posterior lumbar interbody fusion surgery (n = 225; male: female, 93:134) | HGS and SMI | Patients with low HGS (n = 86; mean age, 66.0 ± 9.0 years) Patients with normal HGS (n = 139; mean age, 65.0 ± 9.0 years) Prevalence of sarcopenia: 38.2% | LOS postoperative complications | A longer LOS (median 10 vs. 8 days) and a higher incidence of serious postoperative complications (15.1% vs. 3.6%) were observed in the low HGS group. |
| Kwon et al. (2020) [22] | Retrospective | Korea; patients who underwent spinal surgery for LSS (n = 278; male: female, 96:182) | HGS | Females in the low HGS group (n = 91; mean age, 69.5 ± 6.5 years); Males in the low HGS group (n = 48; mean age, 69.9 ± 6.5 years); Females in the high HGS group (n = 91; mean age, 64.5 ± 7.1 years); Males in the high HGS group (n = 48; mean age, 65.4 ± 9.7 years) Prevalence of sarcopenia: 50.0% | ODI, EQ-5D, VAS for back or leg pain, functional mobility tests (AST, SMT, TUG, STS) | In females, postoperative EQ-5D and ODI were clinically improved in the high HGS group. |
| Bokshan et al. (2017) [17] | Retrospective | Rhode Island (USA); patients who underwent thoracolumbar spine surgery (n = 50; male:female, 26:24) | Fell into the lowest tertile for their sex-specific TPA (the cross-sectional areas of the left and right psoas muscles at the level of the transverse process of L-4 on CT) | Patients with sarcopenia (n = 16; mean age, 76.6 ± 2.2 years) Patients without sarcopenia (n = 34; mean age, 70.8 ± 1.4 years) Prevalence of sarcopenia: 32.0% | Inpatient costs, transfusion rate, and rate of advanced imaging utilization | Patients with sarcopenia were 2.1 times as likely to require a blood transfusion (43.8% vs. 20.6%) and exhibited a 2.6-fold greater usage of advanced imaging (68.8% vs. 26.5%), associated with higher diagnostic imaging costs (USD 2452 vs. USD 801). |
| Inose et al. (2018) [12] | Retrospective | Japan; patients who underwent spinal surgery for LSS and lumbar compression fracture (n = 74; male:female, 33:52) | AWGS 2014 criteria SMI (DXA) determined by cutoff values only | Patients with sarcopenia (n = 37; mean age, 74.8 ± 0.9 years) Patients without sarcopenia (n = 37; mean age, 73.0 ± 1.0 years) Prevalence of sarcopenia: 47.4% | JOA score, VAS score (lower back pain, lower extremity pain, lower extremity numbness), patients who undergo rehabilitation | JOA scores (24.7 ± 0.4 vs. 23.0 ± 0.6) and recovery rates (68.6 ± 3.3 vs. 53.8 ± 5.2) at the final follow-up were significantly reduced in the sarcopenia subgroup. |
| Wu et al. (2021) [8] | Meta-analysis | Japan, Canada, the US, Korea; patients with LDSD (n = 1953) (Extracted from 14 studies) | None | None | Prevalence of sarcopenia, postoperative pain VAS, postoperative QOL | The overall prevalence of sarcopenia among patients with LDSD was 24.8% (95% CI, 17.3–34.3%). Patients with sarcopenia did not experience increased lower back and leg pain. However, lower QOL (SMD, −0.63; 95% CI, −0.84–−0.41) was observed postoperatively. |
| Koshimizu et al. (2018) [11] | Prospective | Japan; patients who underwent cervical laminoplasty (n = 171; male: female, 114: 57) | Sanada Classification SMI (DXA) | Patients with sarcopenia (n = 48; male:female, 37:11; mean age, 75.1 ± 8.9 years) Patients without sarcopenia (n = 123; male:female, 77:46; mean age, 70.3 ± 8.9 years) Prevalence of sarcopenia: 28.1% | JOA score, SF-36 | The SF-36 score at 1 year postoperatively was higher in the non-sarcopenia group than that in the sarcopenia group. The JOA score was higher in the non-sarcopenia group at 1 year postoperatively. |
| McKenzie et al. (2019) [18] | Retrospective | USA; patients who underwent a single-level lumbar fusion for DS (n = 97; male:female, 46:51) | Sarcopenia is defined as 1 SD lower than the mean of the paraspinal muscle index by MRI | Patients with sarcopenia (n = 16; mean age, 64.6 ± 16.9 years) Patients without sarcopenia (n = 81; mean age, 61.6 ± 13.3 years) Prevalence of sarcopenia: 18.1% | ODI, SF-12 Physical (SF-12 P), SF-12 Mental (SF-12 M) and back pain VAS scores | No significant differences in ODI, SF-12, or back pain VAS scores. |
| Wada et al. (2020) [15] | Prospective | Japan; preoperative patients with LSS (n = 74; male:female, 36:38) | Low SMI (BIA) by AWGS 2019 | Fallers (n = 24, median age, 73.0, range: 67.3–76.8 years) Non-fallers (n = 50; median age, 68.0, range: 63.0–76.0 years) Prevalence of sarcopenia: 20.3% | Falls occurred 12 months postoperatively | Preoperative low muscle mass predicted the occurrence of falls during the first 12 months after surgery (OR, 4.46; 95% CI, 1.02–19.63) |
| Wada et al. (2021) [16] | Prospective | Japan; preoperative patients with LSS (n = 73; male:female, 38:35) | Low SMI (BIA) by AWGS 2019 | Patients with sarcopenia (n = 16; median age, 75.0; range, 70.3–81.3 years) Patients without sarcopenia (n = 57; median age, 68.0; range, 63.0–76.0 years) Prevalence of sarcopenia: 21.9% | NRS: leg pain, low back pain, JOA score, PCS, FABQ, HADS, walking velocity, HGS | The sarcopenia group had higher FABQ-PA scores than the normal group. Low muscle mass was significantly related to changes in the FABQ-PA score. |
| Akbik et al. (2022) [19] | Retrospective | USA; patients who underwent thoracolumbar ASD surgery (≥4 levels) (n = 235; male:female, 80:155) | The lowest quartile of PMI values measured at L3 by CT | Patients with sarcopenia (n = 59; mean age, 69.2 ± 9.6 years) Patients without sarcopenia (n = 176; mean age, 69.7 ± 7.4 years) Prevalence of sarcopenia: 25.1% | ODI, postoperative complications, LOS, reoperation, mortality | No significant differences in ODI, postoperative complications, LOS, reoperation, or mortality. |
| Eguchi et al. (2018) [10] | Retrospective | Japan; female patients who underwent surgery for LSS (n = 34) | Sanada Classification SMI (DXA) | Patients with Sarcopenia (n = 9) Patients with pre-sarcopenia (n = 12) Patients without sarcopenia (n = 13) Average age not stated Prevalence of sarcopenia: 26.5% | VAS for LBP, JOA score, RDQ | Patients with sarcopenia had lower RDQ at 6 months postoperatively than normal subjects. |
| Ruffilli et al. (2022) [26] | Retrospective | Italy; patients aged 50–85 years with LDSD treated with short posterior arthrodesis (3 levels or less) (n = 308; 148 male, 160 female) | PLVI by MRI (PLVI = (left psoas CSA + right psoas CSA)/2/L4 vertebral body CSA), which is the mean CSA of the psoas major divided by the mean area of the L4 vertebral body). PLVI is stratified into high and low groups at a cutoff value of 0.71 at baseline | Patients with sarcopenia (n = 153; mean age, 65.3 ± 6.4 years) Patients without sarcopenia (n = 155; mean age, 62.3 ± 5.7 years) Prevalence of sarcopenia: 49.7% | SSI | SSI was evenly distributed between low and high PLVI. |
| Sakai et al. (2020) [14] | Case-control study (retrospective) | Japan; patients with LSS who underwent surgical treatment (n = 235; male: female, 135:100) | AWGS2014 SMI by DXA | Patients with Sarcopenia (n = 33; mean age, 76.7 ± 5.9 years) Patients without sarcopenia (n = 171; mean age, 72.3 ± 5.5 years) Prevalence of sarcopenia: 14.0% | RDQ, EQ5D, SF36 | Postoperatively, all three groups had good surgical outcomes. There were no significant differences between the sarcopenia and non-sarcopenia groups. |
| Barile et al. (2022) [27] | Retrospective | Italy; patients with LDSD who underwent a short (3 levels or less) posterior lumbar fusion (n = 304; male: female, 149:155) | PLVI by MRI (PLVI = (left psoas CSA + right psoas CSA)/2/L4 vertebral body CSA), which is the mean CSA of the psoas major divided by the mean area of the L4 vertebral body). PLVI is stratified into high and low groups at a cutoff value of 0.71 at baseline | Patients with sarcopenia (n = 154; mean age, 63.6 ± 5.9 years) Patients without sarcopenia (n = 150; mean age, 64.6 ± 6.0 years) Prevalence of sarcopenia: 50.7% | SSI | Sarcopenia (Low PLVI) was not associated with postoperative SSI |
| Pinter et al. (2022) [20] | Retrospective | USA; patients undergoing posterior cervical fusion from C2 to T2 for myelopathy with or without radiculopathy (n = 99; male:female, 55:44) | Goutalier classification of bilateral multifidus muscles at the C5-C6 level by MRI | Goutalier 0–1 (n = 28; mean age, 61.6 ± 9.0 years) Goutalier 1.5–2 (n = 5; mean age, 64.2 ± 9.2 years) Goutalier 2.5–4 (severe sarcopenia) (n = 26; mean age, 64.6 ± 8.9 years) Prevalence of sarcopenia: 26.1% | NDI, VAS neck scores, PROMIS Physical and Mental Component Scores | Patients with severe sarcopenia were more likely to report worsening of NDI, VAS Neck score, and PROMIS |
| Toyoda et al. (2019) [13] | Retrospective | Japan; patients aged >65 years who underwent minimally invasive lumbar decompression surgery (n = 130; male:female, 70:60) | SMI (BIA) by AWGS 2014 | Patients with sarcopenia (n = 26; mean age, 80.9 ± 5.7 years) Dynapenia (n = 41; mean age, 77.5 ± 6.3) Patients without sarcopenia (n = 57; mean age, 74.6 ± 5.8 years) Prevalence of sarcopenia: 20.0% | JOA score VAS for leg pain, low back pain | No significant differences were observed between the sarcopenia and non-sarcopenia groups. |
| Li et al. (2021) [24] | Retrospective | China; patients who underwent a single-level stand-alone LLIF for lumbar diseases (n = 69; male:female, 28:41) | Low SMI (BIA) by AWGS 2019 | Patients with sarcopenia (n = 16; median age, 66.5 years) Patients without sarcopenia subjects (n = 41; median age, 59.0 years) Prevalence of sarcopenia: 23.1% | ODI, back pain VAS | Postoperative ODI scores were higher in the sarcopenia group (35.1 vs. 25.1%) than those in normal subjects, and the percentage of ODI improvement was lower in the sarcopenia group (30.5% vs. 47.3%) than that in normal subjects. There was no significant difference in pain VAS. |
| Li et al. (2022) [25] | Retrospective | China; patients with LSS (n = 50; male: female, 22:28) | SMI at L3 level by CT (<45.4 cm2/m2 for males and <34.4 cm2/m2 for females) No description of the relevant muscle | Patients with sarcopenia (n = 25; male:female, 13:12; mean age, 64.8 years) Patients without sarcopenia (n = 25; male:female, 9:16; mean age 59.2 years) Prevalence of sarcopenia: 50.0% | Operative time, intraoperative blood loss, postoperative drainage volume, LOS, complications, pain VAS score, and ODI | The duration of hospitalization in the sarcopenia group was significantly longer than that in the non-sarcopenia group. Postoperative differences in VAS and ODI scores for lower back pain were significantly higher in the sarcopenia group than those in the non-sarcopenia group. |
| Albright et al. (2023) [21] | Retrospective | USA; patients who underwent index lumbar spine arthrodesis (n = 239,953; male: female, 104,319:135,634) | ICD code | Patients with sarcopenia (n = 1087; male:female, 519:568; mean age, 61.0 ± 13.7 years) Control patients (n = 1087; male:female, 530:557; mean age, 61.1 ± 13.2 years) Prevalence of sarcopenia: 4.5% | 90-Day surgical and medical complication rates; cumulative rate of revision surgeries and readmission rates for all causes; and treatment costs | Patients with sarcopenia were more likely to be diagnosed with UTI (OR, 1.41) and to undergo incisional drainage (OR, 2.66). Patients with sarcopenia showed a high cumulative rehospitalization rate (OR, 1.24) |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kitsuda, Y.; Wada, T.; Tanishima, S.; Osaki, M.; Nagashima, H.; Hagino, H. Impact of Sarcopenia on Spinal Spondylosis: A Literature Review. J. Clin. Med. 2023, 12, 5401. https://doi.org/10.3390/jcm12165401
Kitsuda Y, Wada T, Tanishima S, Osaki M, Nagashima H, Hagino H. Impact of Sarcopenia on Spinal Spondylosis: A Literature Review. Journal of Clinical Medicine. 2023; 12(16):5401. https://doi.org/10.3390/jcm12165401
Chicago/Turabian StyleKitsuda, Yuki, Takashi Wada, Shinji Tanishima, Mari Osaki, Hideki Nagashima, and Hiroshi Hagino. 2023. "Impact of Sarcopenia on Spinal Spondylosis: A Literature Review" Journal of Clinical Medicine 12, no. 16: 5401. https://doi.org/10.3390/jcm12165401
APA StyleKitsuda, Y., Wada, T., Tanishima, S., Osaki, M., Nagashima, H., & Hagino, H. (2023). Impact of Sarcopenia on Spinal Spondylosis: A Literature Review. Journal of Clinical Medicine, 12(16), 5401. https://doi.org/10.3390/jcm12165401