
Electrocardiographic Parameters Associated with Adverse Outcomes in Children with Cardiomyopathies



Abstract
1. Introduction
2. Materials and Methods
2.1. Electrocardiography (ECG)
2.2. Echocardiography
2.3. Statistical Analysis
3. Results
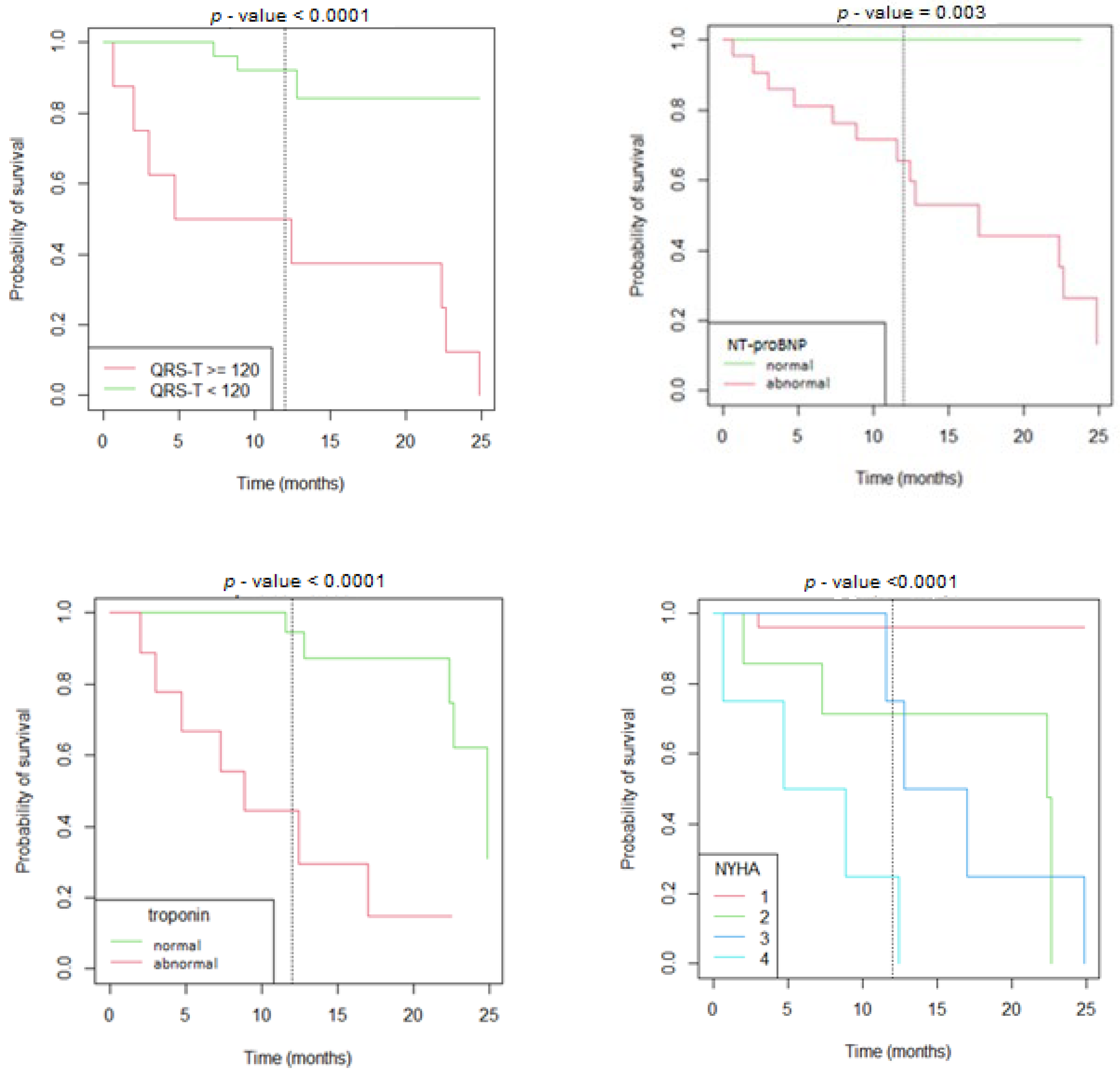
3.1. Dilated Cardiomyopathy
3.2. Hypertrophic Cardiomyopathy
4. Discussion
4.1. Dilated Cardiomyopathy
4.2. Hypertrophic Cardiomyopathy
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Oehler, A.; Feldman, T.; Henrikson, C.A.; Tereshchenko, L.G. QRS-T angle: A review. Ann. Noninvasive Electrocardiol. 2014, 19, 534–542. [Google Scholar] [CrossRef] [PubMed]
- Chaudhry, U.; Cortez, D.; Platonov, P.G.; Carlson, J.; Borgquist, R. Vectorcardiography Findings Are Associated with Recurrent Ventricular Arrhythmias and Mortality in Patients with Heart Failure Treated with Implantable Cardioverter-Defibrillator Device. Cardiology 2020, 145, 784–794. [Google Scholar] [CrossRef] [PubMed]
- Pavri, B.B.; Hillis, M.B.; Subacius, H.; Brumberg, G.E.; Schaechter, A.; Levine, J.H.; Kadish, A.; Defibrillators in Nonischemic Cardiomyopathy Treatment Evaluation (DEFINITE) Investigators. Prognostic value and temporal behavior of the planar QRS-T angle in patients with nonischemic cardiomyopathy. Circulation 2008, 117, 3181–3186. [Google Scholar] [CrossRef] [PubMed]
- Li, S.N.; Zhang, X.L.; Cai, G.L.; Lin, R.W.; Jiang, H.; Chen, J.Z.; Xu, B.; Huang, W. Prognostic Significance of Frontal QRS-T Angle in Patients with Idiopathic Dilated Cardiomyopathy. Chin. Med. J. 2016, 129, 1904–1911. [Google Scholar] [CrossRef]
- Guner, A.; Kalcik, M.; Celik, M.; Uzun, F.; Cizgici, A.Y.; Agus, H.Z.; Aslan, S.; Guner, E.G.; Ulutas, A.E.; Bayam, E.; et al. Impaired repolarization parameters may predict fatal ventricular arrhythmias in patients with hypertrophic cardiomyopathy (from the CILICIA Registry). J. Electrocardiol. 2020, 63, 83–90. [Google Scholar] [CrossRef]
- Cortez, D.; Graw, S.; Mestroni, L. In Hypertrophic Cardiomyopathy, the Spatial Peaks QRS-T Angle Identifies Those with Sustained Ventricular Arrhythmias. Clin. Cardiol. 2016, 39, 459–463. [Google Scholar] [CrossRef]
- Hanses, U.; Kleinsorge, M.; Roos, L.; Yigit, G.; Li, Y.; Barbarics, B.; El-Battrawy, I.; Lan, H.; Tiburcy, M.; Hindmarsh, R.; et al. Intronic CRISPR Repair in a Preclinical Model of Noonan Syndrome-Associated Cardiomyopathy. Circulation 2020, 142, 1059–1076. [Google Scholar] [CrossRef]
- Sedaghat-Hamedani, F.; Rebs, S.; El-Battrawy, I.; Chasan, S.; Krause, T.; Haas, J.; Zhong, R.; Liao, Z.; Xu, Q.; Zhou, X.; et al. Identification of SCN5a p.C335R Variant in a Large Family with Dilated Cardiomyopathy and Conduction Disease. Int. J. Mol. Sci. 2021, 22, 12990. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Zhao, Z.; Lan, H.; Li, X.; Yucel, G.; Lang, S.; Sattler, K.; Schunemann, J.D.; Zimmermann, W.H.; Cyganek, L.; et al. Ion Channel Dysfunctions in Dilated Cardiomyopathy in Limb-Girdle Muscular Dystrophy. Circ. Genom. Precis. Med. 2018, 11, e001893. [Google Scholar] [CrossRef]
- Fan, X.; Yang, G.; Kowitz, J.; Duru, F.; Saguner, A.M.; Akin, I.; Zhou, X.; El-Battrawy, I. Preclinical short QT syndrome models: Studying the phenotype and drug-screening. Europace 2022, 24, 481–493. [Google Scholar] [CrossRef]
- El-Battrawy, I.; Lan, H.; Cyganek, L.; Maywald, L.; Zhong, R.; Zhang, F.; Xu, Q.; Lee, J.; Duperrex, E.; Hierlemann, A.; et al. Deciphering the pathogenic role of a variant with uncertain significance for short QT and Brugada syndromes using gene-edited human-induced pluripotent stem cell-derived cardiomyocytes and preclinical drug screening. Clin. Transl. Med. 2021, 11, e646. [Google Scholar] [CrossRef] [PubMed]
- El-Battrawy, I.; Lang, S.; Zhou, X.; Akin, I. Different genotypes of Brugada syndrome may present different clinical phenotypes: Electrophysiology from bench to bedside. Eur. Heart J. 2021, 42, 1270–1272. [Google Scholar] [CrossRef] [PubMed]
- Pappone, C.; Micaglio, E.; Locati, E.T.; Monasky, M.M. The omics of channelopathies and cardiomyopathies: What we know and how they are useful. Eur. Heart J. Suppl. 2020, 22, L105–L109. [Google Scholar] [CrossRef] [PubMed]
- Cortez, D.; Sharma, N.; Cavanaugh, J.; Tuozo, F.; Derk, G.; Lundberg, E.; Weiner, K.; Kiciman, N.; Alejos, J.; Landeck, B.; et al. Lower spatial QRS-T angle rules out sustained ventricular arrhythmias in children with hypertrophic cardiomyopathy. Cardiol. Young 2017, 27, 354–358. [Google Scholar] [CrossRef]
- Cortez, D.; Sharma, N.; Imundo, J.R. Pediatric noncompaction patients with high spatial QRS-T angles are at increased risk for ventricular tachycardia. Ann. Noninvasive Electrocardiol. 2019, 24, e12588. [Google Scholar] [CrossRef]
- Lipshultz, S.E.; Law, Y.M.; Asante-Korang, A.; Austin, E.D.; Dipchand, A.I.; Everitt, M.D.; Hsu, D.T.; Lin, K.Y.; Price, J.F.; Wilkinson, J.D.; et al. Cardiomyopathy in Children: Classification and Diagnosis: A Scientific Statement from the American Heart Association. Circulation 2019, 140, e9–e68. [Google Scholar] [CrossRef]
- Perry, E.; Aris, A.; Michael, B.; Martin, B.; Cecchi, F.; Charron, P.; Hagege, A.A.; Lafont, A.; Limongelli, G.; Mahrholdt, H. ESC Guidelines on diagnosis and management of hypertrophic cardiomyopathy: The Task Force for the Diagnosis and Management of Hypertrophic Cardiomyopathy of the European Society of Cardiology (ESC). Eur. Heart J. 2014, 35, 2733–2779. [Google Scholar]
- Jenni, R.; Oechslin, E.; Schneider, J.; Attenhofer Jost, C.; Kaufmann, P.A. Echocardiographic and pathoanatomical characteristics of isolated left ventricular non-compaction: A step towards classification as a distinct cardiomyopathy. Heart 2001, 86, 666–671. [Google Scholar] [CrossRef]
- Ross, R.D.; Daniels, S.R.; Schwartz, D.C.; Hannon, D.W.; Shukla, R.; Kaplan, S. Plasma norepinephrine levels in infants and children with congestive heart failure. Am. J. Cardiol. 1987, 59, 911–914. [Google Scholar] [CrossRef]
- Kors, J.A.; van Herpen, G.; Sittig, A.C.; van Bemmel, J.H. Reconstruction of the Frank vectorcardiogram from standard electrocardiographic leads: Diagnostic comparison of different methods. Eur. Heart J. 1990, 11, 1083–1092. [Google Scholar] [CrossRef]
- Cortez, D.; Sharma, N.; Devers, C.; Devers, E.; Schlegel, T.T. Visual transform applications for estimating the spatial QRS-T angle from the conventional 12-lead ECG: Kors is still most Frank. J. Electrocardiol. 2014, 47, 12–19. [Google Scholar] [CrossRef] [PubMed]
- Lopez, L.; Colan, S.D.; Frommelt, P.C.; Ensing, G.J.; Kendall, K.; Younoszai, A.K.; Lai, W.W.; Geva, T. Recommendations for quantification methods during the performance of a pediatric echocardiogram: A report from the Pediatric Measurements Writing Group of the American Society of Echocardiography Pediatric and Congenital Heart Disease Council. J. Am. Soc. Echocardiogr. Off. Publ. Am. Soc. Echocardiogr. 2010, 23, 465–495. [Google Scholar] [CrossRef] [PubMed]
- Chen, S.; Motonaga, K.S.; Hollander, S.A.; Almond, C.S.; Rosenthal, D.N.; Kaufman, B.D.; May, L.J.; Avasarala, K.; Dao, D.T.; Dubin, A.M.; et al. Electrocardiographic repolarization abnormalities and increased risk of life-threatening arrhythmias in children with dilated cardiomyopathy. Heart Rhythm 2016, 13, 1289–1296. [Google Scholar] [CrossRef] [PubMed]
- Ture, M.; Balik, H.; Akin, A.; Bilici, M.; Nergiz, A. The relationship between electrocardiographic data and mortality in children diagnosed with dilated cardiomyopathy. Eur. J. Pediatr. 2020, 179, 813–819. [Google Scholar] [CrossRef]
- Meulen, M.; Boer, S.; du Marchie Sarvaas, G.; Blom, N.; Harkel, A.; Breur, H.; Rammeloo, L.; Tanke, R.; Bogers, A.; Helbing, W.; et al. Predicting outcome in children with dilated cardiomyopathy: The use of repeated measurements of risk factors for outcome. ESC Heart Fail. 2021, 8, 1472–1481. [Google Scholar] [CrossRef]
- Li, X.; Luo, R.; Jiang, R.; Kong, H.; Tang, Y.; Shu, Y.; Hua, W. The prognostic use of serum concentrations of cardiac troponin-I, CK-MB and myoglobin in patients with idiopathic dilated cardiomyopathy. Heart Lung 2014, 43, 219–224. [Google Scholar] [CrossRef]
- Kawahara, C.; Tsutamoto, T.; Nishiyama, K.; Yamaji, M.; Sakai, H.; Fujii, M.; Yamamoto, T.; Horie, M. Prognostic role of high-sensitivity cardiac troponin T in patients with nonischemic dilated cardiomyopathy. Circ. J. Off. J. Jpn. Circ. Soc. 2011, 75, 656–661. [Google Scholar]
- Kadakia, R.S.; Link, M.S.; Dominic, P.; Morin, D.P. Sudden cardiac death in nonischemic cardiomyopathy. Prog. Cardiovasc. Dis. 2019, 62, 235–241. [Google Scholar] [CrossRef]
- Chmielewski, P.; Michalak, E.; Kowalik, I.; Franaszczyk, M.; Sobieszczanska-Malek, M.; Truszkowska, G.; Stepien-Wojno, M.; Biernacka, E.K.; Foss-Nieradko, B.; Lewandowski, M.; et al. Can Circulating Cardiac Biomarkers Be Helpful in the Assessment of LMNA Mutation Carriers? J. Clin. Med. 2020, 9, 1443. [Google Scholar] [CrossRef]
- Bharucha, T.; Lee, K.J.; Daubeney, P.E.; Nugent, A.W.; Turner, C.; Sholler, G.F.; Robertson, T.; Justo, R.; Ramsay, J.; Carlin, J.B.; et al. Sudden death in childhood cardiomyopathy: Results from a long-term national population-based study. J Am Coll Cardiol 2015, 65, 2302–2310. [Google Scholar] [CrossRef]
- Norrish, G.; Topriceanu, C.; Qu, C.; Field, E.; Walsh, H.; Ziolkowska, L.; Olivotto, I.; Passantino, S.; Favilli, S.; Anastasakis, A.; et al. The role of the electrocardiographic phenotype in risk stratification for sudden cardiac death in childhood hypertrophic cardiomyopathy. Eur. J. Prev. Cardiol. 2022, 29, 645–653. [Google Scholar] [CrossRef] [PubMed]
- Cortez, D.; Schlegel, T.T.; Ackerman, M.J.; Bos, J.M. ECG-derived spatial QRS-T angle is strongly associated with hypertrophic cardiomyopathy. J. Electrocardiol. 2017, 50, 195–202. [Google Scholar] [CrossRef] [PubMed]
- Kaski, J.P.; Tomé-Esteban, M.T.; Mead-Regan, S.; Pantazis, A.; Marek, J.; Deanfield, J.E.; McKenna, W.J.; Elliott, P.M. B-type natriuretic peptide predicts disease severity in children with hypertrophic cardiomyopathy. Heart 2008, 94, 1307. [Google Scholar] [CrossRef] [PubMed]
- Coats, C.J.; Gallagher, M.J.; Foley, M.; O’Mahony, C.; Critoph, C.; Gimeno, J.; Dawnay, A.; McKenna, W.J.; Elliott, P.M. Relation between serum N-terminal pro-brain natriuretic peptide and prognosis in patients with hypertrophic cardiomyopathy. Eur. Heart J. 2013, 34, 2529–2537. [Google Scholar] [CrossRef]
- Aquaro, G.D.; Corsi, E.; Todiere, G.; Grigoratos, C.; Barison, A.; Barra, V.; Di Bella, G.; Emdin, M.; Ricci, F.; Pingitore, A. Magnetic Resonance for Differential Diagnosis of Left Ventricular Hypertrophy: Diagnostic and Prognostic Implications. J. Clin. Med. 2022, 11, 651. [Google Scholar] [CrossRef] [PubMed]
- Kubo, T.; Kitaoka, H.; Yamanaka, S.; Hirota, T.; Baba, Y.; Hayashi, K.; Iiyama, T.; Kumagai, N.; Tanioka, K.; Yamasaki, N.; et al. Significance of High-Sensitivity Cardiac Troponin T in Hypertrophic Cardiomyopathy. J. Am. Coll. Cardiol. 2013, 62, 1252–1259. [Google Scholar] [CrossRef]
- Gommans, D.H.F.; Cramer, G.E.; Fouraux, M.A.; Heijmans, S.; Michels, M.; Timmermans, J.; Verheugt, F.W.A.; de Boer, R.A.; Kofflard, M.J.M.; Brouwer, M.A. Usefulness of High-Sensitivity Cardiac Troponin T to Predict Long-Term Outcome in Patients with Hypertrophic Cardiomyopathy. Am. J. Cardiol. 2021, 152, 120–124. [Google Scholar] [CrossRef]
- Jensen, C.J.; Lambers, M.; Zadeh, B.; Wambach, J.M.; Nassenstein, K.; Bruder, O. QRS-T angle in patients with Hypertrophic Cardiomyopathy—A comparison with Cardiac Magnetic Resonance Imaging. Int. J. Med. Sci. 2021, 18, 821–825. [Google Scholar] [CrossRef]



{kind=link}
{kind=link}
| DCM n = 19 | HCM n = 17 | LVNC n = 6 | Control n = 19 | p-Value | |
|---|---|---|---|---|---|
| gender (n female/male) | 10/9 | 8/9 | 5/1 | 10/9 | 0.49 |
| Age (years) | 8 (3–14) | 10 (3–16.5) | 10.5 (8–15.5) | 8 (4–15) | 0.73 |
| BSA (m2) | 1.1 (0.6–1.8) | 1.5(0.6–1.9) | 1.1(0.9–1.3) | 1.2(0.7–1.7) | 0.85 |
| observation time (months) | 14 ± 8 | 11 ± 7 | 12 ± 8 | n/a | 0.42 |
| QRS-T Angle | |||
|---|---|---|---|
| No End Point | Met End Point | p-Value | |
| VT | 70.1° ± 31.8° | 137.2° ± 25.3° | <0.001 |
| ICD | 72.5° ± 34.5° | 135.6° ± 24.2° | <0.001 |
| HTx | 74.7° ± 36.6° | 133.7° ± 22.8° | <0.001 |
| All end points | 64.7° ± 28° | 133.2° ± 23° | <0.001 |
| DCM no MACE n = 13 | DCM MACE n = 6 | p-Value | |
|---|---|---|---|
| HR (bpm) | 88 (82–100) | 100 (74–137) | 0.759 |
| PQ (ms) | 123.8 ± 18.5 | 140.0 ± 28.9 | 0.157 |
| QRS (ms) | 76.2 ± 10.4 | 85.0 ± 18.7 | 0.317 |
| QTc (ms) | 392.9 ± 31.4 | 431.1 ± 38.9 | 0.035 |
| QRS-T (degrees) | 48.2 ± 22.9 | 133.7 ± 22.8 | <0.001 |
| Negative T-waves ≥ 2 leads | 0 | 4 (66%) | 0.007 |
| NT-proBNP (pg/mL) | 58 (37–146) | 3068 (2123–3810) | <0.001 |
| Troponin (ng/mL) | 2.7 (1.5–9.5) | 48.9 (25.9–95.4) | 0.013 |
| NYHA/Ross (I/II/III/IV) | 13 (100%)/0/0/0 | 0/1 (17%)/1 (17%)/4 (66%) | <0.001 |
| LVEF % | 44.4 ± 6.78 | 21.9 ± 5.78 | <0.001 |
| LVIDd z-score | 2.86 ± 0.87 | 5.50 ± 0.77 | <0.001 |
| LVPWD z-score | 0.33 ± 0.493 | 1.07 ± 0.66 | 0.042 |
| HCM no MACE n = 11 | HCM MACE n = 6 | p-Value | |
|---|---|---|---|
| HR (bpm) | 97.4 ± 26.98 | 73.8 ± 17.72 | 0.048 |
| PQ (ms) | 120 (120–135) | 140 (140–163) | 0.021 |
| QRS (ms) | 70 (70–70) | 105 (85–118) | 0.002 |
| QTc (ms) | 406.9 ± 27.46 | 433.6 ± 34.32 | 0.1 |
| QRS-T (degrees) | 84.6 ± 25.69 | 132.5 ± 26 | 0.004 |
| Negative T-waves ≥ 2 leads | 2 (18%) | 5 (100%) | 0.012 |
| ST elevation | 0 | 3 (50%) | 0.055 |
| ST depression | 1 (9%) | 3 (50%) | 0.193 |
| LVH | 0 (0%) | 5 (83%) | 0.416 |
| NT-proBNP (pg/mL) | 124.5 (45–908) | 2659 (1611–4894) | 0.011 |
| Troponin (ng/mL) | 8.7 (1.5–26.4) | 50.1 (24.4–131.1) | 0.06 |
| NYHA/Ross (I/II/III/IV) | 8 (73%)/3 (27%)/0/0 | 1 (17%)/3 (50%)/2 (33%)/0 | 0.038 |
| LVEF % | 61.9 ± 6.73 | 51.7 ± 19.01 | 0.253 |
| LVIDD z-score | −1.87 ± 1.576 | −1.74 ± 2.471 | 0.909 |
| LVPWD z-score | 2.90 (2.15–4.1) | 6.40 (2.85–10.25) | 0.191 |
| IVSd z-score | 7.4 ± 4.4 | 12.6 ± 4.7 | 0.052 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Luczak-Wozniak, K.; Obsznajczyk, K.; Niszczota, C.; Werner, B. Electrocardiographic Parameters Associated with Adverse Outcomes in Children with Cardiomyopathies. J. Clin. Med. 2022, 11, 6930. https://doi.org/10.3390/jcm11236930
Luczak-Wozniak K, Obsznajczyk K, Niszczota C, Werner B. Electrocardiographic Parameters Associated with Adverse Outcomes in Children with Cardiomyopathies. Journal of Clinical Medicine. 2022; 11(23):6930. https://doi.org/10.3390/jcm11236930
Chicago/Turabian StyleLuczak-Wozniak, Katarzyna, Klaudia Obsznajczyk, Cezary Niszczota, and Bożena Werner. 2022. "Electrocardiographic Parameters Associated with Adverse Outcomes in Children with Cardiomyopathies" Journal of Clinical Medicine 11, no. 23: 6930. https://doi.org/10.3390/jcm11236930
APA StyleLuczak-Wozniak, K., Obsznajczyk, K., Niszczota, C., & Werner, B. (2022). Electrocardiographic Parameters Associated with Adverse Outcomes in Children with Cardiomyopathies. Journal of Clinical Medicine, 11(23), 6930. https://doi.org/10.3390/jcm11236930