
High Prevalence of Scoliosis in a Large Cohort of Patients with Prader-Willi Syndrome

 ,
,  ,
,  , ,
, ,  and
and
Abstract
:1. Introduction
2. Patients and Methods
2.1. Study Population
2.2. Auxological Data
2.3. Scoliosis Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of the Cohort
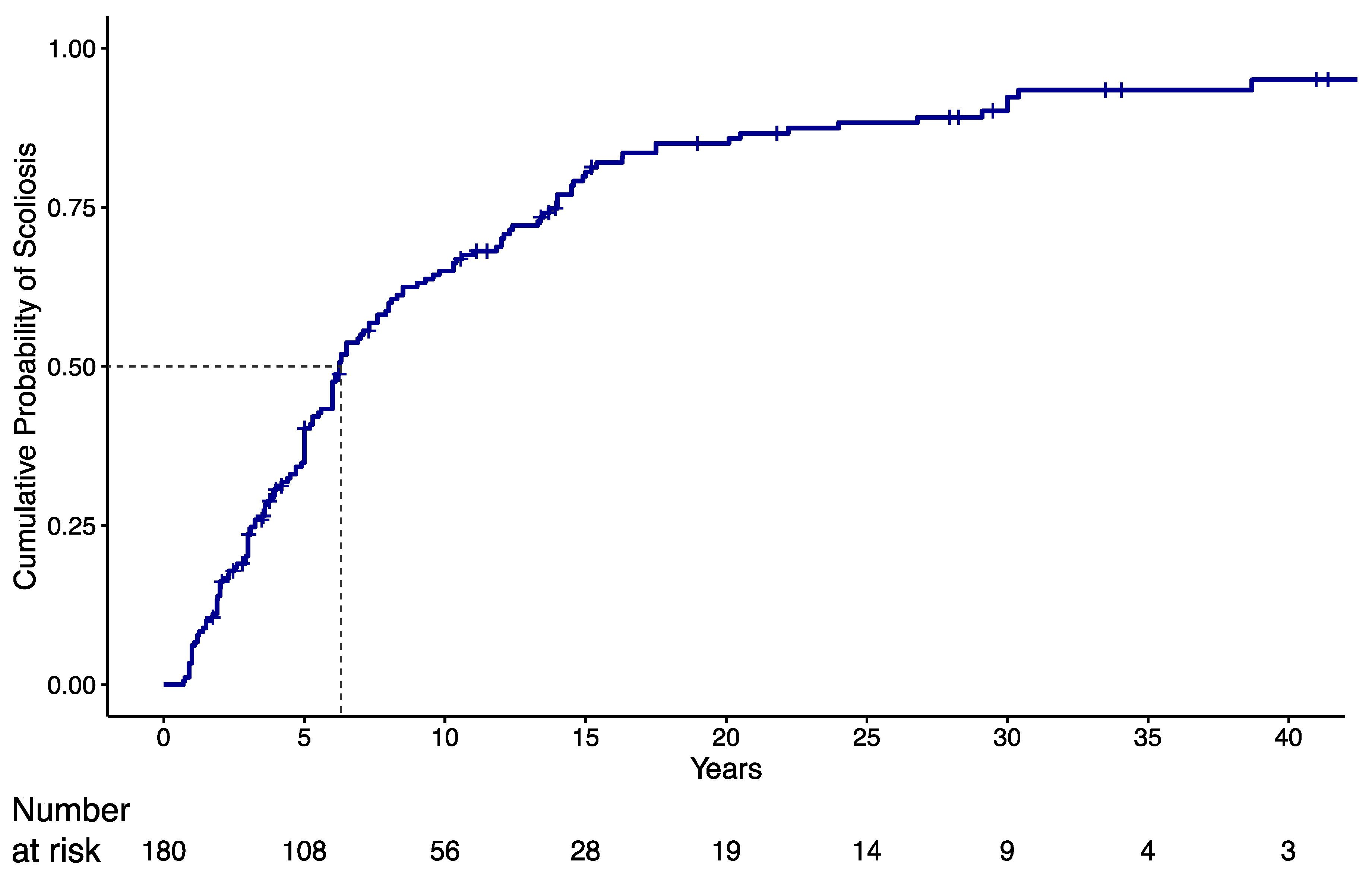
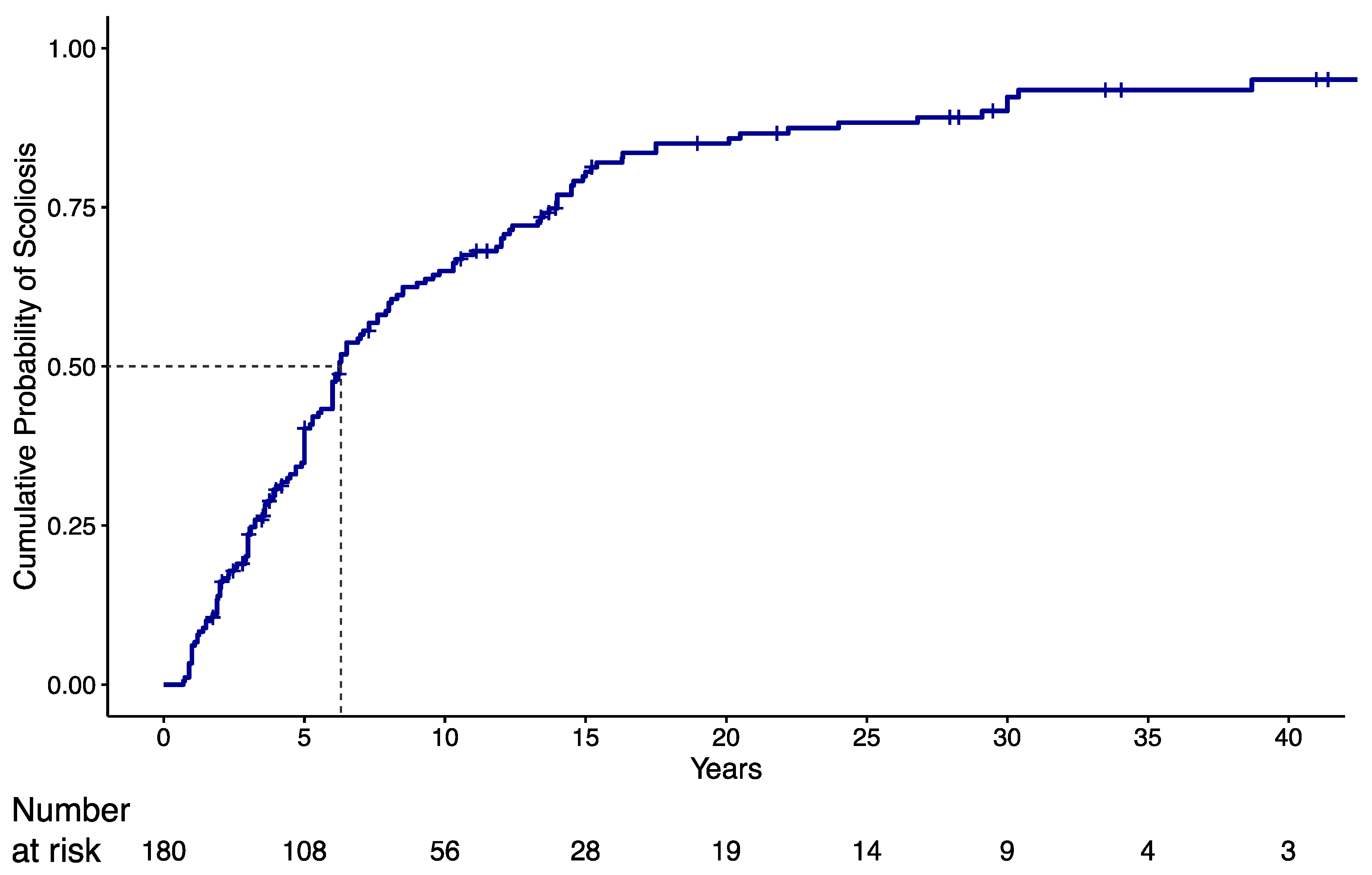
3.2. Scoliosis
3.3. Predictive Factors for Scoliosis
3.4. Clinical and Anthropometric Measurements at Final Evaluation According to Scoliosis
3.5. Severity of Scoliosis
3.6. Scoliosis Treatment
4. Discussion and Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Bar, C.; Diene, G.; Molinas, C.; Bieth, E.; Casper, C.; Tauber, M. Early diagnosis and care is achieved but should be improved in infants with Prader-Willi syndrome. Orphanet J. Rare Dis. 2017, 12, 1–6. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Butler, M.G.; Hartin, S.N.; Hossain, W.A.; Manzardo, A.M.; Kimonis, V.; Dykens, E.; Gold, J.A.; Kim, S.-J.; Weisensel, N.; Tamura, R.; et al. Molecular genetic classification in Prader-Willi syndrome: A multisite cohort study. J. Med. Genet. 2019, 56, 149–153. [Google Scholar] [CrossRef] [PubMed]
- Cassidy, S.B.; Schawartz, S.; Miller, J.L.; Driscoll, D.J. Prader-Willi syndrome. Genet. Med. 2012, 14, 10–26. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tauber, M.; Hoybye, C. Endocrine disorders in Prader-Willi syndrome: A model to understand and treat hypothalamic dysfunction. Lancet Diabetes Endocrinol. 2021, 9, 235–246. [Google Scholar] [CrossRef]
- Shim, J.S.; Lee, S.H.; Seo, S.W.; Koo, K.H.; Jin, D.K. The musculoskeletal manifestations of Prader-Willi syndrome. J. Pediatr. Orthop. 2010, 30, 390–395. [Google Scholar] [CrossRef] [PubMed]
- Odent, T.; Accadbled, F.; Koureas, G.; Cournot, M.; Moine, A.; Diene, G.; Molinas, C.; Pinto, G.; Tauber, M.; Gomes, B.; et al. Scoliosis in patients with Prader-Willi syndrome. Pediatrics 2008, 122, e499–e503. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tan, H.L.; Urquhart, D.S. Respiratory complications in children with Prader Willi Syndrome. Paediatr. Respir. Rev. 2017, 22, 52–59. [Google Scholar] [CrossRef] [PubMed]
- Pacoricona Alfaro, D.L.; Diene, G.; Pinto, G.; Salles, J.P.; Gennero, I.; Faye, S.; Molinas, C.; Valette, M.; Arnaud, C.; Tauber, M. Is ghrelin a biomarker of early-onset scoliosis in children with Prader-Willi syndrome? Orphanet J. Rare Dis. 2021, 16, 305. [Google Scholar] [CrossRef] [PubMed]
- Accadbled, F.; Odent, T.; Moine, A.; Chau, E.; Glorion, C.; Diene, G.; de Gauzy, J.S. Complications of scoliosis surgery in Prader-Willi syndrome. Spine 2008, 33, 394–401. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- de Lind van Wijngaarden, R.F.A.; de Klerk, L.W.L.; Festen, D.A.M.; Hokken-Koelega, A.C.S. Scoliosis in Prader–Willi syndrome: Prevalence, effects of age, gender, body mass index, lean body mass and genotype. Arch. Dis. Child. 2008, 93, 1012–1016. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- van Bosse, H.J.P.; Butler, M.G. Clinical observations and treatment approaches for scoliosis in Prader-Willi syndrome. Genes 2020, 11, 260. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sinnema, M.; Maaskant, M.A.; van Schrojenstein Lantman-de Valk, H.M.; Boer, H.; Curfs, L.M.; Schrander-Stumpel, C.T. The use of medical care and the prevalence of serious illness in an adult Prader-Willi syndrome cohort. Eur. J. Med. Genet. 2013, 56, 397–403. [Google Scholar] [CrossRef] [PubMed]
- Pellikaan, K.; Rosenberg, A.G.W.; Kattentidt-Mouravieva, A.A.; Kersseboom, R.; Bos-Roubos, A.G.; Veen-Roelofs, J.M.C.; van Wieringen, N.; Hoekstra, F.M.E.; van den Berg, S.A.A.; van der Lely, A.J.; et al. Missed Diagnoses and Health Problems in Adults with Prader-Willi Syndrome: Recommendations for Screening and Treatment. J. Clin. Endocrinol. Metab. 2020, 105, e4671–e4687. [Google Scholar] [CrossRef] [PubMed]
- Proffitt, J.; Osann, K.; McManus, B.; Kimonis, V.E.; Heinemann, J.; Butler, M.G.; Stevenson, D.A.; Gold, J.A. Contributing factors of mortality in Prader-Willi syndrome. Am. J. Med. Genet. Part A 2019, 179, 196–205. [Google Scholar] [CrossRef] [PubMed]
- Butler, J.V.; Whittington, J.E.; Holland, A.J.; Boer, H.; Clarke, D.; Webb, T. Prevalence of, and risk factors for, physical ill-health in people with Prader-Willi syndrome: A population-based study. Dev. Med. Child Neurol. 2002, 44, 248–255. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Nagai, T.; Iida, T.; Ozeki, S.; Nohara, Y. Epidemiological aspects of scoliosis in a cohort of Japanese patients with Prader-Willi syndrome. Spine J. 2009, 9, 809–816. [Google Scholar] [CrossRef] [PubMed]
- Murakami, N.; Obata, K.; Abe, Y.; Oto, Y.; Kido, Y.; Itabashi, H.; Tsuchiya, T.; Tanaka, Y.; Yoshino, A.; Nagai, T. Scoliosis in Prader–Willi syndrome: Effect of growth hormone therapy and value of paravertebral muscle volume by CT in predicting scoliosis progression. Am. J. Med. Genet. Part A 2012, 158, 1628–1632. [Google Scholar] [CrossRef] [PubMed]
- Coupaye, M.; Tauber, M.; Cuisset, L.; Laurier, V.; Bieth, E.; Lacorte, J.M.; Oppert, J.M.; Clément, K.; Poitou, C. Effect of genotype and previous GH treatment on adiposity in adults with Prader-Willi syndrome. J. Clin. Endocrinol. Metab. 2016, 101, 4895–4903. [Google Scholar] [CrossRef] [PubMed]
- Nagai, T.; Obata, K.; Ogata, T.; Murakami, N.; Katada, Y.; Yoshino, A.; Sakazume, S.; Tomita, Y.; Sakuta, R.; Niikawa, N. Growth hormone therapy and scoliosis in patients with Prader-Willi syndrome. Am. J. Med. Genet. Part A 2006, 140, 1623–1627. [Google Scholar] [CrossRef]
- Butler, M.G.; Miller, J.L.; Forster, J.L. Prader-Willi syndrome-Clinical genetics, diagnosis and treatment approaches: An update. Curr. Pediatr. Rev. 2019, 15, 207–244. [Google Scholar] [CrossRef] [PubMed]
- Di Felice, F.; Zaina, F.; Donzelli, S.; Negrini, S. The natural history of idiopathic scoliosis during growth: A meta-analysis. Am. J. Phys. Med. Rehabil. 2018, 97, 346–356. [Google Scholar] [CrossRef] [PubMed]
- Weinstein, S.L. The Natural History of Adolescent Idiopathic Scoliosis. J. Pediatr. Orthop. 2019, 39, S44–S46. [Google Scholar] [CrossRef] [PubMed]
- Grootjen, L.N.; Rutges, J.P.H.J.; Damen, L.; Donze, S.H.; Juriaans, A.F.; Kerkhof, G.F.; Hokken-Koelega, A.C.S. Effects of 8 years of growth hormone treatment on scoliosis in children with Prader-Willi syndrome. Eur. J. Endocrinol. 2021, 185, 47–55. [Google Scholar] [CrossRef] [PubMed]
- Cacciari, E.; Milani, S.; Balsamo, A.; Spada, E.; Bona, G.; Cavallo, L.; Cerutti, F.; Gargantini, L.; Greggio, N.; Tonini, G.; et al. Italian cross-sectional growth charts for height, weight and BMI (2 to 20 years). J. Endocrinol. Investig. 2006, 29, 581–593. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Obesity and Overweight. 2011. Available online: http://www.who.int/mediacentre/factsheets/fs311/en/ (accessed on 9 December 2021).
- Tanner, J.M.; Whitehouse, R.H. Clinical longitudinal standards for height, weight, height velocity, weight velocity and stages of puberty. Arch. Dis. Child. 1976, 51, 170–179. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Berven, S.H.; Lowe, T. The Scoliosis Research Society classification for adult spinal deformity. Neurosurg. Clin. N. Am. 2007, 18, 207–213. [Google Scholar] [CrossRef] [PubMed]
- R Core Team. R: A Language and Environment for Statistical Computing; R Foundation for Statistical Computing: Vienna, Austria, 2020; Available online: https://www.R-project.org/ (accessed on 21 December 2021).
- Holm, V.A.; Cassidy, S.B.; Butler, M.G.; Hanchett, J.M.; Greenswag, L.R.; Whitman, B.Y.; Greenberg, F. Prader-Willi syndrome: Consensus diagnostic criteria. Pediatrics 1993, 91, 398–402. [Google Scholar] [CrossRef] [PubMed]
- Crinò, A.; Di Giorgio, G.; Livieri, C.; Grugni, G.; Beccaria, L.; Bosio, L.; Corrias, A.; Chiumello, G.; Trifirò, G.; Salvatoni, A.; et al. A survey on Prader-Willi syndrome in the Italian population: Prevalence of historical and clinical signs. J. Pediatr. Endocrinol. Metab. 2009, 22, 883–894. [Google Scholar] [CrossRef] [PubMed]
- Hakonarson, H.; Moskovitz, J.; Daigle, K.L.; Cassidy, S.B.; Cloutier, M.M. Pulmonary function abnormalities in Prader-Willi syndrome. J. Pediatr. 1995, 126, 565–570. [Google Scholar] [CrossRef]
- Tokutomi, T.; Chida, A.; Asano, Y.; Ishiwata, T.; Koike, Y.; Motegi, A.; Asazuma, T.; Nonoyama, S. A non-obese boy with Prader-Willi syndrome shows cardiopulmonary impairment due to severe kyphoscoliosis. Am. J. Med. Genet. Part A 2006, 140, 1978–1980. [Google Scholar] [CrossRef]
- Nixon, G.M.; Brouillette, R.T. Sleep and breathing in Prader-Willi syndrome. Pediatr. Pulmonol. 2002, 34, 209–217. [Google Scholar] [CrossRef] [PubMed]
- Nakamura, Y.; Murakami, N.; Iida, T.; Ozeki, S.; Asano, S.; Nohara, Y.; Nagai, T. The characteristics of scoliosis in Prader-Willi syndrome (PWS): Analysis of 58 scoliosis patients with PWS. J. Orthop. Sci. 2015, 20, 17–22. [Google Scholar] [CrossRef] [PubMed]
- Greenswag, L.R. Adults with Prader-Willi syndrome: A survey of 232 cases. Dev. Med. Child Neurol. 1987, 29, 145–152. [Google Scholar] [CrossRef] [PubMed]
- Butler, M.G. Prader-Willi syndrome: Current understanding of cause and diagnosis. Am. J. Med. Genet. 1990, 35, 319–332. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Laurier, V.; Lapeyrade, A.; Copet, P.; Demeer, G.; Silvie, M.; Bieth, E.; Coupaye, M.; Poitou, C.; Lorenzini, F.; Labrousse, F.; et al. Medical, psychological and social features in a large cohort of adults with Prader-Willi syndrome: Experience from a dedicated centre in France. J. Intellect. Disabil. Res. 2015, 59, 411–421. [Google Scholar] [CrossRef] [PubMed]
- Deal, C.L.; Tony, M.; Höybye, C.; Allen, D.B.; Tauber, M.; Christiansen, J. S; Growth Hormone in Prader-Willi Syndrome Clinical Care Guidelines Workshop Participants. GrowthHormone Research Society workshop summary: Consensus guidelines for recombinant human growth hormone therapy in Prader-Willi syndrome. J. Clin. Endocrinol. Metab. 2013, 98, E1072–E1087. [Google Scholar] [CrossRef] [PubMed]
- de Lind van Wijngaarden, R.F.; de Klerk, L.W.; Festen, D.A.; Duivenvoorden, H.J.; Otten, B.J.; Hokken-Koelega, A.C. Randomized controlled trial to investigate the effects of growth hormone treatment on scoliosis in children with Prader-Willi syndrome. J. Clin. Endocrinol. Metab. 2009, 94, 1274–1280. [Google Scholar] [CrossRef] [PubMed] [Green Version]

{kind=link}
| Overall Cohort | Children (Age < 18 yrs) | Adults (Age ≥ 18 yrs) | |
|---|---|---|---|
| Number | 180 | 106 (58.9%) | 74 (41.1%) |
| Age at evaluation; yrs | 17.6 ± 12 (1.7 to 49.7) | 9.3 ± 5 (1.7 to 17.9) | 29.5 ± 8.6 (18 to 49.7) |
| Age at PWS diagnosis; yrs | 0.8 [0.2; 3.6] (0.1 to 20.5) | 0.2 [0.1; 0.9] (0.1 to 15) | 3.2 [1; 10] (0.1 to 20.5) |
| Genetics | |||
| del15 | 99 (55%) | 53 (50%) | 46 (62.2%) |
| UPD15 | 78 (43.3%) | 50 (47.2%) | 28 (37.8%) |
| Other | 3 (1.7%) | 3 (2.8%) | 0 (0%) |
| Gender | |||
| Male | 84 (46.7%) | 50 (47.2%) | 34 (45.9%) |
| Female | 96 (53.3%) | 56 (52.8%) | 40 (54.1%) |
| Pubertal status (Tanner) | |||
| 1 | 61 (33.9%) | 61 (57.5%) | 0 (0%) |
| 2 | 27 (15%) | 23 (21.7%) | 4 (5.4%) |
| 3 | 45 (25%) | 16 (15.1%) | 29 (39.2%) |
| 4 | 47 (26.1%) | 6 (5.7%) | 41 (55.4%) |
| BMI (kg/m2) | 29 ± 11.2 (12.5 to 64.6) | 24.1 ± 9.6 (12.5 to 64.6) | 36.1 ± 9.4 (21.7 to 59.7) |
| BMI SDS | 1.65 ± 1.59 (−3.48 to 4.48) | 1.04 ± 1.63 (−3.84 to 4.48) | 2.53 ± 1.03 (−0.2 to 4.01) |
| Obesity; n (%) | 85 (47.2%) | 30 (28.3%) | 55 (74.3%) |
| GH therapy | |||
| Never | 30 (16.7%) | 9 (8.5%) | 21 (28.4%) |
| Current or past | 150 (83.3%) | 97 (91.5%) | 53 (71.6%) |
| Age at start of GH therapy; yrs | 2.5 [0.9; 6.5] (0.2 to 32) | 1.3 [0.7; 2.7] (0.2 to 11.7) | 8.5 [3.9; 12] (0.6 to 32) |
| Duration of GH therapy; yrs | 6.3 [2.8; 9.8] (0.1 to 20.3) | 5.3 [2.4; 8.5] (0.1 to 14.2) | 9 [3.3; 11.9] (0.5 to 20.3) |
| Without Scoliosis | With Scoliosis | HR [95% C.I.] | p-Value | |
|---|---|---|---|---|
| Number | 30 (17%) | 150 (83%) | ||
| Genotype | ||||
| del15 | 14 (46.7%) | 85 (56.7%) | ref | - |
| UPD15 | 14 (46.7%) | 64 (42.7%) | 1.1 [0.79 to 1.53] | 0.561 |
| Other | 2 (6.7%) | 1 (0.7%) | 0.3 [0.04 to 2.17] | 0.234 |
| Gender | ||||
| Male | 16 (53.3%) | 68 (45.3%) | ref | - |
| Female | 14 (46.7%) | 82 (54.7%) | 1.29 [0.93 to 1.78] | 0.127 |
| Therapy with GH | ||||
| Never treated or started therapy after scoliosis diagnosis | 5 (16.7%) | 64 (42.7%) | ref | - |
| Yes (before scoliosis diagnosis) | 25 (83.3%) | 86 (57.3%) | 1.08 [0.78 to 1.78] | 0.655 |
| Without Scoliosis | With Scoliosis | p-Value | |
|---|---|---|---|
| Number | 30 (16.7%) | 150 (83.3%) | |
| Age at observation; yrs | 10.8 [3.5; 23.3] (1.7 to 41.4) | 16.5 [9; 25.7] (1.7 to 49.7) | 0.022 |
| Pubertal stage | 0.088 | ||
| 1 | 16 (53.3) | 45 (30) | |
| 2 | 2 (6.7) | 25 (16.7) | |
| 3 | 7 (23.3) | 38 (25.3) | |
| 4 | 5 (16.7) | 42 (28) | |
| BMI (kg/m2) | 26.8 ± 12.9 (13.8 to 64.6) | 29.5 ± 10.9 (12.5 to 59.7) | 0.302 |
| BMI SDS | 1.4 ± 1.8 (−1.9 to 4.5) | 1.7 ± 1.6 (−3.8 to 4.4) | 0.310 |
| Mild | Moderate | Severe | Overall p-Value | |
|---|---|---|---|---|
| Number | 58 (38.7%) | 43 (28.7%) | 49 (32.6%) | |
| Genetics | 1 | |||
| del15 | 33 (56.9%) | 24 (55.8%) | 28 (57.1%) | |
| UPD15 | 24 (41.4%) | 19 (44.2%) | 21 (42.9%) | |
| Other | 1 (1.7%) | 0 (0%) | 0 (0%) | |
| Gender | 0.025 | |||
| Male | 33 (56.9%) | 20 (46.5%) | 15 (30.6%) | |
| Female | 25 (43.1%) | 23 (53.5%) | 34 (69.4%) | |
| Therapy with GH | 0.302 | |||
| Never treated or started therapy after scoliosis diagnosis | 24 (41.4%) | 15 (34.9%) | 25 (51%) | |
| Yes (before scoliosis diagnosis) | 34 (58.6%) | 28 (65.1%) | 24 (49%) | |
| Age at start of GH therapy; yrs | 2.3 [0.8; 6.6] (0.3 to 32) | 2.1 [0.8; 7.8] (0.2 to 21) | 2.7 [1.2; 6.8] (0.5 to 24) | 0.830 |
| Age at diagnosis of scoliosis; yrs | 6.2 [3; 12.6] (0.8 to 43.4) | 6.5 [4.7; 12.4] (0.9 to 30.4) | 3.8 [2.1; 6.1] (0.7 to 22.2) | 0.005 |
| BMI (kg/m2) | 28.9 ± 11.1 (12.6 to 54.9) | 29 ± 10.8 (12.5 to 57.7) | 30.6 ± 10.9 (13.5 to 59.7) | 0.695 |
| BMI SDS | 1.69 ± 1.7 (−3.84 to 4.42) | 1.58 ± 1.51 (−3.01 to 3.96) | 1.84 ± 1.43 (−2.02 to 4.01) | 0.726 |
| Obesity; n (%) | 30 (51.7%) | 17 (39.5%) | 26 (53.1%) | 0.362 |
| Variables | Sample Characteristics |
|---|---|
| Age at surgery (yrs) | 13.1 [10.6; 14.8] (5 to 27.5) |
| Gender | |
| Male | 9 (34.6%) |
| Female | 17 (65.4%) |
| Genotype | |
| del15 | 15 (57.7%) |
| UPD15 | 11 (42.3%) |
| GH treatment (before surgery) | |
| No | 2 (7.7%) |
| Yes | 24 (92.3%) |
| Age at start of GH therapy; yrs | 2.7 [1.8; 8.5] (0.5 to 16) |
| Duration of GH therapy; yrs | 9.3 ± 4.05 (1.3 to 16.8) |
| Age at diagnosis of scoliosis; yrs | 3.4 [2.3; 6] (0.9 to 14.5) |
| Brace (before surgery) | 25 (96.2%) |
| BMI (kg/m2) | 29.3 ± 8.4 (17.3 to 52.5) |
| BMI SDS | 1.75 ± 1.22 (−1.22 to 3.97) |
| Obesity; n (%) | 13 (50%) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Crinò, A.; Armando, M.; Crostelli, M.; Mazza, O.; Bruzzese, D.; Convertino, A.; Fintini, D.; Bocchini, S.; Ciccone, S.; Sartorio, A.; et al. High Prevalence of Scoliosis in a Large Cohort of Patients with Prader-Willi Syndrome. J. Clin. Med. 2022, 11, 1574. https://doi.org/10.3390/jcm11061574
Crinò A, Armando M, Crostelli M, Mazza O, Bruzzese D, Convertino A, Fintini D, Bocchini S, Ciccone S, Sartorio A, et al. High Prevalence of Scoliosis in a Large Cohort of Patients with Prader-Willi Syndrome. Journal of Clinical Medicine. 2022; 11(6):1574. https://doi.org/10.3390/jcm11061574
Chicago/Turabian StyleCrinò, Antonino, Michela Armando, Marco Crostelli, Osvaldo Mazza, Dario Bruzzese, Alessio Convertino, Danilo Fintini, Sarah Bocchini, Sara Ciccone, Alessandro Sartorio, and et al. 2022. "High Prevalence of Scoliosis in a Large Cohort of Patients with Prader-Willi Syndrome" Journal of Clinical Medicine 11, no. 6: 1574. https://doi.org/10.3390/jcm11061574
APA StyleCrinò, A., Armando, M., Crostelli, M., Mazza, O., Bruzzese, D., Convertino, A., Fintini, D., Bocchini, S., Ciccone, S., Sartorio, A., & Grugni, G. (2022). High Prevalence of Scoliosis in a Large Cohort of Patients with Prader-Willi Syndrome. Journal of Clinical Medicine, 11(6), 1574. https://doi.org/10.3390/jcm11061574