
Symptoms of Infarction in Women: Is There a Real Difference Compared to Men? A Systematic Review of the Literature with Meta-Analysis

 , , ,
, , ,
Abstract
1. Introduction
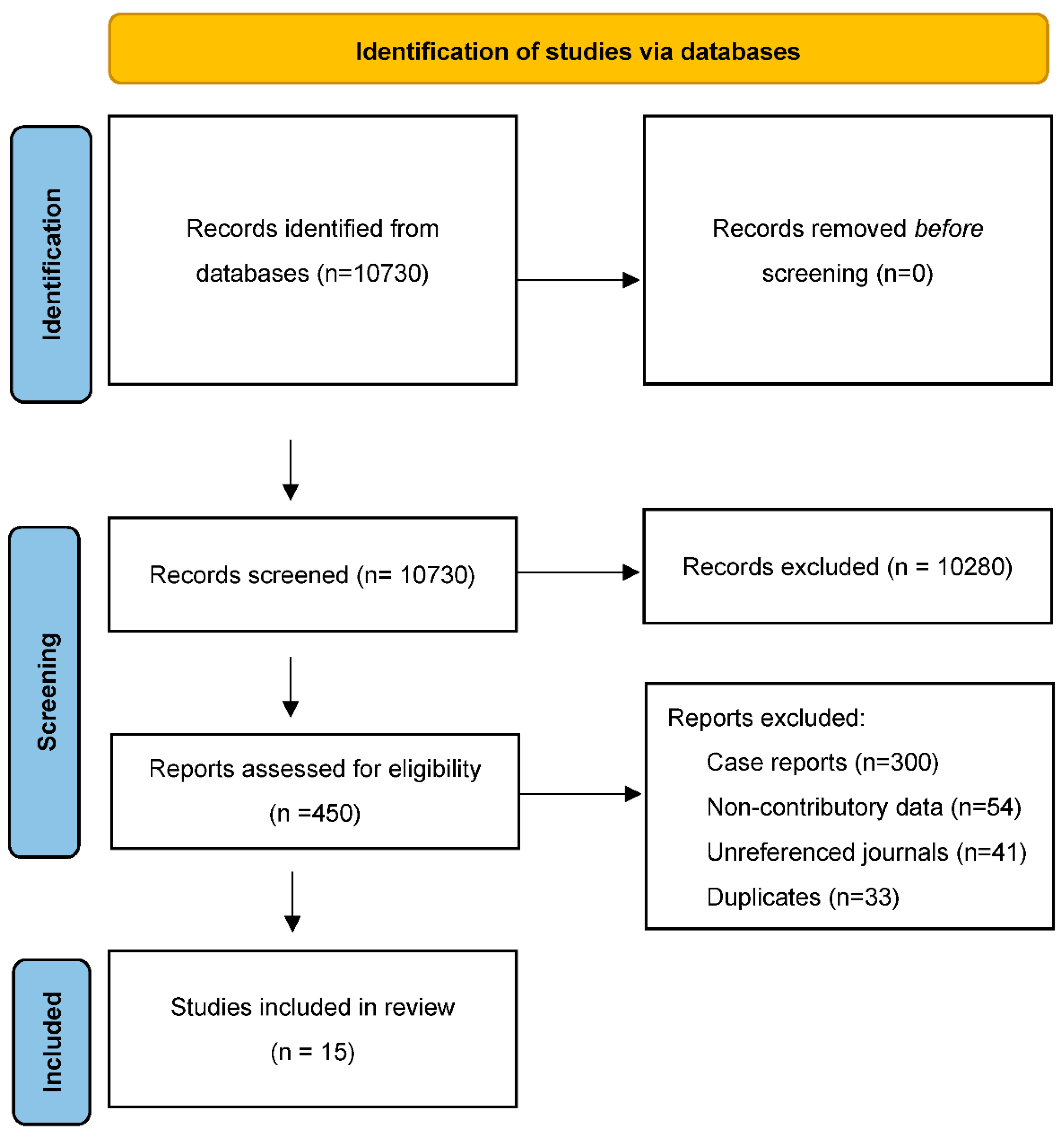
2. Materials and Methods
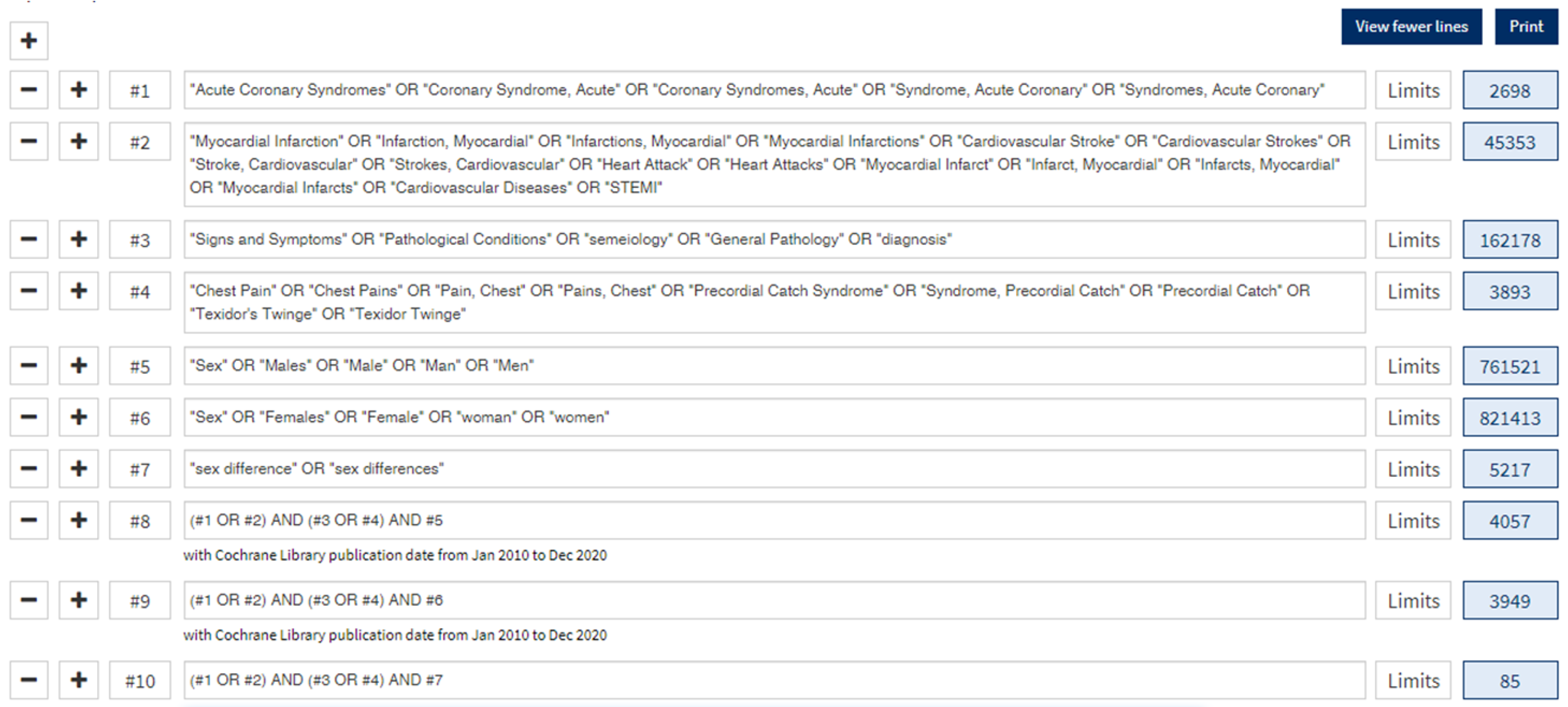
2.1. Study Design
2.2. Data Collection and Processing
2.3. Quality Assessment
2.4. Statistical Analysis
3. Results
3.1. Characteristics of Included Studies
3.2. Patients’ Characteristics
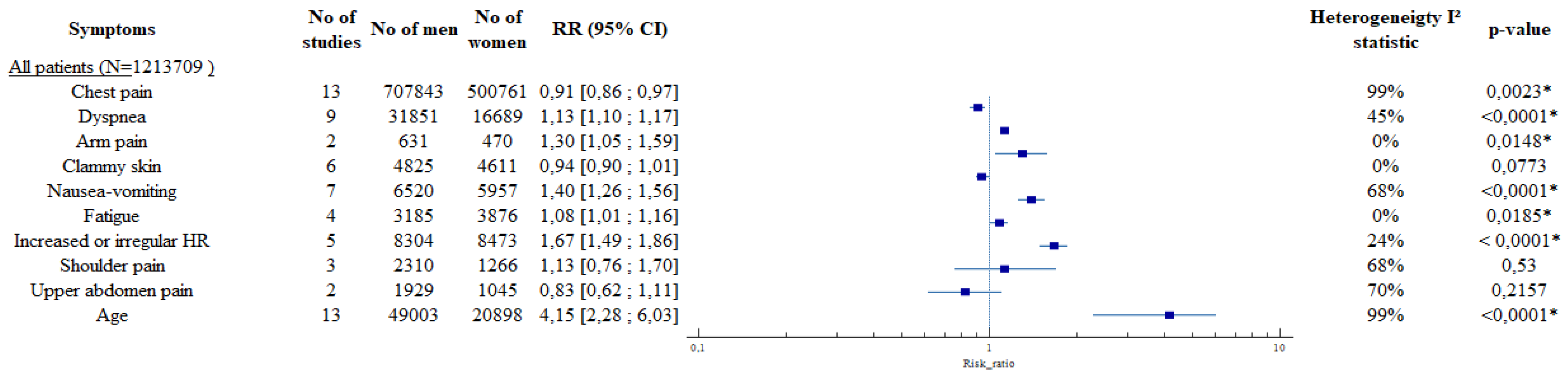
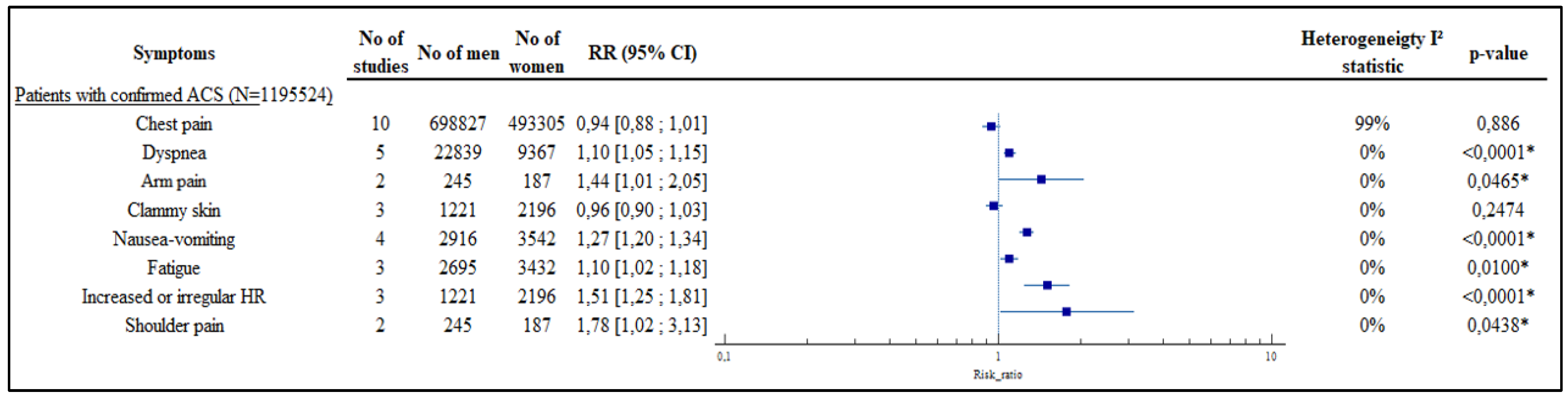
3.3. Symptoms
4. Discussion
Limitations
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Cardiovascular Diseases. 2017. Available online: https://www.who.int/fr/news-room/fact-sheets/detail/cardiovascular-diseases-(cvds) (accessed on 4 August 2021).
- World Health Organization. The Top 10 Causes of Death. Available online: https://www.who.int/fr/news-room/fact-sheets/detail/the-top-10-causes-of-death (accessed on 4 August 2021).
- Thygesen, K.; Alpert, J.S.; Jaffe, A.S.; Chaitman, B.R.; Bax, J.J.; Morrow, D.A.; White, H.D.; Executive Group on behalf of the Joint European Society of Cardiology (ESC)/American College of Cardiology (ACC)/American Heart Association (AHA)/World Heart Federation (WHF) Task Force for the Universal Definition of Myocardial Infarction. Fourth Universal Definition of Myocardial Infarction (2018). Circulation 2018, 138, e618–e651. [Google Scholar] [CrossRef] [PubMed]
- Collet, J.P.; Thiele, H.; Barbato, E.; Barthélémy, O.; Bauersachs, J.; Bhatt, D.L.; Dendale, P.; Dorobantu, M.; Edvardsen, T.; Folliguet, T.; et al. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur. Heart J. 2021, 42, 1289–1367. [Google Scholar] [CrossRef]
- DeVon, H.A.; Mirzaei, S.; Zègre-Hemsey, J. Typical and Atypical Symptoms of Acute Coronary Syndrome: Time to Retire the Terms? J. Am. Heart Assoc. 2020, 9, e015539. [Google Scholar] [CrossRef] [PubMed]
- Park, J.-S.; Kim, Y.-J.; Shin, D.-G.; Jeong, J.-O.; Ahn, Y.-K.; Chung, W.-S.; Seung, K.-B.; Kim, C.-J.; Cho, M.-C.; Jang, Y.-S.; et al. Gender Differences in Clinical Features and In-hospital Outcomes in ST-segment Elevation Acute Myocardial Infarction: From the Korean Acute Myocardial Infarction Registry (KAMIR) Study. Clin. Cardiol. 2010, 33, E1–E6. [Google Scholar] [CrossRef] [PubMed]
- Butala, N.M.; Desai, M.M.; Linnander, E.L.; Wong, Y.R.; Mikhail, D.G.; Ott, L.S.; Spertus, J.A.; Bradley, E.H.; Aaty, A.A.; Abdelfattah, A.; et al. Gender Differences in Presentation, Management, and In-Hospital Outcomes for Patients with AMI in a Lower-Middle Income Country: Evidence from Egypt. PLoS ONE 2011, 6, e25904. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, J.H.; Leifheit-Limson, E.C.; Watanabe, E.; Allen, N.B.; Garavalia, B.; Garavalia, L.S.; Spertus, J.A.; Krumholz, H.M.; Curry, L.A. Symptom Recognition and Healthcare Experiences of Young Women With Acute Myocardial Infarction. Circ. Cardiovasc. Qual. Outcomes 2015, 8, S31–S38. [Google Scholar] [CrossRef] [PubMed]
- Bjerking, L.H.; Hansen, K.W.; Madsen, M.; Jensen, J.S.; Madsen, J.K.; Sørensen, R.; Galatius, S. Use of diagnostic coronary angiography in women and men presenting with acute myocardial infarction: A matched cohort study. BMC Cardiovasc. Disord. 2016, 16, 120. [Google Scholar] [CrossRef]
- Canto, J.G.; Rogers, W.J.; Goldberg, R.J.; Peterson, E.D.; Wenger, N.K.; Vaccarino, V.; Kiefe, C.I.; Frederick, P.; Sopko, G.; Zheng, Z.-J.; et al. Association of Age and Sex with Myocardial Infarction Symptom Presentation and In-Hospital Mortality. JAMA J. Am. Med. Assoc. 2012, 307, 813–822. [Google Scholar] [CrossRef]
- Devon, H.A.; Rosenfeld, A.; Steffen, A.D.; Daya, M. Sensitivity, specificity, and sex differences in symptoms reported on the 13-item acute coronary syndrome checklist. J. Am. Heart Assoc. 2014, 3, e000586. [Google Scholar] [CrossRef]
- Ferry, A.V.; Anand, A.; Strachan, F.E.; Mooney, L.; Stewart, S.D.; Marshall, L.; Chapman, A.; Lee, K.K.; Jones, S.; Orme, K.; et al. Presenting Symptoms in Men and Women Diagnosed with Myocardial Infarction Using Sex-Specific Criteria. J. Am. Heart Assoc. 2019, 8, e012307. [Google Scholar] [CrossRef]
- Rubini Gimenez, M.; Reiter, M.; Twerenbold, R.; Reichlin, T.; Wildi, K.; Haaf, P.; Wicki, K.; Zellweger, C.; Hoeller, R.; Moehring, B.; et al. Sex-specific chest pain characteristics in the early diagnosis of acute myocardial infarction. JAMA Intern. Med. 2014, 174, 241–249. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.K.; Ferry, A.V.; Anand, A.; Strachan, F.E.; Chapman, A.; Kimenai, D.M.; Meex, S.J.; Berry, C.; Findlay, I.; Reid, A.; et al. Sex-Specific Thresholds of High-Sensitivity Troponin in Patients with Suspected Acute Coronary Syndrome. J. Am. Coll. Cardiol. 2019, 74, 2032–2043. [Google Scholar] [CrossRef] [PubMed]
- Lichtman, J.H.; Leifheit, E.C.; Safdar, B.; Bao, H.; Krumholz, H.M.; Lorenze, N.P.; Daneshvar, M.; Spertus, J.A.; D’Onofrio, G. Sex Differences in the Presentation and Perception of Symptoms Among Young Patients with Myocardial Infarction: Evidence from the VIRGO Study (Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients). Circulation 2018, 137, 781–790. [Google Scholar] [CrossRef] [PubMed]
- Nanna, M.G.; Hajduk, A.; Krumholz, H.M.; Murphy, T.E.; Dreyer, R.P.; Alexander, K.P.; Mary Geda, M.; Tsang, S.; Welty, F.K.; Safdar, B.; et al. Sex-Based Differences in Presentation, Treatment, and Complications among Older Adults Hospitalized for Acute Myocardial Infarction: The SILVER-AMI Study. Circ. Cardiovasc. Qual. Outcomes 2019, 12, e005691. [Google Scholar] [CrossRef]
- Patel, A.; Vishwanathan, S.; Nair, T.; Bahuleyan, C.G.; Jayaprakash, V.L.; Baldridge, A.S.; Huffman, M.; Prabhakaran, D.; Mohanan, P.P. Sex Differences in the Presentation, Diagnosis, and Management of Acute Coronary Syndromes: Findings from the Kerala-India ACS Registry. Glob. Heart 2015, 10, 273–280. [Google Scholar] [CrossRef] [PubMed]
- Pelter, M.M.; Riegel, B.; McKinley, S.; Moser, D.K.; Doering, L.V.; Meischke, H.; Davidson, P.; Baker, H.; Yang, W.; Dracup, K. Are there symptom differences in patients with coronary artery disease presenting to the ED ultimately diagnosed with or without ACS? Am. J. Emerg. Med. 2012, 30, 1822–1828. [Google Scholar] [CrossRef]
- Shah, A.; Griffiths, M.; Lee, K.K.; McAllister, D.; Hunter, A.L.; Ferry, A.V.; Cruikshank, A.; Reid, A.; Stoddart, M.; Strachan, F.; et al. High sensitivity cardiac troponin and the under-diagnosis of myocardial infarction in women: Prospective cohort study. BMJ 2015, 350, g7873. [Google Scholar] [CrossRef]
- Shehab, A.; Bhagavathula, A.S.; Alhabib, K.F.; Ullah, A.; Suwaidi, J.A.; Almahmeed, W.; AlFaleh, H.; Zubaid, M. Age-Related Sex Differences in Clinical Presentation, Management, and Outcomes in ST-Segment-Elevation Myocardial Infarction: Pooled Analysis of 15 532 Patients From 7 Arabian Gulf Registries. J. Am. Heart Assoc. 2020, 9, e013880. [Google Scholar] [CrossRef] [PubMed]
- Sörensen, N.A.; Neumann, J.T.; Ojeda, F.; Schäfer, S.; Magnussen, C.; Keller, T.; Lackner, K.J.; Zeller, T.; Karakas, M.; Münzel, T.; et al. Relations of Sex to Diagnosis and Outcomes in Acute Coronary Syndrome. J. Am. Heart Assoc. 2018, 7, e007297. [Google Scholar] [CrossRef]
- van der Meer, M.G.; Backus, B.E.; van der Graaf, Y.; Cramer, M.J.; Appelman, Y.; Doevendans, P.A.; Six, A.J.; Nathoe, H.M. The diagnostic value of clinical symptoms in women and men presenting with chest pain at the emergency department, a prospective cohort study. PLoS ONE 2015, 10, e0116431. [Google Scholar] [CrossRef]
- You, B.; Zhu, B.; Su, X.; Liu, F.; Wang, B. Gender Differences among Elderly Patients with Primary Percutaneous Coronary Intervention. Aging Dis. 2018, 9, 852–860. [Google Scholar] [CrossRef] [PubMed]
- Perrino, C.; Ferdinandy, P.; Bøtker, H.E.; Brundel, B.J.J.M.; Collins, P.; Davidson, S.M.; den Ruijter, H.M.; Engel, F.B.; Gerdts, E.; Girao, H.; et al. Improving translational research in sex-specific effects of comorbidities and risk factors in ischaemic heart disease and cardioprotection: Position paper and recommendations of the ESC Working Group on Cellular Biology of the Heart. Cardiovasc Res. 2021, 117, 367–385. [Google Scholar] [CrossRef]
- Canto, J.G.; Goldberg, R.J.; Hand, M.M.; Bonow, R.O.; Sopko, G.; Pepine, C.J.; Long, T. Symptom presentation of women with acute coronary syndromes: Myth vs reality. Arch. Intern. Med. 2007, 167, 2405–2413. [Google Scholar] [CrossRef] [PubMed]
- Arslanian-Engoren, C.; Patel, A.; Fang, J.; Armstrong, D.; Kline-Rogers, E.; Duvernoy, C.S.; Eagle, K.A. Symptoms of Men and Women Presenting With Acute Coronary Syndromes. Am. J. Cardiol. 2006, 98, 1177–1181. [Google Scholar] [CrossRef]
- Jneid, H.; Fonarow, G.; Cannon, C.P.; Hernandez, A.F.; Palacios, I.F.; Maree, A.; Wells, Q.; Bozkurt, B.; LaBresh, K.A.; Liang, L.; et al. Sex Differences in Medical Care and Early Death After Acute Myocardial Infarction. Circulation 2008, 118, 2803–2810. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G.; PRISMA Group. Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. PLoS Med. 2009, 6, e1000097. [Google Scholar] [CrossRef]
- Wells, G.A. The Ottawa Hospital Research Institute. Available online: http://www.ohri.ca/programs/clinical_epidemiology/oxford.asp (accessed on 26 August 2021).
- Dey, S.; Flather, M.D.; Devlin, G.; Brieger, D.; Gurfinkel, E.P.; Steg, P.G.; Fitzgerald, G.; Jackson, E.A.; Eagle, K.A.; Global Registry of Acute Coronary Events Investigators. Sex-related differences in the presentation, treatment and outcomes among patients with acute coronary syndromes: The Global Registry of Acute Coronary Events. Heart 2009, 95, 20–26. [Google Scholar] [CrossRef] [PubMed]
- Kirchberger, I.; Heier, M.; Kuch, B.; Wende, R.; Meisinger, C. Sex Differences in Patient-Reported Symptoms Associated with Myocardial Infarction (from the Population-Based MONICA/KORA Myocardial Infarction Registry). Am. J. Cardiol. 2011, 107, 1585–1589. [Google Scholar] [CrossRef]
- van Oosterhout, R.E.M.; de Boer, A.R.; Maas, A.H.E.M.; Rutten, F.H.; Bots, M.L.; Peters, S.A.E. Sex Differences in Symptom Presentation in Acute Coronary Syndromes: A Systematic Review and Meta-analysis. J. Am. Heart Assoc. 2020, 9, e014733. [Google Scholar] [CrossRef]
- Connaitre les Numéros D’urgence. Available online: https://www.gouvernement.fr/risques/connaitre-les-numeros-d-urgence (accessed on 5 August 2021).
- Harvard Medical School. Chest Pain. Available online: https://www.health.harvard.edu/decision_guide/chest-pain#yesiamexperiencingonormoreofthesesymptoms (accessed on 5 August 2021).
- Birnbach, B.; Höpner, J.U.; Mikolajczyk, R. Cardiac symptom attribution and knowledge of the symptoms of acute myocardial infarction: A systematic review. BMC Cardiovasc. Disord. 2020, 20, 445. [Google Scholar] [CrossRef]
- Fédération Française de Cardiologie. Rétrospective de Nos Campagnes Vidéo. Available online: https://fedecardio.org/nous-connaitre/retrospective-publicitaire/ (accessed on 5 August 2021).





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Author, Year Published, Journal | Impact Factor 2018 | Adapted Newcastle-Ottawa Scale | Region, State, Country | Study Group | Design | ACS Definition for Inclusion | Sample Size | Men | Women |
|---|---|---|---|---|---|---|---|---|---|
| Bjerking, 2016, BMC Cardiovasc Disord [9] | 1.947 | 4 + 1 = 5 | Denmark | 4000 patients admitted with first AMI 250 females randomly selected; 250 males matched on age and availability of cardiac invasive facilities in the index hospital. 1 patent excluded because of no access to medical record | Matched cohort study | ICD 10th edition codes for ACS I21-I21.9 | 499 | 249 | 250 |
| Canto, 2012, JAMA [10] | 51.273 | 4 + 2 = 6 | U.S.A. | 1977 hospitals who participated at the National Registry of Myocardial Infarction (NRMI) | Observational Study | ICD 9th edition 410.X1 OR supporting evidence of MI (elevated cardiac biomarker level, electrocardiographic evidence of ACS, or alternative enzymatic, nuclear cardiac imaging, or autopsy evidence indicative of ACS) | 1,143,513 | 661,932 | 481,581 |
| DeVon, 2014, J Am Heart Assoc [11] | 4.66 | 4 + 2 + 1 = 7 | U.S.A. | Patients admitted in 4 large medical centers: 1 in the Midwest, 2 in the Pacific Northwest, 1 in the West region of the United States | Prospective Observational Study | ECG criteria (new ST elevation at the J-point > 0.1 mV in 2 contiguous leads and/or new horizontal or down-sloping ST depression > 0.05 mV in 2 contiguous leads and/or T inversion > 0.1 mV in 2 contiguous leads with prominent R wave) and/or troponin criteria (outside the referenced norm for the institution) | 736 | 464 | 272 |
| Ferry, 2019, J Am Heart Assoc [12] | 4.66 | 4 + 2 = 6 | Scotland | Patients admitted in the ED of the Royal Infirmary of Edinburgh for suspected ACS | Substudy of a prospective trial | requested cardiac troponin for suspected ACS | 1941 | 1185 | 756 |
| Gimenez, 2014, JAMA Int Med [13] | 20.768 | 4 + 1 = 5 | Switzerland, Spain, Italy | Patients admitted in 9 study centers who participated at the Advantageous Predictors of Acute Coronary Syndrome Evaluation (APACE) study, with symptoms suggestive of AMI | Prospective Observational Study | acute chest pain with an onset or peak within the last 12 h | 2475 | 1679 | 796 |
| Lee, 2019, J Am Col Cardiol [14] | 18.639 | 4 + 2 = 6 | Scotland | All patients with suspected ACS who presented in the 10 participating hospitals of the High-Sensitivity Troponin in the Evaluation of Patients | Stepped-wedge, cluster-randomized controlled trial | suspected acute coronary syndrome and had paired troponin measurement with the contemporary and the trial assay | 10,360 | 5369 | 4991 |
| Lichtman, 2018, Circulation [15] | 23.054 | 4 + 2 + 1 = 7 | U.S.A. | Patients hospitalized with AMI in 103 hospitals participating in the Variation in Recovery: Role of Gender on Outcomes of Young AMI Patients (VIRGO) study | Prospective Observational Study | increased cardiac biomarkers levels AND symptoms of ischemia OR ECG changes indicative of new ischemia (new ST-T changes or development of pathological Q waves) | 2985 | 976 | 2009 |
| Nanna, 2019, Circ Cardiovasc Qual Outcomes [16] | 4.378 | 4 + 2 + 1 = 7 | U.S.A. | Patients hospitalized for AMI, enrolled in the ComprehenSIVe Evaluation of Risk Factors in Older Patients with Acute Myocardial Infarction (SILVER-AMI) study. | Prospective Observational Study | criteria for the Third Universal Definition of acute myocardial infraction | 3041 | 1695 | 1346 |
| Patel, 2015, Glob Heart [17] | 3.238 | 4 + 2 + 1 = 7 | India | ACS admissions in 125 hospitals who participated in the Kerala ACS Registry | Prospective Observational Study | admission with chest pain AND at least one of the following criteria (ST-segment elevation in 2 contiguous leads with ou without reciprocal ST-segment depression OR troponin or creatinin kinase-myocardial band elevation OR ST-segment depression OR T-wave inversion in 2 contiguous leads with an history of coronary heart disease) | 25,748 | 19,923 | 5825 |
| Pelter, 2012, Am J Emerg Med [18] | 1.651 | 4 + 1 = 5 | U.S.A., New Zealand, Australia | Secondary analysis of the Patient Response to Myocardial Infarction following a Teaching Intervention Offered by Nurses (PROMOTION) trial | Secondary analysis of a randomized controlled trial | 565 | 367 | 198 | |
| Shah, 2015, BMJ [19] | 27.604 | 4 + 2 = 6 | Scotland | Patients presenting to the Royal Infirmary of Edinburg with suspected ACS | Prospective Cohort Study | suspected an acute coronary syndrome | 1126 | 622 | 504 |
| Shebab, 2020, J Am Heart Ass [20] | 4.66 | 4 + 2 = 6 | Kuwait, Qatar, Bahrain, United Arab Emirates, Oman, Yemen, Saudi Arabia | Patients with a diagnosis of ACS enrolled in one of the 7 Arabian Gulf Registry | Prospective Consecutive Study | standard definition according to published American College of Cardiology/european Society of Cardiology | 15,532 | 13,499 | 2033 |
| Sörensen, 2018, J Am Heart Ass [21] | 4.66 | 4 + 1 = 5 | Germany | Patients presenting to the ED of the University Heart Center Hamburg, enrolled in the Biomarkers in Acute Cardiac Care (BACC) study and in the StenoCardia Study | Prospective Cohort Study | ACS suspected OR acute chest pain | 2520 | 1640 | 880 |
| Van de Meer, 2015, PLOS ONE [22] | 2.776 | 4 + 2 + 1 = 7 | Netherlands | All patient admitted to the cardiac ED with chest pain, enrolled in “the prospective validation of the HEART score” | Prospective Observational Study | chest pain | 2331 | 1328 | 1003 |
| You, 2018, Aging and Disease [23] | 4.232 | 4 = 4 | China | Patients with STEMI admitted in 2 hospitals and undergo to PPCI | Prospective Observational Study | STEMI who underwent PPCI | 337 | 220 | 117 |
| Symptoms | No of Studies | No of Men | No of Women | RR (95%CI) | Heterogeneigty I2 Statistic | p-Value |
|---|---|---|---|---|---|---|
| All patients (N = 1,213,709) | ||||||
| Chest pain | 13 | 707,842 0.8528 [0.7998; 0.8936] | 500,761 0.7831 [0.7177; 0.8368] | 0.91 [0.86; 0.97] | 99% | 0.0023 * |
| Dyspnea | 9 | 31,851 0.3113 [0.2060; 0.4405] | 16,689 0.3595 [0.2442; 0.4937] | 1.13 [1.10; 1.17] | 45% | <0.0001 * |
| Arm pain | 2 | 631 0.2072 [0.1309; 0.3120] | 470 0.2736 [0.1743; 0.4020] | 1.30 [1.05; 1.59] | 0% | 0.0148 * |
| Clammy skin | 6 | 4825 0.2520 [0.1579; 0.3771] | 4611 0.2312 [0.1349; 0.3671] | 0.94 [0.90; 1.01] | 0% | 0.0773 |
| Nausea-vomiting | 7 | 6520 0.2283 [0.1502; 0.3312] | 5957 0.3277 [0.2266; 0.4478] | 1.40 [1.26; 1.56] | 68% | <0.0001 * |
| Fatigue | 4 | 3185 0.2300 [0.0788; 0.5107] | 3876 0.2368 [0.0752; 0.5420] | 1.08 [1.01; 1.16] | 0% | 0.0185 * |
| Palpitations | 5 | 8304 0.0729 [0.0332; 0.1524] | 8473 0.1222 [0.0576; 0.2407] | 1.67 [1.49; 1.86] | 24% | <0.0001 * |
| Shoulder pain | 3 | 2310 0.0947 [0.0333; 0.2410] | 1266 0.1161 [0.0371; 0.3093] | 1.13 [0.76; 1.70] | 68% | 0.5300 |
| Upper abdomen pain | 2 | 1929 0.0575 [0.0282; 0.1137] | 1045 0.0632 [0.0499; 0.0796] | 0.83 [0.62; 1.11] | 70% | 0.2157 |
| Age | 13 | 49,003 | 20,898 | 4.15 [2.28; 6.03] | 99% | <0.0001 * |
| Patients with confirmed ACS (N = 1,195,524) | ||||||
| Chest pain | 10 | 698,827 0.8404 [0.7868; 0.8826] | 493,305 0.7932 [0.7272; 0.8466] | 0.94 [0.88; 1.01] | 99% | 0.886 |
| Dyspnea | 5 | 22,839 0.3104 [0.1809; 0.4785] | 9367 0.3726 [0.2164; 0.5609] | 1.10 [1.05; 1.15] | 0% | <0.0001 * |
| Arm Pain | 2 | 245 0.1959 [0.1509; 0.2504] | 187 0.3513 [0.2189; 0.5113] | 1.44 [1.01; 2.05] | 0% | 0.0465 * |
| Clammy skin | 3 | 1221 0.2966 [0.1185; 0.5695] | 2196 0.2915 [0.1202; 0.5532] | 0.96 [0.90; 1.03] | 0% | 0.2474 |
| Nausea-vomiting | 4 | 2916 0.2856 [0.1517; 0.4719] | 3542 0.3860 [0.2265; 0.5744] | 1.27 [1.20; 1.34] | 0% | <0.0001 * |
| Fatigue | 3 | 2695 0.3331 [0.2539; 0.4229] | 3432 0.3725 [0.2902; 0.4629] | 1.10 [1.02; 1.18] | 0% | 0.0100 * |
| Palpitations | 3 | 1221 0.0807 [0.0328; 0.1854] | 2196 0.1443 [0.0617; 0.3017] | 1.51 [1.25; 1.81] | 0% | <0.0001 * |
| Shoulder pain | 2 | 245 0.1005 [0.0279; 0.3028] | 187 0.2107 [0.0541; 0.5545] | 1.78 [1.02; 3.13] | 0% | 0.0438 * |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cardeillac, M.; Lefebvre, F.; Baicry, F.; Le Borgne, P.; Gil-Jardiné, C.; Cipolat, L.; Peschanski, N.; Abensur Vuillaume, L. Symptoms of Infarction in Women: Is There a Real Difference Compared to Men? A Systematic Review of the Literature with Meta-Analysis. J. Clin. Med. 2022, 11, 1319. https://doi.org/10.3390/jcm11051319
Cardeillac M, Lefebvre F, Baicry F, Le Borgne P, Gil-Jardiné C, Cipolat L, Peschanski N, Abensur Vuillaume L. Symptoms of Infarction in Women: Is There a Real Difference Compared to Men? A Systematic Review of the Literature with Meta-Analysis. Journal of Clinical Medicine. 2022; 11(5):1319. https://doi.org/10.3390/jcm11051319
Chicago/Turabian StyleCardeillac, Martin, François Lefebvre, Florent Baicry, Pierrick Le Borgne, Cédric Gil-Jardiné, Lauriane Cipolat, Nicolas Peschanski, and Laure Abensur Vuillaume. 2022. "Symptoms of Infarction in Women: Is There a Real Difference Compared to Men? A Systematic Review of the Literature with Meta-Analysis" Journal of Clinical Medicine 11, no. 5: 1319. https://doi.org/10.3390/jcm11051319
APA StyleCardeillac, M., Lefebvre, F., Baicry, F., Le Borgne, P., Gil-Jardiné, C., Cipolat, L., Peschanski, N., & Abensur Vuillaume, L. (2022). Symptoms of Infarction in Women: Is There a Real Difference Compared to Men? A Systematic Review of the Literature with Meta-Analysis. Journal of Clinical Medicine, 11(5), 1319. https://doi.org/10.3390/jcm11051319