
Elevated Plasma Soluble C-Type Lectin-like Receptor 2 Is Associated with the Worsening of Coronavirus Disease 2019

 ,
, 
 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
- (a)
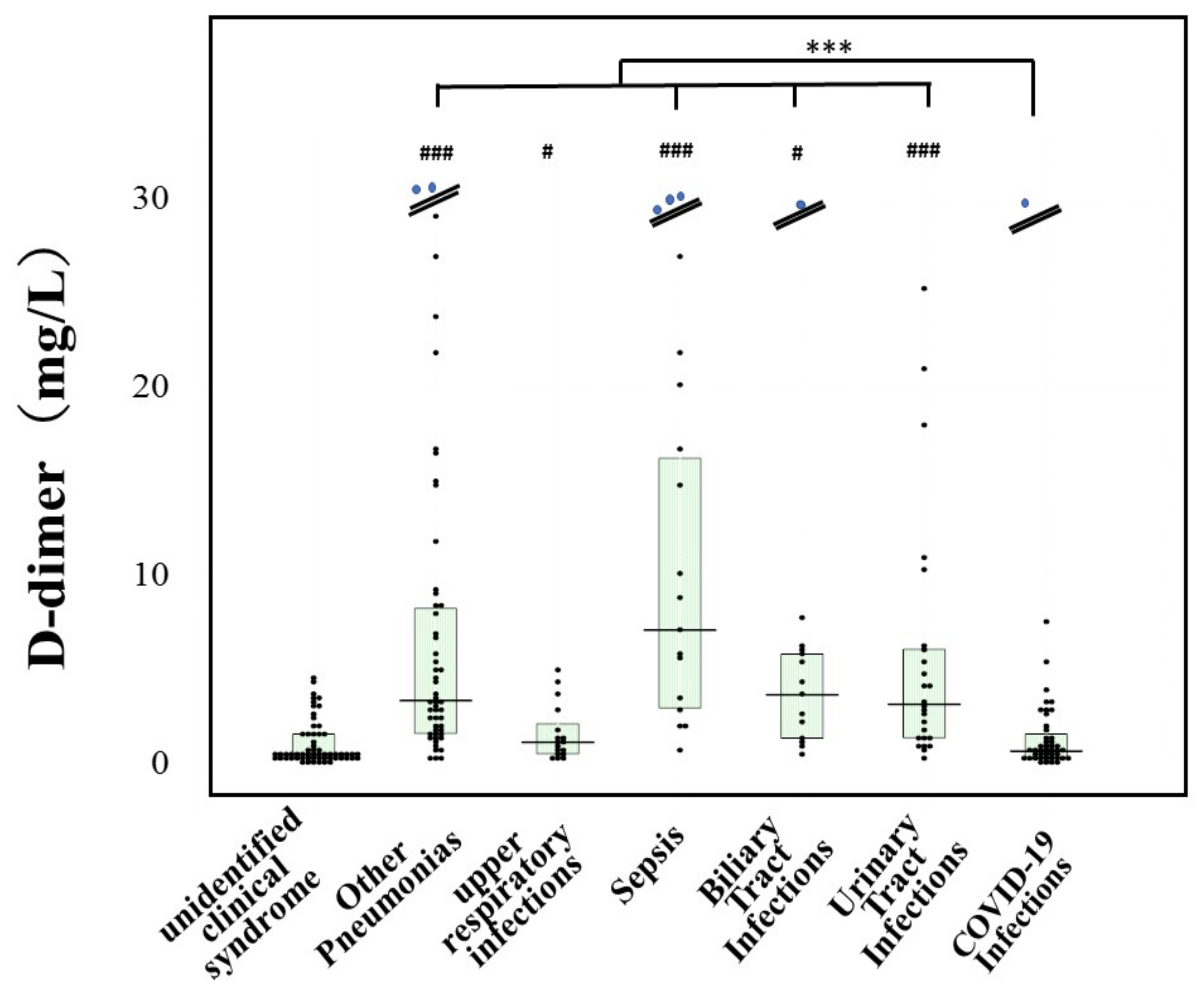
- Sex, age, mortality, frequency of association with DIC, laboratory data (e.g., platelet count, PT-INR, and D-dimer levels in patients with COVID-19 infection were compared with those in patients suffering from other infections.
- (b)
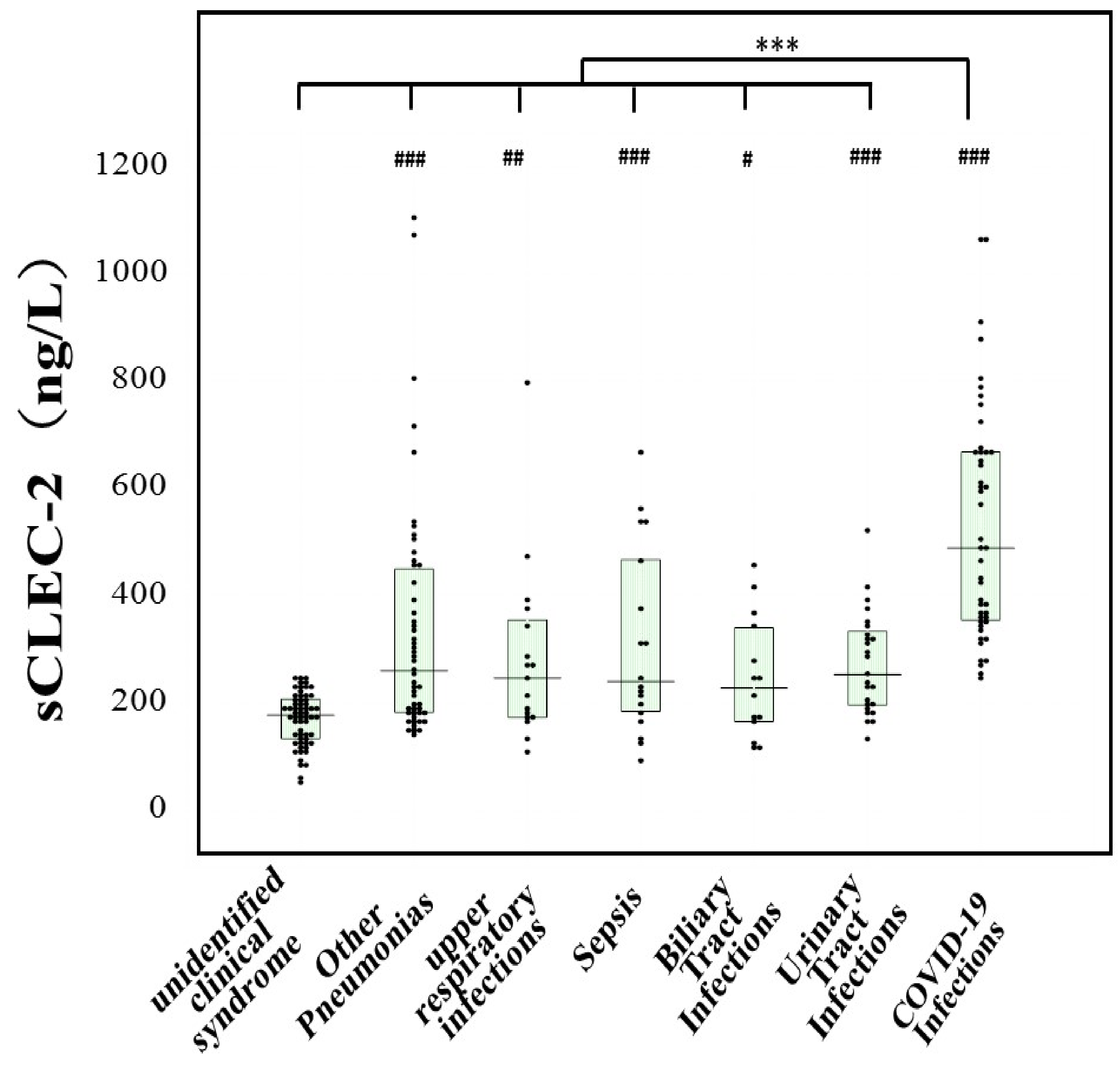
- Comparison of plasma sCLEC-2 levels between patients with COVID-19 infection and patients suffering with other infections.
- (c)
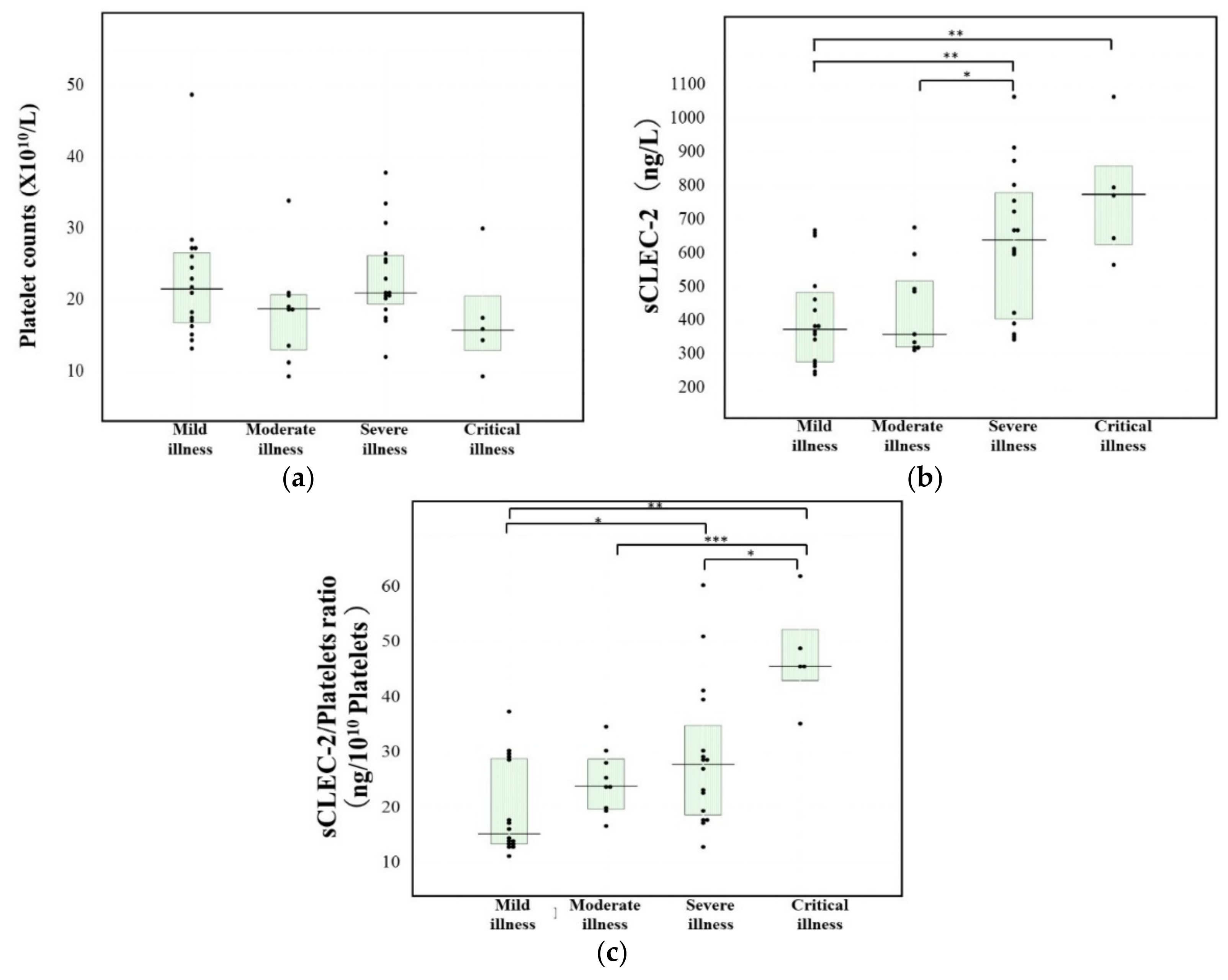
- Sex, age, mortality and laboratory data were examined among the four clinical stages of COVID-19 infection.
- (d)
- The plasma sCLEC-2 levels and sCLEC-2/platelets ratio were examined among the four clinical stages of COVID-19 infection.
2.2. Statistical Analyses
3. Results
4. Discussion
5. Limitations and Further Study
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: A retrospective cohort study. Lancet 2020, 395, 1054–1062. [Google Scholar] [CrossRef]
- Jiang, F.; Deng, L.; Zhang, L.; Cai, Y.; Cheung, C.W.; Xia, Z. Review of the Clinical Characteristics of Coronavirus Disease 2019 (COVID-19). J. Gen. Intern. Med. 2020, 35, 1545–1549. [Google Scholar] [CrossRef] [Green Version]
- Gavriatopoulou, M.; Ntanasis-Stathopoulos, I.; Korompoki, E.; Fotiou, D.; Migkou, M.; Tzanninis, I.-G.; Psaltopoulou, T.; Kastritis, E.; Terpos, E.; Dimopoulos, M.A. Emerging treatment strategies for COVID-19 infection. Clin. Exp. Med. 2021, 21, 167–179. [Google Scholar] [CrossRef] [PubMed]
- Machhi, J.; Herskovitz, J.; Senan, A.M.; Dutta, D.; Nath, B.; Oleynikov, M.D.; Blomberg, W.R.; Meigs, D.D.; Hasan, M.; Patel, M.; et al. The Natural History, Pathobiology, and Clinical Manifestations of SARS-CoV-2 Infections. J. Neuroimmune Pharmacol. 2020, 21, 1–28. [Google Scholar] [CrossRef] [PubMed]
- Hertanto, D.M.; Wiratama, B.S.; Sutanto, H.; Wungu, C.D.K. Immunomodulation as a Potent COVID-19 Pharmacotherapy: Past, Present and Future. J. Inflamm. Res. 2021, 14, 3419–3428. [Google Scholar] [CrossRef] [PubMed]
- Berlin, D.A.; Gulick, R.M.; Martinez, F.J. Severe Covid-19. N. Engl. J. Med. 2020, 383, 2451–2460. [Google Scholar] [CrossRef] [PubMed]
- Gandhi, R.T.; Lynch, J.B.; Del Rio, C. Mild or Moderate Covid-19. N. Engl. J. Med. 2020, 383, 1757–1766. [Google Scholar] [CrossRef] [PubMed]
- Chan, N.C.; Weitz, J.I. COVID-19 coagulopathy, thrombosis, and bleeding. Blood 2020, 136, 381–383. [Google Scholar] [CrossRef] [PubMed]
- Available online: https://www.mhlw.go.jp/content/000785119.pdf (accessed on 25 July 2021).
- Yamamoto, A.; Wada, H.; Ichikawa, Y.; Mizuno, H.; Tomida, M.; Masuda, J.; Makino, K.; Kodama, S.; Yoshida, M.; Fukui, S.; et al. Evaluation of Biomarkers of Severity in Patients with COVID-19 Infection. J. Clin. Med. 2021, 10, 3775. [Google Scholar] [CrossRef] [PubMed]
- Terpos, E.; Ntanasis-Stathopoulos, I.; Elalamy, I.; Kastritis, E.; Sergentanis, T.N.; Politou, M.; Psaltopoulou, T.; Gerotziafas, G.; Dimopoulos, M.A. Hematological findings and complications of COVID-19. Am. J. Hematol. 2020, 95, 834–847. [Google Scholar] [CrossRef] [Green Version]
- Gabrielli, M.; Lamendola, P.; Esperide, A.; Valletta, F.; Franceschi, F. COVID-19 and thrombotic complications: Pulmonary thrombosis rather than embolism? Thromb. Res. 2020, 193, 98. [Google Scholar] [CrossRef]
- Manne, B.K.; Denorme, F.; Middleton, E.A.; Portier, I.; Rowley, J.W.; Stubben, C.J. Platelet gene expression and function in COVID-19 patients. Blood 2020, 136, 1317–1329. [Google Scholar] [CrossRef]
- Canzano, P.; Brambilla, M.; Porro, B.; Cosentino, N.; Tortorici, E.; Vicini, S.; Poggio, P.; Cascella, A.; Pengo, M.F.; Veglia, F.; et al. Platelet and Endothelial Activation as Potential Mechanisms Behind the Thrombotic Complications of COVID-19 Patients. JACC Basic Transl. Sci. 2021, 6, 202–218. [Google Scholar] [CrossRef]
- Suzuki-Inoue, K.; Fuller, G.L.; Garcia, A.; Eble, J.A.; Pohlmann, S.; Inoue, O.; Gartner, T.K.; Hughan, S.C.; Pearce, A.C.; Laing, G.D.; et al. A novel Syk-dependent mechanism of platelet activation by the C-type lectin receptor sCLEC-2. Blood 2006, 107, 542–549. [Google Scholar] [CrossRef] [Green Version]
- Yamashita, Y.; Suzuki, K.; Mastumoto, T.; Ikejiri, M.; Ohishi, K.; Katayama, N.; Suzuki-Inoue, K.; Wada, H. Elevated plasma levels of soluble C-type lectinlike receptor 2 (sCLEC-2) in patients with thrombotic microangiopathy. Thromb. Res. 2019, 178, 54–58. [Google Scholar] [CrossRef]
- Yamamoto, A.; Wada, H.; Ichkawa, Y.; Tanaka, M.; Tashiro, H.; Shiraki, K.; Shimpo, H.; Yamashita, Y.; Mastumoto, T.; Shimaoka, M.; et al. Soluble C-Type Lectin-Like Receptor 2 Is a Biomarker for Disseminated Intravascular Coagulation. J. Clin. Med. 2021, 10, 2860. [Google Scholar] [CrossRef]
- Inoue, O.; Osada, M.; Nakamura, J.; Kazama, F.; Shirai, T.; Tsukiji, N.; Sasaki, T.; Yokomichi, H.; Dohi, T.; Kaneko, M.; et al. Soluble CLEC-2 is generated independently of ADAM10 and is increased in plasma in acute coronary syndrome: Comparison with soluble GPVI. Int. J. Hematol. 2019, 110, 285–294. [Google Scholar] [CrossRef]
- Nishigaki, A.; Ichikawa, Y.; Ezaki, M.; Yamamoto, A.; Suzuki, K.; Tachibana, K.; Kamon, T.; Horie, S.; Masuda, J.; Makino, K.; et al. Soluble C-Type Lectin-Like Receptor 2 Elevation in Patients with Acute Cerebral Infarction. J. Clin. Med. 2021, 10, 3408. [Google Scholar] [CrossRef]
- Clinical Spectrum of SARS-CoV-2 Infection. Available online: https://www.covid19treatmentguidelines.nih.gov/overview/clinical-spectrum/ (accessed on 14 December 2021).
- Kobayashi, N.; Maekawa, T.; Takada, M.; Tanaka, H.; Gonmori, H. Criteria for Diagnosis of DIC Based on the Analysis of Clinical and Laboratory Findings in 345 DIC Patients Collected by the Research Committee on DIC in Japan. Curr. Stud. Hematol. Blood Transfus. 1983, 49, 265–275. [Google Scholar] [CrossRef]
- Ikeda, N.; Wada, H.; Ichikawa, Y.; Ezaki, M.; Tanaka, M.; Hiromori, S.; Shiraki, K.; Moritani, I.; Yamamoto, A.; Shimpo, H.; et al. D-dimer kit with a High FDP/D-Dimer Ratio is Useful for Diagnosing Thrombotic Diseases. Clin. Appl. Thromb. Hemost. 2022, 28. [Google Scholar] [CrossRef]
- Al-Samkari, H.; Karp Leaf, R.S.; Dzik, W.H. COVID-19 and coagulation: Bleeding and thrombotic manifestations of SARS-CoV-2 infection. Blood 2020, 136, 489–500. [Google Scholar] [CrossRef]
- Page, E.M.; Ariëns, R.A.S. Mechanisms of thrombosis and cardiovascular complications in COVID-19. Thromb. Res. 2021, 200, 1–8. [Google Scholar] [CrossRef]
- Connors, J.M.; Levy, J.H. COVID-19 and its implications for thrombosis and anticoagulation. Blood 2020, 135, 2033–2040. [Google Scholar] [CrossRef]
- Zuo, Y.; Yalavarthi, S.; Shi, H.; Gockman, K.; Zuo, M.; Madison, J.A.; Blair, C.; Weber, A.; Barnes, B.J.; Egeblad, M.; et al. Neutrophil extracellular traps (NETs) in COVID-19. JCI Insight 2020, 5, e138999. [Google Scholar]
- Matsunaga, N.; Hayakawa, K.; Terada, M.; Ohtsu, H.; Asai, Y.; Tsuzuki, S.; Suzuki, S.; Toyoda ASuzuki, K.; Endo, M.; Fujii, N.; et al. Clinical epidemiology of hospitalized patients with COVID-19 in Japan: Report of the COVID-19 Registry Japan. Clin Infect Dis. 2021, 73, e3677-89. [Google Scholar] [CrossRef]
- Yang, X.; Yang, Q.; Wang, Y.; Wu, Y.; Xu, J.; Yu, Y.; Shang, Y. Thrombocytopenia and its association with mortality in patients with COVID-19. J. Thromb. Haemost. 2020, 18, 1469–1472. [Google Scholar] [CrossRef]
- Wada, H.; Matsumoto, T.; Suzuki, K.; Imai, H.; Katayama, N.; Iba, T.; Matsumoto, M. Differences and similarities between disseminated intravascular coagulation and thrombotic microangiopathy. Thromb. J. 2018, 16, 14. [Google Scholar] [CrossRef]
- Passariello, M.; Vetrei, C.; Amato, F.; De Lorenzo, C. Interactions of Spike-RBD of SARS-CoV-2 and Platelet Factor 4: New Insights in the Etiopathogenesis of Thrombosis. Int. J. Mol. Sci. 2021, 22, 8562. [Google Scholar] [CrossRef]
- Nazy, I.; Jevtic, S.D.; Moore, J.C.; Huynh, A.; Smith, J.W.; Kelton, J.G.; Arnold, D.M. Platelet-activating immune complexes identified in critically ill COVID-19 patients suspected of heparin-induced thrombocytopenia. J. Thromb. Haemost. 2021, 19, 1342–1347. [Google Scholar] [CrossRef]
- Ishikura, H.; Irie, Y.; Kawamura, M.; Hoshino, K.; Nakamura, Y.; Mizunuma, M.; Maruyama, J.; Nakashio, M.; Suzuki-Inoue, K.; Kitamura, T. Early recognition of sepsis-induced coagulopathy using the CPAC2 index: A ratio of soluble type C lectin-like receptor 2 (sCLEC-2) level and platelet count. Platelets 2022, 24, 1–10. [Google Scholar] [CrossRef]
- Salah, H.M.; Mehta, J.L. Meta-Analysis of the Effect of Aspirin on Mortality in COVID-19. Am. J. Cardiol. 2021, 142, 158–159. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Underlying Diseases | N | F (%):M | Age (Years) | Death (%) | DIC | Platelets (×1010/L) | PT-INR | D-Dimer (mg/L) |
|---|---|---|---|---|---|---|---|---|
| Unidentified Clinical Syndrome | 60 | 31 (51.7%):29 | 56.5 # (48.0–75.0) | 0 | 0 (0) | 23.1 (17.9–27.0) | 0.96 ### (0.91–1.00) | 0.5 (0.4–1.6) |
| Other Pneumoniae | 53 | 23 (43.4%):30 | 81.0 ***### (71.0–85.0) | 9 (17.0) | 6 (11.3) | 25.4 (17.7–27.7) | 1.12 ***## (1.05–1.20) | 3.4 ***### (1.8–8.7) |
| Upper Respiratory Infections | 17 | 10 (58.8%):7 | 71.0 *# (50.3–77.3) | 0 (0) | 0 (0) | 25.4 (17.7–27.7) | 1.03 ** (0.96–1.09) | 1.2 * (0.6–2.2) |
| Sepsis | 18 | 7 (38.9%):11 | 67.0 ***# (49.0–83.0) | 3 (16.7) | 7 (38.9) | 13.7 **# (8.3–21.3) | 1.20 ***### (1.11–1.42) | 9.5 ***### (3.6–21.9) |
| Biliary Tract Infections | 14 | 8 (57.1%):6 | 84.5 ***### (76.0–92.0) | 0 (0) | 1 (14.3) | 16.6 * (8.5–26.6) | 1.05 *** (0.96–1.15) | 4.1 ***### (1.5–6.1) |
| Urinary Tract Infections | 25 | 18 (72.0%):7 | 79.0 ***### (67.8–86.0) | 0 (0) | 0 (4.0) | 20.7 (17.2–25.8) * | 1.08 *** (1.01–1.13) | 3.2 ***### (1.4–6.1) |
| COVID-19 Infections | 46 | 21 (45.7%):25 | 51.0 (28.0–67.0) | 2 (4.3) | 0 (0) | 20.7 (17.2–25.8) | 1.04 *** (1.01–1.08) | 0.8 (0.4–1.8) |
| N | F:M | Age (Years) | Death (%) | Platelets (×1010/L) | PT-INR | D-Dimer (mg/L) | |
|---|---|---|---|---|---|---|---|
| Mild Illness | 16 | 8:8 | 31.0 (24.5–64.5) | 1 (6.3) | 21.6 (16.9–26.7) | 1.0 (1.0-1.1) | 0.5 (0.3–0.7) |
| Moderate Illness | 9 | 7:2 | 55.0 (26.5–70.0) | 0 (0) | 18.8 (13.1–20.8) | 1.0 (1.0-1.1) | 0.9 (0.4–2.9) |
| Severe Illness | 16 | 5:11 | 52.0 (34.0–58.0) | 1 (6.3) | 21.0 (19.5–16.3) | 1.1 (1.0-1.1) | 1.0 (0.7–1.7) ** |
| Critical Illness | 5 | 1:4 | 60.0 (54.8–71.3) | 0 (0) | 15.8 (13.0–20.6) | 1.2 (1.1-1.2) | 3.4 (1.0–15.0) ** |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Wada, H.; Ichikawa, Y.; Ezaki, M.; Yamamoto, A.; Tomida, M.; Yoshida, M.; Fukui, S.; Moritani, I.; Shiraki, K.; Shimaoka, M.; et al. Elevated Plasma Soluble C-Type Lectin-like Receptor 2 Is Associated with the Worsening of Coronavirus Disease 2019. J. Clin. Med. 2022, 11, 985. https://doi.org/10.3390/jcm11040985
Wada H, Ichikawa Y, Ezaki M, Yamamoto A, Tomida M, Yoshida M, Fukui S, Moritani I, Shiraki K, Shimaoka M, et al. Elevated Plasma Soluble C-Type Lectin-like Receptor 2 Is Associated with the Worsening of Coronavirus Disease 2019. Journal of Clinical Medicine. 2022; 11(4):985. https://doi.org/10.3390/jcm11040985
Chicago/Turabian StyleWada, Hideo, Yuhuko Ichikawa, Minoru Ezaki, Akitaka Yamamoto, Masaki Tomida, Masamichi Yoshida, Shunsuke Fukui, Isao Moritani, Katsuya Shiraki, Motomu Shimaoka, and et al. 2022. "Elevated Plasma Soluble C-Type Lectin-like Receptor 2 Is Associated with the Worsening of Coronavirus Disease 2019" Journal of Clinical Medicine 11, no. 4: 985. https://doi.org/10.3390/jcm11040985
APA StyleWada, H., Ichikawa, Y., Ezaki, M., Yamamoto, A., Tomida, M., Yoshida, M., Fukui, S., Moritani, I., Shiraki, K., Shimaoka, M., Iba, T., Suzuki-Inoue, K., & Shimpo, H. (2022). Elevated Plasma Soluble C-Type Lectin-like Receptor 2 Is Associated with the Worsening of Coronavirus Disease 2019. Journal of Clinical Medicine, 11(4), 985. https://doi.org/10.3390/jcm11040985