
Comparative Effectiveness of Apixaban and Rivaroxaban Lead-in Dosing in VTE Treatment: Observational Multicenter Real-World Study
 , , , , ,
, , , , ,
Abstract
1. Introduction
2. Materials and Methods
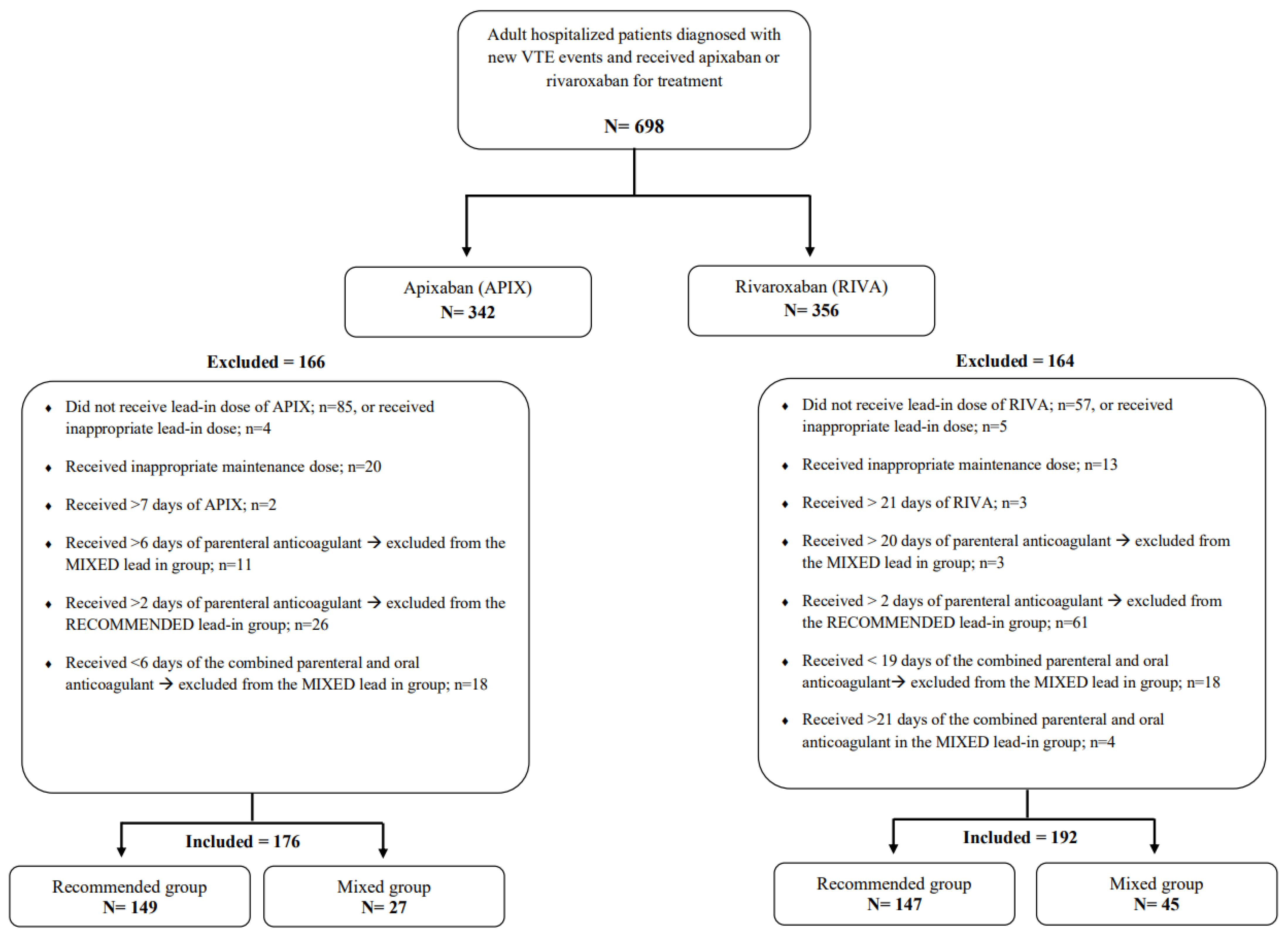
2.1. Study Design, Setting, and Patients
2.2. Data Collection and Outcomes
2.3. Statistical Analysis
3. Results
3.1. Patients’ Demographics and Medical Histories
3.2. VTE Events and Medications Used
3.3. Clinical Outcomes
3.3.1. rVTE
3.3.2. MB
3.3.3. CRNMB and Rehospitalization
3.3.4. Sub-Group Analysis
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Limone, B.L.; Hernandez, A.V.; Michalak, D.; Bookhart, B.K.; Coleman, C.I. Timing of recurrent venous thromboembolism early after the index event: A meta-analysis of randomized controlled trials. Thromb. Res. 2013, 132, 420–426. [Google Scholar] [CrossRef] [PubMed]
- Centers for Disease Control and Prevention. Venous thromboembolism (blood clots). 2022. Available online: https://www.cdc.gov/ncbddd/dvt/data.html (accessed on 9 June 2022).
- Hillis, C.; Crowther, M.A. Acute phase treatment of VTE: Anticoagulation, including non-vitamin K antagonist oral anticoagulants. Thromb. Haemost. 2015, 113, 1193–1202. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Gallus, A.; Goldhaber, S.Z.; Haas, S.; Huisman, M.V.; Hull, R.D.; Kakkar, A.K.; Misselwitz, F.; Schellong, S. Treatment of proximal deep-vein thrombosis with the oral direct factor Xa inhibitor rivaroxaban (BAY 59-7939): The ODIXa-DVT (oral direct factor Xa inhibitor BAY 59-7939 in patients with acute symptomatic deep-vein thrombosis) study. Circulation 2007, 116, 180–187. [Google Scholar] [CrossRef] [PubMed]
- Beckman, M.G.; Hooper, W.C.; Critchley, S.E.; Ortel, T.L. Venous thromboembolism: A public health concern. Am. J. Prev. Med. 2010, 38 (Suppl. S4), S495–S501. [Google Scholar] [CrossRef] [PubMed]
- Buller, H.R.; Lensing, A.W.A.; Prins, M.H.; Agnelli, G.; Cohen, A.; Gallus, A.; Misselwitz, F.; Raskob, G.; Schellong, S.; Segers, A. A dose-ranging study evaluating once-daily oral administration of the factor Xa inhibitor rivaroxaban in the treatment of patients with acute symptomatic deep vein thrombosis: The Einstein-DVT Dose-Ranging Study. Blood 2008, 112, 2242–2247. [Google Scholar] [CrossRef] [PubMed]
- Agnelli, G.; Buller, H.R.; Cohen, A.; Curto, M.; Gallus, A.S.; Johnson, M.; Masiukiewicz, U.; Pak, R.; Thompson, J.; Raskob, G.E.; et al. Oral apixaban for the treatment of acute venous thromboembolism. N. Engl. J. Med. 2013, 369, 799–808. [Google Scholar] [CrossRef] [PubMed]
- Bauersachs, R.; Berkowitz, S.D.; Brenner, B.; Buller, H.R.; Decousus, H.; Gallus, A.S. Oral rivaroxaban for symptomatic venous thromboembolism. N. Engl. J. Med. 2010, 363, 2499–2510. [Google Scholar] [PubMed]
- Büller, H.R.; Prins, M.H.; Lensin, A.W.; Decousus, H.; Jacobson, B.F.; Minar, E. Oral rivaroxaban for the treatment of symptomatic pulmonary embolism. N. Engl. J. Med. 2012, 366, 1287–1297. [Google Scholar] [PubMed]
- Schulman, S.; Kakkar, A.K.; Goldhaber, S.Z.; Schellong, S.; Eriksson, H.; Mismetti, P.; Christiansen, A.V.; Friedman, J.; Le Maulf, F.; Peter, N.; et al. Treatment of acute venous thromboembolism with dabigatran or warfarin and pooled analysis. Circulation 2014, 129, 764–772. [Google Scholar] [CrossRef] [PubMed]
- Büller, H.R.; Décousus, H.; Grosso, M.A.; Mercuri, M.; Middeldorp, S.; Prins, M.H. Edoxaban versus warfarin for the treatment of symptomatic venous thromboembolism. N. Engl. J. Med. 2013, 369, 1406–1415. [Google Scholar] [PubMed]
- Williams, M.; Ahuja, T.; Raco, V.; Papadopoulos, J.; Green, D.; Yuriditsky, E.; Arnouk, S. Real world prescribing practices of apixaban or rivaroxaban lead-in doses for the treatment of venous thromboembolism in hospitalized patients. J. Thromb. Thrombolysis 2022, 54, 219–229. [Google Scholar] [CrossRef] [PubMed]
- Kuijer, P.M.; Hutten, B.A.; Prins, M.H.; Büller, H.R. Prediction of the risk of bleeding during anticoagulant treatment for venous thromboembolism. Arch. Intern. Med. 1999, 159, 457–460. [Google Scholar] [CrossRef] [PubMed]
- Schulman, S.; Kearon, C. Definition of major bleeding in clinical investigations of antihemostatic medicinal products in non-surgical patients. J. Thromb. Haemost. 2005, 3, 692–694. [Google Scholar] [CrossRef] [PubMed]
- Stevens, S.M.; Woller, S.C.; Baumann Kreuziger, L.; Bounameaux, H.; Doerschug, K.; Geersing, G.J.; Huisman, M.V.; Kearon, C.; King, C.S.; Knighton, A.J.; et al. Executive Summary: Antithrombotic Therapy for VTE Disease: Second Update of the CHEST Guideline and Expert Panel Report. Chest 2021, 160, 2247–2259. [Google Scholar] [CrossRef] [PubMed]
- Ortel, T.L.; Neumann, I.; Ageno, W.; Beyth, R.; Clark, N.P.; Cuker, A.; Hutten, B.A.; Jaff, M.R.; Manja, V.; Schulman, S.; et al. American Society of Hematology 2020 guidelines for management of venous thromboembolism: Treatment of deep vein thrombosis and pulmonary embolism. Blood Adv. 2020, 4, 4693–4738. [Google Scholar] [CrossRef] [PubMed]
- Konstantinides, S.V.; Meyer, G.; Becattini, C.; Bueno, H.; Geersing, G.J.; Harjola, V.-P.; Huisman, M.V.; Humbert, M.; Jennings, C.S.; Jiménez, D.; et al. 2019 ESC Guidelines for the diagnosis and management of acute pulmonary embolism developed in collaboration with the European Respiratory Society (ERS). Eur. Heart J. 2020, 41, 543–603. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.K.; Gohel, M.; Baekgaard, N.; Bauersachs, R.; Bellmunt-Montoya, S.; Black, S.A.; Cate-Hoek, A.J.T.; Elalamy, I.; Enzmann, F.K.; Geroulakos, G.; et al. Editor’s Choice—European Society for Vascular Surgery (ESVS) 2021 Clinical Practice Guidelines on the Management of Venous Thrombosis. Eur. J. Vasc. Endovasc. Surg. 2021, 61, 9–82. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Patient Characteristics | Overall | Lead-in Group | p-Value | |
|---|---|---|---|---|
| Mixed | Recommended | |||
| Overall number of patients | 368 | 72 | 296 | |
| Age in years, mean (SD) | 53.1 ± 19.6 | 55.2 ± 19.2 | 52.6 ± 19.7 | 0.316 |
| BMI (kg/m2), mean (SD) | 30.8 ± 7.0 | 29.3 ± 7.1 | 31.1 ± 6.9 | 0.054 |
| Hospital length of Stay (days) | 6.1 ± 13.3 | 12.2 ± 25.3 | 4.6 ± 7.4 | <0.0001 |
| Gender | 0.355 | |||
| Male | 131 (35.6) | 29 (40.3) | 102 (34.5) | |
| Female | 237 (64.4) | 43 (59.7) | 194 (65.5) | |
| Pre-existing conditions | ||||
| Atrial fibrillation | 8 (2.2) | 3 (4.2) | 5 (1.7) | 0.192 |
| Coronary artery disease | 19 (5.2) | 6 (8.3) | 13 (4.4) | 0.229 |
| Hypertension | 137 (37.2) | 33 (45.8) | 104 (35.1) | 0.092 |
| Valvular disease | 3 (0.8) | 1 (1.4) | 2 (0.7) | 0.481 |
| Stroke | 33 (9.0) | 5 (6.9) | 28 (9.5) | 0.503 |
| Transient ischemic attack | 3 (0.8) | 0 (0.0) | 3 (1.0) | 1.000 |
| Diabetes mellitus | 124 (33.7) | 27 (37.5) | 97 (32.8) | 0.446 |
| Chronic kidney disease | 18 (4.9) | 3 (4.2) | 15 (5.1) | 1.000 |
| Active smoking | 28 (7.6) | 5 (6.9) | 23 (7.8) | 0.323 |
| Thrombophilia | 13 (3.5) | 3 (4.2) | 10 (3.4) | 0.419 |
| Active cancer | 12 (3.3) | 5 (6.9) | 7 (2.4) | 0.061 |
| On chemotherapy (among patients with cancer) | 5 (41.7) | 2 (40.0) | 3 (42.9) | 1.000 |
| History of MB (within 12 months) | 22 (6.0) | 8 (11.1) | 14 (4.7) | 0.058 |
| History of CRNMB (within 12 months) | 11 (3.0) | 1 (1.4) | 10 (3.4) | 0.698 |
| History of any bleeding (within 12 months) | 8 (2.2) | 2 (2.8) | 6 (2.0) | 0.651 |
| Concomitant antithrombotic medications | ||||
| Aspirin | 54 (14.7) | 9 (12.5) | 45 (15.2) | 0.547 |
| P2Y12 Inhibitors | 10 (2.7) | 3 (4.2) | 7 (2.4) | 0.623 |
| Risk Factors for VTE recurrence | ||||
| History of previous VTE | 39 (10.6) | 4 (5.6) | 35 (11.8) | 0.119 |
| Type of historical VTE | 0.0006 | |||
| DVT | 27 (69.2) | 0 (0.0) | 27 (0.8) | --- |
| PE | 9 (23.1) | 4 (100) | 5 (14.3) | 0.638 |
| DVT plus PE | 3 (7.7) | 0 (0.0) | 3 (8.6) | |
| Time of historical VTE | 0.258 | |||
| Within 3 months | 3 (7.7) | 0 (0.0) | 3 (8.6) | |
| Within 12 months | 2 (5.1) | 0 (0.0) | 2 (5.7) | |
| Within >12 months | 32 (82.1) | 3 (75.0) | 29 (82.9) | |
| Use of oral contraceptive or ERT | 43 (11.7) | 5 (6.9) | 38 (12.8) | 0.148 |
| Obesity (BMI ≥ 30) | 181 (49.2) | 31 (43.1) | 150 (50.7) | 0.349 |
| Immobility | 83 (22.6) | 18 (25.0) | 65 (22.0) | 0.515 |
| Major general surgery (within one year) | 41 (11.1) | 11 (15.3) | 30 (10.1) | 0.254 |
| Time of major surgery | 0.550 | |||
| Within 3 months | 30 (73.2) | 7 (63.6) | 23 (76.7) | |
| Within 3–6 months | 3 (7.3) | 2 (18.2) | 1 (3.3) | |
| Within 6–12 months | 3 (7.3) | 1 (9.1) | 2 (6.7) | |
| Within >12 months | 4 (9.8) | 1 (9.1) | 3 (10.0) | |
| Orthopedic surgery (within one year) | 29 (7.9) | 8 (11.1) | 21 (7.1) | 0.282 |
| Time of orthopedic surgery | 0.622 | |||
| Within 3 months | 25 (86.2) | 8 (100.0) | 17 (81.0) | |
| Within 12 months | 2 (6.9) | 0 (0.0) | 2 (9.5) | |
| Within >12 months | 1 (3.4) | 0 (0.0) | 2 (9.5) | |
| Laboratory Values | Overall | Lead-in Group | p-Value | |
|---|---|---|---|---|
| Mixed | Recommended | |||
| Scr at lead-in dose initiation (mg/dL) | 0.8 ± 0.3 | 0.71 ± 0.2 | 0.77 ± 0.3 | 0.120 |
| eGFR at lead-in dose initiation (mL/min/1.73 m2) | 102.7 ± 46.8 | 115.4 ± 65.7 | 99.6 ± 40.5 | 0.009 |
| CrCl at lead-in dose initiation (ml/min) | 103.2 ± 50.0 | 109.7 ± 68.3 | 101.7 ± 44.5 | 0.223 |
| Hgb level before lead-in dose initiation (g/dL) | 12.5 ± 2.1 | 11.7 ± 2.2 | 12.7 ± 2.0 | <0.001 |
| Patient Characteristics | Overall | Lead-in Group | p-Value | |
|---|---|---|---|---|
| Mixed | Recommended | |||
| Overall number of patients | 368 | 72 | 296 | |
| Type of current VTE event | <0.001 | |||
| DVT | 151 (41.0) | 10 (13.9) | 141 (47.6) | 0.601 |
| Proximal | 109 (72.2) | 8 (80.0) | 101 (71.6) | |
| Distal | 14 (9.3) | 0 (0.0) | 14 (9.9) | |
| Mixed | 21 (13.9) | 2 (20.0) | 19 (13.5) | |
| Unspecified | 7 (4.6) | 0 (0.0) | 7 (5.0) | |
| PE | 188 (51.1) | 54 (75.0) | 134 (45.3) | 0.086 |
| Segmental | 68 (36.2) | 16 (29.6) | 52 (38.8) | |
| Subsegmental | 28 (14.9) | 5 (9.3) | 23 (17.2) | |
| Mixed | 58 (30.9) | 18 (33.3) | 40 (29.9) | |
| Unspecified | 34 (18.1) | 15 (27.8) | 19 (14.2) | |
| DVT plus PE | 29 (7.9) | 8 (11.1) | 21 (7.1) | |
| DVT type | 0.562 | |||
| Proximal | 12 (41.4) | 3 (37.5) | 9 (42.9) | |
| Distal | 6 (20.7) | 1 (12.5) | 5 (23.8) | |
| Mixed | 5 (17.2) | 1 (12.5) | 4 (19.0) | |
| Unspecified | 6 (20.7) | 3 (37.5) | 3 (14.3) | |
| PE type | 0.468 | |||
| Segmental | 11 (37.9) | 3 (37.5) | 8 (38.1) | |
| Subsegmental | 2 (6.9) | 1 (12.5) | 1 (4.8) | |
| Mixed | 9 (31.1) | 1 (12.5) | 8 (38.1) | |
| Unspecified | 7 (24.1) | 3 (37.5) | 4 (19.0) | |
| VTE Etiology | 0.694 | |||
| Provoked | 203 (55.2) | 37 (51.4) | 166 (56.1) | |
| Unprovoked | 81 (22.0) | 16 (22.2) | 65 (22.0) | |
| Not reported | 84 (22.8) | 19 (26.4) | 65 (22.0) | |
| Bleeding Risk a | 0.297 | |||
| High risk | 11 (3.0) | 4 (5.6) | 7 (2.4) | |
| Intermediate risk | 283 (76.9) | 52 (72.2) | 231 (78.0) | |
| Low risk | 74 (20.1) | 16 (22.2) | 58 (19.6) | |
| Patient Status | Overall | Apixaban | Rivaroxaban |
|---|---|---|---|
| Overall number of patients | 368 | 176 | 192 |
| Recommended-lead-in dosing group | 296 | 149 | 147 |
| Type of parenteral anticoagulant used | |||
| LMWH (enoxaparin) | 168 (56.8) | 68 (45.6) | 100 (68.0) |
| UFH | 29 (9.8) | 22 (14.8) | 7 (4.8) |
| Fondaparinux | 1 (0.3) | 1 (0.7) | 0 (0.00) |
| None | 98 (33.1) | 58 (38.9) | 40 (27.2) |
| Duration for the received lead-in dose of DOAC (days) | 7.0 ± 0.0 | 21.0 ± 0.0 | |
| Duration for the received parenteral anticoagulant (days) | 1.3 ± 0.4 | 1.2 ± 0.4 | |
| Duration for the received parenteral anticoagulant and DOAC (days) | 8.3 ± 0.4 | 22.2 ± 0.4 | |
| Mixed-lead-in dosing group | 72 | 27 | 45 |
| Type of parenteral anticoagulant used | |||
| LMWH (enoxaparin) | 61 (84.7) | 21 (77.8) | 40 (88.9) |
| UFH | 11 (15.3) | 6 (22.2) | 5 (11.1) |
| Duration of the received lead-in dose of DOAC (days) | 4.0 ± 1.1 | 15.0 ± 3.1 | |
| Duration of the received parenteral anticoagulant (days) | 2.2 ± 1.4 | 5.6 ± 3.1 | |
| Duration of the received parenteral anticoagulant and DOAC (days) | 6.2 ± 0.8 | 20.7 ± 0.8 |
| Patient Characteristic | Overall | Lead-in Group | p-Value | |
|---|---|---|---|---|
| Mixed | Recommended | |||
| Overall number of patients | 368 | 72 | 296 | |
| rVTE event | ||||
| During hospitalization | 2 (0.5) | 0 (0.0) | 2 (0.7) | 1.000 |
| Within 30 days a | 2 (0.5) | 0 (0.0) | 2 (0.7) | 1.000 |
| Cumulative within 90 days b | 3 (0.8) | 1 (1.4) | 2 (0.7) | 0.481 |
| Patients with at least one rVTE within 90 days c | 5 (1.4) | 1 (1.4) | 4 (1.4) | 1.000 |
| MB event | ||||
| During hospitalization | 18 (4.9) | 7 (9.7) | 11 (3.7) | 0.060 |
| Within 30 days | 4 (1.1) | 0 (0.0) | 4 (1.4) | 1.000 |
| Cumulative within 90 days | 6 (1.6) | 1 (1.4) | 5 (1.7) | 1.000 |
| Patients with at least one MB within 90 days | 21 (5.7) | 7 (9.7) | 14 (4.7) | 0.150 |
| CRNMB event | ||||
| During hospitalization | 12 (3.3) | 3 (4.2) | 9 (3.0) | 0.890 |
| Within 30 days | 27 (7.3) | 4 (5.6) | 23 (7.8) | 0.518 |
| Cumulative within 90 days | 27 (7.3) | 4 (5.6) | 23 (7.8) | 0.518 |
| Patients with at least one CRNMB within 90 days | 36 (9.8) | 7 (9.7) | 29 (9.8) | 0.984 |
| Rehospitalization d | ||||
| Within 30 days | 7 (1.9) | 0 (0.0) | 7 (2.4) | 0.353 |
| Cumulative within 90 days | 15 (4.1) | 2 (2.8) | 13 (4.4) | 0.745 |
| Death during hospitalization | 0 (0.0) | 0 (0.0) | 0 (0.0) | --- |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Alshaya, O.A.; Korayem, G.B.; Al Yami, M.S.; Qudayr, A.H.; Althewaibi, S.; Fetyani, L.; Alshehri, S.; Alnashmi, F.; Albasseet, M.; Alshehri, L.; et al. Comparative Effectiveness of Apixaban and Rivaroxaban Lead-in Dosing in VTE Treatment: Observational Multicenter Real-World Study. J. Clin. Med. 2023, 12, 199. https://doi.org/10.3390/jcm12010199
Alshaya OA, Korayem GB, Al Yami MS, Qudayr AH, Althewaibi S, Fetyani L, Alshehri S, Alnashmi F, Albasseet M, Alshehri L, et al. Comparative Effectiveness of Apixaban and Rivaroxaban Lead-in Dosing in VTE Treatment: Observational Multicenter Real-World Study. Journal of Clinical Medicine. 2023; 12(1):199. https://doi.org/10.3390/jcm12010199
Chicago/Turabian StyleAlshaya, Omar A., Ghazwa B. Korayem, Majed S. Al Yami, Asma H. Qudayr, Sara Althewaibi, Lolwa Fetyani, Shaden Alshehri, Fai Alnashmi, Maram Albasseet, Lina Alshehri, and et al. 2023. "Comparative Effectiveness of Apixaban and Rivaroxaban Lead-in Dosing in VTE Treatment: Observational Multicenter Real-World Study" Journal of Clinical Medicine 12, no. 1: 199. https://doi.org/10.3390/jcm12010199
APA StyleAlshaya, O. A., Korayem, G. B., Al Yami, M. S., Qudayr, A. H., Althewaibi, S., Fetyani, L., Alshehri, S., Alnashmi, F., Albasseet, M., Alshehri, L., Alhushan, L. M., & Almohammed, O. A. (2023). Comparative Effectiveness of Apixaban and Rivaroxaban Lead-in Dosing in VTE Treatment: Observational Multicenter Real-World Study. Journal of Clinical Medicine, 12(1), 199. https://doi.org/10.3390/jcm12010199