
Evaluating the 0–10 Point Pain Scale on Adolescent Opioid Use in US Emergency Departments

 , , ,
, , , 
 ,
,
Abstract
:1. Introduction
2. Methods
2.1. Study Design and Setting
2.2. Patient and Public Involvement
2.3. Selection of Population
2.4. Variables
2.5. Pain Score Measurement
2.6. Statistical Analysis
3. Results
3.1. Participants
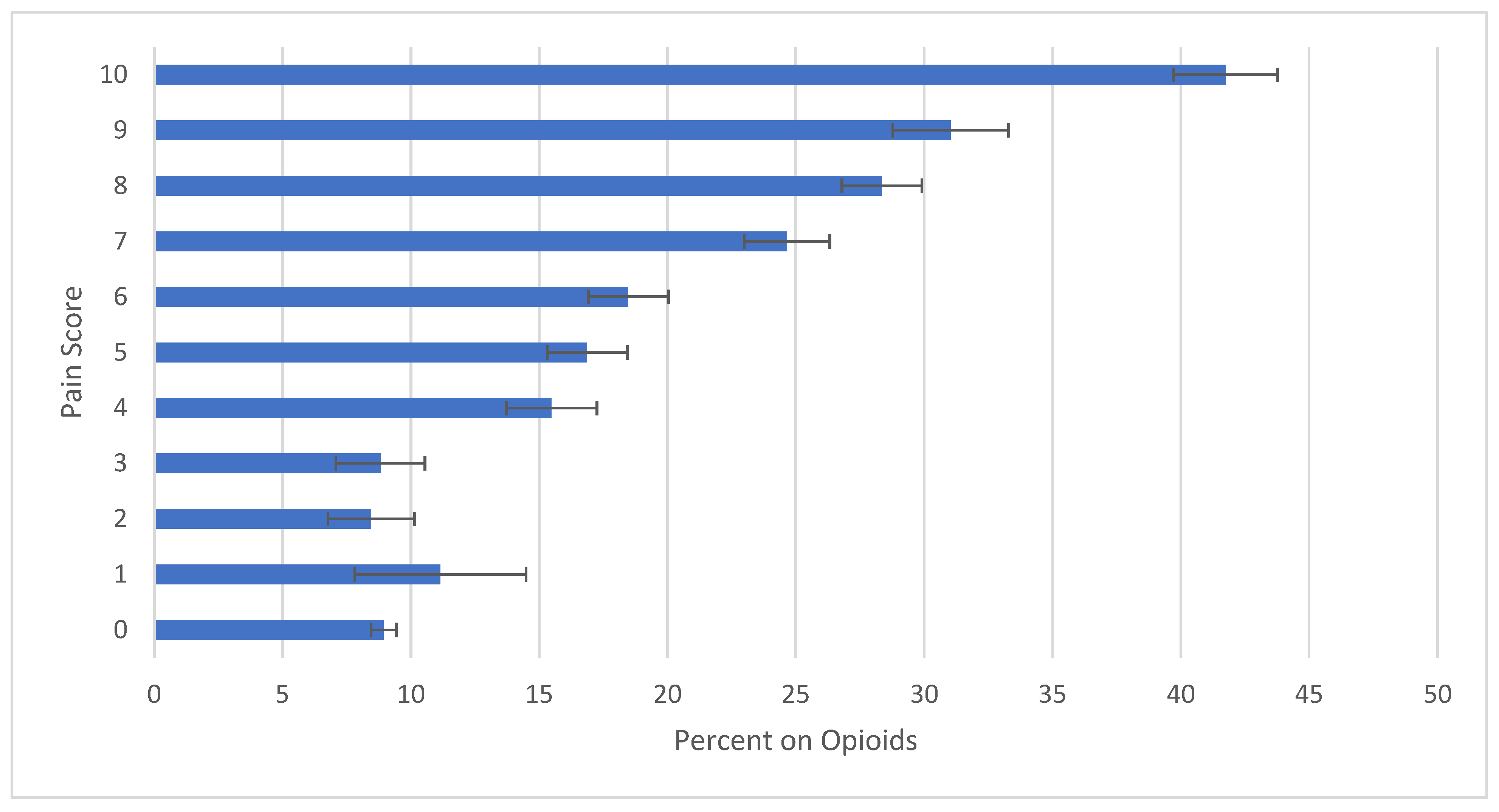
3.2. Pain Scale Alone
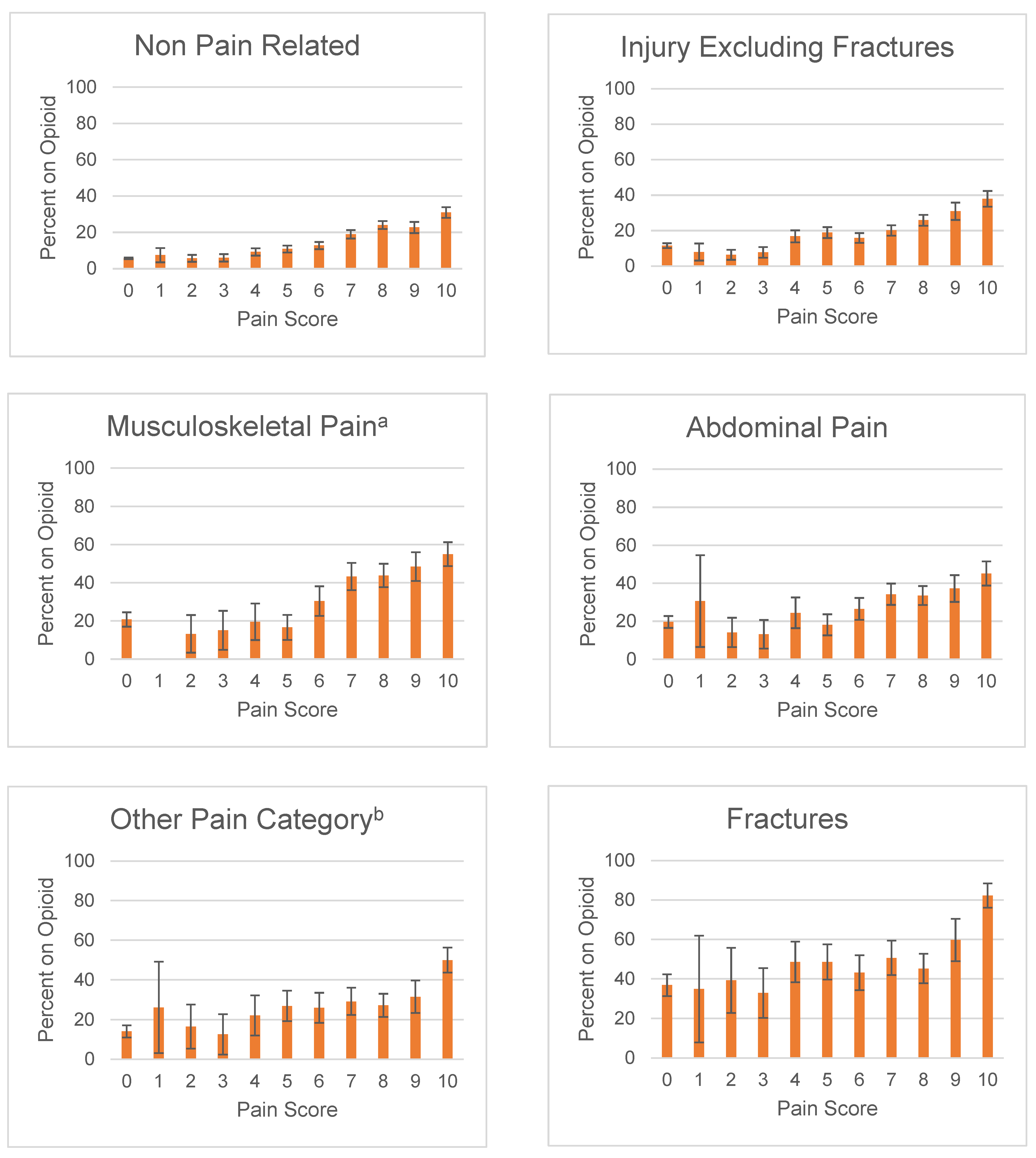
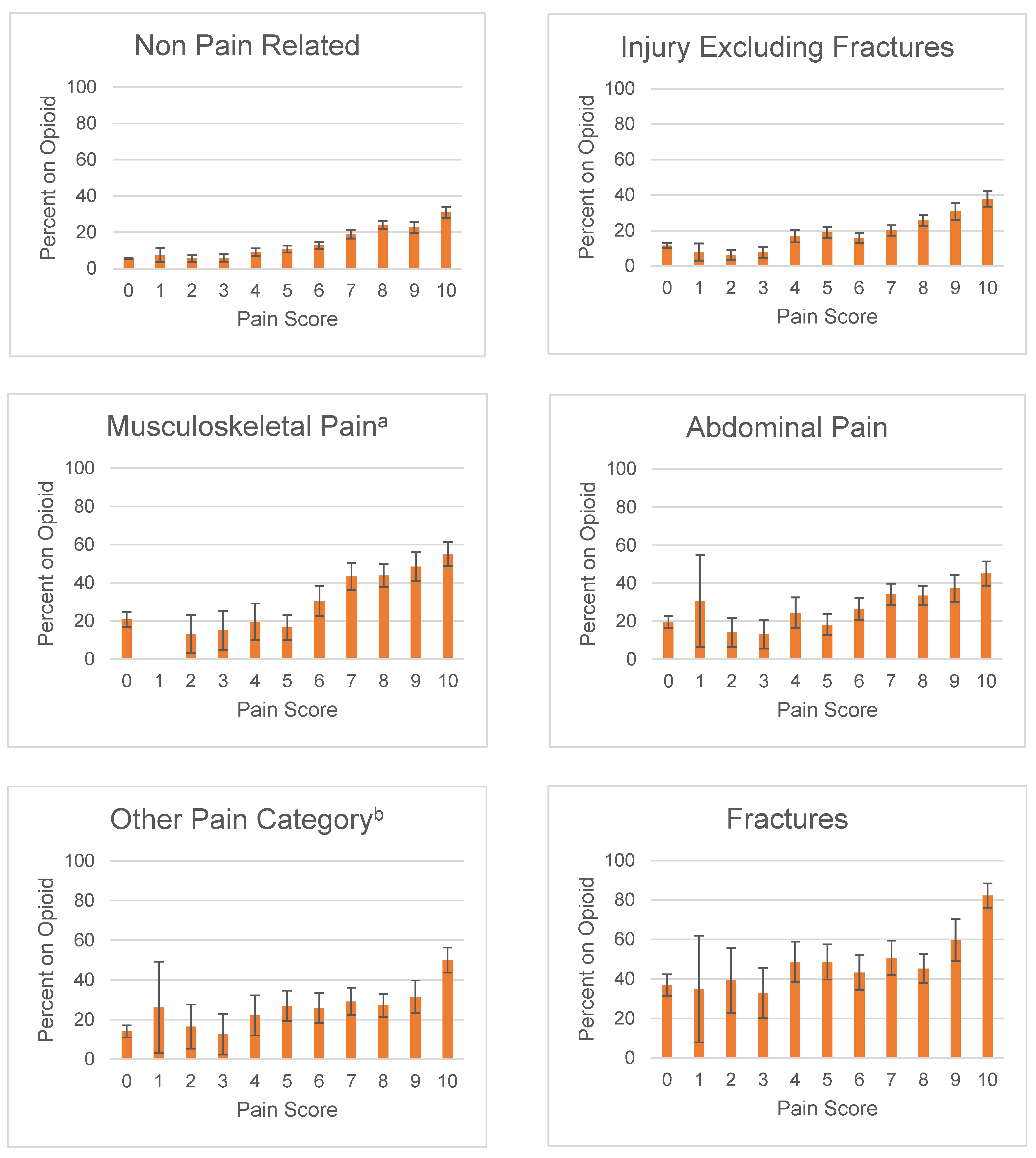
3.3. Diagnosis
3.3.1. Fractures
3.3.2. Musculoskeletal pain
3.3.3. Abdominal pain
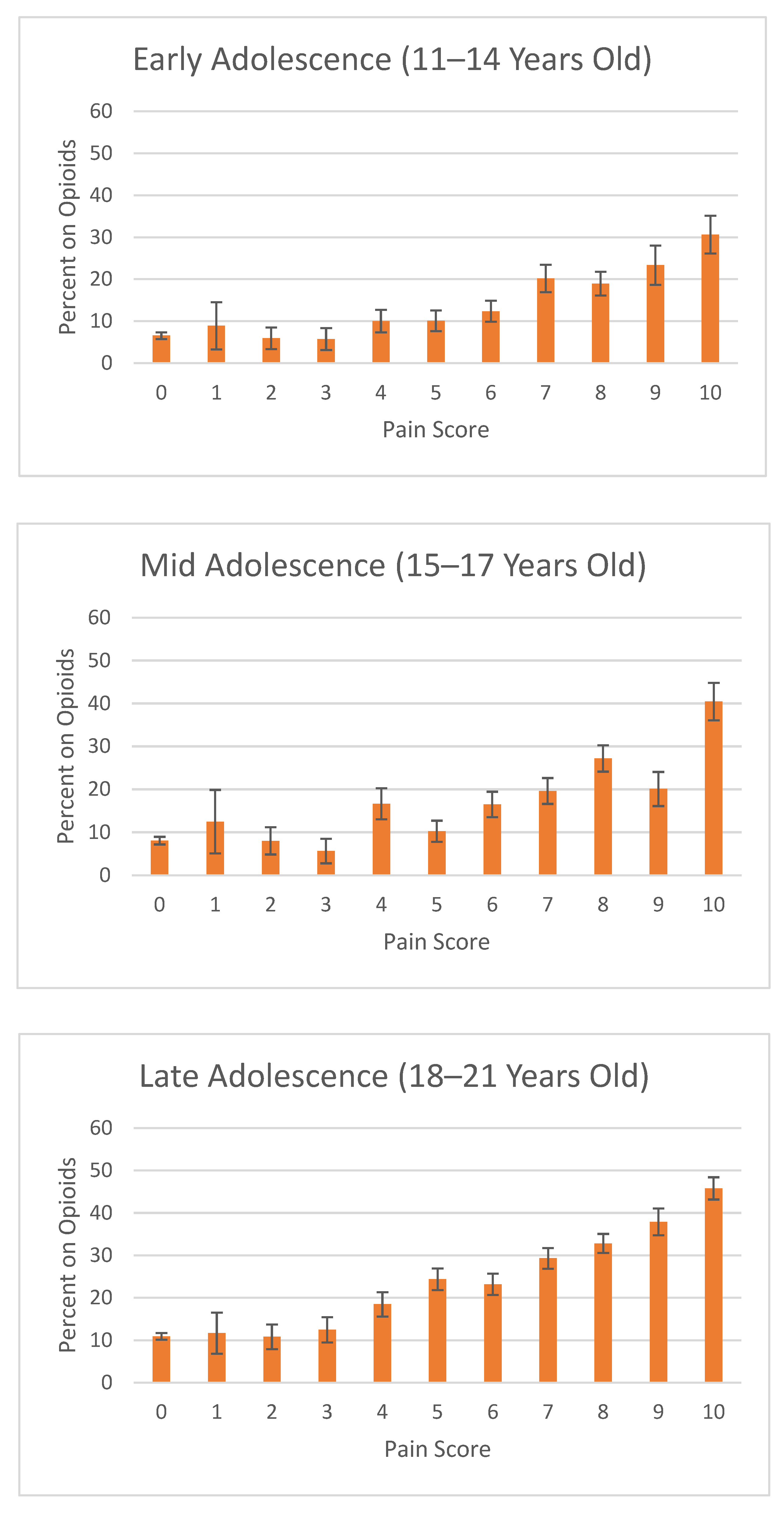
3.4. Patient Age
3.5. Patient Sex Differences
3.6. Multivariate Analyses: Logistic Regression
4. Discussion
5. Limitations
6. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- CDC. National Hospital Ambulatory Medical Care Survey: 2015 Emergency Department Summary Tables. 2018. Available online: https://www.cdc.gov/nchs/data/nhamcs/web_tables/2015_ed_web_tables.pdf (accessed on 2 December 2021).
- CDC. National Center for Health Statistics—Health, United States, 2019—Data Finder. 2019. Available online: https://www.cdc.gov/nchs/hus/contents2019.htm?search=Emergency_department_visits (accessed on 2 December 2021).
- California, M.B.O. Guidelines for Prescribing Controlled Substances for Pain; Medical Board of California: Sacramento, CA, USA, 2014.
- Dowell, D.; Haegerich, T.M.; Chou, R. CDC Guideline for Prescribing Opioids for Chronic Pain—United States, 2016. MMWR Recomm. Rep. 2016, 65, 1–49. Available online: https://www.cdc.gov/mmwr/volumes/65/rr/rr6501e1.htm (accessed on 10 June 2020). [CrossRef]
- World Health Organization. WHO Guidelines on the Pharmacological Treatment of Persisting Pain in Children with Medical Illnesses; WHO: Geneva, Switzerland, 2012. [Google Scholar]
- Cravero, J.P.; Agarwal, R.; Berde, C.; Birmingham, P.; Coté, C.J.; Galinkin, J.; Isaac, L.; Kost-Byerly, S.; Krodel, D.; Maxwell, L.; et al. The Society for Pediatric Anesthesia recommendations for the use of opioids in children during the perioperative period. Paediatr. Anaesth. 2019, 29, 547–571. [Google Scholar] [CrossRef] [Green Version]
- Kroenke, K.; Alford, D.P.; Argoff, C.; Canlas, B.; Covington, E.; Frank, J.W.; Haake, K.J.; Hanling, S.; Hooten, W.M.; Kertesz, S.G.; et al. Challenges with Implementing the Centers for Disease Control and Prevention Opioid Guideline: A Consensus Panel Report. Pain Med. 2019, 20, 724–735. [Google Scholar] [CrossRef]
- Twycross, A.; Voepel-Lewis, T.; Vincent, C.; Franck, L.S.; von Baeyer, C.L. A debate on the proposition that self-report is the gold standard in assessment of pediatric pain intensity. Clin. J. Pain 2015, 31, 707–712. [Google Scholar] [CrossRef] [PubMed]
- Stanford, E.A.; Chambers, C.T.; Craig, K.D. The role of developmental factors in predicting young children’s use of a self-report scale for pain. Pain 2006, 120, 16–23. [Google Scholar] [CrossRef] [PubMed]
- Fowler-Kerry, S.; Lander, J. Assessment of sex differences in children’s and adolescents’ self-reported pain from venipuncture. J. Pediatr. Psychol. 1991, 16, 783–793. [Google Scholar] [CrossRef] [PubMed]
- Fortier, M.A.; Anderson, C.T.; Kain, Z.N. Ethnicity matters in the assessment and treatment of children’s pain. Pediatrics 2009, 124, 378–380. [Google Scholar] [CrossRef]
- Miech, R.; Johnston, L.; O’Malley, P.M.; Keyes, K.M.; Heard, K. Prescription Opioids in Adolescence and Future Opioid Misuse. Pediatrics 2015, 136, e1169–e1177. [Google Scholar] [CrossRef] [Green Version]
- Schroeder, A.R.; Dehghan, M.; Newman, T.B.; Bentley, J.P.; Park, K.T. Association of Opioid Prescriptions From Dental Clinicians for US Adolescents and Young Adults With Subsequent Opioid Use and Abuse. JAMA Intern. Med. 2019, 179, 145–152. [Google Scholar] [CrossRef]
- Yacisin, K. QuickStats: Percentage of Emergency Department Visits that Had an Opioid Ordered or Prescribed, by Age Group—National Hospital Ambulatory Medical Care Survey, United States, 2006–2015. MMWR Morb. Mortal Wkly Rep. 2018, 67, 344. Available online: https://www.cdc.gov/mmwr/volumes/67/wr/mm6711a8.htm (accessed on 10 June 2020).
- Chakravarthy, B.; Shah, S.; Lotfipour, S. Prescription drug monitoring programs and other interventions to combat prescription opioid abuse. West J. Emerg. Med. 2012, 13, 422–425. [Google Scholar] [CrossRef]
- Tamayo-Sarver, J.H.; Dawson, N.V.; Cydulka, R.K.; Wigton, R.S.; Baker, D.W. Variability in emergency physician decision making about prescribing opioid analgesics. Ann. Emerg. Med. 2004, 43, 483–493. [Google Scholar] [CrossRef] [PubMed]
- Hoppe, J.A.; Nelson, L.S.; Perrone, J.; Weiner, S.G.; Rathlev, N.K.; Sanchez, L.D.; Babineau, M.; Griggs, C.A.; Mitchell, P.M.; Ma, J.; et al. Opioid Prescribing in a Cross Section of US Emergency Departments. Ann. Emerg. Med. 2015, 66, 253–259.e1. [Google Scholar] [CrossRef] [Green Version]
- Menchine, M.; Lam, C.N.; Arora, S. Prescription Opioid Use in General and Pediatric Emergency Departments. Pediatrics 2019, 144. [Google Scholar] [CrossRef] [PubMed]
- Johnson Yackey, K. Ouch! Factors that contribute to emergency department pediatric pain control. In AAP Experience; AAP: Orlando, FL, USA, 2013. [Google Scholar]
- Drendel, A.L.; Brousseau, D.C.; Gorelick, M.H. Pain Assessment for Pediatric Patients in the Emergency Department. Pediatrics 2006, 117, 1511. [Google Scholar] [CrossRef] [PubMed]
- US Emergency Department. Nhamcs Micro-Data File Documentation. In The National Bureau of Economic Research; US Emergency Department: Washington, DC, USA, 2010; p. 284. [Google Scholar]
- Hardin, A.P.; Hackell, J.M. Age Limit of Pediatrics. Pediatrics 2017, 140, e20172151. [Google Scholar] [CrossRef] [Green Version]
- National Center for Health Statistics (US). The Ambulatory Care Drug Database System. 2018. Available online: https://www2.cdc.gov/drugs/applicationnav1.asp (accessed on 5 July 2018).
- US Emergency Department. 2006 Nhamcs Micro-Data File Documentation. In The National Bureau of Economic Research; US Emergency Department: Washington, DC, USA, 2006. [Google Scholar]
- National Center for Health Statistics (US). Ambulatory Health Care Data: NAMCS and NHAMCS Description. 2018. Available online: http://www.cdc.gov/nchs/ahcd/ahcd_questionnaires.htm (accessed on 10 June 2020).
- Serlin, R.C.; Mendoza, T.R.; Nakamura, Y.; Edwards, K.R.; Cleeland, C.S. When is cancer pain mild, moderate or severe? Grading pain severity by its interference with function. Pain 1995, 61, 277–284. [Google Scholar] [PubMed]
- Tsze, D.S.; Hirschfeld, G.; Dayan, P.S.; Bulloch, B.; von Baeyer, C.L. Defining No Pain, Mild, Moderate, and Severe Pain Based on the Faces Pain Scale–Revised and Color Analog Scale in Children With Acute Pain. Pediatric Emerg. Care 2018, 34, 537–544. [Google Scholar] [CrossRef] [PubMed]
- McConahay, T.; Bryson, M.; Bulloch, B. Defining mild, moderate, and severe pain by using the color analogue scale with children presenting to a pediatric emergency department. Acad. Emerg. Med. 2006, 13, 341–344. [Google Scholar] [CrossRef]
- NHAMCS. Micro-Data File Documentation. 2015. Available online: https://data.nber.org/nhamcs/docs/nhamcsed2015.pdf (accessed on 29 May 2020).
- Weng, Y.M.; Chang, Y.C.; Lin, Y.J. Triage pain scales cannot predict analgesia provision to pediatric patients with long-bone fracture. Am. J. Emerg. Med. 2010, 28, 412–417. [Google Scholar] [CrossRef]
- Kaplan, C.P.; Sison, C.; Platt, S.L. Does a pain scale improve pain assessment in the pediatric emergency department? Pediatr. Emerg. Care 2008, 24, 605–608. [Google Scholar] [CrossRef]
- Jadav, M.A.; Lloyd, G.; McLauchlan, C.; Hayes, C. Routine pain scoring does not improve analgesia provision for children in the emergency department. Emerg. Med. J. 2009, 26, 695–697. [Google Scholar] [CrossRef] [PubMed]
- Alexander, J.; Manno, M. Underuse of analgesia in very young pediatric patients with isolated painful injuries. Ann. Emerg. Med. 2003, 41, 617–622. [Google Scholar] [CrossRef] [PubMed]
- Kircher, J.; Drendel, A.L.; Newton, A.S.; Plint, A.C.; Vandermeer, B.; Dulai, S.; Ali, S. Acute pediatric musculoskeletal pain management in North America: A practice variation survey. Clin. Pediatr. 2014, 53, 1326–1335. [Google Scholar] [CrossRef]
- Committee on Psychosocial Aspects of Child and Family Health. The assessment and management of acute pain in infants, children, and adolescents. Pediatrics 2001, 108, 793–797. [Google Scholar]

{kind=link}
{kind=link}
{kind=link}
| Variable | Total Patients | Percent on Opioid (CI95) |
|---|---|---|
| Sex | ||
| Female | 92,550,318 | 16.8% (17.3–16.2%) |
| Male | 69,965,625 | 18.1% (18.8–17.5%) |
| Race/Ethnicity | ||
| Black | 39,255,551 | 14.1% (14.8–13.3%) |
| Hispanic | 29,956,070 | 15.7% (16.6–14.7%) |
| Other | 4,179,126 | 18.3% (20.7–15.9%) |
| White | 89,125,196 | 19.3% (19.9–18.7%) |
| Age | ||
| 11–14 | 42,416,187 | 11.3% (12.0–10.7%) |
| 15–17 | 41,730,020 | 14.7% (15.5–13.9%) |
| 18–21 | 78,369,736 | 22% (22.7–21.4%) |
| MSA | ||
| Metropolitan area | 120,279,731 | 17.9% (18.4–17.4%) |
| Non-metropolitan area | 24,884,524 | 15.5% (16.6–14.4%) |
| Unknown | 17,351,688 | 16.5% (17.6–15.3%) |
| Episode Of Care | ||
| Initial visit to this ED | 144,282,632 | 17.3% (17.7–16.8%) |
| Follow-up visit to this ED | 7,330,229 | 20.9% (22.9–18.9%) |
| Unknown/Missing Data | 10,903,082 | 15.9% (17.4–14.4%) |
| Time Interval | ||
| 2008–2012 | 73,585,030 | 20.9% (21.5–20.3%) |
| 2013–2017 | 88,930,913 | 14.4% (15.0–13.8%) |
| Prolonged Visit | ||
| Not Prolonged | 109,946,374 | 18.9% (19.4–18.4%) |
| Prolonged Visit | 8,829,988 | 25.6% (27.5–23.8%) |
| Unknown/Missing Data | 43,739,581 | 11.8% (12.6–11.0%) |
| Odds Ratio (CI95) | ||
|---|---|---|
| (Intercept) | 0.014 (0.009–0.023) | |
| Ethnicity | Other | |
| Black | 0.775 (0.550–1.093) | |
| Hispanic | 0.992 (0.713–1.379) | |
| White | 1.241 (0.904–1.703) | |
| Diagnosis | Non Pain Related | |
| Abdominal Pain | 1.98 (1.650–2.375) * | |
| Fractures | 6.653 (5.289–8.369) * | |
| Injury excluding fracture | 1.391 (1.211–1.598) * | |
| Musculoskeletal Pain | 2.573 (2.105–3.144) * | |
| Other Pain Category | 1.845 (1.498–2.271) * | |
| Sex | Male | |
| Female | 0.811 (0.716–0.918) | |
| Payment Method | Private Insurance | |
| Medicaid, CHIP, State | 0.760 (0.668–0.865) | |
| Other Payment Method | 0.832 (0.685–1.01) | |
| Self-Pay | 1.058 (0.895–1.25) | |
| Adolescent Age | 11–14 | |
| 15–17 | 1.424 (1.203–1.687) * | |
| 18–21 | 2.399 (2.059–2.795) * | |
| Prolonged ED visit | Not Prolonged | |
| Prolonged | 1.700 (1.405–2.057) * | |
| Missing Data | 0.647 (0.552–0.759) | |
| Region | Northeast | |
| Midwest | 1.674 (1.353–2.072) * | |
| South | 2.076 (1.723–2.501) * | |
| West | 2.613 (2.089–3.267) * | |
| Pain Scale | PAINSCALE | 1.253 (1.224–1.283) * |
| Episode of Care | Initial visit to this ED | |
| Follow-up visit to this ED | 1.408 (1.120–1.771) * | |
| Unknown/Missing Data | 1.094 (0.807–1.485) | |
| Metropolitan Area | Non Metropolitan Area | |
| Metropolitan Area | 1.237 (1.003–1.526) * | |
| Unknown | 0.936 (0.72–1.217) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Phan, M.T.; Tomaszewski, D.M.; Arbuckle, C.; Yang, S.; Jenkins, B.; Fortier, M.A.; Heyming, T.; Linstead, E.; Donaldson, C.; Kain, Z. Evaluating the 0–10 Point Pain Scale on Adolescent Opioid Use in US Emergency Departments. J. Clin. Med. 2022, 11, 38. https://doi.org/10.3390/jcm11010038
Phan MT, Tomaszewski DM, Arbuckle C, Yang S, Jenkins B, Fortier MA, Heyming T, Linstead E, Donaldson C, Kain Z. Evaluating the 0–10 Point Pain Scale on Adolescent Opioid Use in US Emergency Departments. Journal of Clinical Medicine. 2022; 11(1):38. https://doi.org/10.3390/jcm11010038
Chicago/Turabian StylePhan, Michael T., Daniel M. Tomaszewski, Cody Arbuckle, Sun Yang, Brooke Jenkins, Michelle A. Fortier, Theodore Heyming, Erik Linstead, Candice Donaldson, and Zeev Kain. 2022. "Evaluating the 0–10 Point Pain Scale on Adolescent Opioid Use in US Emergency Departments" Journal of Clinical Medicine 11, no. 1: 38. https://doi.org/10.3390/jcm11010038
APA StylePhan, M. T., Tomaszewski, D. M., Arbuckle, C., Yang, S., Jenkins, B., Fortier, M. A., Heyming, T., Linstead, E., Donaldson, C., & Kain, Z. (2022). Evaluating the 0–10 Point Pain Scale on Adolescent Opioid Use in US Emergency Departments. Journal of Clinical Medicine, 11(1), 38. https://doi.org/10.3390/jcm11010038