
Signs, Symptoms, and Morphological Features of Idiopathic Condylar Resorption in Orthodontic Patients: A Survey-Based Study



Abstract
:1. Introduction
2. Materials and Methods
2.1. Participants
2.2. Malocclusion
- Maxillary protrusion, malocclusion with overjet >5 mm;
- Mandibular prognathism, malocclusion with anterior crossbite;
- Posterior crossbite, malocclusion with posterior unilateral or bilateral crossbite;
- Open bite, malocclusion with negative overbite;
- Deep bite, malocclusion with overbite >5 mm;
- Crowding, malocclusion with malpositioning of teeth.
2.3. Clinical Examination
- TMJ sounds, including clicking and crepitus, on joint palpation during jaw opening and closing movements.
- TMJ pain on joint palpation from the lateral and posterior sides.
- Tenderness on palpation in 10 masticatory muscles including the deep and superficial masseter, anterior and posterior parts of the temporalis, posterior belly of the digastric, sternocleidomastoid, and trapezius.
- Maximum pain-free mouth opening was measured using calipers. Limitations in mouth opening were defined as mouth opening < 40 mm and/or mandibular lateral deviation ≥5 mm at maximum mouth opening.
2.4. Questionnaire
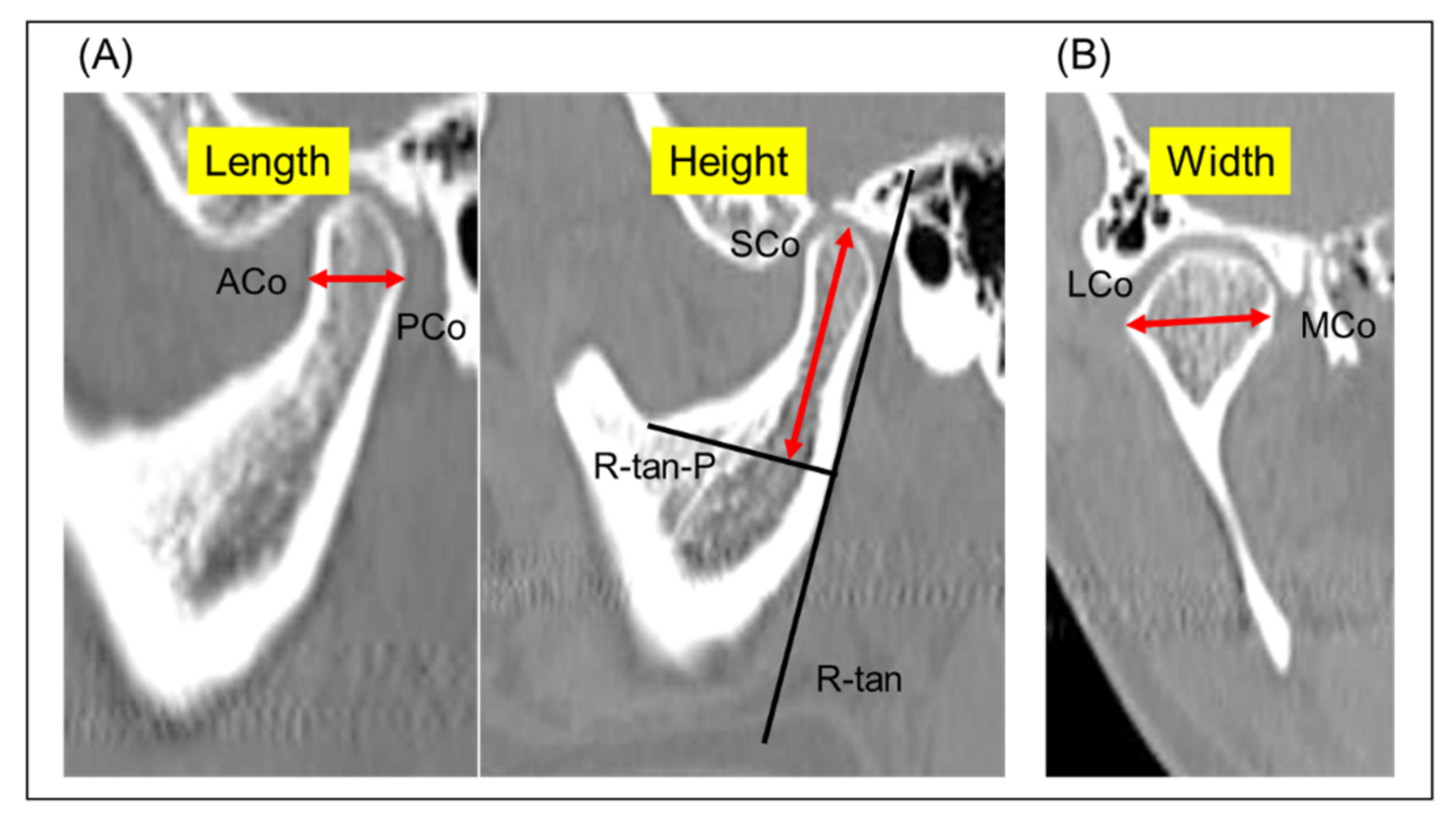
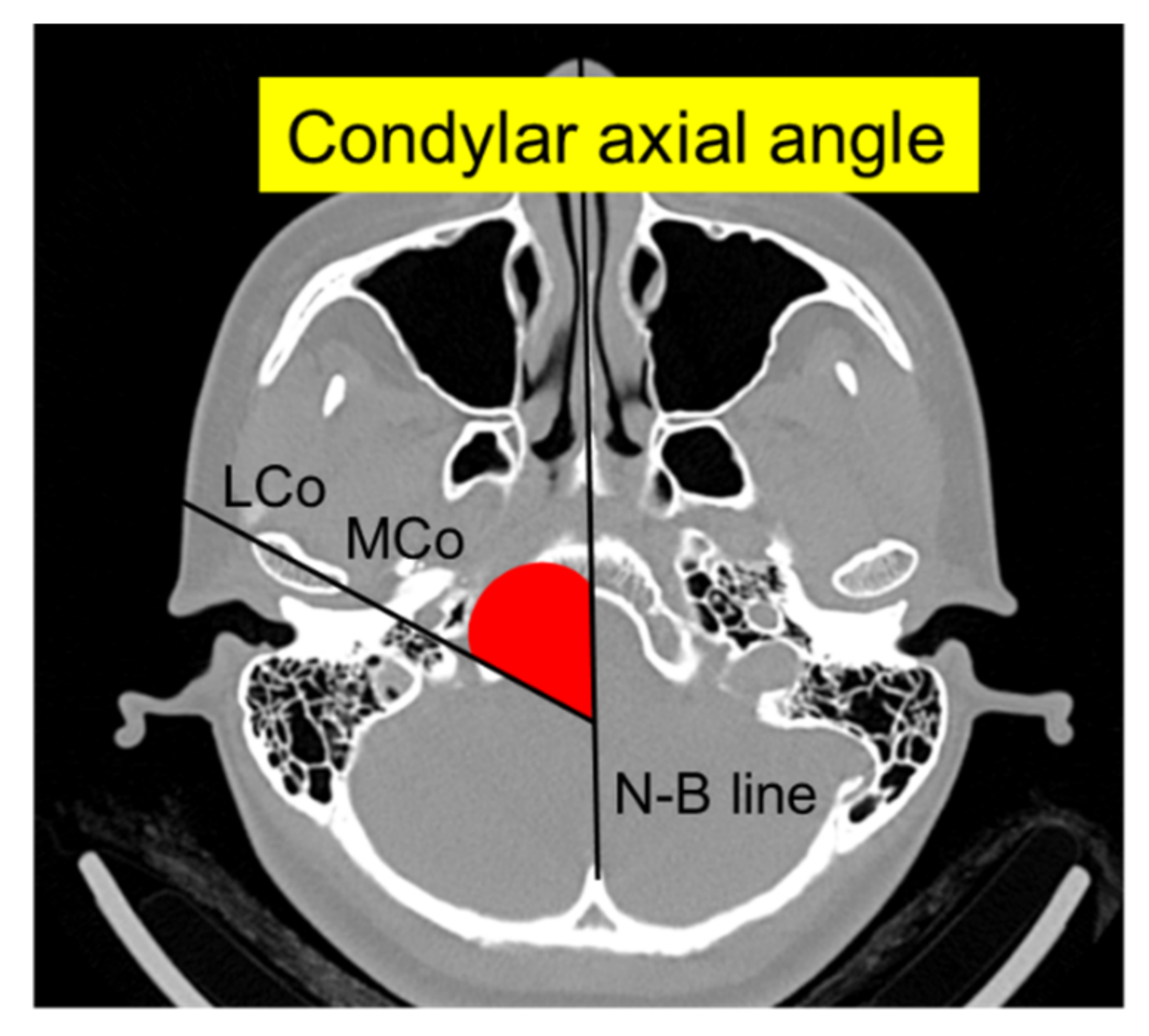
2.5. Three-Dimensional CT of TMJ
2.6. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Tanaka, E.; Koolstra, J.H. Biomechanics of the temporomandibular joint. J. Dent. Res. 2008, 87, 989–991. [Google Scholar] [CrossRef]
- Tanaka, E.; Kawai, N.; Hanaoka, K.; van Eijden, T.; Sasaki, A.; Aoyama, J.; Tanaka, M.; Tanne, K. Shear properties of the temporomandibular joint disc in relation to compressive and shear strain. J. Dent. Res. 2004, 83, 476–479. [Google Scholar] [CrossRef] [PubMed]
- Shibukawa, Y.; Young, B.; Wu, C.; Yamada, S.; Long, F.; Pacfici, M.; Koyama, E. Temporomandibular joint formation and condyle growth require Indian hedgehog signaling. Dev. Dyn. 2007, 236, 426–434. [Google Scholar] [CrossRef]
- Kantomaa, T.; Tuominen, M.; Pirttiniemi, P. Effect of mechanical forces on chondrocyte maturation and differentiation in the mandibular condyle of the rat. J. Dent. Res. 1994, 73, 1150–1156. [Google Scholar] [CrossRef]
- Wolford, L.M.; Cardenas, L. Idiopathic condylar resorption: Diagnosis, treatment protocol, and outcomes. Am. J. Orthod. Dentofac. Orthop. 1999, 116, 667–677. [Google Scholar] [CrossRef]
- Mercuri, L.G.; Handelman, C.S. Idiopathic condylar resorption: What should we do? Oral Maxillofac. Surg. Clin. N. Am. 2020, 32, 105–116. [Google Scholar] [CrossRef]
- Arnett, G.W.; Milam, S.B.; Gottesman, L. Progressive mandibular retrusion-idiopathic condylar resorption. Part I. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 8–15. [Google Scholar] [CrossRef]
- Arnett, G.W.; Milam, S.B.; Gottesman, L. Progressive mandibular retrusion-idiopathic condylar resorption. Part II. Am. J. Orthod. Dentofac. Orthop. 1996, 110, 117–127. [Google Scholar] [CrossRef]
- Arnett, G.W.; Gunson, M.J. Risk factors in the initiation of condylar resorption. Semin. Orthod. 2013, 19, 81–88. [Google Scholar] [CrossRef] [Green Version]
- Hatcher, D.C. Progressive condylar resorption: Pathologic processes and imaging considerations. Semin. Orthod. 2013, 19, 97–105. [Google Scholar] [CrossRef]
- Mehra, P.; Wolford, L.M. The Mitek mini anchor for TMJ disc repositioning: Surgical technique and results. Int. J. Oral Maxillofac. Surg. 2001, 30, 497–503. [Google Scholar] [CrossRef] [PubMed]
- Posnick, J.C.; Fantuzzo, J.J. Idiopathic condylar resorption: Current clinical perspectives. J. Oral Maxillofac. Surg. 2007, 65, 1617–1623. [Google Scholar] [CrossRef] [PubMed]
- Yuan, M.; Xie, Q.; Shen, P.; Yang, C. Do sex hormone imbalances contribute to idiopathic condylar resorption? Int. J. Oral Maxillofac. Surg. 2021, 50, 1244–1248. [Google Scholar] [CrossRef] [PubMed]
- Schiffman, E.; Ohrbach, R.; Truelove, E.; Look, J.; Anderson, G.; Goulet, J.P.; List, T.; Svensson, P.; Gonzalez, Y.; Lobbezoo, F.; et al. Diagnostic criteria for temporomandibular disorders (DC/TMD) for clinical and research applications: Recommendations of the international RDC/TMD consortium network and orofacial pain special interest group. J. Oral Facial Pain Headache 2014, 28, 6–27. [Google Scholar] [CrossRef]
- Kristensen, K.D.; Schmidt, B.; Stoustrup, P.; Pedersen, T.K. Idiopathic condylar resorptions: 3-dimensional condylar bony deformation, signs and symptoms. Am. J. Orthod. Dentofac. Orthop. 2017, 152, 214–223. [Google Scholar] [CrossRef]
- Gunson, M.J.; Arnett, G.W.; Formby, B.; Falzone, C.; Mathur, R.; Alexander, C. Oral contraceptive pill use and abnormal menstrual cycles in women with severe condylar resorption: A case for low serum 17β-estradiol as a major factor in progressive condylar resorption. Am. J. Orthod. Dentofac. Orthop. 2009, 136, 772–779. [Google Scholar] [CrossRef]
- Yang, H.J.; Hwang, S.J. Bone mineral density and mandibular advancement as contributing factors for postoperative relapse after orthognathic surgery in patients with preoperative idiopathic condylar resorption: A prospective study with preliminary 1-year follow-up. Oral Surg. Oral Med. Oral Pathol. Oral Radiol. 2015, 120, 112–118. [Google Scholar] [CrossRef]
- Alsabban, L.; Amarista, F.J.; Mercuri, L.; Perez, D. Idiopathic condylar resorption: A survey and review of the literature. J. Oral Maxillofac. Surg. 2018, 76, 2316.e1–2316.e13. [Google Scholar] [CrossRef]
- Feng, C.; Ji, P.; Luo, P.; Xu, J. Estrogen-mediated microRNA-101-3p expression represses hyaluronan synthase 2 in synovial fibroblasts from idiopathic condylar resorption patients. J. Oral Maxillofac. Surg. 2019, 77, 1582–1593. [Google Scholar] [CrossRef]
- Wu, Y.; Kadota-Watanabe, C.; Ogawa, T.; Moriyama, K. Combination of estrogen deficiency and excessive mechanical stress aggravates temporomandibular joint osteoarthritis in vivo. Arch. Oral Biol. 2019, 102, 39–46. [Google Scholar] [CrossRef]
- Ootake, T.; Ishii, T.; Sueishi, K.; Watanabe, A.; Ishizuka, Y.; Amano, K.; Nagao, M.; Nishimura, K.; Nishii, Y. Effects of mechanical stress and deficiency of dihydrotestosterone or 17β-estradiol on temporomandibular joint osteoarthritis in mice. Osteoarthr. Cart. 2021, 29, 1575–1589. [Google Scholar] [CrossRef]
- Nogami, S.; Yamauchi, K.; Satomi, N.; Yamaguchi, Y.; Yokota, S.; Abe, Y.; Takahashi, T. Risk factors related to aggressive condylar resorption after orthognathic surgery for females: Retrospective study. Cranio 2017, 35, 250–258. [Google Scholar] [CrossRef] [PubMed]
- Gonçalves, J.R.; Cassano, D.S.; Wolford, L.M.; Santos-Pinto, A.; Márquez, I.M. Postsurgical stability of counterclockwise maxillomandibular advancement surgery: Affect of articular disc repositioning. J. Oral Maxillofac. Surg. 2008, 66, 724–738. [Google Scholar] [CrossRef] [PubMed]
- Dalewski, B.; Białkowska, K.; Pałka, Ł.; Jakubowska, A.; Kiczmer, P.; Sobolewska, E. COL5A1 RS12722 is associated with temporomandibular joint anterior disc displacement without reduction in polish caucasians. Cells 2021, 10, 2423. [Google Scholar] [CrossRef] [PubMed]
- Dalewski, B.; Kamińska, A.; Białkowska, K.; Jakubowska, A.; Sobolewska, E. Association of estrogen receptor 1 and tumor necrosis factor α polymorphisms with temporomandibular joint anterior disc displacement without reduction. Dis. Markers. 2020, 2020, 6351817. [Google Scholar] [CrossRef] [PubMed]
- Politis, C.; Van De Vyvere, G.; Agbaje, J.O. Condylar resorption after orthognathic surgery. J. Craniofac. Surg. 2019, 30, 168–174. [Google Scholar] [CrossRef] [PubMed]
- Hattori-Hara, E.; Mitsui, S.N.; Mori, H.; Arafurue, K.; Kawaoka, T.; Ueda, K.; Yasue, A.; Kuroda, S.; Koolstra, J.H.; Tanaka, E. Influence of unilateral disc displacement on stress in the contralateral joint with normally-positioned disc in human temporomandibular joint. J. Craniomaxillofac. Surg. 2014, 42, 2018–2024. [Google Scholar] [CrossRef]
- Tanaka, E.; Rodrigo, D.P.; Tanaka, M.; Kawaguchi, A.; Shibazaki, T.; Tanne, K. Stress analysis in the TMJ during jaw opening by use of a three-dimensional finite element model based on magnetic resonance images. Int. J. Oral Maxillofac. Surg. 2001, 30, 421–430. [Google Scholar] [CrossRef]
- Munakata, K.; Miyashita, H.; Nakahara, T.; Shiba, H.; Sugahara, K.; Katakura, A.; Nakagawa, T. The use of SPECT/CT to assess resorptive activity in mandibular condyles. Int. J. Oral Maxillofac. Surg. 2021. [Google Scholar] [CrossRef]

{kind=link}
{kind=link}
| ICR | TMD | |||
|---|---|---|---|---|
| Male | 2 | 0.3 | 138 | 20.9 |
| Female | 10 | 0.9 | 312 | 29.1 |
| Total | 12 | 0.7 | 450 | 25.9 |
| ICR (n, 12) | TMD (n, 450) | Control (n, 1273) | ||||
|---|---|---|---|---|---|---|
| n | % | n | % | n | % | |
| Maxillary protrusion | 12 | 100.0 | 122 | 27.1 | 256 | 20.1 |
| Mandibular protrusion | 0 | 0.0 | 66 | 14.7 | 258 | 20.3 |
| Posterior crossbite | 2 | 16.7 | 37 | 8.2 | 75 | 5.9 |
| Open bite | 9 | 75.0 | 52 | 11.6 | 55 | 4.3 |
| Deep bite | 0 | 0.0 | 9 | 2.0 | 23 | 1.8 |
| Crowding | 0 | 0.0 | 144 | 32.0 | 540 | 42.4 |
| Other | 0 | 0.0 | 20 | 4.4 | 66 | 5.2 |
| ICR (n = 12) | TMD (n = 450) | p Value | |
|---|---|---|---|
| Age (years), mean (SD) | 16.4 (4.5) | 17.9 (5.1) | |
| Sex, n | |||
| Female | 10 | 312 | |
| Male | 2 | 138 | |
| Reported history, n (%) | |||
| Joint sounds | 6 (50.0) | 203 (45.1) | 0.36 |
| Joint pain | 5 (41.7) | 110 (24.4) | 0.17 |
| Difficulty of mouth opening | 6 (50.0) | 71 (15.8) | <0.01 |
| Headache | 2 (16.7) | 106 (23.6) | 0.58 |
| Stiff shoulder | 1 (8.3) | 103 (22.9) | 0.23 |
| Masticatory muscle pain | 2 (16.7) | 27 (6.0) | 0.13 |
| arafunctional habits | 8 (66.7) | 292 (64.9) | 0.90 |
| Maxillofacial trauma | 2 (16.7) | 73 (16.2) | 0.96 |
| Orthodontic treatment | 4 (33.3) | 44 (9.8) | <0.01 |
| Objective findings | |||
| Joint sounds | 9 (75.0) | 261 (58.0) | 0.24 |
| Joint pain | 3 (25.0) | 41 (9.1) | 0.06 |
| Masticatory muscle tenderness | 1 (8.3) | 34 (7.6) | 0.92 |
| Mandibular shift at max. opening | 4 (33.3) | 73 (16.2) | 0.11 |
| Maximal mouth-opening (mm) | 35.1 ± 6.6 | 42.4 ± 7.4 | <0.01 |
| Case 1 | Case 2 | Case 3 | Case 4 | Case 5 | Case 6 | Case 7 | Case 8 | Case 9 | Case 10 | Case 11 | Case 12 | |
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Sex | Female | Male | Female | Female | Female | Female | Female | Female | Female | Female | Female | Male |
| Age at onset, years | 16 | 15 | 12 | 17 | 13 | 14 | 10 | 16 | 14 | 14 | 12 | 5 |
| Type of malocclusion | Maxillary protrusion and open bite | Maxillary protrusion and open bite | Maxillary protrusion and open bite | Maxillary protrusion & open bite and posterior crossbite | Maxillary protrusion and open bite | Maxillary protrusion and open bite | Maxillary protrusion and open bite and posterior crossbite | Maxillary protrusion and open bite | Maxillary protrusion and open bite | Maxillary protrusion | Maxillary protrusion | Maxillary protrusion |
| TMD symptoms | (+) | (±) | (−) | (+) | (+) | (−) | (+) | (+) | (+) | (+) | (+) | (+) |
| Orthodontic treatment | (−) | (+) | (+) | (+) | (−) | (−) | (−) | (−) | (−) | (+) | (−) | (−) |
| Third molars extraction | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) |
| History of trauma | (+) | (−) | (+) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) |
| Parafunctional habits | (+) | (−) | (−) | (+) | (−) | (−) | (+) | (+) | (+) | (+) | (+) | (+) |
| Nail biting and chin rest | Thumb sucking and chin rest | Mouth breathing and tongue thrusting | Thumb sucking and mouth breathing | Mouth breathing and chin rest | Chin rest | Tongue thrusting | Nail biting | |||||
| Systemic diseases | (−) | (−) | (−) | (±) | (−) | (−) | (−) | (−) | (+) | (+) | (+) | (−) |
| Oral contraceptive use | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (−) | (+) | (−) |
| Skeletal pattern (before and after onset) | Cl II → Cl II | Cl III → Cl II | Cl II → Cl II | Cl III→ Cl I | Cl II → Cl II | Cl II → Cl II | Cl II→ Cl II | Cl II → Cl II | Cl II → Cl II | Cl II → Cl II | Cl II → Cl II | Cl I → Cl I |
| Mean | SD | p Value | |
|---|---|---|---|
| Condylar width (mm) | |||
| ICR | 14.1 | 2.0 | |
| TMD | 18.0 | 1.6 | |
| Difference | 3.9 | <0.001 | |
| Condylar length (mm) | |||
| ICR | 8.0 | 2.8 | |
| TMD | 8.5 | 1.2 | |
| Difference | 0.5 | 0.51 | |
| Condylar height (mm) | |||
| ICR | 12.6 | 4.1 | |
| TMD | 21.7 | 3.5 | |
| Difference | 9.1 | <0.001 | |
| Condylar axial angle (°) | |||
| ICR | 44.6 | 12.1 | |
| TMD | 73.5 | 6.1 | |
| Difference | 28.9 | <0.001 |
| n (%) | Anterior | Normal | Posterior |
|---|---|---|---|
| ICR | 1 (8.3) | 4 (33.3) | 7 (58.3) |
| TMD | 6 (60.0) | 4 (40.0) | 0 (0.0) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Iwasa, A.; Tanaka, E. Signs, Symptoms, and Morphological Features of Idiopathic Condylar Resorption in Orthodontic Patients: A Survey-Based Study. J. Clin. Med. 2022, 11, 1552. https://doi.org/10.3390/jcm11061552
Iwasa A, Tanaka E. Signs, Symptoms, and Morphological Features of Idiopathic Condylar Resorption in Orthodontic Patients: A Survey-Based Study. Journal of Clinical Medicine. 2022; 11(6):1552. https://doi.org/10.3390/jcm11061552
Chicago/Turabian StyleIwasa, Akihiko, and Eiji Tanaka. 2022. "Signs, Symptoms, and Morphological Features of Idiopathic Condylar Resorption in Orthodontic Patients: A Survey-Based Study" Journal of Clinical Medicine 11, no. 6: 1552. https://doi.org/10.3390/jcm11061552
APA StyleIwasa, A., & Tanaka, E. (2022). Signs, Symptoms, and Morphological Features of Idiopathic Condylar Resorption in Orthodontic Patients: A Survey-Based Study. Journal of Clinical Medicine, 11(6), 1552. https://doi.org/10.3390/jcm11061552