
A Prospective Randomized Study Comparing Functional Outcome in Distal Fibula Fractures between Conventional AO Semitubular Plating and Minimal Invasive Intramedullary “Photodynamic Bone Stabilisation”
 , , ,
, , ,  ,
, 
Abstract
1. Introduction
2. Materials and Methods
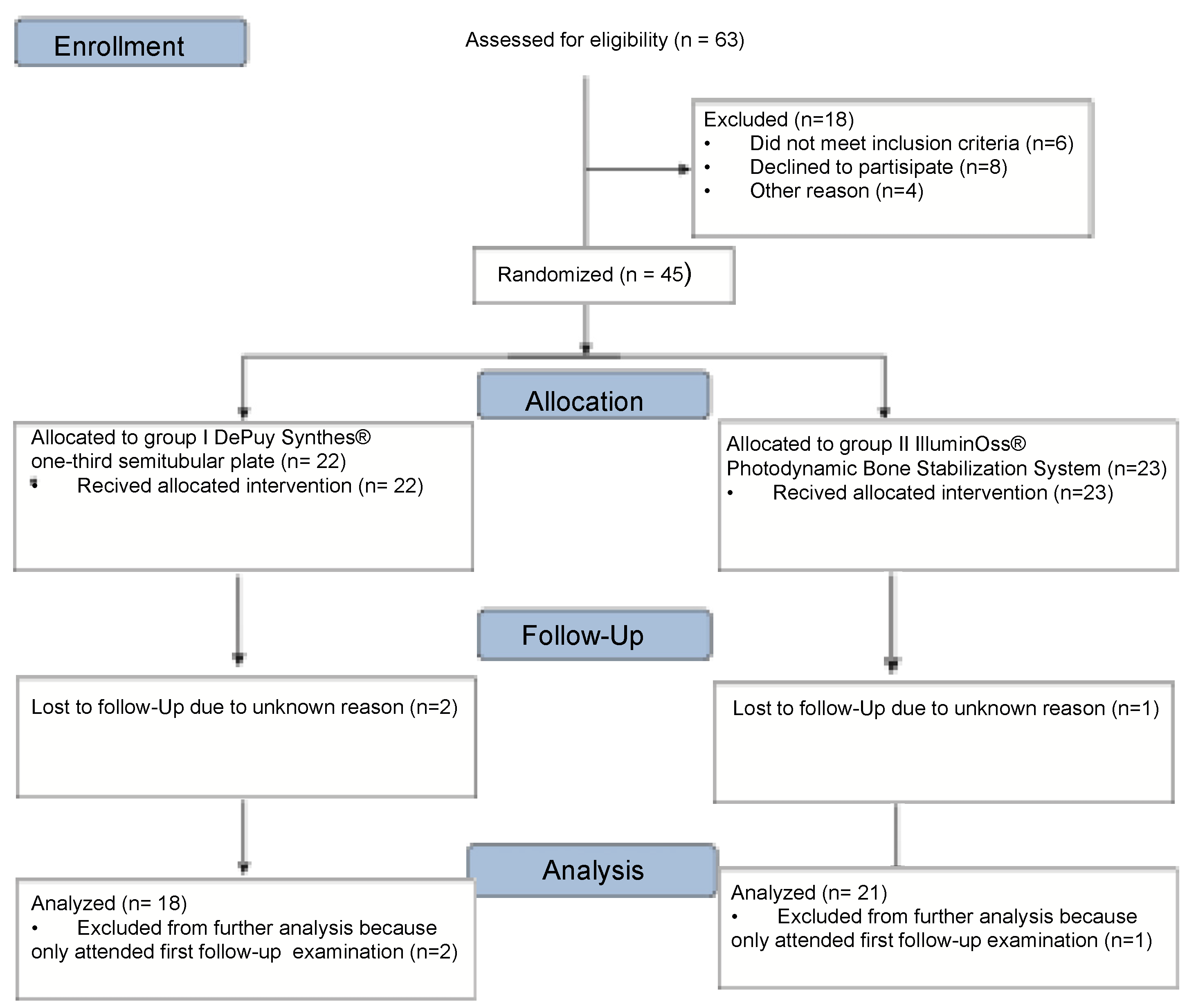
2.1. Patients
2.2. Surgical Technique and Postoperative Therapy
2.3. Follow-Up Evaluation
2.4. Statistics and Sample Size Calculation
3. Results
3.1. Epidemiological Data
3.2. Clinical Outcome
3.3. Radiological Follow Up
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
Abbreviations
References
- Court-Brown, C.M.; Caesar, B. Epidemiology of adult fractures: A review. Injury 2006, 37, 691–697. [Google Scholar] [CrossRef]
- Grutter, R.; Cordey, J.; Wahl, D.; Koller, B.; Regazzoni, P. A biomechanical enigma: Why are tibial fractures not more frequent in the elderly? Injury 2000, 31 (Suppl. S3), C72–C77. [Google Scholar] [CrossRef]
- Crevoisier, X.; Baalbaki, R.; Dos Santos, T.; Assal, M. Ankle fractures in the elderly patient. Rev. Med. Suisse 2014, 10, 2420–2423. [Google Scholar]
- Koval, K.J.; Lurie, J.; Zhou, W.; Sparks, M.B.; Cantu, R.V.; Sporer, S.M.; Weinstein, J. Ankle fractures in the elderly: What you get depends on where you live and who you see. J. Orthop. Trauma 2005, 19, 635–639. [Google Scholar] [CrossRef]
- Kannus, P.; Palvanen, M.; Niemi, S.; Parkkari, J.; Jrvinen, M. Increasing number and incidence of low-trauma ankle fractures in elderly people: Finnish statistics during 1970–2000 and projections for the future. Bone 2002, 31, 430–433. [Google Scholar] [CrossRef]
- Karlamangla, A.; Tinetti, M.; Guralnik, J.; Studenski, S.; Wetle, T.; Reuben, D. Comorbidity in older adults: Nosology of impairment, diseases, and conditions. J. Gerontol. Ser. A 2007, 62, 296–300. [Google Scholar] [CrossRef]
- Leyes, M.; Torres, R.; Guillén, P. Complications of open reduction and internal fixation of ankle fractures. Foot Ankle Clin. 2003, 8, 131–147. [Google Scholar] [CrossRef]
- Tsukada, S.; Otsuji, M.; Shiozaki, A.; Yamamoto, A.; Komatsu, S.; Yoshimura, H.; Ikeda, H.; Hoshino, A. Locking versus non-locking neutralization plates for treatment of lateral malleolar fractures: A randomized controlled trial. Int. Orthop. 2013, 37, 2451–2456. [Google Scholar] [CrossRef]
- Yeo, E.D.; Kim, H.J.; Cho, W.I.; Lee, Y.K. A Specialized Fibular Locking Plate for Lateral Malleolar Fractures. J. Foot Ankle Surg. 2015, 54, 1067–1071. [Google Scholar] [CrossRef]
- Jain, S.; Haughton, B.A.; Brew, C. Intramedullary fixation of distal fibular fractures: A systematic review of clinical and functional outcomes. J. Orthop. Traumatol. 2014, 15, 245–254. [Google Scholar] [CrossRef]
- Dabash, S.; Eisenstein, E.D.; Potter, E.; Kusnezov, N.; Thabet, A.M.; Abdelgawad, A.A. Unstable Ankle Fracture Fixation Using Locked Fibular Intramedullary Nail in High-Risk Patients. J. Foot Ankle Surg. 2019, 58, 357–362. [Google Scholar] [CrossRef]
- Swart, E.; Bezhani, H.; Greisberg, J.; Vosseller, J.T. How long should patients be kept non-weight bearing after ankle fracture fixation? A survey of OTA and AOFAS members. Injury 2015, 46, 1127–1130. [Google Scholar] [CrossRef]
- Kristensen, K.D. Ankle Fractures: Supination-Eversion Fractures of Stage IV: Primary and Late Results of Operative and Non—Operative Treatment AU—Yde, Johannes. Acta Orthop. Scand. 1980, 51, 981–990. [Google Scholar]
- Makwana, N.K.; Bhowal, B.; Harper, W.M.; Hui, A.W. Conservative versus operative treatment for displaced ankle fractures in patients over 55 years of age. J. Bone Jt. Surgery. Br. 2001, 83, 525–529. [Google Scholar] [CrossRef]
- Eckel, T.T.; Glisson, R.R.; Anand, P.; Parekh, S.G. Biomechanical Comparison of 4 Different Lateral Plate Constructs for Distal Fibula Fractures. Foot Ankle Int. 2013, 34, 1588–1595. [Google Scholar] [CrossRef]
- Kim, T.; Ayturk, U.M.; Haskell, A.; Miclau, T.; Puttlitz, C.M. Fixation of Osteoporotic Distal Fibula Fractures: A Biomechanical Comparison of Locking Versus Conventional Plates. J. Foot Ankle Surg. 2007, 46, 2–6. [Google Scholar] [CrossRef]
- Klos, K.; Sauer, S.; Hoffmeier, K.; Gras, F.; Fröber, R.; Hofmann, G.O.; Mückley, T. Biomechanical Evaluation of Plate Osteosynthesis of Distal Fibula Fractures with Biodegradable Devices. Foot Ankle Int. 2009, 30, 243–251. [Google Scholar] [CrossRef]
- McKenna, P.B.; O’Shea, K.; Burke, T. Less is more: Lag screw only fixation of lateral malleolar fractures. Int. Orthop. 2006, 31, 497–502. [Google Scholar] [CrossRef]
- Sain, A.; Garg, S.; Sharma, V.; Meena, U.K.; Bansal, H. Osteoporotic Distal Fibula Fractures in the Elderly: How to Fix Them. Cureus 2020, 12, e6552. [Google Scholar] [CrossRef]
- Zyskowski, M.; Wurm, M.; Greve, F.; Pesch, S.; von Matthey, F.; Pflüger, P.; Crönlein, M.; Biberthaler, P.; Kirchhoff, C. Is early full weight bearing safe following locking plate ORIF of distal fibula fractures? BMC Musculoskelet. Disord. 2021, 22, 159. [Google Scholar] [CrossRef]
- Rehman, H.; McMillan, T.; Rehman, S.; Clement, A.; Finlayson, D. Intrmedullary versus extramedullary fixation of lateral malleolus fractures. Int. J. Surg. 2015, 22, 54–61. [Google Scholar] [CrossRef]
- White, T.O.; Bugler, K.E.; Appleton, P.; Will, E.; McQueen, M.M.; Court-Brown, C.M. A prospective randomised controlled trial of the fibular nail versus standard open reduction and internal fixation for fixation of ankle fractures in elderly patients. Bone Jt. J. 2016, 98, 1248–1252. [Google Scholar] [CrossRef]
- Fleming, J.J. Intramedullary Nailing of Fibular Fractures. Clin. Podiatr. Med. Surg. 2018, 35, 259–270. [Google Scholar] [CrossRef]
- Ebraheim, N.A.; Maten, J.W.V.; Delaney, J.R.; White, E.; Hanna, M.; Liu, J. Cannulated Intramedullary Screw Fixation of Distal Fibular Fractures. Foot Ankle Spéc. 2018, 12, 264–271. [Google Scholar] [CrossRef]
- Challagundla, S.R.; Shewale, S.; Cree, C.; Hawkins, A. Intramedullary fixation of lateral malleolus using Fibula Rod System in ankle fractures in the elderly. Foot Ankle Surg. 2018, 24, 423–426. [Google Scholar] [CrossRef]
- Tas, D.B.; Smeeing, D.P.; Emmink, B.L.; Govaert, G.A.; Hietbrink, F.; Leenen, L.P.; Houwert, R.M. Intramedullary Fixation Versus Plate Fixation of Distal Fibular Fractures: A Systematic Review and Meta-Analysis of Randomized Controlled Trials and Observational Studies. J. Foot Ankle Surg. 2019, 58, 119–126. [Google Scholar] [CrossRef]
- Coifman, O.; Bariteau, J.T.; Shazar, N.; Tenenbaum, S.A. Lateral malleolus closed reduction and internal fixation with intramedullary fibular rod using minimal invasive approach for the treatment of ankle fractures. Foot Ankle Surg. 2019, 25, 79–83. [Google Scholar] [CrossRef]
- Amaha, K.; Arimoto, T.; Saito, M.; Tasaki, A.; Tsuji, S. Shorter recovery can be achieved from using walking boot after operative treatment of an ankle fracture. Asia-Pac. J. Sport. Med. Arthrosc. Rehabil. Technol. 2016, 7, 10–14. [Google Scholar] [CrossRef]
- Di Stasio, A.J., 2nd; Jaggears, F.R.; DePasquale, L.V.; Frassica, F.J.; Turen, C.H. Protected early motion versus cast immobilization in postoperative management of ankle fractures. Contemp. Orthop. 1994, 29, 273–277. [Google Scholar]
- Bonness, E.K.; Siebler, J.C.; Reed, L.K.; Lyden, E.R.; Mormino, M.A. Immediate Weight-Bearing Protocol for the Determination of Ankle Stability in Patients with Isolated Distal Fibular Fractures. J. Orthop. Trauma 2018, 32, 534–537. [Google Scholar] [CrossRef]
- Curtis, E.M.; van der Velde, R.; Moon, R.J.; van den Bergh, J.P.; Geusens, P.; de Vries, F.; van Staa, T.P.; Cooper, C.; Harvey, N.C.W. Epidemiology of fractures in the United Kingdom 1988-2012: Variation with age, sex, geography, ethnicity and socioeconomic status. Bone 2016, 87, 19–26. [Google Scholar] [CrossRef]
- Van Laarhoven, C.J.; Meeuwis, J.D.; der Werken, C.V. Postoperative treatment of internally fixed ankle fractures: A prospective randomised study. J. Bone Jt. Surg. Br. Vol. 1996, 78, 395–399. [Google Scholar] [CrossRef]
- Kortekangas, T.; Haapasalo, H.; Flinkkilä, T.; Ohtonen, P.; Nortunen, S.; Laine, H.-J.; Järvinen, T.; Pakarinen, H. Three week versus six week immobilisation for stable Weber B type ankle fractures: Randomised, multicentre, non-inferiority clinical trial. BMJ 2019, 364, k5432. [Google Scholar] [CrossRef] [PubMed]
- Appleton, P.; McQueen, M.; Court-Brown, C. The Fibula Nail for Treatment of Ankle Fractures in Elderly and High Risk Patients. Tech. Foot Ankle Surg. 2006, 5, 204–208. [Google Scholar] [CrossRef]
- Smeeing, D.P.J.; Houwert, R.M.; Briet, J.P.; Groenwold, R.H.H.; Lansink, K.W.W.; Leenen, L.P.H.; van der Zwaal, P.; Hoogendoorn, J.M.; van Heijl, M.; Verleisdonk, E.J.; et al. Weight-bearing or non-weight-bearing after surgical treatment of ankle fractures: A multicenter randomized controlled trial. Eur. J. Trauma Emerg. Surg. 2018, 46, 121–130. [Google Scholar] [CrossRef]
- Gauthé, R.; Desseaux, A.; Rony, L.; Tarissi, N.; Dujardin, F. Ankle fractures in the elderly: Treatment and results in 477 patients. Orthop. Traumatol. Surg. Res. 2016, 102, S241–S244. [Google Scholar] [CrossRef]
- Wukich, D.K.; Joseph, A.; Ryan, M.; Ramirez, C.; Irrgang, J.J. Outcomes of Ankle Fractures in Patients with Uncomplicated versus Complicated Diabetes. Foot Ankle Int. 2011, 32, 120–130. [Google Scholar] [CrossRef]
- Ahl, T.; Dalen, N.; Selvik, G. Mobilization after operation of ankle fractures Good results of early motion and weight bearing. Acta Orthop. Scand. 1988, 59, 302–306. [Google Scholar] [CrossRef]
- Simanski, C.J.; Maegele, M.G.; Lefering, R.; Lehnen, D.M.; Kawel, N.; Riess, P.; Nedim, Y.; Thomas, T.; Bertil, B. Functional treatment and early weightbearing after an ankle fracture: A prospective study. J. Orthop. Trauma 2006, 20, 108–114. [Google Scholar] [CrossRef]
- Zyskowski, M.; Crönlein, M.; Heidt, E.; Biberthaler, P.; Kirchhoff, C. Osteosynthesis of distal fibular fractures with IlluminOss: Video article. Unfallchirurg 2017, 120, 6–11. [Google Scholar] [CrossRef][Green Version]
- Weber, B.G.; Colton, C. Malleolar Fractures. In Manual of Internal Fixation: Techniques Recommended by the AO-ASIF Group; Springer: Berlin/Heidelberg, Germany, 1991; pp. 595–612. [Google Scholar]
- Benirschke, S.K.; Melder, I.; Henley, M.B.; Routt, M.L.; Smith, D.G.; Chapman, J.R.; Swiontkowski, M.F. Closed interlocking nailing of femoral shaft fractures: Assessment of technical complications and functional outcomes by comparison of a prospective database with retrospective review. J. Orthop. Trauma 1993, 7, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Hooper, G.J.; Keddell, R.G.; Penny, I.D. Conservative management or closed nailing for tibial shaft fractures. A randomised prospective trial. J. Bone Jt. Surg. 1991, 73, 83–85. [Google Scholar] [CrossRef] [PubMed]
- Yuan, H.; Wang, R.; Zheng, J.; Yang, Y. Intramedullary Nailing and Minimally Invasive Percutaneous Plate Osteosynthesis in Treatment of Displaced Clavicular Mid-shaft Fractures: A Prospective Study. Z. Orthopädie Und Unf. 2019, 158, 604–610. [Google Scholar] [CrossRef] [PubMed]
- Peeperkorn, S.; Nijs, S.; Hoekstra, H. Why Fibular Nailing Can Be an Efficient Treatment Strategy for AO Type 44-B Ankle Fractures in the Elderly. J. Foot Ankle Surg. 2018, 57, 961–966. [Google Scholar] [CrossRef] [PubMed]
- Switaj, P.J.; Fuchs, D.; Alshouli, M.; Patwardhan, A.G.; Voronov, L.I.; Muriuki, M.; Havey, R.M.; Kadakia, A.R. A biomechanical comparison study of a modern fibular nail and distal fibular locking plate in AO/OTA 44C2 ankle fractures. J. Orthop. Surg. Res. 2016, 11, 100. [Google Scholar] [CrossRef]
- Charlson, M.E.; Pompei, P.; Ales, K.L.; MacKenzie, C.R. A new method of classifying prognostic comorbidity in longitudinal studies: Development and validation. J. Chronic Dis. 1987, 40, 373–383. [Google Scholar] [CrossRef]
- Malleolar Segment. J. Orthop. Trauma 2018, 32, 67.
- Bhimani, R.; Lubberts, B.; Hagemeijer, N.; Zhao, J.Z.; Saengsin, J.; Sato, G.; Waryasz, G.R.; DiGiovanni, C.W.; Guss, D. The Lateral Hook Test: What is the Amount of Force that Should Be Applied to Evaluate Syndesmotic Instability Using Arthroscopy? Foot Ankle Orthop. 2022, 7, 2473011421S00117. [Google Scholar] [CrossRef]
- Sman, A.D.; Hiller, C.E.; Rae, K.; Linklater, J.; Black, D.; Nicholson, L.; Burns, J.; Refshauge, K. Diagnostic accuracy of clinical tests for ankle syndesmosis injury. Br. J. Sport. Med. 2013, 49, 323–329. [Google Scholar] [CrossRef]
- Hocevar, L.A.; Fitzgerald, B.M. American Society of Anesthesiologists Staging. In StatPearls; StatPearls Publishing LLC.: Treasure Island, FL, USA, 2019. [Google Scholar]
- Hayes, M.J.P.B. Experimental developement of the graphics rating method. Physiol. Bull. 1921, 18, 98–99. [Google Scholar]
- Olerud, C.; Molander, H. A scoring scale for symptom evaluation after ankle fracture. Arch. Orthop. Trauma Surg. 1984, 103, 190–194. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, J.; Peterson, L. Evaluation of ankle joint function: The use of a scoring scale. Foot 1991, 1, 15–19. [Google Scholar] [CrossRef]
- Lauge, N. Fractures of the ankle: Analytic Historic Survey as the Basis of New Experimental, Roentgenologic and Clinical Investigations. Arch. Surg. 1948, 56, 259–317. [Google Scholar] [CrossRef]
- Schepers, T.; Van Lieshout, E.; De Vries, M.; Van der Elst, M. Increased rates of wound complications with locking plates in distal fibular fractures. Injury 2011, 42, 1125–1129. [Google Scholar] [CrossRef] [PubMed]
- Yde, J. The Lauge Hansen Classification of Malleolar Fractures. Acta Orthop. Scand. 1980, 51, 181–192. [Google Scholar] [CrossRef]
- Dogra, A.; Rangan, A. Early mobilisation versus immobilisation of surgically treated ankle fractures. Prospective randomised control trial. Injury 1999, 30, 417–419. [Google Scholar] [CrossRef]
- Autoren, H.; Belzl, U.; Ernst, S.; Heining, U.; Hirsch, T.; Riedel, J.; Schmidt, M.; Settner, S. Deutsche Gesellschaft für Orthopädie und Unfallchirurgie (DGOU). Available online: https://dgou.de/fileadmin/dgou/dgou/Dokumente/News/News/2020/2020_Nachbehandlungsempfehlungen.pdf (accessed on 1 February 2022).
- Müller, M.; Greve, F.; Rittstieg, P.; Beirer, M.; Biberthaler, P. Documentation of self-reported patient outcomes in trauma surgery: Clinical benefits of patient reported outcome measures. Unfallchirurg 2020, 123, 354–359. [Google Scholar] [CrossRef]
- Giordano, V.; Boni, G.; Godoy-Santos, A.L.; Pires, R.E.; Fukuyama, J.M.; Koch, H.A.; Giannoudis, P.V. Nailing the fibula: Alternative or standard treatment for lateral malleolar fracture fixation? A broken paradigm. Eur. J. Trauma Emerg. Surg. 2020, 47, 1911–1920. [Google Scholar] [CrossRef]
- Milstrey, A.; Baumbach, S.F.; Pfleiderer, A.; Evers, J.; Boecker, W.; Raschke, M.J.; Polzer, H.; Ochman, S. Trends of incidence and treatment strategies for operatively treated distal fibula fractures from 2005 to 2019: A nationwide register analysis. Arch. Orthop. Trauma. Surg. 2021, 142, 3771–3777. [Google Scholar] [CrossRef]
- Asloum, Y.; Bedin, B.; Roger, T.; Charissoux, J.-L.; Arnaud, J.-P.; Mabit, C. Internal fixation of the fibula in ankle fractures. A prospective, randomized and comparative study: Plating versus nailing. Orthop. Traumatol. Surg. Res. 2014, 100, S255–S259. [Google Scholar] [CrossRef]
- Shih, C.-A.; Jou, I.-M.; Lee, P.-Y.; Lu, C.-L.; Su, W.-R.; Yeh, M.-L.; Wu, P.-T. Treating AO/OTA 44B lateral malleolar fracture in patients over 50 years of age: Periarticular locking plate versus non-locking plate. J. Orthop. Surg. Res. 2020, 15, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Dingemans, S.A.; Lodeizen, O.A.; Goslings, J.C.; Schepers, T. Reinforced fixation of distal fibula fractures in elderly patients; A meta-analysis of biomechanical studies. Clin. Biomech. 2016, 36, 14–20. [Google Scholar] [CrossRef] [PubMed]









{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Rehabilitation Protocol | Week 1–6 after Surgery | Week 7–12 after Surgery |
| DePuy Synthes® One-Third Semitubular Plate | partial weight bearing 20 kg | increase weight bearing load |
| Walking boot | train away the walking boot | |
| crouches | crouches till full weight bearing | |
| pain-adapted motion without limitation | pain-adapted motion without limitation | |
| Week 1–3 after Surgery | Week 4–12 after Surgery | |
| IlluminOss® Photodynamic Bone Stabilization System | full weight bearing | full weight bearing |
| Walking boot | train away the walking boot and switch to an ankle brace | |
| no crouches | no crouches | |
| pain-adapted motion without limitation | pain-adapted motion without limitation |
| Characteristics | DePuy Synthes® One-Third Semitubular Plate | IlluminOss® Photodynamic Bone Stabilization System |
|---|---|---|
| Mean age (years) | ∅76 ± 8 | ∅80 ± 8 |
| Sex (male: female) | 8:10 | 7:14 |
| Side (right:left) | 10:8 | 10:11 |
| Mean BMI | ∅26 | ∅24 |
| Mean CCI | ∅2 ± 1 | ∅2 ± 1 |
| ASA Scoring | ||
| ASA I | 2 | 3 |
| ASA II | 13 | 12 |
| ASA III | 3 | 6 |
| Surgery time (minutes) | ∅45 ± 5 | ∅36 ± 4 |
| Minor Complication | DePuy Synthes® One-Third Semitubular Plate | IlluminOss® Photodynamic Bone Stabilization System | p-Values |
|---|---|---|---|
| Swelling/redness | 2 (11%) | ||
| deep vein thrombosis | 1 (5.5%) | ||
| respiratory infection | 1 (5.5%) | ||
| p = 0.01 | |||
| Major Complication | |||
| deep wound infection | 1 (5.5%) | ||
| Loss of reposition | 1 (4.7%) | ||
| p = 0.47 |
| Treatment Group | Scores | 6 Weeks | 12 Weeks | 6 Months | 12 Months |
|---|---|---|---|---|---|
| VAS | |||||
| Group I | 4 ±.1 | 2.94 ± 0.89 | 2.41 ± 1.00 | 1.94 ± 0.65 | |
| Group II | 3.19 ± 0.9 | 2.52 ± 0.92 | 2.2 ± 0.76 | 1.70 ± 0.73 | |
| p value | 0.01 | 0.09 | 0.24 | 0.15 | |
| OMAS | |||||
| Group I | ∅44.3 ± 18 | ∅55.9 ± 16 | ∅63.8 ± 15 | ∅70.3 ± 8 | |
| Group II | ∅63.7 ± 12 | ∅67.5 ± 14 | ∅71.2 ± 10 | ∅76.2 ± 10 | |
| p value | 0.01 | 0.01 | 0.06 | 0.07 | |
| KPSS | |||||
| Group I | ∅40.61 ± 10 | ∅52.30 ± 11 | ∅66.52 ± 12 | ∅69.98 ± 13 | |
| Group II | ∅57.04 ± 10 | ∅61.17 ± 9 | ∅72.3 ± 11 | ∅76.63 ± 9 | |
| p value | 0.01 | 0.02 | 0.06 | 0.06 |
| ROM | 6 Weeks | 12 Weeks | 6 Months | 12 Months |
|---|---|---|---|---|
| Group I | ||||
| Extension(dorsiflexion) | ∅4 ± 2 | ∅10 ± 3 | ∅14 ± 2 | ∅18 ± 2 |
| Flexion | ∅20 ± 4 | ∅23 ± 4 | ∅32 ± 4 | ∅35 ± 3 |
| Group II | ||||
| Extension(dorsiflexion) | ∅10 ± 2 | ∅15 ± 4 | ∅18 ± 4 | ∅18 ± 2 |
| Flexion | ∅25 ± 4 | ∅32 ± 3 | ∅34 ± 4 | ∅36 ± 2 |
| p value | ||||
| Extension(dorsiflexion) | 0.01 | 0.01 | 0.03 | 0.47 |
| Flexion | 0.01 | 0.01 | 0.07 | 0.19 |
| Interval between Trauma and Surgery | Days |
| general | ∅8 days |
| DePuy Synthes® one-third semitubular plate | ∅9 days |
| IlluminOss® Photodynamic Bone Stabilization System | ∅4 days |
| p = 0.01 | |
| Length of Hospital Stay | Days |
| general | ∅6 days |
| DePuy Synthes® one-third semitubular plate | ∅9 days |
| IlluminOss® Photodynamic Bone Stabilization System | ∅5 days |
| p = 0.05 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Zyskowski, M.; Wurm, M.; Greve, F.; Zehnder, P.; Pflüger, P.; Müller, M.; Biberthaler, P.; Kirchhoff, C. A Prospective Randomized Study Comparing Functional Outcome in Distal Fibula Fractures between Conventional AO Semitubular Plating and Minimal Invasive Intramedullary “Photodynamic Bone Stabilisation”. J. Clin. Med. 2022, 11, 7178. https://doi.org/10.3390/jcm11237178
Zyskowski M, Wurm M, Greve F, Zehnder P, Pflüger P, Müller M, Biberthaler P, Kirchhoff C. A Prospective Randomized Study Comparing Functional Outcome in Distal Fibula Fractures between Conventional AO Semitubular Plating and Minimal Invasive Intramedullary “Photodynamic Bone Stabilisation”. Journal of Clinical Medicine. 2022; 11(23):7178. https://doi.org/10.3390/jcm11237178
Chicago/Turabian StyleZyskowski, Michael, Markus Wurm, Frederik Greve, Philipp Zehnder, Patrick Pflüger, Michael Müller, Peter Biberthaler, and Chlodwig Kirchhoff. 2022. "A Prospective Randomized Study Comparing Functional Outcome in Distal Fibula Fractures between Conventional AO Semitubular Plating and Minimal Invasive Intramedullary “Photodynamic Bone Stabilisation”" Journal of Clinical Medicine 11, no. 23: 7178. https://doi.org/10.3390/jcm11237178
APA StyleZyskowski, M., Wurm, M., Greve, F., Zehnder, P., Pflüger, P., Müller, M., Biberthaler, P., & Kirchhoff, C. (2022). A Prospective Randomized Study Comparing Functional Outcome in Distal Fibula Fractures between Conventional AO Semitubular Plating and Minimal Invasive Intramedullary “Photodynamic Bone Stabilisation”. Journal of Clinical Medicine, 11(23), 7178. https://doi.org/10.3390/jcm11237178