
Implementing a Multifaceted Intervention among Internal Medicine Residents with Audit and Educative Data Feedback Significantly Reduces Low-Value Care in Hospitalized Patients

 ,
,
Abstract
1. Introduction
2. Materials and Methods
2.1. Setting and Study Design
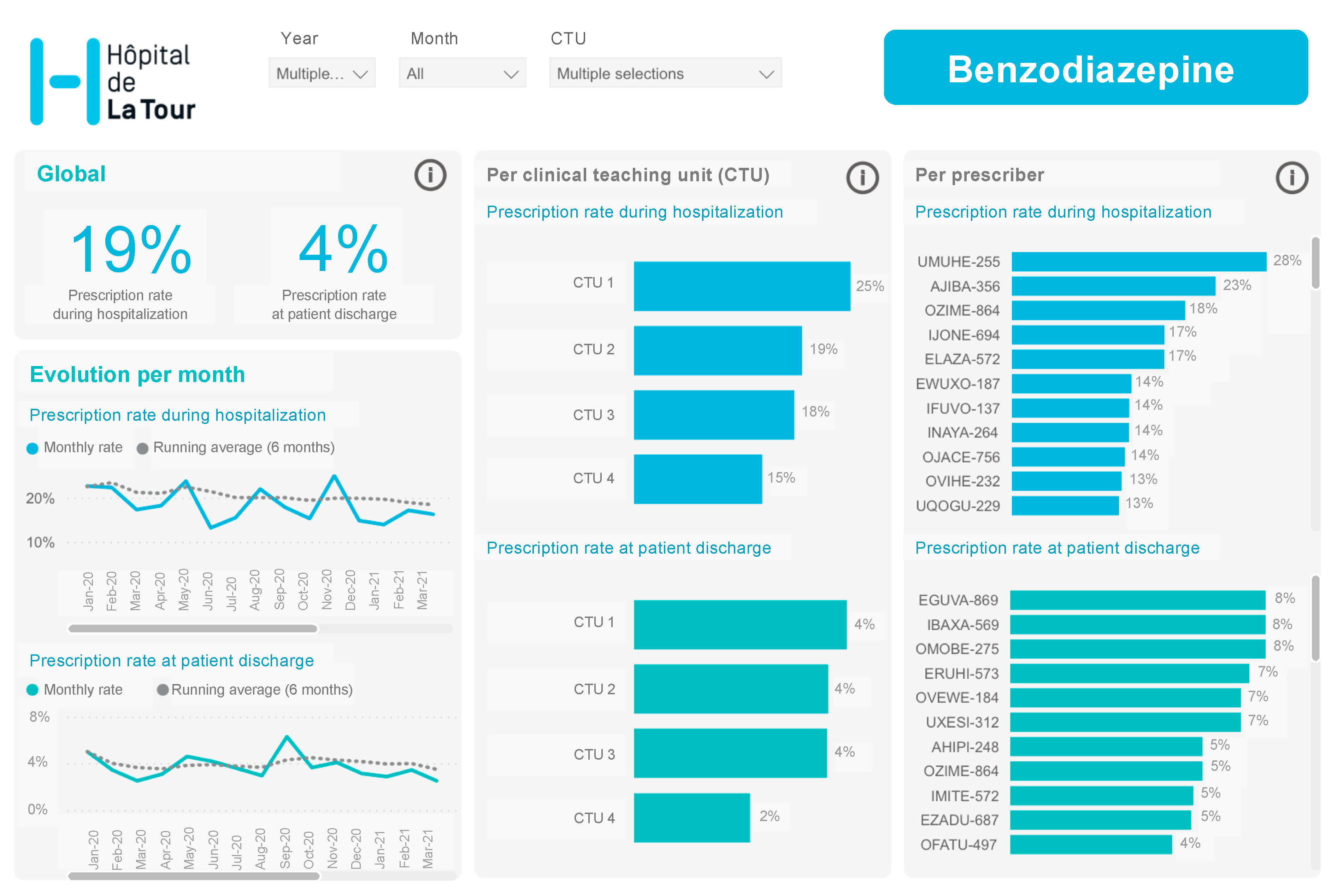
2.2. Intervention
2.3. Medical Tests, Procedures and Associated Costs
2.4. Safety Indicators
2.5. Data Extraction
2.6. Statistical Analyses
3. Results
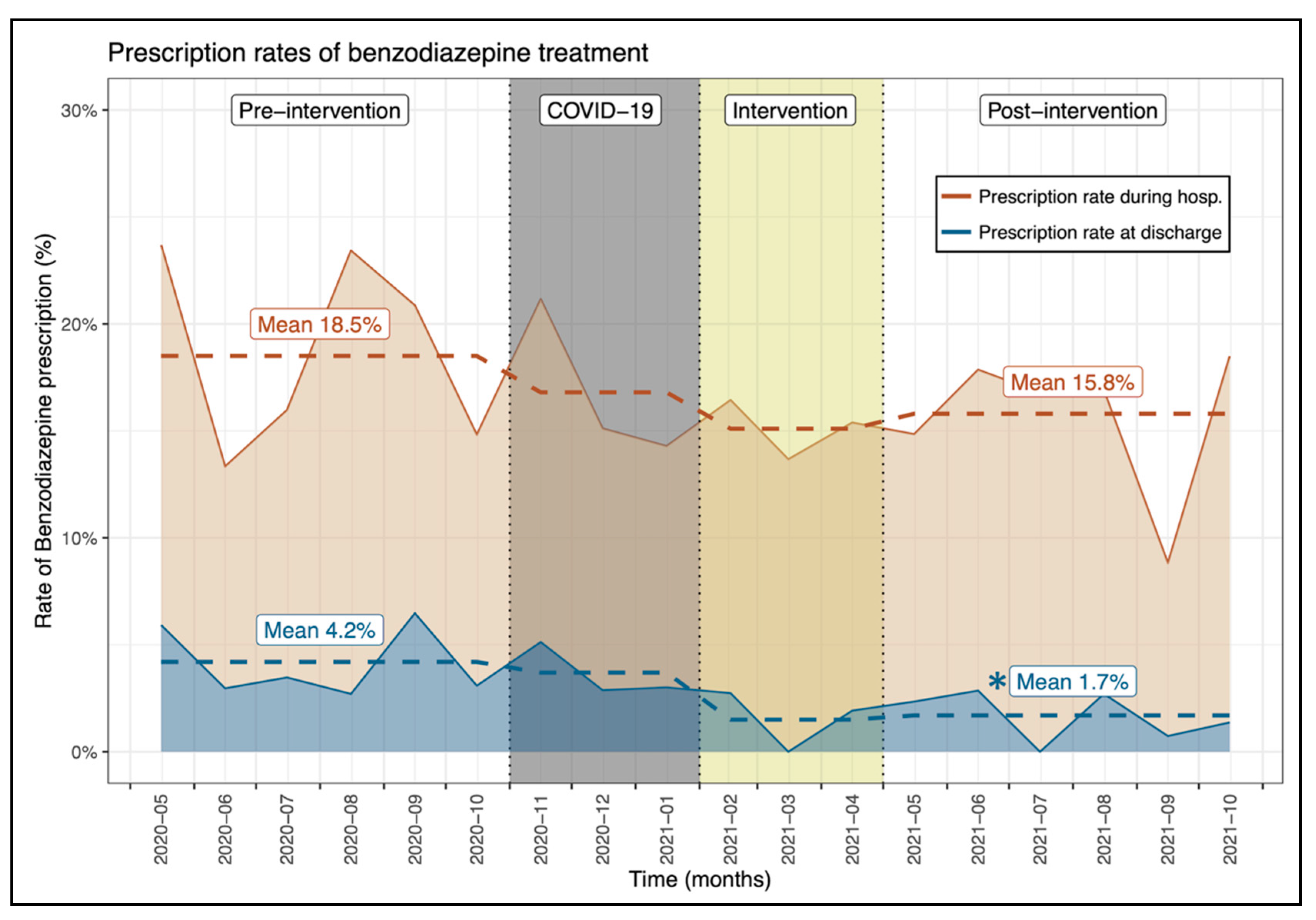
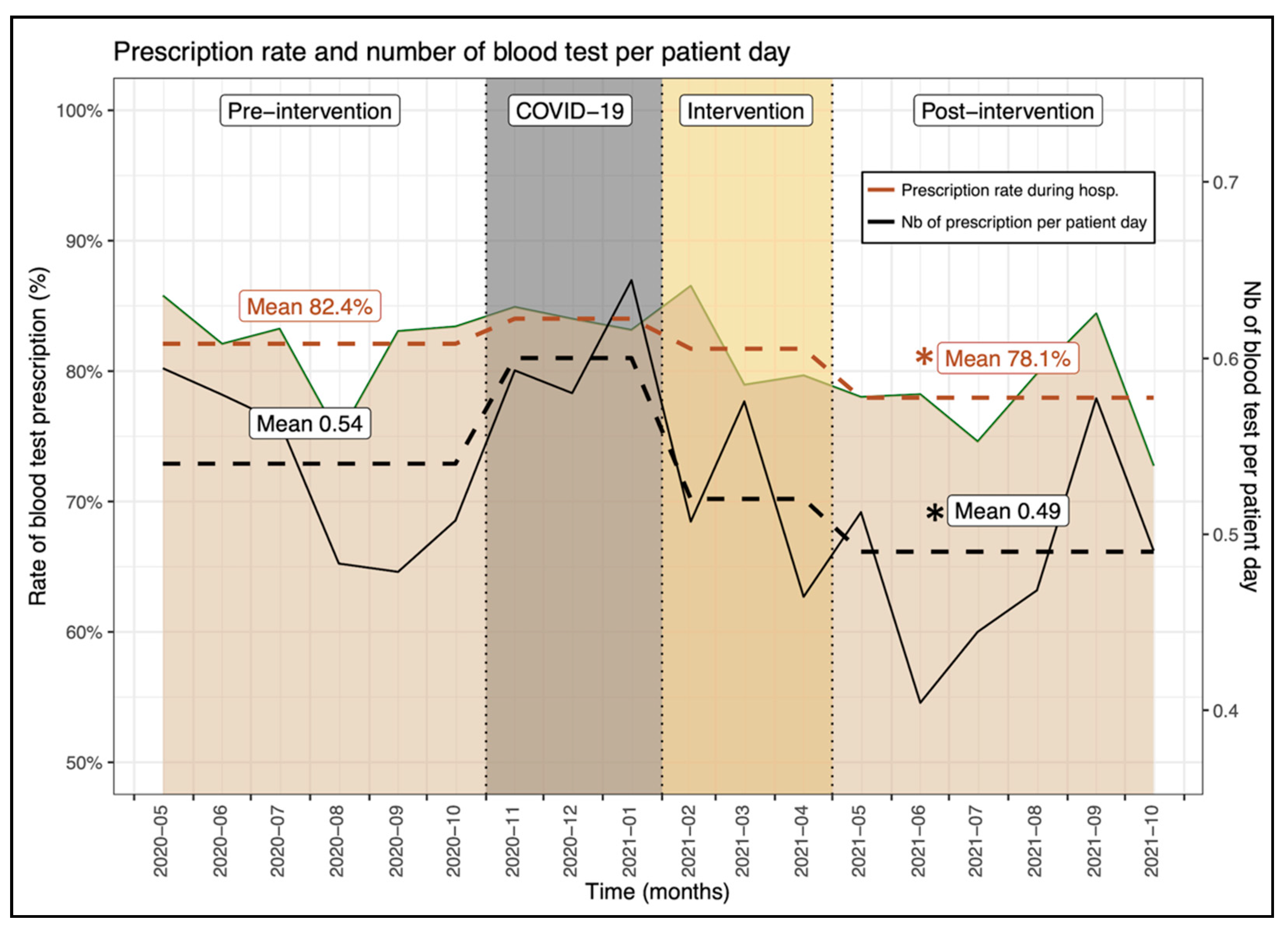
3.1. Intervention Effects during Hospitalization
3.2. Intervention Effects at Patient Discharge
3.3. Safety Endpoints
3.4. Intervention Effects on Laboratory Costs
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Born, K.B.; Levinson, W. Choosing Wisely campaigns globally: A shared approach to tackling the problem of overuse in healthcare. J. Gen. Fam. Med. 2019, 20, 9–12. [Google Scholar] [CrossRef] [PubMed]
- Levinson, W.; Born, K.; Wolfson, D. Choosing Wisely Campaigns: A Work in Progress. JAMA 2018, 319, 1975–1976. [Google Scholar] [CrossRef] [PubMed]
- Bavamian, S.; Gabutti, L.; Kherad, O.; Rodondi, N.; Rutishauser, J.; Waeber, G.; Meier, C.A. Vers une pratique en médecine interne hospitalière plus performante. Prim. Hosp. Care 2016, 16, 243–245. Available online: http://www.primary-care.ch/docs/primarycare/2016/13/fr/pc-f-01310.pdf (accessed on 9 March 2022).
- Available online: http://www.smartermedicine.ch (accessed on 7 February 2022).
- Wolfson, D.; Santa, J.; Slass, L. Engaging physicians and consumers in conversations about treatment overuse and waste: A short history of the choosing wisely campaign. Acad. Med. 2014, 89, 990–995. [Google Scholar] [CrossRef] [PubMed]
- Niven, D.J.; Mrklas, K.J.; Holodinsky, J.K.; Straus, S.E.; Hemmelgarn, B.R.; Jeffs, L.P.; Stelfox, H.T. Towards understanding the de-adoption of low-value clinical practices: A scoping review. BMC Med. 2015, 13, 255. [Google Scholar] [CrossRef]
- Bhatia, R.S.; Levinson, W.; Shortt, S.; Pendrith, C.; Fric-Shamji, E.; Kallewaard, M.; Peul, W.; Veillard, J.; Elshaug, A.; Forde, I.; et al. Measuring the effect of Choosing Wisely: An integrated framework to assess campaign impact on low-value care. BMJ Qual. Saf. 2015, 24, 523–531. [Google Scholar] [CrossRef] [PubMed]
- Kjelle, E.; Andersen, E.R.; Soril, L.J.J.; van Bodegom-Vos, L.; Hofmann, B.M. Interventions to reduce low-value imaging—A systematic review of interventions and outcomes. BMC Health Serv. Res. 2021, 21, 983. [Google Scholar] [CrossRef]
- Cliff, B.Q.; Avancena, A.L.V.; Hirth, R.A.; Lee, S.D. The Impact of Choosing Wisely Interventions on Low-Value Medical Services: A Systematic Review. Milbank Q. 2021, 99, 1024–1058. [Google Scholar] [CrossRef]
- Available online: https://www.acponline.org/clinical-information/high-value-care/medical-educators-resources/newly-revised-curriculum-for-educators-and-residents-version-40 (accessed on 9 March 2022).
- Mehra, T.; Muller, C.T.; Volbracht, J.; Seifert, B.; Moos, R. Predictors of High Profit and High Deficit Outliers under SwissDRG of a Tertiary Care Center. PLoS ONE 2015, 10, e0140874. [Google Scholar] [CrossRef]
- Halfon, P.; Eggli, Y.; Pretre-Rohrbach, I.; Meylan, D.; Marazzi, A.; Burnand, B. Validation of the potentially avoidable hospital readmission rate as a routine indicator of the quality of hospital care. Med. Care 2006, 44, 972–981. [Google Scholar] [CrossRef]
- Halfon, P.; Eggli, Y.; van Melle, G.; Chevalier, J.; Wasserfallen, J.B.; Burnand, B. Measuring potentially avoidable hospital readmissions. J. Clin. Epidemiol. 2002, 55, 573–587. [Google Scholar] [CrossRef]
- SQLape. Available online: https://www.sqlape.com/ (accessed on 9 March 2022).
- Winkelman, J.W. Insomnia Disorder. N. Engl. J. Med. 2015, 373, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Xing, D.; Ma, X.L.; Ma, J.X.; Wang, J.; Yang, Y.; Chen, Y. Association between use of benzodiazepines and risk of fractures: A meta-analysis. Osteoporos. Int. 2014, 25, 105–120. [Google Scholar] [CrossRef] [PubMed]
- Allain, H.; Bentue-Ferrer, D.; Polard, E.; Akwa, Y.; Patat, A. Postural instability and consequent falls and hip fractures associated with use of hypnotics in the elderly: A comparative review. Drugs Aging 2005, 22, 749–765. [Google Scholar] [CrossRef]
- Luta, X.; Bagnoud, C.; Lambiris, M.; Decollogny, A.; Eggli, Y.; Le Pogam, M.A.; Marques-Vidal, P.; Marti, J. Patterns of benzodiazepine prescription among older adults in Switzerland: A cross-sectional analysis of claims data. BMJ Open 2020, 10, e031156. [Google Scholar] [CrossRef] [PubMed]
- Schumacher, L.; Dobrinas, M.; Tagan, D.; Sautebin, A.; Blanc, A.L.; Widmer, N. Prescription of Sedative Drugs during Hospital Stay: A Swiss Prospective Study. Drugs Real World Outcomes 2017, 4, 225–234. [Google Scholar] [CrossRef][Green Version]
- Ribeiro, P.R.S.; Schlindwein, A.D. Benzodiazepine deprescription strategies in chronic users: A systematic review. Fam. Pract. 2021, 38, 684–693. [Google Scholar] [CrossRef]
- Salisbury, A.C.; Reid, K.J.; Alexander, K.P.; Masoudi, F.A.; Lai, S.M.; Chan, P.S.; Bach, R.G.; Wang, T.Y.; Spertus, J.A.; Kosiborod, M. Diagnostic blood loss from phlebotomy and hospital-acquired anemia during acute myocardial infarction. Arch. Intern. Med. 2011, 171, 1646–1653. [Google Scholar] [CrossRef]
- Thavendiranathan, P.; Bagai, A.; Ebidia, A.; Detsky, A.S.; Choudhry, N.K. Do blood tests cause anemia in hospitalized patients? The effect of diagnostic phlebotomy on hemoglobin and hematocrit levels. J. Gen. Intern. Med. 2005, 20, 520–524. [Google Scholar] [CrossRef]
- Koch, C.G.; Li, L.; Sun, Z.; Hixson, E.D.; Tang, A.; Phillips, S.C.; Blackstone, E.H.; Henderson, J.M. Hospital-acquired anemia: Prevalence, outcomes, and healthcare implications. J. Hosp. Med. 2013, 8, 506–512. [Google Scholar] [CrossRef]
- Thakkar, R.N.; Kim, D.; Knight, A.M.; Riedel, S.; Vaidya, D.; Wright, S.M. Impact of an educational intervention on the frequency of daily blood test orders for hospitalized patients. Am. J. Clin. Pathol. 2015, 143, 393–397. [Google Scholar] [CrossRef]
- Scarpignato, C.; Gatta, L.; Zullo, A.; Blandizzi, C.; SIF-ALGO-FIMMG Group; Italian Society of Pharmacology, The Italian Association of Hospital Gastroenterologist; The Italian Federation of General Practitioners. Effective and safe proton pump inhibitor therapy in acid-related diseases—A position paper addressing benefits and potential harms of acid suppression. BMC Med. 2016, 14, 179. [Google Scholar] [CrossRef] [PubMed]
- Lenoir, C.; El Biali, M.; Luthy, C.; Grosgurin, O.; Desmeules, J.A.; Rollason, V. Snapshot of proton pump inhibitors prescriptions in a tertiary care hospital in Switzerland: Less is more? Int. J. Clin. Pharm. 2019, 41, 1634–1641. [Google Scholar] [CrossRef] [PubMed]
- Born, K.; Kool, T.; Levinson, W. Reducing overuse in healthcare: Advancing Choosing Wisely. BMJ 2019, 367, l6317. [Google Scholar] [CrossRef] [PubMed]
- Cabana, M.D.; Rand, C.S.; Powe, N.R.; Wu, A.W.; Wilson, M.H.; Abboud, P.A.; Rubin, H.R. Why don’t physicians follow clinical practice guidelines? A framework for improvement. JAMA 1999, 282, 1458–1465. [Google Scholar] [CrossRef]
- Halpape, K.; Sulz, L.; Schuster, B.; Taylor, R. Audit and Feedback-Focused approach to Evidence-based Care in Treating patients with pneumonia in hospital (AFFECT Study). Can. J. Hosp. Pharm. 2014, 67, 17–27. [Google Scholar] [CrossRef]
- Meeker, D.; Linder, J.A.; Fox, C.R.; Friedberg, M.W.; Persell, S.D.; Goldstein, N.J.; Knight, T.K.; Hay, J.W.; Doctor, J.N. Effect of Behavioral Interventions on Inappropriate Antibiotic Prescribing among Primary Care Practices: A Randomized Clinical Trial. JAMA 2016, 315, 562–570. [Google Scholar] [CrossRef]
- Ambasta, A.; Ma, I.W.Y.; Woo, S.; Lonergan, K.; Mackay, E.; Williamson, T. Impact of an education and multilevel social comparison-based intervention bundle on use of routine blood tests in hospitalised patients at an academic tertiary care hospital: A controlled pre-intervention post-intervention study. BMJ Qual. Saf. 2020, 29, 1–2. [Google Scholar] [CrossRef]
- Iams, W.; Heck, J.; Kapp, M.; Leverenz, D.; Vella, M.; Szentirmai, E.; Valerio-Navarrete, I.; Theobald, C.; Goggins, K.; Flemmons, K.; et al. A Multidisciplinary Housestaff-Led Initiative to Safely Reduce Daily Laboratory Testing. Acad. Med. 2016, 91, 813–820. [Google Scholar] [CrossRef]
- Yarbrough, P.M.; Kukhareva, P.V.; Horton, D.; Edholm, K.; Kawamoto, K. Multifaceted intervention including education, rounding checklist implementation, cost feedback, and financial incentives reduces inpatient laboratory costs. J. Hosp. Med. 2016, 11, 348–354. [Google Scholar] [CrossRef]
- Yoong, S.L.; Hall, A.; Stacey, F.; Grady, A.; Sutherland, R.; Wyse, R.; Anderson, A.; Nathan, N.; Wolfenden, L. Nudge strategies to improve healthcare providers’ implementation of evidence-based guidelines, policies and practices: A systematic review of trials included within Cochrane systematic reviews. Implement. Sci. 2020, 15, 50. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, P.; Lang, E.; Mackenzie, M.; Hirandani, R.; Lys, R.; Laupacis, M.; Murray, H. CJEM Debate Series: #ChoosingWisely—The Choosing Wisely campaign will not impact physician behaviour and choices. Can. J. Emerg. Med. 2018, 20, 170–175. [Google Scholar] [CrossRef]
- Brehaut, J.C.; Colquhoun, H.L.; Eva, K.W.; Carroll, K.; Sales, A.; Michie, S.; Ivers, N.; Grimshaw, J.M. Practice Feedback Interventions: 15 Suggestions for Optimizing Effectiveness. Ann. Intern. Med. 2016, 164, 435–441. [Google Scholar] [CrossRef] [PubMed]
- Mehrotra, A.; Reid, R.O.; Adams, J.L.; Friedberg, M.W.; McGlynn, E.A.; Hussey, P.S. Physicians with the least experience have higher cost profiles than do physicians with the most experience. Health Aff. 2012, 31, 2453–2463. [Google Scholar] [CrossRef]
- Stammen, L.A.; Stalmeijer, R.E.; Paternotte, E.; Oudkerk Pool, A.; Driessen, E.W.; Scheele, F.; Stassen, L.P. Training Physicians to Provide High-Value, Cost-Conscious Care: A Systematic Review. JAMA 2015, 314, 2384–2400. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.; Petterson, S.; Phillips, R.; Bazemore, A.; Mullan, F. Spending patterns in region of residency training and subsequent expenditures for care provided by practicing physicians for Medicare beneficiaries. JAMA 2014, 312, 2385–2393. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
| Pre-Intervention Period (1095 Patients) | Post-Intervention Period (1155 Patients) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| N (%) | N(%) | ||||||
| ± SD | Med | (IQR) | ±SD | Med | (IQR) | ||
| Patient characteristics | |||||||
| Age | 74.1 ± 15.5 | 77.5 | (67.0–85.0) | 73.3 ± 15.9 | 77.0 | (65.0–84.0) | 0.231 * |
| PCCL | 1.7 ± 1.6 | 2.0 | (0.0–3.0) | 1.7 ± 1.5 | 2.0 | (0.0–3.0) | 0.688 * |
| Length of stay (days) | 8.9 ± 8.7 | 6.7 | (3.3–11.2) | 8.8 ± 7.5 | 7.0 | (3.9–11.2) | 0.291 * |
| Age ≥ 65 y.o | 843 (77.0) | 835 (72.3) | 0.185 | ||||
| Male sex | 577 (52.7) | 584 (50.6) | 0.312 | ||||
| During hospitalisation | |||||||
| Patients with prescription | |||||||
| Benzodiazepine (≥65 y.o) | 156 (18.5) | 132 (15.8) | 0.143 | ||||
| Proton Pump Inhibitor | 186 (17.0) | 188 (16.3) | 0.652 | ||||
| Blood test | 902 (83.1) | 902 (78.1) | 0.011 | ||||
| Phys. prescription rate (%) ⟟ | |||||||
| Benzodiazepine (≥65 y.o) | 15.4 ± 17.6 | 14.6 | (0.0–22.6) | 11.7 ± 11.8 | 12.5 | (0.0–19.1) | 0.623 ⋄ |
| Proton Pump Inhibitor | 14.6 ± 14.3 | 13.5 | (13.5–0.0) | 16.4 ± 20.6 | 15.8 | (0.0–21.3) | 0.384 ⋄ |
| Blood test | 82.1 ± 22.2 | 83.6 | (81.2–100.0) | 78.4 ± 21.1 | 80.8 | (80.8–72.3) | 0.035 ⋄ |
| Blood tests per patient day ** | 0.54 ± 0.43 | 0.42 | (0.26–0.69) | 0.49 ± 0.60 | 0.37 | (0.20–0.57) | <0.001 * |
| At patient discharge | |||||||
| Patients with prescription | |||||||
| Benzodiazepine (≥65 y.o) | 35 (4.2) | 14 (1.7) | 0.003 | ||||
| Proton Pump Inhibitor | 101 (9.2) | 108 (9.4) | 0.917 | ||||
| Phys. prescription rate (%) ⟟ | |||||||
| Benzodiazepine (≥65 y.o) | 4.0 ± 7.5 | 0.0 | (0.0–5.5) | 0.7 ± 2.1 | 0.0 | (0.0–0.0) | 0.025 ⋄ |
| Proton Pump Inhibitor | 8.6 ± 11.9 | 5.4 | (0.0–9.3) | 6.0 ± 6.2 | 5.7 | (0.0–9.3) | 0.394 ⋄ |
| Pre-Intervention (n = 1095 Patients) | Post-Intervention (n = 1155 Patients) | p-Value | |||||
|---|---|---|---|---|---|---|---|
| N (%) | N(%) | ||||||
| ± SD | Med | (IQR) | ± SD | Med | (IQR) | ||
| Pot. avoid. readmission | |||||||
| Eligible hospitalisations | 656 | 685 | |||||
| Readmission rate (%) | 41 (6.3%) | 36 (5.3%) | 0.434 | ||||
| Readmission delay (days) | 11.9 ± 10.1 | 8.0 | (3.0–21.0) | 14.3 ± 8.6 | 14.0 | (6.5–22.3) | 0.160 * |
| Premature deaths | |||||||
| Eligible hospitalisations | 992 | 1069 | |||||
| Death rate (%) | 24 (2.4%) | 22 (2.1%) | 0.579 | ||||
| Complications | |||||||
| Eligible hospitalisations | 1056 | 1133 | |||||
| Global complication score | 0.37 ± 1.17 | 0.00 | (0.00–0.00) | 0.30 ± 0.95 | 0.00 | (0.00–0.00) | 0.310 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Kherad, O.; Bottequin, E.; Steiner, D.; Alibert, A.; Eurin, R.; Bothorel, H. Implementing a Multifaceted Intervention among Internal Medicine Residents with Audit and Educative Data Feedback Significantly Reduces Low-Value Care in Hospitalized Patients. J. Clin. Med. 2022, 11, 2435. https://doi.org/10.3390/jcm11092435
Kherad O, Bottequin E, Steiner D, Alibert A, Eurin R, Bothorel H. Implementing a Multifaceted Intervention among Internal Medicine Residents with Audit and Educative Data Feedback Significantly Reduces Low-Value Care in Hospitalized Patients. Journal of Clinical Medicine. 2022; 11(9):2435. https://doi.org/10.3390/jcm11092435
Chicago/Turabian StyleKherad, Omar, Ezra Bottequin, Dorsaf Steiner, Axelle Alibert, Rodolphe Eurin, and Hugo Bothorel. 2022. "Implementing a Multifaceted Intervention among Internal Medicine Residents with Audit and Educative Data Feedback Significantly Reduces Low-Value Care in Hospitalized Patients" Journal of Clinical Medicine 11, no. 9: 2435. https://doi.org/10.3390/jcm11092435
APA StyleKherad, O., Bottequin, E., Steiner, D., Alibert, A., Eurin, R., & Bothorel, H. (2022). Implementing a Multifaceted Intervention among Internal Medicine Residents with Audit and Educative Data Feedback Significantly Reduces Low-Value Care in Hospitalized Patients. Journal of Clinical Medicine, 11(9), 2435. https://doi.org/10.3390/jcm11092435