
Therapeutic Effect of Intense Pulsed Light in Patients with Sjögren’s Syndrome Related Dry Eye

 ,
, 
Abstract
:1. Introduction
2. Materials and Methods
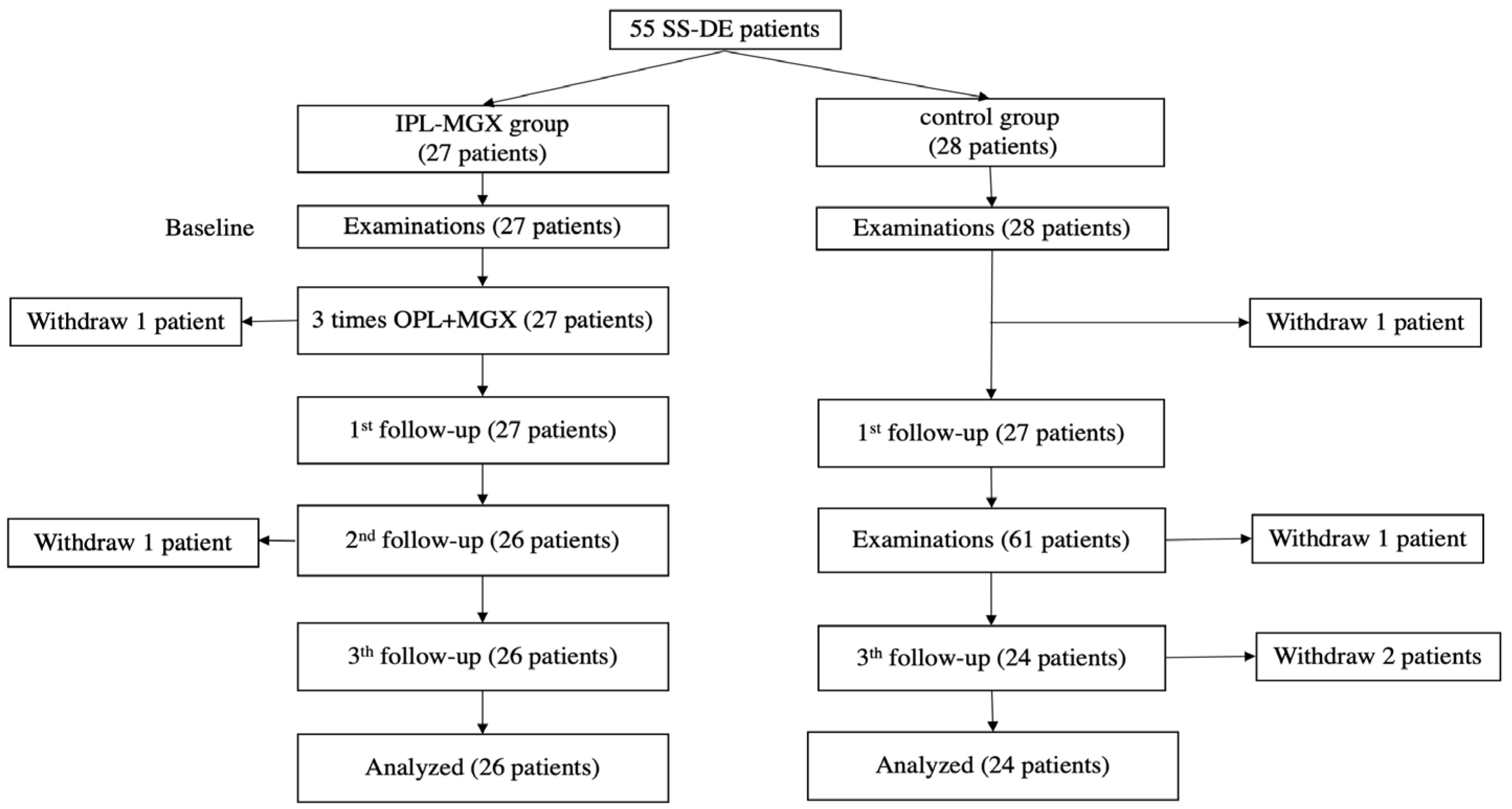
2.1. Subjects
2.2. Experimental Design
2.3. IPL-MGX Treatment
2.4. Clinical Assessment
2.4.1. Ocular Surface Disease Index (OSDI)
2.4.2. Schirmer’s I Test (SIT)
2.4.3. Tear Meniscus Height (TMH) and Conjunctival Hyperemia
2.4.4. Tear Film Stability
2.4.5. Corneal Fluorescein Staining (CFS)
2.4.6. Meibomian Gland (MG) Morphology
2.4.7. Eyelid Margin Abnormalities
2.4.8. Meibomian Gland Expression (MGX)
2.4.9. Meibum Quality
2.4.10. Safety Assessments
2.5. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Moutsopoulos, H.M. Sjogren’s syndrome: Autoimmune epithelitis. Clin. Immunol. Immunopathol. 1994, 72, 162–165. [Google Scholar] [CrossRef] [PubMed]
- Skopouli, F.N.; Fox, P.C.; Galanopoulou, V.; Atkinson, J.C.; Jaffe, E.S.; Moutsopoulos, H.M. T cell subpopulations in the labial minor salivary gland histopathologic lesion of Sjogren’s syndrome. J. Rheumatol. 1991, 18, 210–214. [Google Scholar] [PubMed]
- Uchino, M.; Schaumberg, D.A. Dry Eye Disease: Impact on Quality of Life and Vision. Curr. Ophthalmol. Rep. 2013, 1, 51–57. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bjordal, O.; Norheim, K.B.; Rodahl, E.; Jonsson, R.; Omdal, R. Primary Sjogren’s syndrome and the eye. Surv. Ophthalmol. 2020, 65, 119–132. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wang, Y.; Qin, Q.; Liu, B.; Fu, Y.; Lin, L.; Huang, X.; Jin, X. Clinical Analysis: Aqueous-Deficient and Meibomian Gland Dysfunction in Patients With Primary Sjogren’s Syndrome. Front. Med. 2019, 6, 291. [Google Scholar] [CrossRef]
- Foulks, G.N.; Forstot, S.L.; Donshik, P.C.; Forstot, J.Z.; Goldstein, M.H.; Lemp, M.A.; Nelson, J.D.; Nichols, K.K.; Pflugfelder, S.C.; Tanzer, J.M.; et al. Clinical guidelines for management of dry eye associated with Sjogren disease. Ocul. Surf. 2015, 13, 118–132. [Google Scholar] [CrossRef]
- Hong, S.; Kim, T.; Chung, S.H.; Kim, E.K.; Seo, K.Y. Recurrence after topical nonpreserved methylprednisolone therapy for keratoconjunctivitis sicca in Sjogren’s syndrome. J. Ocul. Pharmacol. Ther. 2007, 23, 78–82. [Google Scholar] [CrossRef]
- Sall, K.; Stevenson, O.D.; Mundorf, T.K.; Reis, B.L. Two multicenter, randomized studies of the efficacy and safety of cyclosporine ophthalmic emulsion in moderate to severe dry eye disease. CsA Phase 3 Study Group. Ophthalmology 2000, 107, 631–639. [Google Scholar] [CrossRef]
- Rosenberg, E.S.; Asbell, P.A. Essential fatty acids in the treatment of dry eye. Ocul. Surf. 2010, 8, 18–28. [Google Scholar] [CrossRef]
- Qiu, W.; Liu, Z.; Ao, M.; Li, X.; Wang, W. Punctal plugs versus artificial tears for treating primary Sjogren’s syndrome with keratoconjunctivitis SICCA: A comparative observation of their effects on visual function. Rheumatol. Int. 2013, 33, 2543–2548. [Google Scholar] [CrossRef]
- Petznick, A.; Tong, L.; Chung, R.; Wang, J.C.; Koh, M.; Salleh, R.; Waduthantri, S. Autologous plasma eyedrops prepared in a closed system: A treatment for dry eye. Eye 2013, 27, 1102. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Craig, J.P.; Chen, Y.H.; Turnbull, P.R. Prospective trial of intense pulsed light for the treatment of meibomian gland dysfunction. Investig. Ophthalmol. Vis. Sci. 2015, 56, 1965–1970. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Dell, S.J.; Gaster, R.N.; Barbarino, S.C.; Cunningham, D.N. Prospective evaluation of intense pulsed light and meibomian gland expression efficacy on relieving signs and symptoms of dry eye disease due to meibomian gland dysfunction. Clin. Ophthalmol. 2017, 11, 817–827. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Huo, Y.; Mo, Y.; Wu, Y.; Fang, F.; Jin, X. Therapeutic effect of intense pulsed light with optimal pulse technology on meibomian gland dysfunction with and without ocular Demodex infestation. Ann. Transl. Med. 2021, 9, 238. [Google Scholar] [CrossRef] [PubMed]
- Arita, R.; Fukuoka, S.; Mizoguchi, T.; Morishige, N. Multicenter Study of Intense Pulsed Light for Patients with Refractory Aqueous-Deficient Dry Eye Accompanied by Mild Meibomian Gland Dysfunction. J. Clin. Med. 2020, 9, 3467. [Google Scholar] [CrossRef]
- Shiboski, S.C.; Shiboski, C.H.; Criswell, L.; Baer, A.; Challacombe, S.; Lanfranchi, H.; Schiodt, M.; Umehara, H.; Vivino, F.; Zhao, Y.; et al. American College of Rheumatology classification criteria for Sjogren’s syndrome: A data-driven, expert consensus approach in the Sjogren’s International Collaborative Clinical Alliance cohort. Arthritis Care Res. 2012, 64, 475–487. [Google Scholar] [CrossRef] [PubMed]
- Fitzpatrick, T.B. The validity and practicality of sun-reactive skin types I through VI. Arch. Dermatol. 1988, 124, 869–871. [Google Scholar] [CrossRef]
- Hong, H.; Choi, Y.; Hahn, S.; Park, S.K.; Park, B.J. Nomogram for sample size calculation on a straightforward basis for the kappa statistic. Ann. Epidemiol. 2014, 24, 673–680. [Google Scholar] [CrossRef]
- Zhang, X.; Song, N.; Gong, L. Therapeutic Effect of Intense Pulsed Light on Ocular Demodicosis. Curr. Eye Res. 2019, 44, 250–256. [Google Scholar] [CrossRef]
- Arita, R.; Fukuoka, S.; Morishige, N. Therapeutic efficacy of intense pulsed light in patients with refractory meibomian gland dysfunction. Ocul. Surf. 2019, 17, 104–110. [Google Scholar] [CrossRef]
- Wei, Y.; Asbell, P.A. The core mechanism of dry eye disease is inflammation. Eye Contact Lens 2014, 40, 248–256. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yan, X.; Hong, J.; Jin, X.; Chen, W.; Rong, B.; Feng, Y.; Huang, X.; Li, J.; Song, W.; Lin, L.; et al. The Efficacy of Intense Pulsed Light Combined With Meibomian Gland Expression for the Treatment of Dry Eye Disease Due to Meibomian Gland Dysfunction: A Multicenter, Randomized Controlled Trial. Eye Contact Lens 2021, 47, 45–53. [Google Scholar] [CrossRef] [PubMed]



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristic | IPL-MGX Group (n = 26) | Control Group (n = 24) | p-Value | |
|---|---|---|---|---|
| Age (year), mean SD (range) | 53.46 ± 10.71 (32–78) | 51.71 ± 13.32 (30–67) | 0.861 | |
| Sex (male/female) | 1/25 | 0/24 | 1.000 | |
| History of DE (years), mean SD (range) | 6.38 ± 4.34 (1–14) | 6.92 ± 5.14 (1–16) | 0.792 | |
| History of SS (years), mean SD (range) | 8.19 ± 4.72 (1–17) | 8.29 ± 5.38 (1–20) | 0.961 | |
| Refractory SS-DE | 23 (88.46%) | 21 (87.5%) | 1.000 | |
| Previous treatments | Lubricant eyedrops or ointment | 26 | 23 | 0.968 |
| warm compress and massage | 23 | 22 | 1.000 | |
| Topical anti-inflammatory | 19 | 17 | 0.860 | |
| Contact lenses | 1 | 1 | 1.000 | |
| Moisture chamber spectacles | 2 | 1 | 1.000 | |
| Punctal plugs | 1 | 1 | 1.000 | |
| Systemic immunosuppression | 14 | 11 | 0.571 | |
| Characteristic | Group | BL | 9 Weeks after Treatment Onset | 12 Weeks after Treatment Onset | 15 Weeks after Treatment Onset | |||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Mean ± SD | p-Value for | Mean ± SD | p-Value vs. | p-Value for | Mean ± SD | p-Value vs. | p-Value for | Mean ± SD | p-Value vs. | p-Value for | ||
| IPL-MGX vs. Control | BL | IPL-MGX vs. Control | BL | IPL-MGX vs. Control | BL | IPL-MGX vs. Control | ||||||
| BCVA (logMAR) | IPL-MGX group | 0.31 ± 0.29 | 0.625 | 0.15 ± 0.17 | 0.001 | 0.352 | 0.15 ± 0.17 | <0.001 | 0.341 | 0.16 ± 0.18 | <0.001 | 0.352 |
| control | 0.31 ± 0.37 | 0.30 ± 0.36 | 0.109 | 0.31 ± 0.37 | 0.581 | 0.31 ± 0.38 | 1.000 | |||||
| OSDI (0–100) | IPL-MGX group | 77.20 ± 15.18 | 0.934 | 48.34 ± 18.70 | <0.001 | <0.001 | 41.57 ± 17.14 | <0.001 | <0.001 | 44.42 ± 15.44 | <0.001 | <0.001 |
| Control | 76.68 ± 16.39 | 72.07 ± 18.70 | 0.002 | 72.53 ± 16.31 | 0.028 | 70.74 ± 16.80 | 0.002 | |||||
| Conjunctival congestion | IPL-MGX group | 1.82 ± 0.77 | 0.831 | 1.65 ± 0.58 | 0.074 | 0.606 | 1.55 ± 0.56 | 0.005 | 0.163 | 1.53 ± 0.58 | 0.002 | 0.227 |
| Control | 1.80 ± 0.66 | 1.75 ± 0.64 | 0.087 | 1.80 ± 0.67 | 0.885 | 1.75 ± 0.62 | 0.091 | |||||
| TMH (mm) | IPL-MGX group | 0.13 ± 0.04 | 0.453 | 0.14 ± 0. 04 | 0.253 | 0.869 | 0.16 ± 0.04 | 0.013 | 0.453 | 0.15 ± 0.03 | 0.037 | 0.837 |
| Control | 0.14 ± 0.04 | 0.14 ± 0.04 | 0.445 | 0.15 ± 0.04 | 0.005 | 0.15 ± 0.04 | <0.001 | |||||
| SIT (mm/5min) | IPL-MGX group | 3.42 ± 2.80 | 0.929 | 4.27 ± 2.99 | 0.248 | 0.337 | 3.85 ± 1.74 | 0.201 | 0.798 | 4.62 ± 2.45 | 0.024 | 0.306 |
| Control | 3.62 ± 3.00 | 3.75 ± 3.34 | 0.718 | 4.20 ± 3.37 | 0.054 | 4.08 ± 3.27 | 0.069 | |||||
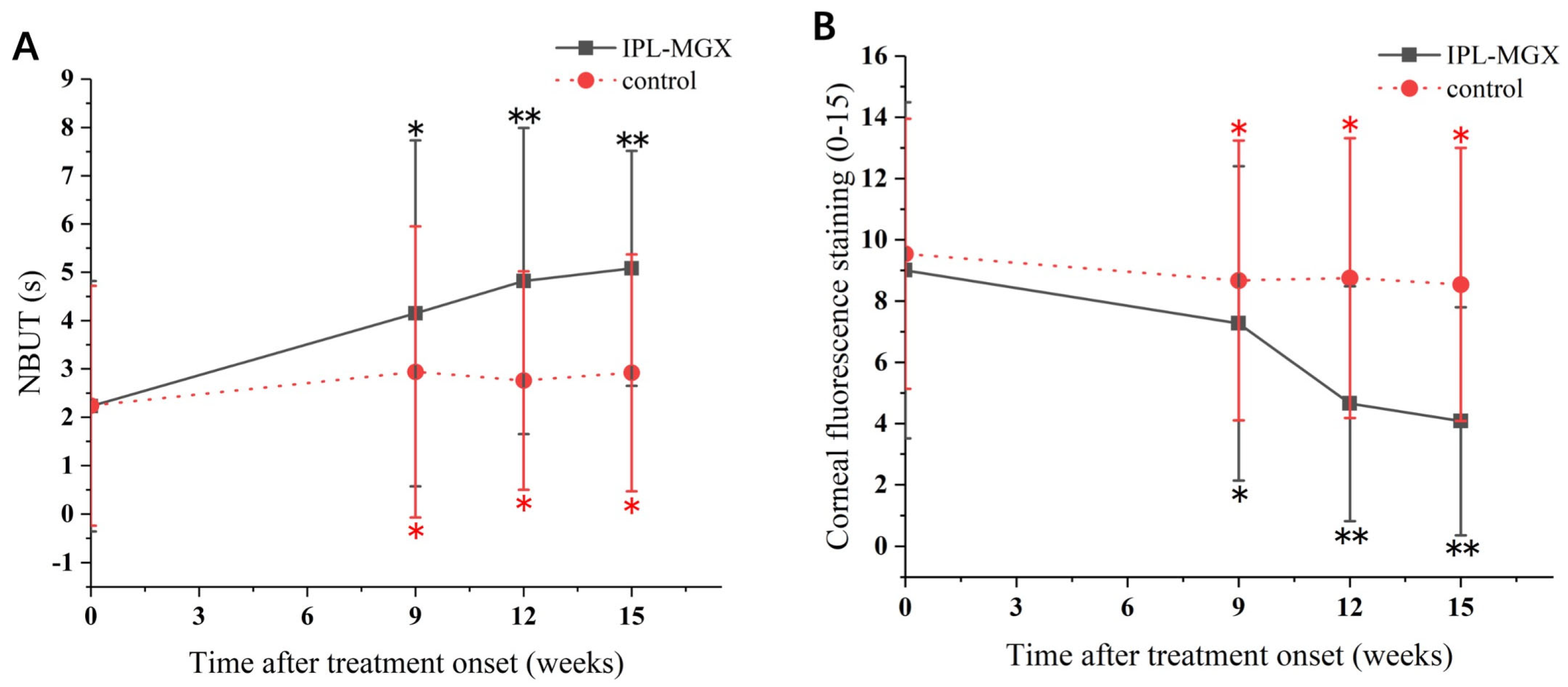
| NBUT (s) | IPL-MGX group | 2.23 ± 2.59 | 0.800 | 4.15 ± 3.58 | 0.001 | 0.551 | 4.82 ± 3.17 | <0.001 | 0.009 | 5.08 ± 2.433 | <0.001 | 0.006 |
| Control | 2.24 ± 2.48 | 2.94 ± 3.01 | 0.001 | 2.76 ± 2.26 | 0.019 | 2.92 ± 2.45 | 0.007 | |||||
| Corneal fluorescence staining (0–15) | IPL-MGX group | 9.00 ± 5.49 | 0.822 | 7.27 ± 5.13 | 0.001 | 0.399 | 4.65 ± 3.83 | <0.001 | 0.001 | 4.08 ± 3.72 | <0.001 | 0.001 |
| Control | 9.54 ± 4.41 | 8.67 ± 4.57 | 0.002 | 8.75 ± 4.57 | 0.003 | 8.54 ± 4.46 | 0.003 | |||||
| MG dropouts (0–3) | IPL-MGX group | 1.58 ± 1.24 | 0.502 | 1.46 ± 1.217 | 0.257 | 0.283 | 1.46 ± 1.17 | 0.257 | 0.283 | 1.46 ± 1.17 | 0.257 | 0.283 |
| control | 1.79 ± 1.10 | 1.79 ± 1.10 | 1.000 | 1.79 ± 1.10 | 1.000 | 1.79 ± 1.1 | 1.000 | |||||
| Lid margin abnormality (0–4) | IPL-MGX group | 2.73 ± 1.34 | 0.968 | 1.96 ± 0.96 | <0.001 | 0.026 | 1.92 ± 0.93 | <0.001 | 0.012 | 1.96 ± 0.10 | <0.001 | 0.019 |
| control | 2.75 ± 1.33 | 2.67 ± 1.27 | 0.317 | 2.70 ± 1.29 | 0.083 | 2.67 ± 1.24 | 0.157 | |||||
| MG expressibility (0–9) | IPL-MGX group | 6.00 ± 3.29 | 0.733 | 3.88 ± 2.72 | <0.001 | 0.026 | 3.73 ± 2.22 | <0.001 | 0.040 | 4.12 ± 2.32 | 0.002 | 0.094 |
| control | 5.83 ± 3.12 | 5.71 ± 3.00 | 0.429 | 5.21 ± 2.89 | 0.001 | 5.25 ± 2.91 | 0.003 | |||||
| meibum quality (0–24) | IPL-MGX group | 5.92 ± 7.16 | 0.360 | 13.26 ± 8.40 | <0.001 | 0.003 | 15.35 ± 7.49 | <0.001 | <0.001 | 14.92 ± 6.25 | <0.001 | 0.001 |
| control | 6.88 ± 7.57 | 7.21 ± 7.73 | 0.114 | 7.54 ± 7.58 | 0.013 | 7.63 ± 7.60 | 0.007 | |||||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Huo, Y.; Wan, Q.; Hou, X.; Zhang, Z.; Zhao, J.; Wu, Z.; Jin, X. Therapeutic Effect of Intense Pulsed Light in Patients with Sjögren’s Syndrome Related Dry Eye. J. Clin. Med. 2022, 11, 1377. https://doi.org/10.3390/jcm11051377
Huo Y, Wan Q, Hou X, Zhang Z, Zhao J, Wu Z, Jin X. Therapeutic Effect of Intense Pulsed Light in Patients with Sjögren’s Syndrome Related Dry Eye. Journal of Clinical Medicine. 2022; 11(5):1377. https://doi.org/10.3390/jcm11051377
Chicago/Turabian StyleHuo, Yanan, Qi Wan, Xinzhu Hou, Zhiyong Zhang, Jinchuan Zhao, Zhiyi Wu, and Xiuming Jin. 2022. "Therapeutic Effect of Intense Pulsed Light in Patients with Sjögren’s Syndrome Related Dry Eye" Journal of Clinical Medicine 11, no. 5: 1377. https://doi.org/10.3390/jcm11051377
APA StyleHuo, Y., Wan, Q., Hou, X., Zhang, Z., Zhao, J., Wu, Z., & Jin, X. (2022). Therapeutic Effect of Intense Pulsed Light in Patients with Sjögren’s Syndrome Related Dry Eye. Journal of Clinical Medicine, 11(5), 1377. https://doi.org/10.3390/jcm11051377