
The Role of Antihyperglycemic Drugs and Diet on Erectile Function: Results from a Perspective Study on a Population with Prediabetes and Diabetes

 ,
,  , ,
, , 
Abstract
1. Introduction
2. Materials and Methods
Statistical Analysis
3. Results
4. Discussion
Limits and Future Perspective
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Lewis, R.W.; Fugl-Meyer, K.S.; Corona, G.; Hayes, R.D.; Laumann, E.O.; Moreira, E.D.; Rellini, A.H.; Segraves, T. Definitions/Epidemiology/Risk Factors for Sexual Dysfunction. J. Sex. Med. 2010, 7, 1598–1607. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Giorda, C.B.; Cucinotta, D.; Guida, P.; Nada, E.; Aglialoro, A.; Albanese, V.; Albano, S.; Antonangelo, C.; Baccetti, F.; et al. Sexual Dysfunction at the Onset of Type 2 Diabetes: The Interplay of Depression, Hormonal and Cardiovascular Factors. J. Sex. Med. 2014, 11, 2065–2073. [Google Scholar] [CrossRef] [PubMed]
- Isidori, A.M.; Giammusso, B.; Corona, G.; Verze, P.; Albanesi, L.; Antomarchi, F.; Arcaniolo, D.; Balercia, G.; Barbonetti, A.; Barletta, D.; et al. Diagnostic and Therapeutic Workup of Erectile Dysfunction: Results from a Delphi Consensus of Andrology Experts. Sex. Med. 2019, 7, 292–302. [Google Scholar] [CrossRef] [PubMed]
- Faulkner, L.D.; Dowling, A.R.; Stuart, R.C.; Nillni, E.A.; Hill, J.W. Reduced Melanocortin Production Causes Sexual Dysfunction in Male Mice with POMC Neuronal Insulin and Leptin Insensitivity. Endocrinology 2015, 156, 1372–1385. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Moon, K.H.; Park, S.Y.; Kim, Y.W. Obesity and Erectile Dysfunction: From Bench to Clinical Implication. World J. Men’s Health 2019, 37, 138–147. [Google Scholar] [CrossRef]
- Trussell, J.C.; Legro, R.S. Erectile Dysfunction: Does Insulin Resistance Play a Part? Fertil. Steril. 2007, 88, 771–778. [Google Scholar] [CrossRef]
- Defeudis, G.; Mazzilli, R.; Tenuta, M.; Rossini, G.; Zamponi, V.; Olana, S.; Faggiano, A.; Pozzilli, P.; Isidori, A.M.; Gianfrilli, D. Erectile Dysfunction and Diabetes: A Melting Pot of Circumstances and Treatments. Diabetes Metab. Res. Rev. 2022, 38, e3494. [Google Scholar] [CrossRef]
- Chester, B.; Babu, J.R.; Greene, M.W.; Geetha, T. The Effects of Popular Diets on Type 2 Diabetes Management. Diabetes Metab. Res. Rev. 2019, 35, e3188. [Google Scholar] [CrossRef]
- Maurizi, A.R.; Menduni, M.; Del Toro, R.; Kyanvash, S.; Maggi, D.; Guglielmi, C.; Pantano, A.L.; Defeudis, G.; Fioriti, E.; Manfrini, S.; et al. A Pilot Study of D-Chiro-Inositol plus Folic Acid in Overweight Patients with Type 1 Diabetes. Acta Diabetol. 2017, 54, 361–365. [Google Scholar] [CrossRef]
- Defeudis, G.; Khazrai, Y.M.; Di Rosa, C.; Secchi, C.; Montedoro, A.; Maurizi, A.R.; Palermo, A.; Pozzilli, P.; Manfrini, S. Conversation Maps™, an Effective Tool for the Management of Males and Females with Type 2 Diabetes and Mildly Impaired Glycemic Control. Hormones 2018, 17, 113–117. [Google Scholar] [CrossRef]
- American Diabetes Association. Addendum. 9. Pharmacologic Approaches to Glycemic Treatment: Standards of Medical Care in Diabetes—2020. Diabetes Care 2020;43(Suppl. 1):S98–S110. Diabetes Care 2020, 43, 1979. [Google Scholar] [CrossRef] [PubMed]
- Corona, G.; Isidori, A.M.; Aversa, A.; Bonomi, M.; Ferlin, A.; Foresta, C.; La Vignera, S.; Maggi, M.; Pivonello, R.; Vignozzi, L.; et al. Male and Female Sexual Dysfunction in Diabetic Subjects: Focus on New Antihyperglycemic Drugs. Rev. Endocr. Metab. Disord. 2020, 21, 57–65. [Google Scholar] [CrossRef] [PubMed]
- Cignarelli, A.; Genchi, V.A.; D’oria, R.; Giordano, F.; Caruso, I.; Perrini, S.; Natalicchio, A.; Laviola, L.; Giorgino, F. Role of Glucose-Lowering Medications in Erectile Dysfunction. J. Clin. Med. 2021, 10, 2501. [Google Scholar] [CrossRef]
- Defeudis, G.; Mazzilli, R.; Di Tommaso, A.M.; Zamponi, V.; Carlomagno, F.; Tuccinardi, D.; Watanabe, M.; Faggiano, A.; Gianfrilli, D. Effects of Diet and Antihyperglycemic Drugs on Erectile Dysfunction: A Systematic Review. Andrology 2022. [Google Scholar] [CrossRef] [PubMed]
- Rey-Valzacchi, G.N.J.; Costanzo, P.R.; Finger, L.A.; Layus, A.O.; Gueglio, G.M.; Litwak, L.N.E.; Knoblovits, P. Addition of Metformin to Sildenafil Treatment for Erectile Dysfunction in Eugonadal Nondiabetic Men with Insulin Resistance. A Prospective, Randomized, Double-Blind Pilot Study. J. Androl. 2012, 33, 608–614. [Google Scholar] [CrossRef]
- Giagulli, V.A.; Carbone, M.D.; Ramunni, M.I.; Licchelli, B.; De Pergola, G.; Sabbà, C.; Guastamacchia, E.; Triggiani, V. Adding Liraglutide to Lifestyle Changes, Metformin and Testosterone Therapy Boosts Erectile Function in Diabetic Obese Men with Overt Hypogonadism. Andrology 2015, 3, 1094–1103. [Google Scholar] [CrossRef]
- Yue, L.; Xu, J.L.; Dong, J.; da Xjang, G.; Xiang, L.; Zhao, L.S.; Zhang, J.X.; Zhai, Z.Y.; Zhu, G.P.; Liu, M.; et al. Regulatory Effect of Liraglutide on the Expression of ENOS in the Corpus Cavernosum of Diabetic Rats. Zhonghua Nan Ke Xue 2016, 22, 212–218. [Google Scholar]
- Ilias, I. Re: DPP-4 Inhibition Improves a Sexual Condition? Med. Hypotheses 2016, 89, 96. [Google Scholar] [CrossRef]
- Assaly, R.; Gorny, D.; Compagnie, S.; Mayoux, E.; Bernabe, J.; Alexandre, L.; Giuliano, F.; Behr-Roussel, D. The Favorable Effect of Empagliflozin on Erectile Function in an Experimental Model of Type 2 Diabetes. J. Sex. Med. 2018, 15, 1224–1234. [Google Scholar] [CrossRef]
- Wang, F.; Dai, S.; Wang, M.; Morrison, H. Erectile Dysfunction and Fruit/Vegetable Consumption among Diabetic Canadian Men. Urology 2013, 82, 1330–1335. [Google Scholar] [CrossRef]
- Maiorino, M.I.; Bellastella, G.; Caputo, M.; Castaldo, F.; Improta, M.R.; Giugliano, D.; Esposito, K. Effects of Mediterranean Diet on Sexual Function in People with Newly Diagnosed Type 2 Diabetes: The MÈDITA Trial. J. Diabetes Complicat. 2016, 30, 1519–1524. [Google Scholar] [CrossRef] [PubMed]
- Esposito, K.; Giugliano, F.; Di Palo, C.; Giugliano, G.; Marfella, R.; D’Andrea, F.; D’Armiento, M.; Giugliano, D. Effect of Lifestyle Changes on Erectile Dysfunction in Obese Men: A Randomized Controlled Trial. J. Am. Med. Assoc. 2004, 291, 2978–2984. [Google Scholar] [CrossRef]
- Collins, C.E.; Jensen, M.E.; Young, M.D.; Callister, R.; Plotnikoff, R.C.; Morgan, P.J. Improvement in Erectile Function Following Weight Loss in Obese Men: The SHED-IT Randomized Controlled Trial. Obes. Res. Clin. Pract. 2013, 7, e450–e454. [Google Scholar] [CrossRef] [PubMed]
- Adams, S.W.; Emerson, S.G. Gene Therapy for Leukemia and Lymphoma. Hematol. Oncol. Clin. North Am. 1998, 12, 631–648. [Google Scholar] [CrossRef]
- Società Italiana di Diabetologia (SID); Associazione dei Medici Diabetologi (AMD). Linea Guida Della Società Italiana Di Diabetologia (SID) e Dell’Associazione Dei Medici Diabetologi (AMD)–La Terapia Del Diabete Mellito Di Tipo; Istituto Superiore Di Sanità: Rome, Italy, 2021. [Google Scholar]
- Lifestyle Management: Standards of Medical Care in Diabetesd 2018. Diabetes Care 2018, 41, S38–S50. [CrossRef]
- Rosen, R.C.; Cappelleri, J.C.; Smith, M.D.; Lipsky, J.; Peñ, B.M. Development and Evaluation of an Abridged, 5-Item Version of the International Index of Erectile Function (IIEF-5) as a Diagnostic Tool for Erectile Dysfunction. Int. J. Impot. Res. 1999, 11, 319–326. [Google Scholar] [CrossRef]
- Pontiroli, A.E.; Cortelazzi, D.; Morabito, A. Female Sexual Dysfunction and Diabetes: A Systematic Review and Meta-Analysis. J. Sex. Med. 2013, 10, 1044–1051. [Google Scholar] [CrossRef]
- Zamponi, V.; Mazzilli, R.; Bitterman, O.; Olana, S.; Iorio, C.; Festa, C.; Giuliani, C.; Mazzilli, F.; Napoli, A. Association between Type 1 Diabetes and Female Sexual Dysfunction. BMC Women’s Health 2020, 20. [Google Scholar] [CrossRef]
- Fedele, D.; Coscelli, C.; Santeusanio, F.; Bortolotti, A.; Chatenoud, L.; Colli, E.; Landoni, M.; Parazzini, F. Erectile Dysfunction in Diabetic Subjects in Italy. Diabetes Care 1998, 21, 1973–1977. [Google Scholar] [CrossRef]
- Kouidrat, Y.; Pizzol, D.; Cosco, T.; Thompson, T.; Carnaghi, M.; Bertoldo, A.; Solmi, M.; Stubbs, B.; Veronese, N. High Prevalence of Erectile Dysfunction in Diabetes: A Systematic Review and Meta-Analysis of 145 Studies. Diabet. Med. 2017, 34, 1185–1192. [Google Scholar] [CrossRef]
- Corona, G.; de Vita, G.; Sforza, A.; Maggi, M. Obesity and Erectile Dysfunction. Eur. Urol. Rev. 2009, 4, 73–77. [Google Scholar] [CrossRef]
- Corona, G.; Rastrelli, G.; Filippi, S.; Vignozzi, L.; Mannucci, E.; Maggi, M. Erectile Dysfunction and Central Obesity: An Italian Perspective. Asian J. Androl. 2014, 16, 581–591. [Google Scholar] [CrossRef] [PubMed]
- Mazzilli, R.; Zamponi, V.; Olana, S.; Mikovic, N.; Cimadomo, D.; Defeudis, G.; Faggiano, A. Erectile Dysfunction as a Marker of Endocrine and Glycemic Disorders. J. Endocrinol. Invest. 2022. [Google Scholar] [CrossRef] [PubMed]
- Nicolosi, A.; Moreira, E.D.; Shirai, M.; Bin Mohd Tambi, M.I.; Glasser, D.B. Epidemiology of Erectile Dysfunction in Four Countries: Cross-National Study of the Prevalence and Correlates of Erectile Dysfunction. Urology 2003, 61, 201–206. [Google Scholar] [CrossRef]
- Dalaklioglu, S.; Tasatargil, A.; Kuscu, N.; Celik, S.; Celik-Ozenci, C.; Ozdem, S.; Barutcigil, A.; Kucukcetin, I. Protective Effect of Exendin-4 Treatment on Erectile Dysfunction Induced by Chronic Methylglyoxal Administration in Rats. Peptides 2018, 106, 1–8. [Google Scholar] [CrossRef]
- Bajaj, H.S.; Gerstein, H.C.; Rao-Melacini, P.; Basile, J.; Colhoun, H.; Conget, I.; Cushman, W.C.; Dagenais, G.R.; Franek, E.; Hanefeld, M.; et al. Erectile Function in Men with Type 2 Diabetes Treated with Dulaglutide: An Exploratory Analysis of the REWIND Placebo-Controlled Randomised Trial. Lancet Diabetes Endocrinol. 2021, 9, 484–490. [Google Scholar] [CrossRef]
- Maiorino, M.I.; Bellastella, G.; Della Volpe, E.; Casciano, O.; Scappaticcio, L.; Cirillo, P.; Giugliano, D.; Esposito, K. Erectile Dysfunction in Young Men with Type 1 Diabetes. Int. J. Impot. Res. 2017, 29, 17–22. [Google Scholar] [CrossRef]
- Wessells, H.; Penson, D.F.; Cleary, P.; Rutledge, B.N.; Lachin, J.M.; McVary, K.T.; Schade, D.S.; Sarma, A.V. Effect of Intensive Glycemic Therapy on Erectile Function in Men with Type 1 Diabetes. J. Urol. 2011, 185, 1828–1834. [Google Scholar] [CrossRef]
- Esposito, K.; Giugliano, F.; Maiorino, M.I.; Giugliano, D. Dietary Factors, Mediterranean Diet and Erectile Dysfunction. J. Sex. Med. 2010, 7, 2338–2345. [Google Scholar] [CrossRef]
- Osservatorio ARNO Diabete. Available online: https://www.siditalia.it/clinica/linee-guida-societari/send/80-linee-guida-documenti-societari/5025-rapporto-arno-diabete-2019 (accessed on 31 May 2022).




{kind=link}
{kind=link}
{kind=link}
| Total Group No. 163 | Diet No. 21 | Metformin No. 51 | DPP4i No. 19 | SGLT2i No. 25 | GLP1a No. 20 | Insulin No. 23 | SU No. 4 | |
|---|---|---|---|---|---|---|---|---|
| Age (years; mean ± SD, range) | 62.9 ± 9.3 20–75 | 62.1 ± 11.3 33–75 | 64.1 ± 9.9 20–75 | 64.4 ± 8.3 48–75 | 61.9 ± 9.4 41–74 | 62.3 ± 7.6 48–72 | 60.7 ± 9.4 39–75 | 66.0 ± 4.9 59–70 |
| preDM (yes; no., %) | 15/163 9.2% | 15/21 71.4% a | 0/51 0% | 0/19 0% | 0/25 0% | 0/20 0% | 0/23 0% | 0/4 0% |
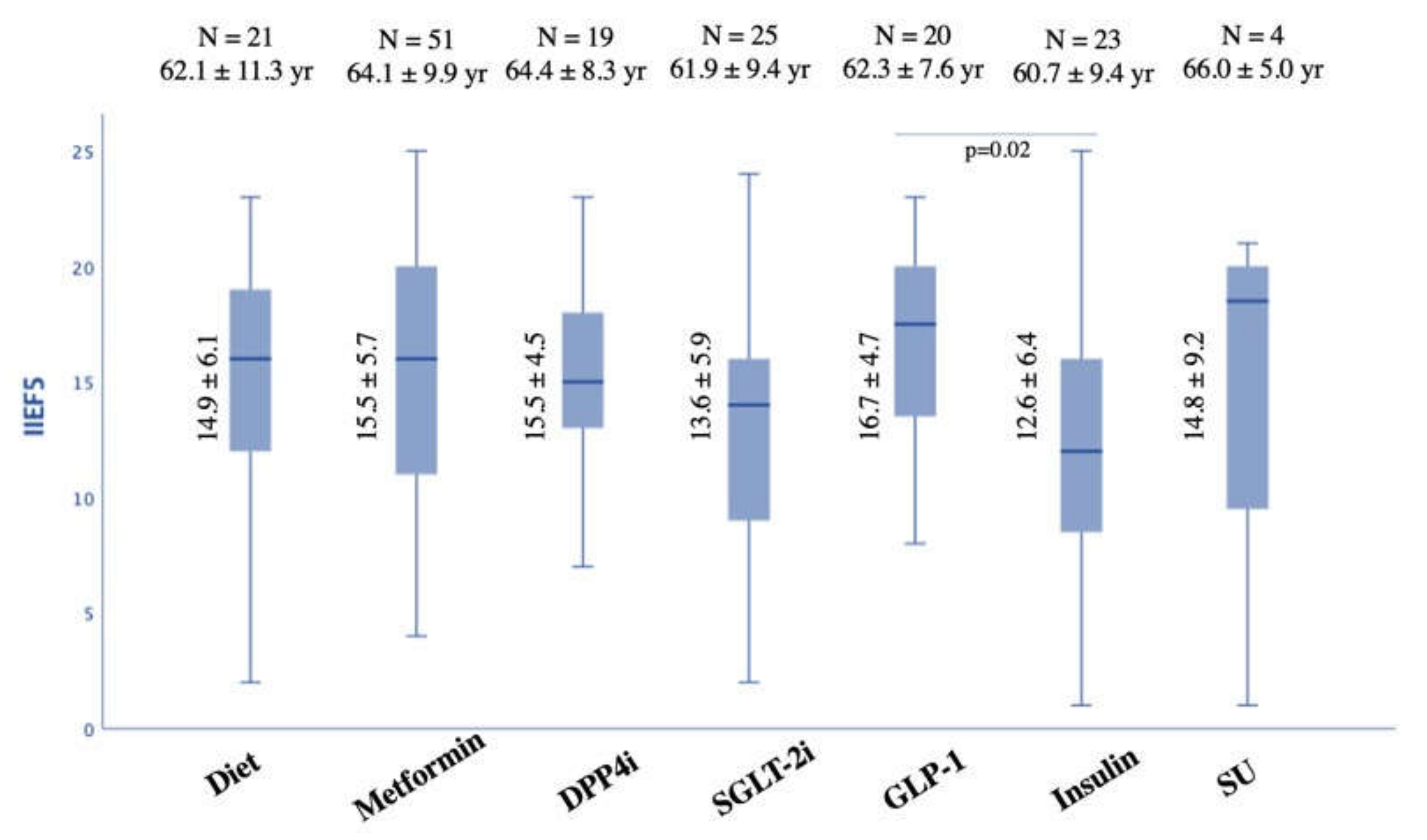
| IIEF-5 (mean ± SD) | 14. ± 5.8 | 14.9 ± 6.1 | 15.5 ± 5.7 | 15.5 ± 4.5 | 13.2 ± 5.9 | 16.7 ± 4.7 b | 12.6 ± 6.4 | 14.8 ± 9.3 |
| IIEF-5 groups | ||||||||
| No ED (> 21) | 21 (12.8%) | 2 (9.5%) | 8 (15.7%) | 2 (10.5%) | 2 (8.0%) | 4 (20.0%) | 3 (13.0%) | 0 (0%) |
| ED (5–21) | 142(87.2%) | 19 (90.5%) | 43 (84.3%) | 17 (89.5%) | 23 (92.0%) | 16 (80.0%) | 20 (87.0%) | 4 (100%) |
| Mild ED (17–21) | 48 (29.4%) | 8 (38.1%) | 16 (31.4%) | 7 (36.8%) | 4 (16.0%) | 8 (40.0%) b | 2 (8.7%) | 3 (75.0%) |
| Mild/Moderate (12–16) | 44 (27.0%) | 6 (28.6%) | 13 (25.5%) | 6 (31.6%) | 8 (32.0%) | 4 (20.0%) | 7 (30.4%) | 0 (0%) |
| Moderate ED (8–11) | 30 (18.4%) | 2 (9.5%) | 8 (15.7%) | 3 (15.8%) | 7 (28.0%) | 4 (20.0%) | 6 (26.1%) | 0 (0%) |
| Severe ED (5–7) | 20 (12.3%) | 3 (14.3% | 6 (11.8%) | 1 (5.3%) | 4 (16.0%) | 0 (0%) | 5 (21.3%) | 1 (25.0%) |
| BMI | 28.4 ± 4.6 | 28.1 ± 3.5 | 28.1 ± 3.6 | 26.4 ± 3.1 | 29.8 ± 5.9 | 29.3 ± 5.6 | 28.1 ± 5.0 | 30.4 ± 2.1 |
| (Kg/m2; mean ± SD, range) | 18.4–45.9 | 19.6–36.7 | 19.6–36.7 | 18.4–32.7 | 21.1–44.3 | 22.5–45.9 | 19–38.6 | 28.1–33.0 |
| BMI groups (n,%) | ||||||||
| Normal weight | 36 (22.1%) | 6 (28.6%) | 8 (15.7%) | 6 (31.6%) | 5 (20.0%) | 5 (25.0%) | 6 (26.1%) | 0 (0%) |
| Overweight | 72 (44.2%) | 9 (42.8%) | 27 (52.9%) | 10 (52.6) | 10 (40.0%) | 7 (35.0%) | 7 (30.4%) | 2 (50.0%) |
| Obese | 55 (33.7%) | 6 (28.6%) | 16 (31.4%) | 3 (15.8%) | 10 (40.0%) | 8 (40.0%) | 10 (43.5%) | 2 (50.0%) |
| Physical activity | 64/163 | 8/21 | 22/51 | 7/19 | 8/25 | 2/20 | 14/23 | 3/4 |
| (yes, no., %) | 39.4% | 38.1% | 43.1% | 36.8% | 32.0% | 10.0% | 60.9% b | 60.9% |
| Smoking habits | ||||||||
| No (no., %) | 53 (32.5%) | 9 (42.9%) | 23 (45.1%) | 1 (5.3%) | 6 (24.0%) | 9 (45.0%) | 3 (13.0%) | 2 (50.0%) |
| Yes (no., %) | 34 (20.9%) | 4 (19.0%) | 5 (9.8%) | 7 (36.8%) | 6 (24.0%) | 2 (10.0%) | 10 (43.5%) c | 0 (0%) |
| In the past (no., %) | 76 (46.6%) | 8 (38.1%) | 23 (45.1%) | 11 (57.9%) | 13 (52.0%) | 9 (45.0%) | 10 (43.5%) | 2 (50.0%) |
| Family history of DM (no., %) | 54/163 74.2% | 11/21 52.4% | 38/51 74.5% | 13/19 68.4% | 19/25 76.0% | 17/20 85.0% | 20/23 87.0% | 4/4 100% |
| DM duration (years; no., %) | 10.9 ± 8.3 0–40 | 5.7 ± 5.1 0–15 c | 7.2 ± 6.6 0–30 | 13.2 ± 9.2 1–34 | 9.6 ± 6.6 0–25 | 12.9 ± 6.9 4–30 | 17.7 ± 8.9 2–40 c | 12.5 ± 11.9 4–30 |
| Treatment duration (mean ± SD) | 3.7 ± 3.1 | 2.0 ± 1.3 | 4.5 ± 3.7 d | 4.5 ± 2.9 | 2.1 ± 1.4 | 2.9 ± 2.4 | 5.1 ± 3.8 | 4.5 ± 2.9 |
| CV comorbidities (no., %) | 152 93.3% | 19 90.5% | 49 96.1% | 17 89.5% | 25 100% | 19 95.0% | 19 82.6% | 4 100% |
| Dyslipidemia (no., %) | 121 74.2% | 14 66.7% | 39 76.5% | 16 84.2% | 18 75.0% | 14 70.0% | 16 69.6% | 4 100% |
| HbA1c (%; mean ± SD, range) | 7.1 ± 1.3 5–16 | 6.0 ± 0.6 5.0–6.8 c | 6.5 ± 0.8 5.5–9.4 | 7.2 ± 0.8 6.0–9.0 | 7.3 ± 0.9 5.5–9.6 | 7.4 ± 0.8 5.8–8.3 | 8.2 ± 2.3 5.2–16.0 c | 6.4 ± 0.8 5.6–7.2 |
| Total Cholesterol (mg/dL; mean ± SD, range) | 160.2 ± 37.5 73–338 | 181.3 ± 47.0 140–338 | 157.2 ± 33.9 97–226 | 153.1 ± 42.4 73–242 | 165.4 ± 36.2 94–226 | 147.8 ± 31.1 89–214 | 166.3 ± 34.9 117–237 | 124.0 ± 36.8 98–150 |
| Triglycerides (mg/dL; mean ± SD, range) | 135.8 ± 69.1 23–388 | 124.3 ± 47.7 37–223 | 128.6 ± 61.3 50–353 | 136.2 ± 79.5 60–388 | 164.2 ± 86.9 52–379 | 139 ± 65.5 51–259 | 127.0 ± 74.2 23–283 | 121.0 ± 36.8 98–150 |
| HDL Cholesterol (mg/dL; mean ± SD, range) | 47.6 ± 12.4 23–105 | 51.5 ± 9.3 33–65 | 48.7 ± 12.0 26–80 | 47.8 ± 19.1 24–105 | 44.8 ± 8.4 31–65 | 45.3 ± 7.5 32–61 | 49.0 ± 14.8 27–81 | 38.5 ± 21.9 23–54 |
| LDL Cholesterol (mg/dL; mean ± SD, range) | 85.5 ± 36.1 14–238 | 114.9 ± 43.2 62.3–238.8 | 87.4 ± 32.9 14.8–157 | 81.3 ± 35.8 18.4–174 | 88.9 ± 39.6 37.8–145.6 | 77.1 ± 28.9 17.4–125 | 97.3 ± 38.3 38.0–178.2 | 61.3 ± 17.4 49–73.6 |
| Total Testosterone (ng/mL; mean ± SD, range) | 4.0 ± 1.8 0.3–11.5 | 4.0 ± 1.6 1.0–7.9 | 4.2 ± 1.7 1.7–8.8 | 4.6 ± 2.8 1.9–11.5 | 3.7 ± 1.7 1.5–7.1 | 3.3 ± 2.1 0.3–5.9 | 3.9 ± 1.5 0.9–5.6 | 2.6 ± 0.2 2.5–2.8 c |
| B, 95%CI, p-Value | |
|---|---|
| Constant IIEF-5 | 24.224, 95%CI from 11.665 to 36.783 |
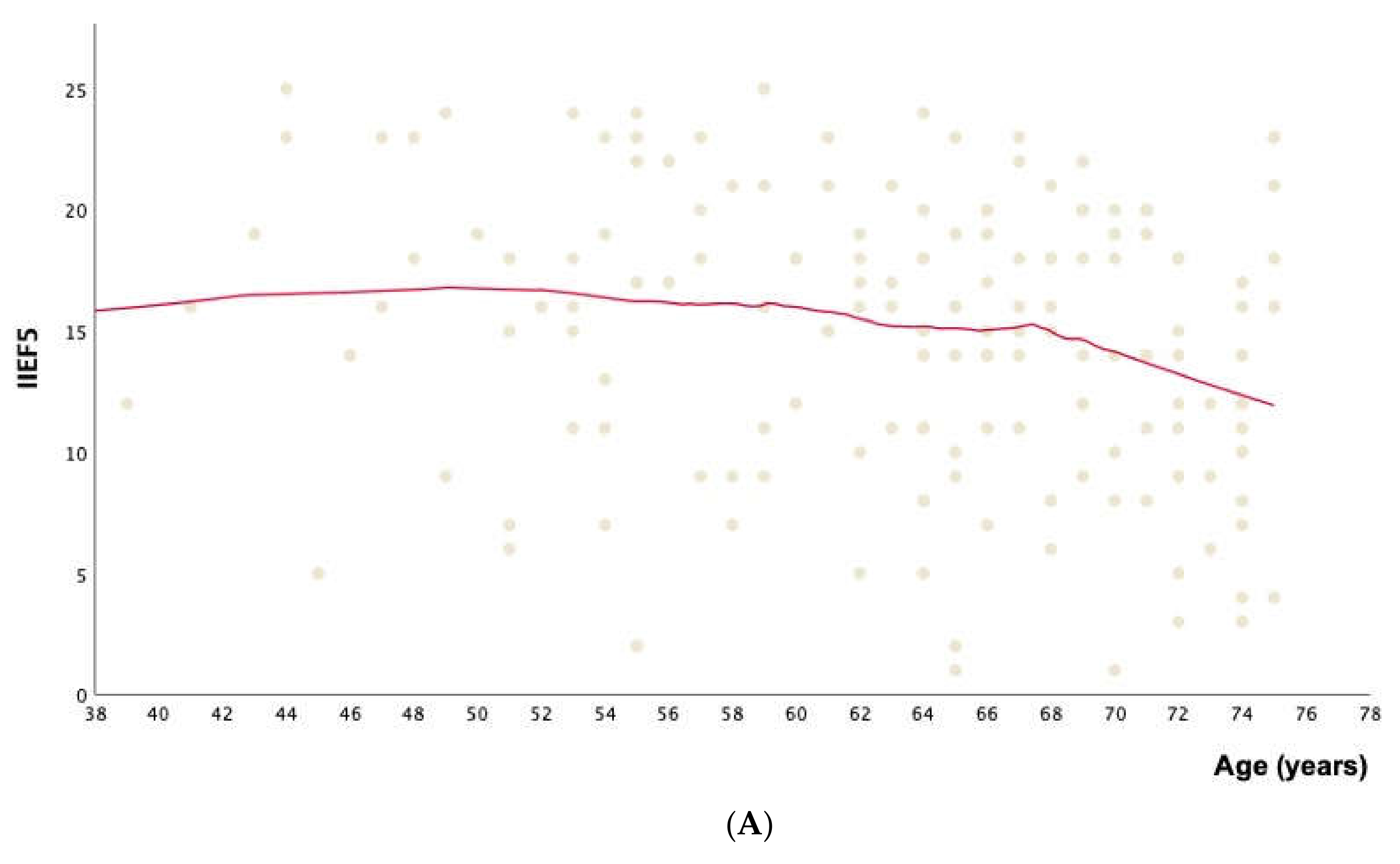
| Age | −0.218, 95%CI from −0.435 to −0.002, p = 0.048 |
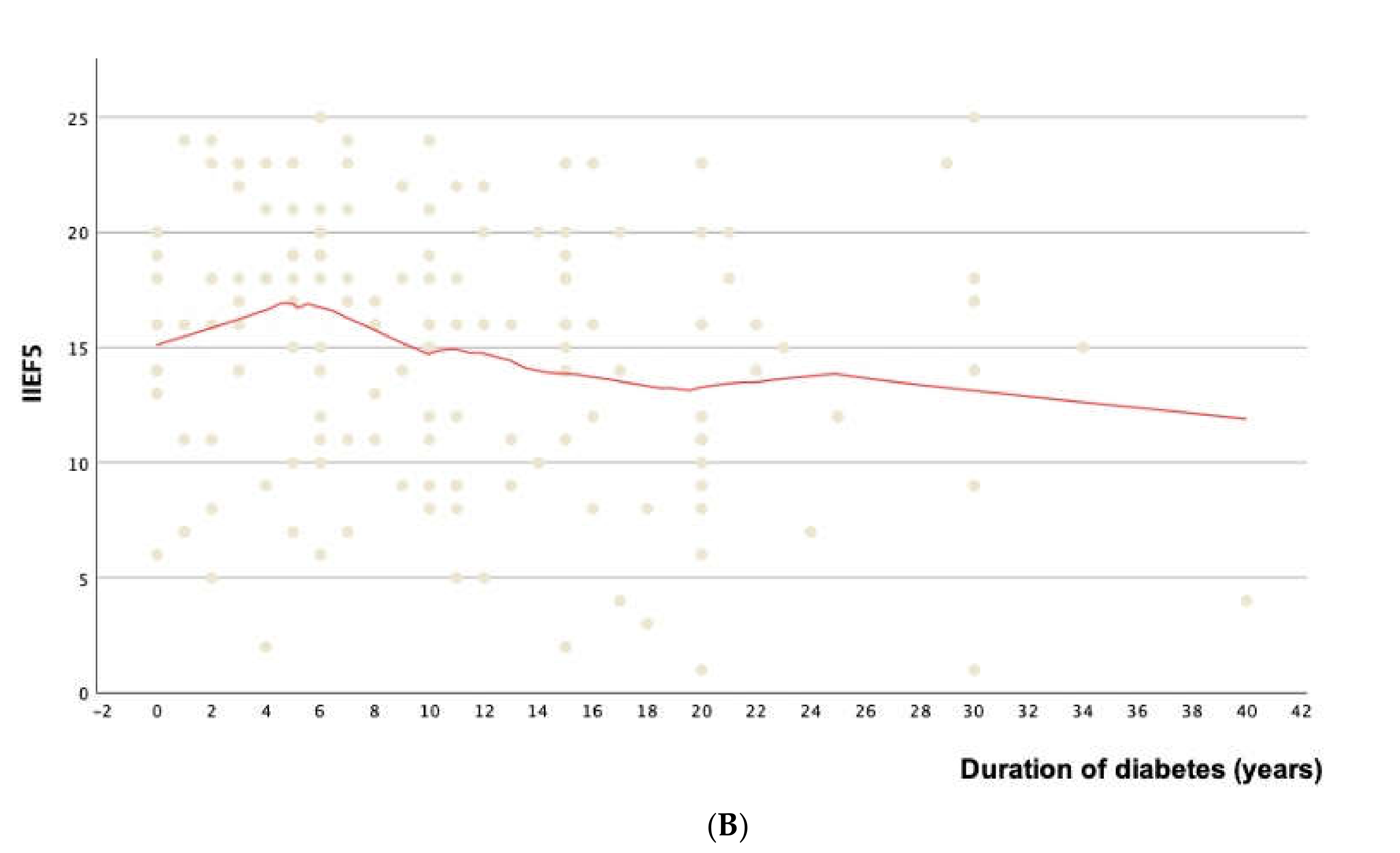
| Duration of DM | +0.091, 95%CI from -0.141 to +0.323, p = 0.413 |
| GLP-1 vs. Insulin | +4.900, 95%CI from +1.256 to +8.544, p = 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2022 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Defeudis, G.; Di Tommaso, A.M.; Di Rosa, C.; Cimadomo, D.; Khazrai, Y.M.; Faggiano, A.; Cincione, R.I.; Napoli, N.; Mazzilli, R. The Role of Antihyperglycemic Drugs and Diet on Erectile Function: Results from a Perspective Study on a Population with Prediabetes and Diabetes. J. Clin. Med. 2022, 11, 3382. https://doi.org/10.3390/jcm11123382
Defeudis G, Di Tommaso AM, Di Rosa C, Cimadomo D, Khazrai YM, Faggiano A, Cincione RI, Napoli N, Mazzilli R. The Role of Antihyperglycemic Drugs and Diet on Erectile Function: Results from a Perspective Study on a Population with Prediabetes and Diabetes. Journal of Clinical Medicine. 2022; 11(12):3382. https://doi.org/10.3390/jcm11123382
Chicago/Turabian StyleDefeudis, Giuseppe, Alfonso Maria Di Tommaso, Claudia Di Rosa, Danilo Cimadomo, Yeganeh Manon Khazrai, Antongiulio Faggiano, Raffaele Ivan Cincione, Nicola Napoli, and Rossella Mazzilli. 2022. "The Role of Antihyperglycemic Drugs and Diet on Erectile Function: Results from a Perspective Study on a Population with Prediabetes and Diabetes" Journal of Clinical Medicine 11, no. 12: 3382. https://doi.org/10.3390/jcm11123382
APA StyleDefeudis, G., Di Tommaso, A. M., Di Rosa, C., Cimadomo, D., Khazrai, Y. M., Faggiano, A., Cincione, R. I., Napoli, N., & Mazzilli, R. (2022). The Role of Antihyperglycemic Drugs and Diet on Erectile Function: Results from a Perspective Study on a Population with Prediabetes and Diabetes. Journal of Clinical Medicine, 11(12), 3382. https://doi.org/10.3390/jcm11123382