
Clinical Characteristics, Risk Factors for Severity and Pharmacotherapy in Hospitalized COVID-19 Patients in the United Arab Emirates

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Population and Setting
2.2. Severity of COVID-19
2.3. Data Collection
2.4. Statistical Analysis
2.5. Ethics
3. Results
3.1. Socio-Demographic and Clinical Characteristics
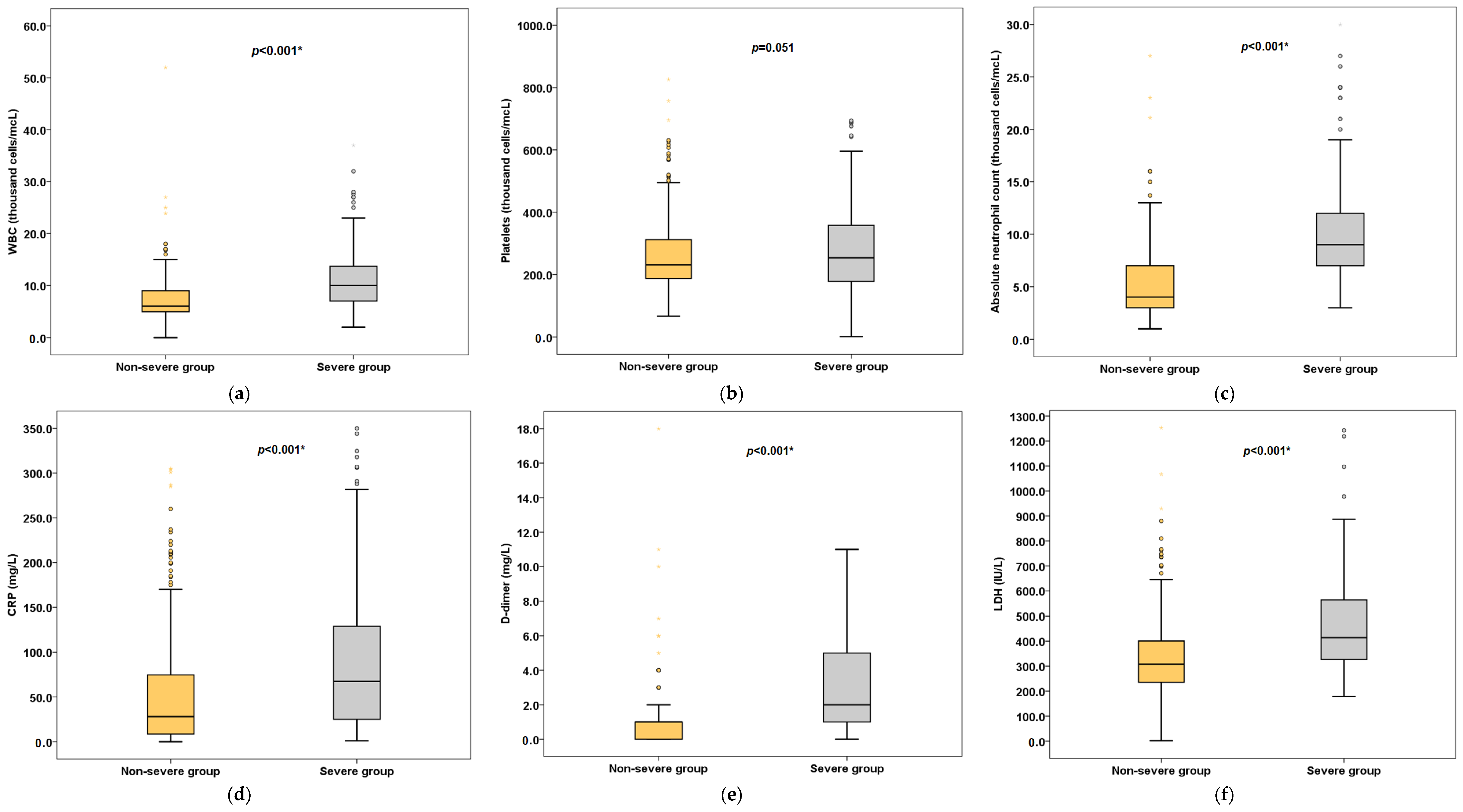
3.2. Vitals and Laboratory Characteristics
3.3. Risk Factors for Severity of Disease
3.4. Pharmacotherapy for COVID-19 Patients
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhu, N.; Zhang, D.; Wang, W.; Li, X.; Yang, B.; Song, J.; Zhao, X.; Huang, B.; Shi, W.; Lu, R.; et al. A Novel Coronavirus from Patients with Pneumonia in China. N. Engl. J. Med. 2020, 382, 727–733. [Google Scholar] [CrossRef]
- Johns Hopkins University and Medicine Coronavirus Resource Center–Global. Available online: https://coronavirus.jhu.edu/ (accessed on 24 October 2021).
- Johns Hopkins University and Medicine Coronavirus Resource Center–United Arab Emirates. Available online: https://coronavirus.jhu.edu/region/united-arab-emirates (accessed on 24 October 2021).
- Wiersinga, W.J.; Rhodes, A.; Cheng, A.C.; Peacock, S.J.; Prescott, H.C. Pathophysiology, Transmission, Diagnosis, and Treatment of Coronavirus Disease 2019 (COVID-19): A Review. JAMA J. Am. Med. Assoc. 2020, 324, 782–793. [Google Scholar] [CrossRef] [PubMed]
- Guan, W.J.; Ni, Z.Y.; Hu, Y.; Liang, W.H.; Ou, C.Q.; He, J.X.; Liu, L.; Shan, H.; Lei, C.L.; Hui, D.S.C.; et al. Clinical Characteristics of Coronavirus Disease 2019 in China. N. Engl. J. Med. 2020, 382, 1708–1720. [Google Scholar] [CrossRef] [PubMed]
- Li, Q.; Guan, X.; Wu, P.; Wang, X.; Zhou, L.; Tong, Y.; Ren, R.; Leung, K.S.M.; Lau, E.H.Y.; Wong, J.Y.; et al. Early Transmission Dynamics in Wuhan, China, of Novel Coronavirus-Infected Pneumonia. N. Engl. J. Med. 2020, 382, 1199–1207. [Google Scholar] [CrossRef] [PubMed]
- Xie, Y.; Wang, Z.; Liao, H.; Marley, G.; Wu, D.; Tang, W. Epidemiologic, Clinical, and Laboratory Findings of the COVID-19 in the Current Pandemic: Systematic Review and Meta-Analysis. BMC Infect. Dis. 2020, 20, 640. [Google Scholar] [CrossRef] [PubMed]
- da Rosa Mesquita, R.; Francelino Silva, L.C.; Santos Santana, F.M.; Farias de Oliveira, T.; Campos Alcântara, R.; Monteiro Arnozo, G.; Rodrigues da Silva Filho, E.; Galdino dos Santos, A.G.; Oliveira da Cunha, E.J.; Salgueiro de Aquino, S.H.; et al. Clinical Manifestations of COVID-19 in the General Population: Systematic Review. Wien Klin. Wochenschr. 2021, 133, 377–382. [Google Scholar] [CrossRef] [PubMed]
- Different COVID-19 Vaccines|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/vaccines/different-vaccines.html (accessed on 25 October 2021).
- Vaccines against COVID-19 in the UAE–The Official Portal of the UAE Government. Available online: https://u.ae/en/information-and-services/justice-safety-and-the-law/handling-the-covid-19-outbreak/vaccines-against-covid-19-in-the-uae (accessed on 25 October 2021).
- Sanders, J.M.; Monogue, M.L.; Jodlowski, T.Z.; Cutrell, J.B. Pharmacologic Treatments for Coronavirus Disease 2019 (COVID-19): A Review. JAMA J. Am. Med. Assoc. 2020, 323, 1824–1836. [Google Scholar] [CrossRef]
- Centers for Disease Control and Prevention (CDC) Therapeutic Options for COVID-19 Patients|CDC. Available online: https://www.cdc.gov/coronavirus/2019-ncov/hcp/therapeutic-options.html (accessed on 25 October 2021).
- National Institutes of Health Therapeutic Management of Hospitalized Adults with COVID-19. Available online: https://www.covid19treatmentguidelines.nih.gov/management/clinical-management/hospitalized-adults--therapeutic-management/ (accessed on 29 September 2020).
- National Clinical Committee for COVID-19 Management. National Guidelines for Clinical Management and Treatment of COVID-19; Version 4; United Arab Emirates Ministry of Health: Dubai, United Arab Emirates, 2020; Volume 19, pp. 1–61. Available online: https://www.dha.gov.ae/en/HealthRegulation/Documents/National_Guidelines_of_COVID_19_1st_June_2020.pdf (accessed on 29 September 2020).
- Overview COVID-19 Rapid Guideline: Managing COVID-19. Available online: https://www.nice.org.uk/guidance/ng191 (accessed on 25 October 2021).
- World Health Organization Weekly Epidemiological Update on COVID-19. 5 October 2021. Available online: https://www.who.int/publications/m/item/weekly-epidemiological-update-on-covid-19---5-october-2021 (accessed on 15 October 2021).
- Reuters UAE’s Daily COVID-19 Cases Fall below 100. Available online: https://www.reuters.com/world/middle-east/uaes-daily-covid-19-cases-fall-below-100–2021–10–17/ (accessed on 20 October 2021).
- Wu, Z.; McGoogan, J.M. Characteristics of and Important Lessons from the Coronavirus Disease 2019 (COVID-19) Outbreak in China. JAMA 2020, 323, 1239. [Google Scholar] [CrossRef]
- Emirates News Agency UAE Continues to Lead in Global Rankings for COVID-19 Vaccination Rates: UAE Government Media Briefing. Available online: https://wam.ae/en/details/1395302980184 (accessed on 20 October 2021).
- Richardson, S.; Hirsch, J.S.; Narasimhan, M.; Crawford, J.M.; McGinn, T.; Davidson, K.W.; Barnaby, D.P.; Becker, L.B.; Chelico, J.D.; Cohen, S.L.; et al. Presenting Characteristics, Comorbidities, and Outcomes among 5700 Patients Hospitalized with COVID-19 in the New York City Area. JAMA J. Am. Med. Assoc. 2020, 323, 2052–2059. [Google Scholar] [CrossRef]
- Pijls, B.G.; Jolani, S.; Atherley, A.; Derckx, R.T.; Dijkstra, J.I.R.; Franssen, G.H.L.; Hendriks, S.; Richters, A.; Venemans-Jellema, A.; Zalpuri, S.; et al. Demographic Risk Factors for COVID-19 Infection, Severity, ICU Admission and Death: A Meta-Analysis of 59 Studies. BMJ Open 2021, 11, e044640. [Google Scholar] [CrossRef]
- Wang, D.; Hu, B.; Hu, C.; Zhu, F.; Liu, X.; Zhang, J.; Wang, B.; Xiang, H.; Cheng, Z.; Xiong, Y.; et al. Clinical Characteristics of 138 Hospitalized Patients With 2019 Novel Coronavirus–Infected Pneumonia in Wuhan, China. JAMA 2020, 323, 1061. [Google Scholar] [CrossRef] [PubMed]
- Peckham, H.; de Gruijter, N.M.; Raine, C.; Radziszewska, A.; Ciurtin, C.; Wedderburn, L.R.; Rosser, E.C.; Webb, K.; Deakin, C.T. Male Sex Identified by Global COVID-19 Meta-Analysis as a Risk Factor for Death and ITU Admission. Nat. Commun. 2020, 11, 6317. [Google Scholar] [CrossRef] [PubMed]
- Yang, X.; Yu, Y.; Xu, J.; Shu, H.; Xia, J.; Liu, H.; Wu, Y.; Zhang, L.; Yu, Z.; Fang, M.; et al. Clinical Course and Outcomes of Critically Ill Patients with SARS-CoV-2 Pneumonia in Wuhan, China: A Single-Centered, Retrospective, Observational Study. Lancet Respir. Med. 2020, 8, 475–481. [Google Scholar] [CrossRef] [Green Version]
- Xu, K.; Zhou, M.; Yang, D.; Ling, Y.; Liu, K.; Bai, T.; Cheng, Z.; Li, J. Application of Ordinal Logistic Regression Analysis to Identify the Determinants of Illness Severity of COVID-19 in China. Epidemiol. Infect. 2020, 148, e146. [Google Scholar] [CrossRef] [PubMed]
- Sun, F.; Kou, H.; Wang, S.; Lu, Y.; Zhao, H.; Li, W.; Zhou, Q.; Jiang, Q.; Cheng, Y.; Yang, K.; et al. An Analytical Study of Drug Utilization, Disease Progression, and Adverse Events among 165 COVID-19 Patients. Annu. Transl. Med. 2021, 9, 306. [Google Scholar] [CrossRef]
- Grasselli, G.; Zangrillo, A.; Zanella, A.; Antonelli, M.; Cabrini, L.; Castelli, A.; Cereda, D.; Coluccello, A.; Foti, G.; Fumagalli, R.; et al. Baseline Characteristics and Outcomes of 1591 Patients Infected with SARS-CoV-2 Admitted to ICUs of the Lombardy Region, Italy. JAMA J. Am. Med. Assoc. 2020, 323, 1574–1581. [Google Scholar] [CrossRef] [Green Version]
- Rawshani, A.; Kjölhede, E.A.; Rawshani, A.; Sattar, N.; Eeg-Olofsson, K.; Adiels, M.; Ludvigsson, J.; Lindh, M.; Gisslén, M.; Hagberg, E.; et al. Severe COVID-19 in People with Type 1 and Type 2 Diabetes in Sweden: A Nationwide Retrospective Cohort Study. Lancet Reg. Health Eur. 2021, 4, 100105. [Google Scholar] [CrossRef]
- Gregory, J.M.; Slaughter, J.C.; Duffus, S.H.; Smith, T.J.; LeStourgeon, L.M.; Jaser, S.S.; McCoy, A.B.; Luther, J.M.; Giovannetti, E.R.; Boeder, S.; et al. COVID-19 Severity Is Tripled in the Diabetes Community: A Prospective Analysis of the Pandemic’s Impact in Type 1 and Type 2 Diabetes. Diabetes Care 2021, 44, 526–532. [Google Scholar] [CrossRef]
- Wu, C.; Chen, X.; Cai, Y.; Xia, J.; Zhou, X.; Xu, S.; Huang, H.; Zhang, L.; Zhou, X.; Du, C.; et al. Risk Factors Associated with Acute Respiratory Distress Syndrome and Death in Patients with Coronavirus Disease 2019 Pneumonia in Wuhan, China. JAMA Intern. Med. 2020, 180, 934. [Google Scholar] [CrossRef] [Green Version]
- Zayet, S.; Kadiane-Oussou, N.J.; Lepiller, Q.; Zahra, H.; Royer, P.-Y.; Toko, L.; Gendrin, V.; Klopfenstein, T. Clinical Features of COVID-19 and Influenza: A Comparative Study on Nord Franche-Comte Cluster. Microbes Infect. 2020, 22, 481–488. [Google Scholar] [CrossRef]
- Islam, M.A.; Kundu, S.; Alam, S.S.; Hossan, T.; Kamal, M.A.; Hassan, R. Prevalence and Characteristics of Fever in Adult and Paediatric Patients with Coronavirus Disease 2019 (COVID-19): A Systematic Review and Meta-Analysis of 17515 Patients. PLoS ONE 2021, 16, e0249788. [Google Scholar] [CrossRef] [PubMed]
- Chew, N.W.; Ngiam, J.N.; Tham, S.M.; Lim, Z.Y.; Li, T.Y.W.; Cen, S.; Yap, E.S.; Tambyah, P.A.; Santosa, A.; Cross, G.B.; et al. Fever as a Predictor of Adverse Outcomes in COVID. QJM Int. J. Med. 2021, 114, 706–714. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Wang, H.; Liang, Z.; Peng, L.; Zhao, F.; Yang, L.; Cao, M.; Wu, W.; Jiang, X.; Zhang, P.; et al. Predicting Illness Severity and Short-Term Outcomes of COVID-19: A Retrospective Cohort Study in China. Innovation 2020, 1, 100007. [Google Scholar] [CrossRef] [PubMed]
- Zheng, Z.; Peng, F.; Xu, B.; Zhao, J.; Liu, H.; Peng, J.; Li, Q.; Jiang, C.; Zhou, Y.; Liu, S.; et al. Risk Factors of Critical & Mortal COVID-19 Cases: A Systematic Literature Review and Meta-Analysis. J. Infect. 2020, 81, e16–e25. [Google Scholar] [CrossRef]
- Kim, S.R.; Nam, S.H.; Kim, Y.R. Risk Factors on the Progression to Clinical Outcomes of COVID-19 Patients in South Korea: Using National Data. Int. J. Environ. Res. Public Health 2020, 17, 8847. [Google Scholar] [CrossRef]
- Liu, D.; Cui, P.; Zeng, S.; Wang, S.; Feng, X.; Xu, S.; Li, R.; Gao, Y.; Yu, R.; Wang, Y.; et al. Risk Factors for Developing into Critical COVID-19 Patients in Wuhan, China: A Multicenter, Retrospective, Cohort Study. EClinicalMedicine 2020, 25, 100471. [Google Scholar] [CrossRef]
- Hariyanto, T.I.; Kurniawan, A. Anemia Is Associated with Severe Coronavirus Disease 2019 (COVID-19) Infection. Transfus. Apher. Sci. 2020, 59, 102926. [Google Scholar] [CrossRef]
- Henry, B.; Cheruiyot, I.; Vikse, J.; Mutua, V.; Kipkorir, V.; Benoit, J.; Plebani, M.; Bragazzi, N.; Lippi, G. Lymphopenia and Neutrophilia at Admission Predicts Severity and Mortality in Patients with COVID-19: A Meta-Analysis. Acta Biomed. 2020, 91, e2020008. [Google Scholar] [CrossRef]
- Zong, X.; Gu, Y.; Yu, H.; Li, Z.; Wang, Y. Thrombocytopenia Is Associated with COVID-19 Severity and Outcome: An Updated Meta-Analysis of 5637 Patients with Multiple Outcomes. Lab. Med. 2021, 52, 10–15. [Google Scholar] [CrossRef]
- Simadibrata, D.M.; Calvin, J.; Wijaya, A.D.; Ibrahim, N.A.A. Neutrophil-to-Lymphocyte Ratio on Admission to Predict the Severity and Mortality of COVID-19 Patients: A Meta-Analysis. Am. J. Emerg. Med. 2021, 42, 60–69. [Google Scholar] [CrossRef]
- Cavalcante-Silva, L.H.A.; Carvalho, D.C.M.; Lima, É.A.; Galvão, J.G.F.M.; da Silva, J.S.F.; Sales-Neto, J.M.; Rodrigues-Mascarenhas, S. Neutrophils and COVID-19: The Road so Far. Int. Immunopharmacol. 2021, 90, 107233. [Google Scholar] [CrossRef] [PubMed]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y.Q.; Wang, Q.; Miao, H. Lymphopenia Predicts Disease Severity of COVID-19: A Descriptive and Predictive Study. Signal. Transduct. Target. Therapy 2020, 5, 33. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological Findings and Complications of COVID. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Zhang, Y.; Zheng, L.; Liu, L.; Zhao, M.; Xiao, J.; Zhao, Q. Liver Impairment in COVID-19 Patients: A Retrospective Analysis of 115 Cases from a Single Centre in Wuhan City, China. Liver Int. 2020, 40, 2095–2103. [Google Scholar] [CrossRef] [Green Version]
- Lei, F.; Liu, Y.; Zhou, F.; Qin, J.; Zhang, P.; Zhu, L.; Zhang, X.; Cai, J.; Lin, L.; Ouyang, S.; et al. Longitudinal Association Between Markers of Liver Injury and Mortality in COVID-19 in China. Hepatology 2020, 72, 389–398. [Google Scholar] [CrossRef]
- Parohan, M.; Yaghoubi, S.; Seraji, A. Liver Injury Is Associated with Severe Coronavirus Disease 2019 (COVID-19) Infection: A Systematic Review and Meta-analysis of Retrospective Studies. Hepatol. Res. 2020, 50, 924–935. [Google Scholar] [CrossRef]
- Tezcan, M.E.; Dogan Gokce, G.; Sen, N.; Zorlutuna Kaymak, N.; Ozer, R.S. Baseline Electrolyte Abnormalities Would Be Related to Poor Prognosis in Hospitalized Coronavirus Disease 2019 Patients. New Microbes New Infect. 2020, 37, 100753. [Google Scholar] [CrossRef]
- Moreno-Pérez, O.; Leon-Ramirez, J.M.; Fuertes-Kenneally, L.; Perdiguero, M.; Andres, M.; Garcia-Navarro, M.; Ruiz-Torregrosa, P.; Boix, V.; Gil, J.; Merino, E.; et al. Hypokalemia as a Sensitive Biomarker of Disease Severity and the Requirement for Invasive Mechanical Ventilation Requirement in COVID-19 Pneumonia: A Case Series of 306 Mediterranean Patients. Int. J. Infect. Dis. 2020, 100, 449–454. [Google Scholar] [CrossRef]
- Hachim, M.Y.; Hachim, I.Y.; Naeem, K.B.; Hannawi, H.; Salmi, I.A.; Hannawi, S. D-Dimer, Troponin, and Urea Level at Presentation With COVID-19 Can Predict ICU Admission: A Single Centered Study. Front. Med. 2020, 7, 585003. [Google Scholar] [CrossRef]
- Zeng, F.; Huang, Y.; Guo, Y.; Yin, M.; Chen, X.; Xiao, L.; Deng, G. Association of Inflammatory Markers with the Severity of COVID-19: A Meta-Analysis. Int. J. Infect. Dis. 2020, 96, 467–474. [Google Scholar] [CrossRef]
- Mahat, R.K.; Panda, S.; Rathore, V.; Swain, S.; Yadav, L.; Sah, S.P. The Dynamics of Inflammatory Markers in Coronavirus Disease-2019 (COVID-19) Patients: A Systematic Review and Meta-Analysis. Clin. Epidemiol. Glob. Health 2021, 11, 100727. [Google Scholar] [CrossRef] [PubMed]
- Deng, Y.; Liu, W.; Liu, K.; Fang, Y.Y.; Shang, J.; Zhou, L.; Wang, K.; Leng, F.; Wei, S.; Chen, L.; et al. Clinical Characteristics of Fatal and Recovered Cases of Coronavirus Disease 2019 in Wuhan, China: A Retrospective Study. Chin. Med. J. 2020, 133, 1261–1267. [Google Scholar] [CrossRef] [PubMed]
- Shi, L.; Wang, Y.; Wang, Y.; Duan, G.; Yang, H. An Updated Meta-analysis on the Relationship between D-dimer Levels and Severity of Coronavirus Disease. Int. J. Lab. Hematol. 2020, 42, e207–e210. [Google Scholar] [CrossRef]
- Henry, B.M.; Aggarwal, G.; Wong, J.; Benoit, S.; Vikse, J.; Plebani, M.; Lippi, G. Lactate Dehydrogenase Levels Predict Coronavirus Disease 2019 (COVID-19) Severity and Mortality: A Pooled Analysis. Am. J. Emerg. Med. 2020, 38, 1722–1726. [Google Scholar] [CrossRef] [PubMed]
- Al Harbi, M.; Al Kaabi, N.; Al Nuaimi, A.; Abdalla, J.; Khan, T.; Gasmelseed, H.; Khan, A.; Hamdoun, O.; Weber, S. Clinical and Laboratory Characteristics of Patients Hospitalised with COVID-19: Clinical Outcomes in Abu Dhabi, United Arab Emirates. BMC Infect. Dis. 2022, 22, 136. [Google Scholar] [CrossRef]
- Cai, Q.; Yang, M.; Liu, D.; Chen, J.; Shu, D.; Xia, J.; Liao, X.; Gu, Y.; Cai, Q.; Yang, Y.; et al. Experimental Treatment with Favipiravir for COVID-19: An Open-Label Control Study. Engineering 2020, 6, 1192–1198. [Google Scholar] [CrossRef]
- Chen, C.; Zhang, Y.; Huang, J.; Yin, P.; Cheng, Z.; Wu, J.; Chen, S.; Zhang, Y.; Chen, B.; Lu, M.; et al. Favipiravir Versus Arbidol for Clinical Recovery Rate in Moderate and Severe Adult COVID-19 Patients: A Prospective, Multicenter, Open-Label, Randomized Controlled Clinical Trial. Front. Pharmacol. 2021, 12, 683296. [Google Scholar] [CrossRef]
- Beigel, J.H.; Tomashek, K.M.; Dodd, L.E.; Mehta, A.K.; Zingman, B.S.; Kalil, A.C.; Hohmann, E.; Chu, H.Y.; Luetkemeyer, A.; Kline, S.; et al. Remdesivir for the Treatment of Covid-19–Final Report. N. Engl. J. Med. 2020, 383, 1813–1826. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Lim, W.S.; Emberson, J.R.; Mafham, M.; Bell, J.L.; Linsell, L.; Staplin, N.; Brightling, C.; Ustianowski, A.; et al. Dexamethasone in Hospitalized Patients with Covid. N. Engl. J. Med. 2021, 384, 693–704. [Google Scholar] [CrossRef]
- Lin, K.J.; Schneeweiss, S.; Tesfaye, H.; D’Andrea, E.; Liu, J.; Lii, J.; Murphy, S.N.; Gagne, J.J. Pharmacotherapy for Hospitalized Patients with COVID-19: Treatment Patterns by Disease Severity. Drugs 2020, 80, 1961–1972. [Google Scholar] [CrossRef]
- Alavi Darazam, I.; Shokouhi, S.; Pourhoseingholi, M.A.; Naghibi Irvani, S.S.; Mokhtari, M.; Shabani, M.; Amirdosara, M.; Torabinavid, P.; Golmohammadi, M.; Hashemi, S.; et al. Role of Interferon Therapy in Severe COVID-19: The COVIFERON Randomized Controlled Trial. Sci. Rep. 2021, 11, 8059. [Google Scholar] [CrossRef] [PubMed]
- Yu, J.; Lu, X.; Tong, L.; Shi, X.; Ma, J.; Lv, F.; Wu, J.; Pan, Q.; Yang, J.; Cao, H.; et al. Interferon-α-2b Aerosol Inhalation Is Associated with Improved Clinical Outcomes in Patients with Coronavirus Disease. Br. J. Clin. Pharmacol. 2021, 87, 4737–4746. [Google Scholar] [CrossRef] [PubMed]
- Pandit, A.; Bhalani, N.; Bhushan, B.L.S.; Koradia, P.; Gargiya, S.; Bhomia, V.; Kansagra, K. Efficacy and Safety of Pegylated Interferon Alfa-2b in Moderate COVID-19: A Phase II, Randomized, Controlled, Open-Label Study. Int. J. Infect. Dis. 2021, 105, 516–521. [Google Scholar] [CrossRef] [PubMed]
- Xu, X.; Han, M.; Li, T.; Sun, W.; Wang, D.; Fu, B.; Zhou, Y.; Zheng, X.; Yang, Y.; Li, X.; et al. Effective Treatment of Severe COVID-19 Patients with Tocilizumab. Proc. Natl. Acad. Sci. USA 2020, 117, 10970–10975. [Google Scholar] [CrossRef]
- RECOVERY Collaborative Group; Horby, P.; Mafham, M.; Linsell, L.; Bell, J.L.; Staplin, N.; Emberson, J.R.; Wiselka, M.; Ustianowski, A.; Elmahi, E.; et al. Effect of Hydroxychloroquine in Hospitalized Patients with Covid. N. Engl. J. Med. 2020, 383, 2030–2040. [Google Scholar] [CrossRef]
- Cavalcanti, A.B.; Zampieri, F.G.; Rosa, R.G.; Azevedo, L.C.P.; Veiga, V.C.; Avezum, A.; Damiani, L.P.; Marcadenti, A.; Kawano-Dourado, L.; Lisboa, T.; et al. Hydroxychloroquine with or without Azithromycin in Mild-to-Moderate Covid. N. Engl. J. Med. 2020, 383, 2041–2052. [Google Scholar] [CrossRef]
- Geleris, J.; Sun, Y.; Platt, J.; Zucker, J.; Baldwin, M.; Hripcsak, G.; Labella, A.; Manson, D.K.; Kubin, C.; Barr, R.G.; et al. Observational Study of Hydroxychloroquine in Hospitalized Patients with Covid. N. Engl. J. Med. 2020, 382, 2411–2418. [Google Scholar] [CrossRef]

{kind=link}
| Variables | All Patients (n = 585) | Severity of COVID-19 | p Value | |
|---|---|---|---|---|
| Non-Severe Group (n = 431) | Severe Group (n = 154) | |||
| Age, years, median (IQR) | 49.0 (39.0–59.0) | 48.0 (38.0–58.0) | 52.0 (42.6–65.0) | 0.006 |
| Age group, n (%) | 0.026 | |||
| ≤45 years | 234 (40.0) | 184 (42.7) | 50 (32.5) | |
| >45 years | 351 (60.0) | 247 (57.3) | 104 (67.5) | |
| Gender, n (%) | 0.001 | |||
| Female | 199 (34) | 163 (37.8) | 36 (23.4) | |
| Male | 386 (66) | 268 (62.2) | 118 (76.6) | |
| Ethnicity, n (%) | 0.97 | |||
| Arab | 191(32.6) | 149 (34.6) | 42 (27.3) | |
| Non-Arabs | 394 (67.4) | 282 (65.4) | 112 (72.7) | |
| Tobacco use, n (%) | 38 (6.5) | 29 (6.7) | 9 (5.8) | 0.893 |
| Alcohol use, n (%) | 26 (4.4) | 20 (4.6) | 6 (3.9) | 0.842 |
| BMI, kg/m2, median (IQR) | 28 (25–33) | 28 (25–32) | 29 (25–33.6) | 0.164 |
| Comorbidities, n (%) | ||||
| Diabetes | 234 (40) | 159 (36.9) | 75 (48.7) | 0.010 |
| Hypertension | 214 (36.6) | 150 (34.8) | 64 (41.6) | 0.135 |
| Obesity | 21 (3.6) | 13 (3) | 8 (5.2) | 0.212 |
| Cardiovascular disease | 119 (20.3) | 80 (18.6) | 39 (25.3) | 0.074 |
| Renal disease | 50 (8.5) | 31 (7.2) | 19 (12.3) | 0.050 |
| Respiratory disease | 33 (5.6) | 22 (5.1) | 11 (7.1) | 0.347 |
| Autoimmune disease | 5 (0.9) | 4 (0.9) | 1 (0.6) | 0.747 |
| Psychological disease | 15 (2.6) | 8 (1.9) | 7 (4.5) | 0.070 |
| Immunosuppression | 4 (0.7) | 3 (0.7) | 1 (0.6) | 0.952 |
| Others | 73 (12.5) | 58 (13.5) | 15 (9.7) | 0.231 |
| No. of comorbidities, median (IQR) | 1.0 (0.0–2.0) | 1.0 (0.0–2.0) | 1.0 (0.0–3.0) | 0.061 |
| No. of comorbidities, n (%) | 0.035 | |||
| None | 200 (34.2) | 157 (36.4) | 43 (27.9) | |
| One to two | 267 (45.6) | 197 (45.7) | 70 (45.5) | |
| More than two | 118 (20.2) | 77 (17.9) | 41 (26.6) | |
| Length of hospital stay, days, median (IQR) | 9.0 (6.0–14.0) | 8.0 (5.0–11.0) | 14.0 (10.0–20.0) | <0.001 |
| Length of hospital stay, n (%) | <0.001 | |||
| ≤7 days | 229 (39.1) | 206 (47.8) | 23 (14.9) | |
| >7 days | 356 (60.9) | 225 (52.2) | 131 (85.1) | |
| Signs and symptoms, n (%) | ||||
| Fever | 465 (79.5) | 321 (74.5) | 144 (93.5) | <0.001 |
| Pneumonia | 477 (81.5) | 324 (75.2) | 153 (99.4) | <0.001 |
| Cough | 417 (71.3) | 304 (70.5) | 113 (73.4) | 0.503 |
| Shortness of breath | 316 (54) | 181 (42) | 135 (87.7) | <0.001 |
| Dyspnea | 107 (18.3) | 60 (13.9) | 47 (30.5) | <0.001 |
| Fatigue | 62 (10.6) | 53 (12.3) | 9 (5.8) | 0.026 |
| Myalgia | 126 (21.5) | 100 (23.2) | 26 (16.9) | 0.102 |
| Rhinorrhea | 19 (3.2) | 17 (3.9) | 2 (1.3) | 0.112 |
| Sore throat | 50 (8.5) | 44 (10.2) | 6 (3.9) | 0.016 |
| Olfactory and taste disorder | 36 (6.2) | 32 (7.4) | 4 (2.6) | 0.032 |
| Chest pain | 67 (11.5) | 53 (12.3) | 14 (9.1) | 0.284 |
| Abdominal pain | 42 (7.2) | 38 (8.8) | 4 (2.6) | 0.010 |
| Diarrhea | 65 (11.1) | 57 (13.2) | 8 (5.2) | 0.006 |
| Nausea or vomiting | 80 (13.7) | 74 (17.2) | 6 (3.9) | <0.001 |
| Headache | 56 (9.6) | 49 (11.4) | 7 (4.5) | 0.013 |
| Chills | 16 (2.7) | 12 (2.8) | 4 (2.6) | 0.903 |
| Wheezing | 2 (0.3) | 2 (0.5) | 0 | 0.397 |
| Rigors | 1 (0.2) | 1 (0.2) | 0 | 0.550 |
| Others | 37 (6.3) | 30 (7) | 7 (4.5) | 0.291 |
| Variable | Severity of COVID-19 | p Value | |
|---|---|---|---|
| Non-Severe Group (n = 431) | Severe Group (n = 154) | ||
| Temperature (°C) | 0.004 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 37 (37–38) | 37 (37–38) | |
| Oxygen saturation (%) | 0.158 | ||
| Sample size | 312 | 145 | |
| Median (IQR) | 97 (95–98) | 96 (91.5–98) | |
| Respiratory rate (breaths/min) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 18 (18–22) | 24 (20–30) | |
| Heart rate (beats/min) | 0.863 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 88 (78–102) | 88.5 (70–105) | |
| Systolic blood pressure (mmHg) | 0.311 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 129 (116–144) | 131 (114.75–145) | |
| Diastolic blood pressure (mmHg) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 78 (68–87) | 73 (64–83.25) | |
| Laboratory parameters | |||
| Red blood count (×106/mcL) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 5 (4–5) | 4 (4–5) | |
| Hemoglobin (gm/dL) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 14 (12–15) | 11.9 (10–13.1) | |
| White blood count (×103/mcL) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 6 (5–9) | 10 (7–13.8) | |
| Absolute count | |||
| Neutrophils (×103/mcL) | <0.001 | ||
| Sample size | 428 | 153 | |
| Median (IQR) | 4 (3–7) | 9 (7–12) | |
| Lymphocytes (×103/mcL) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 1 (1–2) | 1 (1–1) | |
| Platelet count (×103/mcL) | 0.051 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 231 (187–313) | 254 (177–359) | |
| Sodium (mmol/L) | 0.005 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 137 (134–139) | 138 (136–141) | |
| Potassium (mmol/L) | 0.131 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 4 (4–4) | 4 (4–5) | |
| Calcium (mmol/L) | 0.067 | ||
| Sample size | 427 | 152 | |
| Median (IQR) | 2 (2–2) | 2 (2–2) | |
| Magnesium (mmol/L) | 0.626 | ||
| Sample size | 430 | 153 | |
| Median (IQR) | 1 (1–1) | 1 (1–1) | |
| Chloride (mmol/L) | 0.029 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 101 (99–103) | 102 (99–105) | |
| Urea (mmol/L) | <0.001 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 4.1 (3–7) | 9 (5–14) | |
| Serum creatinine (umol/L) | 0.28 | ||
| Sample size | 431 | 154 | |
| Median (IQR) | 81 (68–98) | 89.5 (68–148.75) | |
| Uric acid (umol/L) | 0.707 | ||
| Sample size | 430 | 154 | |
| Median (IQR) | 233 (168–312) | 225.5 (145–303) | |
| Aspartate aminotransferase (IU/L) | 0.001 | ||
| Sample size | 430 | 154 | |
| Median (IQR) | 39 (26–54) | 50 (30–86) | |
| Alanine aminotransferase (IU/L) | <0.001 | ||
| Sample size | 430 | 154 | |
| Median (IQR) | 44 (44–75.2) | 54.5 (35–96.5) | |
| Albumin (gm/L) | <0.001 | ||
| Sample size | 430 | 154 | |
| Median (IQR) | 32 (27–36) | 23 (19.75–28) | |
| Total protein (gm/L) | <0.001 | ||
| Sample size | 429 | 154 | |
| Median (IQR) | 74 (70–79) | 63 (56–72) | |
| Total bilirubin (umol/L) | 0.010 | ||
| Sample size | 430 | 154 | |
| Median (IQR) | 8 (6–12) | 9 (7–15) | |
| Prothrombin time (seconds) | <0.001 | ||
| Sample size | 419 | 150 | |
| Median (IQR) | 12 (11–13) | 13 (12–14) | |
| Partial thromboplastin time (seconds) | 0.001 | ||
| Sample size | 414 | 148 | |
| Median (IQR) | 34 (30–39) | 37 (31–46.75) | |
| International normalized ratio (seconds) | <0.001 | ||
| Sample size | 422 | 149 | |
| Median (IQR) | 1 (1–1) | 1 (1–1) | |
| Blood glucose (mmol/L) | 0.002 | ||
| Sample size | 428 | 154 | |
| Median (IQR) | 7 (6–10) | 8 (6–11) | |
| HbA1C (%) | 0.26 | ||
| Sample size | 369 | 91 | |
| Median (IQR) | 6 (6–8) | 7 (6–9) | |
| Creatine kinase (IU/L) | 0.001 | ||
| Sample size | 378 | 118 | |
| Median (IQR) | 106.5 (61–197.5) | 153 (76–407.75) | |
| Creatine kinase-MB (mcg/L) | <0.001 | ||
| Sample size | 329 | 81 | |
| Median (IQR) | 1 (0–1) | 1 (0.7–2) | |
| Troponin (ng/L) | 0.002 | ||
| Sample size | 394 | 137 | |
| Median (IQR) | 8 (5–17) | 11.18 (6.06–27.45) | |
| Brain-type natriuretic peptide (ng/L) | <0.001 | ||
| Sample size | 353 | 128 | |
| Median (IQR) | 71 (27–195) | 204.5 (60–892.75) | |
| Procalcitonin (ug/L) | <0.001 | ||
| Sample size | 417 | 151 | |
| Median (IQR) | 0 (0–0.02) | 2 (1–5) | |
| D-dimer (mg/L) | <0.001 | ||
| Sample size | 425 | 149 | |
| Median (IQR) | 1 (0–1) | 2 (1–5) | |
| Ferritin (ng/L) | <0.001 | ||
| Sample size | 428 | 146 | |
| Median (IQR) | 439.5 (179–869) | 673.5 (389.75–1489.5) | |
| C-reactive protein (mg/L) | <0.001 | ||
| Sample size | 430 | 154 | |
| Median (IQR) | 28 (8.45–74.7) | 67.5 (25–130.75) | |
| Lactate dehydrogenase (IU/L) | <0.001 | ||
| Sample size | 424 | 147 | |
| Median (IQR) | 308 (235.25–401) | 414 (324–565) | |
| Variable | Level | OR | B | 95% CI | p Value |
|---|---|---|---|---|---|
| Age, years | 1.026 | 0.025 | 1.013–1.039 | <0.001 | |
| Age, years | ≤45 | Ref | |||
| >45 | 1.549 | 0.438 | 1.052–2.283 | 0.027 | |
| Body Mass Index, kg/m2 | <25 | Ref | |||
| ≥25 | 1.052 | 0.051 | 0.676–1.637 | 0.821 | |
| Gender | Male | 1.994 | 0.690 | 1.309–3.037 | 0.001 |
| Female | Ref | ||||
| No. of comorbidities | 1.148 | 0.138 | 1.008–1.307 | 0.038 | |
| Number of comorbidities | ≤2 | Ref | |||
| >2 | 1.668 | 0.512 | 1.081–2.575 | 0.021 | |
| Type of comorbidities (No) | |||||
| Diabetes | Absent | Ref | |||
| Present | 1.624 | 0.485 | 1.120–2.355 | 0.011 | |
| Hypertension | Absent | Ref | |||
| Present | 1.332 | 0.287 | 0.914–1.942 | 0.136 | |
| Obesity | Absent | Ref | |||
| Present | 1.762 | 0.566 | 0.716–4.336 | 0.218 | |
| Cardiovascular disease | Absent | Ref | |||
| Present | 1.488 | 0.397 | 0.961–2.303 | 0.075 | |
| Renal disease | Absent | Ref | |||
| Present | 1.816 | 0.597 | 0.993–3.320 | 0.053 | |
| Respiratory disease | Absent | Ref | |||
| Present | 1.430 | 0.358 | 0.677–3.023 | 0.349 | |
| Autoimmune disease | Absent | Ref | |||
| Present | 0.698 | −0.360 | 0.077–6.291 | 0.748 | |
| Immunosuppression | Absent | Ref | |||
| Present | 0.932 | −0.070 | 0.096–9.032 | 0.932 | |
| Fever | Absent | Ref | |||
| Present | 4.935 | 1.596 | 2.509–9.707 | <0.001 | |
| Cough | Absent | Ref | |||
| Present | 1.151 | 0.141 | 0.762–1.740 | 0.503 | |
| Shortness of breath/Dyspnea | Absent | Ref | |||
| Present | 9.814 | 2.284 | 5.852–16.457 | <0.001 | |
| Fatigue | Absent | Ref | |||
| Present | 0.443 | −0.815 | 0.213–0.921 | 0.029 | |
| Myalgia | Absent | Ref | |||
| Present | 0.672 | −0.397 | 0.417–1.084 | 0.103 | |
| Sore throat | Absent | Ref | |||
| Present | 0.357 | −1.031 | 0.149–0.854 | 0.021 | |
| Chest pain | Absent | Ref | |||
| Present | 0.713 | −0.338 | 0.384–1.326 | 0.285 | |
| Nausea or vomiting | Absent | Ref | |||
| Present | 0.196 | −1.632 | 0.083–0.459 | <0.001 | |
| Headache | Absent | Ref | |||
| Present | 0.371 | −0.991 | 0.164–0.838 | 0.017 | |
| Red blood cells count (×106/mcL) | ≥4.5 | Ref | |||
| <4.5 | 4.807 | 1.570 | 3.244–7.122 | <0.001 | |
| Hemoglobin (gm/dL) | ≥13 | Ref | |||
| <13 | 4.124 | 1.417 | 2.789–6.097 | <0.001 | |
| White blood cells count (×103/mcL) | <4 | Ref | |||
| 4–11 | 1.282 | 0.249 | 0.621–2.645 | 0.501 | |
| >11 | 4.303 | 1.459 | 2.042–9.068 | <0.001 | |
| Neutrophils (×103/mcL) | <2 | Ref | |||
| 2–7 | 2.209 | 0.792 | 0.906–5.385 | 0.081 | |
| >7 | 10.085 | 2.311 | 4.205–24.188 | <0.001 | |
| Lymphocytes (×103/mcL) | <1 | 3.862 | 1.351 | 1.114–13.382 | 0.033 |
| 1–3 | 1.302 | 0.264 | 0.372–4.566 | 0.680 | |
| >3 | Ref | ||||
| Platelet count (×103/mcL) | <150 | 4.883 | 1.586 | 2.646–9.011 | <0.001 |
| 150–450 | 0.704 | −0.352 | 0.440–1.126 | 0.142 | |
| >450 | Ref | ||||
| Blood glucose (mmol/L) | <3.9 | Ref | |||
| 3.9–6.1 | 0.718 | −0.331 | 0.073–7.066 | 0.777 | |
| >6.1 | 1.350 | 0.300 | 0.139–13.127 | 0.796 | |
| HbA1C (%) | <4.8 | Ref | |||
| 4.8–6 | 0.133 | −2.015 | 0.010–1.804 | 0.130 | |
| >6 | 0.808 | −0.214 | 0.073–8.974 | 0.862 | |
| Sodium (mmol/L) | <135 | 23.011 | 3.136 | 6.715–78.847 | <0.001 |
| 135-145 | Ref | ||||
| >145 | 1.077 | 0.074 | 0.701–1.655 | 0.734 | |
| Potassium (mmol/L) | <3.6 | 7.717 | 2.043 | 3.782–15.748 | <0.001 |
| 3.6–5.1 | Ref | ||||
| >5.1 | 1.319 | 0.277 | 0.754–2.307 | 0.331 | |
| Calcium (mmol/L) | <2.6 | Ref | |||
| ≥2.6 | 0.938 | −0.064 | 0.187–4.698 | 0.938 | |
| Urea (mmol/L) | ≤6.5 | Ref | |||
| >6.5 | 5.222 | 1.653 | 3.517–7.754 | <0.001 | |
| Serum creatinine (umol/L) | ≤115 | Ref | |||
| >115 | 2.452 | 0.897 | 1.592–3.777 | <0.001 | |
| Aspartate aminotransferase (IU/L) | ≤37 | Ref | |||
| >37 | 1.592 | 0.465 | 1.082–2.342 | 0.018 | |
| Alanine aminotransferase (IU/L) | ≤63 | Ref | |||
| >63 | 1.602 | 0.471 | 1.096–2.342 | 0.015 | |
| Total bilirubin (umol/L) | ≤17 | Ref | |||
| >17 | 1.492 | 0.400 | 0.894–2.489 | 0.125 | |
| Prothrombin time (secs) | ≤12.3 | Ref | |||
| >12.3 | 3.602 | 1.281 | 2.442–5.312 | <0.001 | |
| Partial thromboplastin time (secs) | ≤37.7 | Ref | |||
| >37.7 | 2.161 | 0.770 | 1.476–3.163 | <0.001 | |
| International normalized ratio (secs) | ≤1.29 | Ref | |||
| >1.29 | 5.969 | 1.787 | 2.709–13.153 | <0.001 | |
| Creatine kinase (IU/L) | ≤308 | Ref | |||
| >308 | 2.144 | 0.763 | 1.318–3.488 | 0.002 | |
| Creatine kinase-MB (IU/L) | ≤3.6 | Ref | |||
| >3.6 | 2.945 | 1.080 | 2.001–4.334 | <0.001 | |
| Troponin (ng/L) | ≤60 | Ref | |||
| >60 | 2.313 | 0.839 | 1.549–3.454 | <0.001 | |
| Brain-type natriuretic peptide (ng/L) | ≤126 | Ref | |||
| >126 | 2.250 | 0.811 | 1.528–3.314 | <0.001 | |
| Procalcitonin (ug/L) | ≤0.10 | Ref | |||
| >0.10 | 3.981 | 1.381 | 2.663–5.951 | <0.001 | |
| D-dimer (mg/L) | ≤0.55 | Ref | |||
| >0.55 | 5.827 | 1.763 | 3.476–9.768 | <0.001 | |
| Ferritin (ng/mL) | ≤388 | Ref | |||
| >388 | 2.636 | 0.969 | 1.733–4.007 | <0.001 | |
| C-reactive protein (mg/L) | ≤3 | Ref | |||
| >3 | 5.067 | 1.623 | 1.999–12.849 | 0.001 | |
| Lactate dehydrogenase (IU/L) | ≤227 | Ref | |||
| >227 | 10.249 | 2.327 | 3.699–28.401 | <0.001 |
| Variable | Level | OR | B | 95% CI | p Value |
|---|---|---|---|---|---|
| Age, years | ≤45 | Ref | |||
| >45 | 2.070 | 0.728 | 1.035–4.141 | 0.040 | |
| Gender | Male | 3.151 | 1.148 | 1.524–6.515 | 0.002 |
| Female | Ref | ||||
| Number of comorbidities | ≤2 | Ref | |||
| >2 | 1.816 | 0.597 | 0.873–3.777 | 0.110 | |
| Type of comorbidities (No) | |||||
| Diabetes | Absent | Ref | |||
| Present | 0.624 | 0.152 | 0.634–2.139 | 0.624 | |
| Fever | Absent | Ref | |||
| Present | 3.681 | 1.303 | 1.340–10.112 | 0.011 | |
| Shortness of breath/Dyspnea | Absent | Ref | |||
| Present | 5.360 | 1.679 | 2.691–10.677 | <0.001 | |
| Fatigue | Absent | Ref | |||
| Present | 0.256 | −1.364 | 0.077–0.853 | 0.027 | |
| Sore throat | Absent | Ref | |||
| Present | 0.695 | −0.364 | 0.215–2.246 | 0.543 | |
| Nausea or vomiting | Absent | Ref | |||
| Present | 0.313 | −1.161 | 0.099–0.992 | 0.048 | |
| Headache | Absent | Ref | |||
| Present | 0.336 | −1.090 | 0.095–1.193 | 0.092 | |
| Red blood cells count (×106/mcL) | ≥4.5 | Ref | |||
| <4.5 | 1.690 | 0.524 | 0.828–3.450 | 0.150 | |
| Hemoglobin (gm/dL) | ≥13 | Ref | |||
| <13 | 3.170 | 1.154 | 1.511–6.650 | 0.002 | |
| White blood cells count (×103/mcL) | <4 | Ref | |||
| 4–11 | 0.813 | −0.207 | 0.248–2.664 | 0.733 | |
| >11 | 1.438 | 0.363 | 0.409–5.053 | 0.571 | |
| Neutrophils (×103/mcL) | <2 | Ref | |||
| 2–7 | 1.830 | 0.604 | 0.621–5.391 | 0.273 | |
| >7 | 4.894 | 1.588 | 1.666–14.373 | 0.004 | |
| Lymphocytes (×103/mcL) | <1 | 7.783 | 2.052 | 1.006–60.198 | 0.049 |
| 1–3 | 4.411 | 1.484 | 0.563–34.554 | 0.158 | |
| >3 | Ref | ||||
| Platelet count (×103/mcL) | <150 | 2.893 | 1.062 | 0.942–8.883 | 0.063 |
| 150–450 | 0.659 | −0.417 | 0.323–1.343 | 0.251 | |
| >450 | Ref | ||||
| Sodium (mmol/L) | <135 | 5.417 | 1.690 | 1.050–27.953 | 0.044 |
| 135–145 | Ref | ||||
| >145 | 1.147 | 0.137 | 0.596–2.208 | 0.682 | |
| Potassium (mmol/L) | <3.6 | 3.364 | 1.213 | 1.028–11.012 | 0.045 |
| 3.6–5.1 | Ref | ||||
| >5.1 | 1.159 | 0.148 | 0.478–2.811 | 0.744 | |
| Urea (mmol/L) | ≤6.5 | Ref | |||
| >6.5 | 3.368 | 1.214 | 1.687–6.726 | 0.001 | |
| Serum creatinine (umol/L) | ≤115 | Ref | |||
| >115 | 0.426 | −0.854 | 0.167–1.088 | 0.074 | |
| Aspartate aminotransferase (IU/L) | ≤37 | Ref | |||
| >37 | 1.171 | 0.158 | 0.601–2.283 | 0.643 | |
| Alanine aminotransferase (IU/L) | ≤63 | Ref | |||
| >63 | 0.782 | −0.245 | 0.404–1.517 | 0.467 | |
| Prothrombin time (secs) | ≤12.3 | Ref | |||
| >12.3 | 1.035 | 0.035 | 0.550–1.950 | 0.915 | |
| Partial thromboplastin time (secs) | ≤37.7 | Ref | |||
| >37.7 | 0.677 | −0.389 | 0.347–1.322 | 0.253 | |
| International normalized ratio (secs) | ≤1.29 | Ref | |||
| >1.29 | 1.100 | 0.096 | 0.259–4.680 | 0.897 | |
| Creatine kinase (IU/L) | ≤308 | Ref | |||
| >308 | 1.039 | 0.038 | 0.466–2.316 | 0.925 | |
| Creatine kinase-MB (IU/L) | ≤3.6 | Ref | |||
| >3.6 | 1.708 | 0.536 | 0.915–3.189 | 0.093 | |
| Troponin (ng/L) | ≤60 | Ref | |||
| > 60 | 1.117 | 0.111 | 0.541–2.305 | 0.765 | |
| Brain-type natriuretic peptide (ng/L) | ≤126 | Ref | |||
| >126 | 0.952 | −0.050 | 0.496–1.825 | 0.881 | |
| Procalcitonin (ug/L) | ≤0.10 | Ref | |||
| >0.10 | 1.379 | 0.321 | 0.671–2.833 | 0.382 | |
| D-dimer (mg/L) | ≤0.55 | Ref | |||
| >0.55 | 1.322 | 0.279 | 0.646–2.703 | 0.445 | |
| Ferritin (ng/mL) | ≤388 | Ref | |||
| >388 | 0.615 | −0.486 | 0.302–1.251 | 0.180 | |
| C-reactive protein (mg/L) | ≤3 | Ref | |||
| >3 | 0.999 | −0.001 | 0.271–3.690 | 0.999 | |
| Lactate dehydrogenase (IU/L) | ≤227 | Ref | |||
| >227 | 6.257 | 1.834 | 1.609–24.325 | 0.008 |
| Drugs | ATC | All Patients (n = 585) | Severity of COVID-19 | p Value | |
|---|---|---|---|---|---|
| Non-Severe Group (n = 431) | Severe Group (n = 154) | ||||
| Antivirals | 524 (89.6) | 375 (87) | 149 (96.8) | 0.001 | |
| Favipiravir | J05AX27 | 409 (69.9) | 278 (64.5) | 131 (85.1) | <0.001 |
| Lopinavir/Ritonavir | J05AR10 | 182 (31.1) | 143 (33.2) | 39 (25.3) | 0.071 |
| Remdesivir | J05AB16 | 50 (8.5) | 26 (6) | 24 (15.6) | <0.001 |
| Oseltamivir | J05AH02 | 3 (0.5) | 3 (0.7) | 0 (0.0) | 0.299 |
| Camostat mesylate | B02AB04 | 72 (12.3) | 42 (9.7) | 30 (19.5) | 0.002 |
| Corticosteroids | 358 (61.2) | 217 (50.3) | 141 (91.6) | <0.001 | |
| Dexamethasone | H02AB02 | 203 (34.7) | 122 (28.3) | 81 (52.6) | <0.001 |
| Methylprednisolone | H02AB04 | 181 (30.9) | 94 (21.8) | 87 (56.5) | <0.001 |
| Hydrocortisone | H02AB09 | 33 (5.6) | 12 (2.8) | 21 (13.6) | <0.001 |
| Prednisone | H02AB07 | 31 (5.3) | 24 (5.6) | 7 (4.5) | 0.627 |
| Betamethasone | H02AB01 | 1 (0.2) | 0 (0.0) | 1 (0.6) | 0.094 |
| Interleukin-6 Inhibitors | 8 (1.4%) | 2 (0.5%) | 6 (3.9%) | <0.001 | |
| Tocilizumab | L04AC07 | 11 (1.9) | 2 (0.5) | 9 (5.8) | <0.001 |
| Interferons | 183 (31.3) | 102 (23.7) | 81 (52.6) | <0.001 | |
| Interferon beta-1b | L03AB08 | 65 (11.1) | 34 (7.9) | 31 (20.1) | <0.001 |
| Interferon alfa-2b | L03AB05 | 115 (19.7) | 70 (16.2) | 45 (29.2) | 0.001 |
| Peginterferon alfa-2a | L03AB11 | 12 (2.1) | 4 (0.9) | 8 (5.2) | 0.001 |
| Cell-based therapy | 21 (3.6) | 15 (3.5) | 6 (3.9) | 0.812 | |
| Stem cells | B05AX04 | 21 (3.6) | 15 (3.5) | 6 (3.9) | 0.812 |
| Antimalarial drugs | 246 (42.1) | 194 (45) | 52 (33.8) | 0.015 | |
| Hydroxychloroquine | P01BA02 | 239 (40.9) | 190 (44.1) | 49 (31.8) | 0.008 |
| Chloroquine | P01BA01 | 41 (7) | 31 (7.2) | 10 (6.5) | 0.771 |
| Antiparasitic drugs | 61 (10.4) | 31 (7.2) | 30 (19.5) | <0.001 | |
| Ivermectin | P02CF01 | 61 (10.4) | 31 (7.2) | 30 (19.5) | <0.001 |
| Antibiotics | 377 (64.4) | 256 (60.1) | 118 (76.6) | <0.001 | |
| Azithromycin | J01FA10 | 78 (13.3) | 60 (13.9) | 18 (11.7) | 0.484 |
| Doxycycline | J01AA02 | 339 (57.9) | 231 (53.6) | 108 (70.1) | <0.001 |
| Anticoagulants | 562 (96.1) | 409 (94.9) | 153 (99.4) | 0.015 | |
| Enoxaparin | B01AB05 | 558 (95.4) | 406 (94.2) | 152 (98.7) | 0.022 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Almarashda, A.M.J.; Rabbani, S.A.; Kurian, M.T.; Cherian, A. Clinical Characteristics, Risk Factors for Severity and Pharmacotherapy in Hospitalized COVID-19 Patients in the United Arab Emirates. J. Clin. Med. 2022, 11, 2439. https://doi.org/10.3390/jcm11092439
Almarashda AMJ, Rabbani SA, Kurian MT, Cherian A. Clinical Characteristics, Risk Factors for Severity and Pharmacotherapy in Hospitalized COVID-19 Patients in the United Arab Emirates. Journal of Clinical Medicine. 2022; 11(9):2439. https://doi.org/10.3390/jcm11092439
Chicago/Turabian StyleAlmarashda, Amna Mohamed Juma, Syed Arman Rabbani, Martin Thomas Kurian, and Ajith Cherian. 2022. "Clinical Characteristics, Risk Factors for Severity and Pharmacotherapy in Hospitalized COVID-19 Patients in the United Arab Emirates" Journal of Clinical Medicine 11, no. 9: 2439. https://doi.org/10.3390/jcm11092439
APA StyleAlmarashda, A. M. J., Rabbani, S. A., Kurian, M. T., & Cherian, A. (2022). Clinical Characteristics, Risk Factors for Severity and Pharmacotherapy in Hospitalized COVID-19 Patients in the United Arab Emirates. Journal of Clinical Medicine, 11(9), 2439. https://doi.org/10.3390/jcm11092439