
Effect of rLH Supplementation during Controlled Ovarian Stimulation for IVF: Evidence from a Retrospective Analysis of 1470 Poor/Suboptimal/Normal Responders Receiving Either rFSH plus rLH or rFSH Alone

 ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. COS Regimen
2.3. Oocyte Retrieval, Fertilization, Embryo Culture and Transfer
2.4. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Baird, D.T.; Collins, J.; Egozcue, J.; Evers, L.H.; Gianaroli, L.; Leridon, H.; Sunde, A.; Templeton, A.; Van Steirteghem, A.; Cohen, J.; et al. Fertility and ageing. Hum. Reprod. Update 2005, 11, 261–276. [Google Scholar] [PubMed] [Green Version]
- Alviggi, C.; Humaidan, P.; Howles, C.M.; Tredway, D.; Hillier, S.G. Biological versus chronological ovarian age: Implications for assisted reproductive technology. Reprod. Biol. Endocrinol. 2009, 7, 101. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Navot, D.; Bergh, P.A.; Williams, M.A.; Garrisi, G.J.; Guzman, I.; Sandler, B.; Grunfeld, L. Poor oocyte quality rather than implantation failure as a cause of age-related decline in female fertility. Lancet 1991, 337, 1375–1377. [Google Scholar] [CrossRef]
- Cimadomo, D.; Fabozzi, G.; Vaiarelli, A.; Ubaldi, N.; Ubaldi, F.M.; Rienzi, L. Impact of Maternal Age on Oocyte and Embryo Competence. Front. Endocrinol. 2018, 9, 327. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nelson, S.; Telfer, E.; Anderson, R.A. The ageing ovary and uterus: New biological insights. Hum. Reprod. Updat. 2013, 19, 67–83. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Davison, S.L.; Bell, R.; Donath, S.; Montalto, J.G.; Davis, S.R. Androgen Levels in Adult Females: Changes with Age, Menopause, and Oophorectomy. J. Clin. Endocrinol. Metab. 2005, 90, 3847–3853. [Google Scholar] [CrossRef] [PubMed]
- Marchiani, S.; Tamburrino, L.; Benini, F.; Pallecchi, M.; Bignozzi, C.; Conforti, A.; Alviggi, C.; Vignozzi, L.; Danza, G.; Pellegrini, S.; et al. LH supplementation of ovarian stimulation protocols influences follicular fluid steroid composition contributing to the improvement of ovarian response in poor responder women. Sci. Rep. 2020, 10, 12907. [Google Scholar] [CrossRef] [PubMed]
- Loumaye, E.; Engrand, P.; Shoham, Z.; Hillier, S.G.; Baird, D.T. Clinical evidence for an LH ’ceiling’ effect induced by administration of recombinant human LH during the late follicular phase of stimulated cycles in World Health Organization type I and type II anovulation. Hum. Reprod. 2003, 18, 314–322. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Filicori, M.; Cognigni, G.E.; Taraborrelli, S.; Spettoli, D.; Ciampaglia, W.; De Fatis, C.T.; Pocognoli, P.; Cantelli, B.; Boschi, S. Luteinzing hormone activity in menotropins optimizes folliculogenesis and treatment in controlled ovarian stimulation. J. Clin. Endocrinol. Metab. 2001, 86, 337–343. [Google Scholar] [CrossRef] [PubMed]
- Messinis, I.E.; Messini, C.I.; Dafopoulos, K. The role of gonadotropins in the follicular phase. Ann. N. Y. Acad. Sci. 2010, 1205, 5–11. [Google Scholar] [CrossRef]
- Palermo, R. Differential actions of FSH and LH during folliculogenesis. Reprod. Biomed. Online 2007, 15, 326–337. [Google Scholar] [CrossRef]
- Filicori, M. The role of luteinizing hormone in folliculogenesis and ovulation induction. Fertil. Steril. 1999, 71, 405–414. [Google Scholar] [CrossRef]
- Freis, A.; Germeyer, A.; Jauckus, J.; Capp, E.; Strowitzki, T.; Zorn, M.; Weber, A.M. Endometrial expression of receptivity markers subject to ovulation induction agents. Arch. Gynecol. Obstet. 2019, 300, 1741–1750. [Google Scholar] [CrossRef] [PubMed]
- MacNaughton, J.; Banah, M.; McCloud, P.; Hee, J.; Burger, H. Age related changes in follicle stimulating hormone, luteinizing hormone, oestradiol and immunoreactive inhibin in women of reproductive age. Clin. Endocrinol. 1992, 36, 339–345. [Google Scholar] [CrossRef] [PubMed]
- Alviggi, C.; Conforti, A.; Esteves, S.C.; Andersen, C.Y.; Bosch, E.; Bühler, K.; Ferraretti, A.P.; De Placido, G.; Mollo, A.; Fischer, R.; et al. Recombinant luteinizing hormone supplementation in assisted reproductive technology: A systematic review. Fertil. Steril. 2018, 109, 644–664. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alviggi, C.; Mollo, A.; Clarizia, R.; De Placido, G. Exploiting LH in ovarian stimulation. Reprod. Biomed. Online 2006, 12, 221–233. [Google Scholar] [CrossRef]
- Conforti, A.; Esteves, S.C.; Humaidan, P.; Longobardi, S.; D’Hooghe, T.; Orvieto, R.; Vaiarelli, A.; Cimadomo, D.; Rienzi, L.; Ubaldi, F.M.; et al. Recombinant human luteinizing hormone co-treatment in ovarian stimulation for assisted reproductive technology in women of advanced reproductive age: A systematic review and meta-analysis of randomized controlled trials. Reprod. Biol. Endocrinol. 2021, 19, 91. [Google Scholar] [CrossRef] [PubMed]
- Mochtar, M.H.; Danhof, N.A.; Ayeleke, R.O.; Van der Veen, F.; van Wely, M. Recombinant luteinizing hormone (rLH) and recombinant follicle stimulating hormone (rFSH) for ovarian stimulation in IVF/ICSI cycles. Cochrane Database Syst. Rev. 2017, 5, Cd005070. [Google Scholar] [CrossRef]
- Xiong, Y.; Bu, Z.; Dai, W.; Zhang, M.; Bao, X.; Sun, Y. Recombinant luteinizing hormone supplementation in women undergoing in vitro fertilization/ intracytoplasmic sperm injection with gonadotropin releasing hormone antagonist protocol: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2014, 12, 109. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hill, M.J.; Levens, E.D.; Levy, G.; Ryan, M.E.; Csokmay, J.M.; DeCherney, A.H.; Whitcomb, B.W. The use of recombinant luteinizing hormone in patients undergoing assisted reproductive techniques with advanced reproductive age: A systematic review and meta-analysis. Fertil. Steril. 2012, 97, 1108–1114.e1. [Google Scholar] [CrossRef]
- Revelli, A.; Pettinau, G.; Basso, G.; Carosso, A.; Ferrero, A.; Dallan, C.; Canosa, S.; Gennarelli, G.; Guidetti, D.; Filippini, C.; et al. Controlled Ovarian Stimulation with recombinant-FSH plus recombinant-LH vs. human Menopausal Gonadotropin based on the number of retrieved oocytes: Results from a routine clinical practice in a real-life population. Reprod. Biol. Endocrinol. 2015, 13, 77. [Google Scholar] [CrossRef] [Green Version]
- Revelli, A.; Gennarelli, G.; Sestero, M.; Canosa, S.; Carosso, A.; Salvagno, F.; Pittatore, G.; Filippini, C.; Benedetto, C. A prospective randomized trial comparing corifollitropin-alpha late-start (day 4) versus standard administration (day 2) in expected poor, normal, and high responders undergoing controlled ovarian stimulation for IVF. J. Assist. Reprod. Genet. 2020, 37, 1163–1170. [Google Scholar] [CrossRef] [PubMed]
- Ferraretti, A.P.; La Marca, A.; Fauser, B.C.; Tarlatzis, B.; Nargund, G.; Gianaroli, L.; on behalf of the ESHRE working group on Poor Ovarian Response Definition. ESHRE consensus on the definition of ‘poor response’ to ovarian stimulation for in vitro fertilization: The Bologna criteria. Hum. Reprod. 2011, 26, 1616–1624. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Esteves, S.C.; Alviggi, C.; Humaidan, P.; Fischer, R.; Andersen, C.Y.; Conforti, A.; Bühler, K.; Sunkara, S.K.; Polyzos, N.P.; Galliano, D.; et al. The POSEIDON Criteria and Its Measure of Success Through the Eyes of Clinicians and Embryologists. Front. Endocrinol. 2019, 10, 814. [Google Scholar] [CrossRef] [PubMed]
- Holte, J.; Berglund, L.; Milton, K.; Garello, C.; Gennarelli, G.; Revelli, A.; Bergh, T. Construction of an evidence-based integrated morphology cleavage embryo score for implantation potential of embryos scored and transferred on day 2 after oocyte retrieval. Hum. Reprod. 2007, 22, 548–557. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alpha Scientists in Reproductive Medicine and ESHRE Special Interest Group of Embryology. The Istanbul consensus workshop on embryo assessment: Proceedings of an expert meeting. Hum Reprod. 2011, 26, 1270–1283. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conforti, A.; Esteves, S.; Cimadomo, D.; Vaiarelli, A.; Di Rella, F.; Ubaldi, F.M.; Zullo, F.; De Placido, G.; Alviggi, C. Management of Women With an Unexpected Low Ovarian Response to Gonadotropin. Front. Endocrinol. 2019, 10, 387. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bosch, E.; Labarta, E.; Crespo, J.; Simon, C.; Remohí, J.; Pellicer, A. Impact of luteinizing hormone administration on gonadotropin-releasing hormone antagonist cycles: An age-adjusted analysis. Fertil. Steril. 2011, 95, 1031–1036. [Google Scholar] [CrossRef] [PubMed]
- von Wolff, M.; Stute, P.; Eisenhut, M.; Marti, U.; Bitterlich, N.; Bersinger, N.A. Serum and follicular fluid testosterone concentrations do not correlate, questioning the impact of androgen supplementation on the follicular endocrine milieu. Reprod. BioMed. Online 2017, 35, 616–623. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ruvolo, G.; Bosco, L.; Pane, A.; Morici, G.; Cittadini, E.; Rochheri, M.C. Lower apoptosis rate in human cumulus cells after administration of recombinant luteinizing hormone to women undergoing ovarian stimulation for in vitro fertilization procedures. Fertil. Steril. 2007, 87, 542–546. [Google Scholar] [CrossRef] [Green Version]
- Huang, Y.; Zhao, Y.; Yu, Y.; Li, R.; Lin, S.; Zhang, C.; Liu, P.; Qiao, J. Altered amphiregulin expression induced by diverse luteinizing hormone receptor reactivity in granulosa cells affects IVF outcomes. Reprod. Biomed. Online 2015, 30, 593–601. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Rimon, E.; Sasson, R.; Dantes, A.; Land-Bracha, A.; Amsterdam, A. Gonadotropin-induced gene regulation in human granulosa cells obtained from IVF patients: Modulation of genes coding for growth factors and their receptors and genes involved in cancer and other diseases. Int. J. Oncol. 2004, 24, 1325–1338. [Google Scholar] [CrossRef] [PubMed]
- Tesarik, J.; Hazout, A.; Mendoza, C. Luteinizing hormone affects uterine receptivity independently of ovarian function. Reprod. Biomed. Online 2003, 7, 59–64. [Google Scholar] [CrossRef]
- Herrler, A.; von Rango, U.; Beier, H.M. Embryo-maternal signalling: How the embryo starts talking to its mother to accomplish implantation. Reprod. Biomed. Online 2003, 6, 244–256. [Google Scholar] [CrossRef]
- Gridelet, V.; Tsampalas, M.; Berndt, S.; Hagelstein, M.T.; Charlet-Renard, C.; Conrath, V.; Ectors, F.; Hugé, F.; Munaut, C.; Foidart, J.M.; et al. Evidence for cross-talk between the LH receptor and LH during implantation in mice. Reprod. Fertil. Dev. 2013, 25, 511–522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Fanchin, R.; de Ziegler, D.; Taieb, J.; Hazout, A.; Frydman, R. Premature elevation of plasma progesterone alters pregnancy rates of in vitro fertilization and embryo transfer. Fertil. Steril. 1993, 59, 1090–1094. [Google Scholar] [CrossRef]
- Fanchin, R.; Righini, C.; Olivennes, F.; Taieb, J.; De Ziegler, D.; Frydman, R. Computerized assessment of endometrial echogenicity: Clues to the endometrial effects of premature progesterone elevation. Fertil. Steril. 1999, 71, 174–181. [Google Scholar] [CrossRef]
- Bosch, E.; Valencia, I.; Escudero, E.; Crespo, J.; Simón, C.; Remohí, J.; Pellicer, A. Premature luteinization during gonadotropin-releasing hormone antagonist cycles and its relationship with in vitro fertilization outcome. Fertil. Steril. 2003, 80, 1444–1449. [Google Scholar] [CrossRef] [PubMed]
- Bosch, E.; Labarta, E.; Crespo, J.; Simon, C.; Remohi, J.; Jenkins, J.; Pellicer, A. Circulating progesterone levels and ongoing pregnancy rates in controlled ovarian stimulation cycles for in vitro fertilization: Analysis of over 4000 cycles. Hum. Reprod. 2010, 25, 2092–2100. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sunkara, S.K.; Rittenberg, V.; Raine-Fenning, N.; Bhattacharya, S.; Zamora, J.; Coomarasamy, A. Association between the number of eggs and live birth in IVF treatment: An analysis of 400 135 treatment cycles. Hum. Reprod. 2011, 26, 1768–1774. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conforti, A.; Esteves, S.C.; Picarelli, S.; Iorio, G.; Rania, E.; Zullo, F.; De Placido, G.; Alviggi, C. Novel approaches for diagnosis and management of low prognosis patients in assisted reproductive technology: The POSEIDON concept. Panminerva. Med. 2019, 61, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Abu-Musa, A.; Haahr, T.; Humaidan, P. Novel Physiology and Definition of Poor Ovarian Response; Clinical Recommendations. Int. J. Mol. Sci. 2020, 21, 2110. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Conforti, A.; Esteves, S.C.; Di Rella, F.; Strina, I.; De Rosa, P.; Fiorenza, A.; Zullo, F.; De Placido, G.; Alviggi, C. The role of recombinant LH in women with hypo-response to controlled ovarian stimulation: A systematic review and meta-analysis. Reprod. Biol. Endocrinol. 2019, 17, 18. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Humaidan, P.; Chin, W.; Rogoff, D.; D’Hooghe, T.; Longobardi, S.; Hubbard, J.; Schertz, J. Efficacy and safety of follitropin alfa/lutropin alfa in ART: A randomized controlled trial in poor ovarian responders. Hum. Reprod. 2017, 32, 544–555. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| rFSH + rLH (n = 801) | rFSH Alone (n = 669) | p | |
|---|---|---|---|
| Age (years) | 37.8 ± 3.7 | 35.3 ± 4.2 | <0.0001 |
| BMI (kg/m2) | 22.6 ± 3.6 | 22.5 ± 3.6 | 0.22 |
| Basal (day 3) FSH (IU/l) | 9.2 ± 3.7 | 7.5 ± 2.6 | <0.0001 |
| AMH (ng/mL) | 0.9 ± 0.6 | 1.6 ± 0.7 | <0.0001 |
| Antral follicle count (AFC) | 7.9 ± 3.3 | 11.0 ± 3.3 | <0.0001 |
| Previous IVF treatments (n) | 0.7 ± 1.0 | 0.3 ± 0.7 | <0.0001 |
| Total FSH dose (IU) | 1727 ± 602 | 2321 ± 769 | <0.0001 |
| Days of stimulation (n) | 11.6 ± 2.4 | 11.4 ± 1.9 | <0.05 |
| Peak E2 (pg/mL) | 1469 ± 951 | 1541 ± 1126 | 0.20 |
| Endometrial thickness (mm) | 9.9 ± 2.2 | 10.1 ± 2.2 | 0.24 |
| OSI (n) | 3.4 ± 3.5 | 3.9 ± 4.0 | <0.0001 |
| Retrieved oocytes (n) | 5.0 ± 3.8 | 7.9 ± 4.1 | <0.0001 |
| Mature (MII) oocytes (n) | 4.0 ± 2.9 | 6.3 ±3.3 | <0.0001 |
| Maturation rate (%) | 81.2 ± 23.2 | 80.9 ± 19.2 | 0.73 |
| Fertilization rate (%) | 69.4 ± 31.2 | 68.6 ± 26.6 | 0.06 |
| Cleavage rate (%) | 96.5 ± 14.3 | 98.1 ± 16.2 | 0.13 |
| Mean embryo score (n) | 7.6 ± 1.7 | 7.5 ± 1.7 | 0.27 |
| Top quality embryos (%) | 52.8 ± 38.7 | 54.2 ± 34.6 | 0.62 |
| Frozen embryos (n) | 0.3 ± 0.9 | 0.6 ± 1.1 | <0.0001 |
| Cycles with no retrieved oocytes % (n) | 3.4 (27) | 1.6 (11) | <0.05 |
| Cycles with no mature oocytes % (n) | 5.9 (47) | 2.2 (15) | <0.0001 |
| Cycles with no fertilized oocytes % (n) | 14.4 (115) | 6.6 (44) | <0.0001 |
| Live birth rate/cycle % (n) | 19.7 (158) | 23.6 (158) | 0.07 |
| Cumulative live birth rate/OPU % (n) | 22.2 (178) | 29.3 (196) | <0.01 |
| rFSH + rLH (n = 263) | rFSH Alone (n = 46) | p | |
|---|---|---|---|
| Age (years) | 38.3 ± 3.5 | 36.4 ± 4.3 | <0.01 |
| BMI (kg/m2) | 22.4 ± 3.0 | 23.3 ± 4.2 | 0.43 |
| Basal (day 3) FSH (IU/l) | 9.9 ± 4.0 | 9.0 ± 4.3 | 0.09 |
| AMH (ng/mL) | 0.5 ± 0.3 | 0.6 ± 0.3 | 0.25 |
| Antral follicle count (AFC) | 4.6 ± 1.4 | 4.5 ± 1.6 | 0.77 |
| Previous IVF treatments (n) | 0.9 ± 1.1 | 0.7 ± 1.1 | 0.12 |
| Total FSH dose (IU) | 1727 ± 558 | 2681 ± 716 | <0.0001 |
| Days of stimulation | 11.4 ± 2.7 | 11.3 ± 2.3 | 0.78 |
| Peak E2 (pg/mL) | 1230 ± 735 | 1078 ± 791 | 0.08 |
| Endometrial thickness (mm) | 9.7 ± 2.3 | 10.1 ± 1.9 | 0.18 |
| OSI (n) | 2.3 ± 1.8 | 1.7 ± 1.3 | <0.05 |
| Retrieved oocytes (n) | 3.8 ± 2.8 | 4.5 ± 3.0 | 0.06 |
| Cycles with ≤3 oocytes % (n) | 55.9 (147) | 41.3 (19) | 0.07 |
| Cycles with 4–6 oocytes % (n) | 28.9 (76) | 37.0 (17) | 0.27 |
| Mature (MII) oocytes (n) | 3.1 ±2.4 | 3.5 ± 2.5 | 0.34 |
| Maturation rate (%) | 82.4 ± 25.8 | 76.2 ± 25.3 | 0.15 |
| Fertilization rate (%) | 68.1 ± 34.5 | 68.7 ± 29.7 | 0.79 |
| Cleavage rate (%) | 97.8 ± 10.7 | 95.5 ± 17.3 | 0.23 |
| Mean embryo score (n) | 7.6 ± 1.7 | 6.9 ± 2.3 | 0.07 |
| Top quality embryos (%) | 53.9 ± 39.3 | 49.0 ± 42.1 | 0.51 |
| Frozen embryos (n) | 0.7 ± 1.4 | 0.1 ± 0.3 | 0.07 |
| Live birth rate/cycle % (n) | 14.1 (37) | 15.2 (7) | 0.84 |
| Cumulative live birth rate/OPU % (n) | 15.6 (41) | 15.2 (7) | 0.95 |
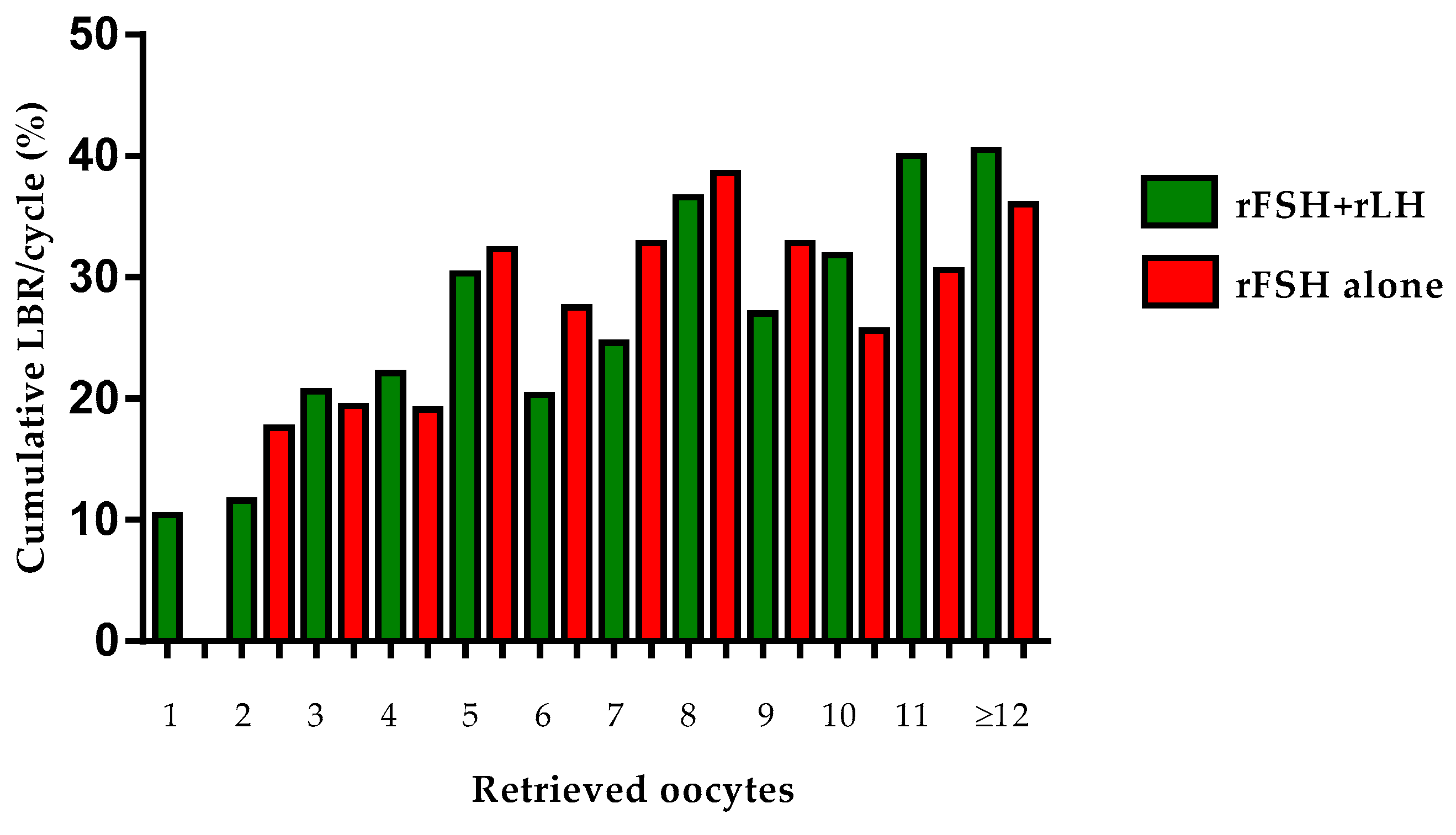
| Cumulative LBR/OPU % (n) | |||
|---|---|---|---|
| Retrieved | rFSH + rLH | rFSH Alone | |
| Oocytes | (n = 774) | (n = 658) | p |
| 1 | 10.4 (7/67) | 0 (0/11) | 0.26 |
| 2 | 11.6 (13/112) | 17.6 (6/34) | 0.36 |
| 3 | 20.6 (20/97) | 19.4 (7/36) | 0.88 |
| 4 | 22.1 (29/131) | 19.1 (9/47) | 0.67 |
| 5 | 30.3 (23/76) | 32.3 (20/62) | 0.80 |
| 6 | 20.3 (13/64) | 27.5 (19/69) | 0.33 |
| 7 | 24.6 (16/65) | 32.8 (21/64) | 0.30 |
| 8 | 36.6 (15/41) | 38.6 (27/70) | 0.84 |
| 9 | 27.0 (10/37) | 32.8 (20/61) | 0.55 |
| 10 | 31.8 (7/22) | 25.6 (11/43) | 0.59 |
| 11 | 40.0 (8/20) | 30.6 (11/36) | 0.47 |
| ≥12 | 40.5 (17/42) | 36.0 (45/125) | 0.60 |
| rFSH + rLH | rFSH Alone | ||
|---|---|---|---|
| (n = 801) | (n = 669) | p | |
| POSEIDON Group 1 | (n = 55, 7%) | (n = 212, 32%) | |
| Age (years) | 31.0 ± 2.5 | 31.3 ± 2.3 | 0.46 |
| AMH (ng/mL) | 1.9 ± 0.5 | 1.9 ± 0.4 | 0.38 |
| Antral follicle count (AFC) | 10.9 ± 3.2 | 12.1 ± 2.9 | <0.05 |
| Retrieved oocytes (n) | 7.8 ± 4.5 | 9.2 ± 4.3 | <0.05 |
| Mature (MII) oocytes (n) | 6.1 ± 4.2 | 7.2 ± 3.3 | 0.08 |
| Fertilization rate (%) | 71.2 ± 28.8 | 70.8 ± 23.5 | 0.92 |
| Top quality embryos (%) | 47.6 ± 34.0 | 56.2 ± 33.8 | 0.11 |
| Cumulative live birth rate/OPU % (n) | 36.4 (20/55) | 38.2 (81/212) | 0.80 |
| POSEIDON Group 2 | (n = 160, 20%) | (n = 269, 40%) | |
| Age (years) | 38.5 ± 2.3 | 38.0 ± 2.4 | <0.05 |
| AMH (ng/mL) | 1.8 ± 0.4 | 1.9 ± 0.4 | <0.01 |
| Antral follicle count (AFC) | 9.9 ± 3.2 | 11.1 ± 2.9 | <0.001 |
| Retrieved oocytes (n) | 7.0 ± 3.7 | 8.2 ± 3.8 | <0.01 |
| Mature (MII) oocytes (n) | 5.5 ± 3.0 | 6.5 ± 3.2 | <0.01 |
| Fertilization rate (%) | 68.8 ± 25.7 | 69.4 ± 26.6 | 0.84 |
| Top quality embryos (%) | 52.1 ± 36.5 | 52.4 ± 33.1 | 0.94 |
| Cumulative live birth rate/OPU % (n) | 24.4 (39/160) | 26.0 (70/269) | 0.70 |
| POSEIDON Group 3 | (n = 81, 10%) | (n = 61, 9%) | |
| Age (years) | 31.8 ± 1.9 | 31.2 ± 3.2 | 0.22 |
| AMH (ng/mL) | 0.6 ± 0.3 | 0.8 ± 0.2 | <0.0001 |
| Antral follicle count (AFC) | 7.1 ± 3.2 | 10.2 ± 3.6 | <0.001 |
| Retrieved oocytes (n) | 4.9 ± 3.0 | 6.8 ± 3.4 | <0.01 |
| Mature (MII) oocytes (n) | 3.7 ± 2.2 | 5.5 ± 3.0 | <0.001 |
| Fertilization rate (%) | 63.7 ± 30.7 | 62.6 ± 30.7 | 0.83 |
| Top quality embryos (%) | 60.7 ± 39.6 | 57.0 ± 39.4 | 0.60 |
| Cumulative live birth rate/OPU % (n) | 29.6 (24/81) | 26.2 (16/61) | 0.66 |
| POSEIDON Group 4 | (n = 505, 63%) | (n = 127, 19%) | |
| Age (years) | 39.2 ± 2.4 | 38.4 ± 2.7 | <0.01 |
| AMH (ng/mL) | 0.6 ± 0.3 | 0.7 ± 0.3 | <0.0001 |
| Antral follicle count (AFC) | 7.0 ± 2.9 | 8.6 ± 3.8 | <0.001 |
| Retrieved oocytes (n) | 4.1 ± 2.9 | 5.3 ± 3.2 | <0.0001 |
| Mature (MII) oocytes (n) | 3.4 ± 2.5 | 4.5 ± 3.0 | <0.001 |
| Fertilization rate (%) | 70.2 ± 33.1 | 65.5 ± 29.0 | 0.13 |
| Top quality embryos (%) | 52.4 ± 39.8 | 53.0 ± 36.6 | 0.88 |
| Cumulative live birth rate/OPU % (n) | 18.8 (95/505) | 22.8 (29/127) | 0.31 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canosa, S.; Carosso, A.R.; Mercaldo, N.; Ruffa, A.; Evangelista, F.; Bongioanni, F.; Benedetto, C.; Revelli, A.; Gennarelli, G. Effect of rLH Supplementation during Controlled Ovarian Stimulation for IVF: Evidence from a Retrospective Analysis of 1470 Poor/Suboptimal/Normal Responders Receiving Either rFSH plus rLH or rFSH Alone. J. Clin. Med. 2022, 11, 1575. https://doi.org/10.3390/jcm11061575
Canosa S, Carosso AR, Mercaldo N, Ruffa A, Evangelista F, Bongioanni F, Benedetto C, Revelli A, Gennarelli G. Effect of rLH Supplementation during Controlled Ovarian Stimulation for IVF: Evidence from a Retrospective Analysis of 1470 Poor/Suboptimal/Normal Responders Receiving Either rFSH plus rLH or rFSH Alone. Journal of Clinical Medicine. 2022; 11(6):1575. https://doi.org/10.3390/jcm11061575
Chicago/Turabian StyleCanosa, Stefano, Andrea Roberto Carosso, Noemi Mercaldo, Alessandro Ruffa, Francesca Evangelista, Francesca Bongioanni, Chiara Benedetto, Alberto Revelli, and Gianluca Gennarelli. 2022. "Effect of rLH Supplementation during Controlled Ovarian Stimulation for IVF: Evidence from a Retrospective Analysis of 1470 Poor/Suboptimal/Normal Responders Receiving Either rFSH plus rLH or rFSH Alone" Journal of Clinical Medicine 11, no. 6: 1575. https://doi.org/10.3390/jcm11061575
APA StyleCanosa, S., Carosso, A. R., Mercaldo, N., Ruffa, A., Evangelista, F., Bongioanni, F., Benedetto, C., Revelli, A., & Gennarelli, G. (2022). Effect of rLH Supplementation during Controlled Ovarian Stimulation for IVF: Evidence from a Retrospective Analysis of 1470 Poor/Suboptimal/Normal Responders Receiving Either rFSH plus rLH or rFSH Alone. Journal of Clinical Medicine, 11(6), 1575. https://doi.org/10.3390/jcm11061575