
Coronary Flow Velocity Reserve Using Dobutamine Test for Noninvasive Functional Assessment of Myocardial Bridging

 , , , ,
, , , ,  , , ,
, , ,
Abstract
:1. Introduction
2. Methods
2.1. Study Population
2.2. Study Protocol
2.3. Exercise Stress-Echocardiography
2.4. Quantitative Coronary Angiography
2.5. Coronary Flow Velocity Reserve Measurements by Transthoracic Doppler Echocardiography
2.6. Statistical Analysis
3. Results
3.1. Coronary Physiological Parameters during Dobutamine Provocation: Relation to Stress-Induced VMA
3.2. Diagnostic Value of Coronary Flow Velocity Reserve with Stress-Induced VMA as the Reference Standard
3.3. Coronary Physiological Parameters during Dobutamine Provocation: Relation to Angiographic Data
4. Discussion
Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
Abbreviations
| CFV | coronary flow velocity |
| CFVR | coronary flow velocity reserve |
| DOB | dobutamine |
| DS | diameter stenosis |
| MB | myocardial bridging |
| MLD | minimal luminal diameter |
| LAD | left anterior descending coronary artery |
| SE | stress-echocardiography |
| QCA | quantitative coronary angiography |
| RD | reference diameter |
| WMA | wall-motion abnormalities |
References
- Hozumi, T.; Yoshida, K.; Ogata, Y.; Akasaka, T.; Asami, Y.; Takagi, T.; Morioka, S. Noninvasive assessment of significant left anterior descending coronary artery stenosis by coronary flow velocity reserve with transthoracic color Doppler. Circulation 1998, 97, 1557–1562. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Hozumi, T.; Yoshida, K.; Akasaka, T.; Asami, Y.; Ogata, Y.; Takagi, T.; Kaji, S.; Kawamoto, T.; Ueda, Y.; Morioka, S. Noninvasive assessment of coronary flow velocity and coronary flow velocity reserve in the left anterior descending coronary artery by Doppler echocardiography: Comparison with invasive technique. J. Am. Coll. Cardiol. 1998, 32, 1251–1259. [Google Scholar] [CrossRef] [Green Version]
- Caiati, C.; Montaldo, C.; Zedda, N.; Bina, A.; Ilicetol, S. New noninvasive method for coronary flow reserve assessment: Contrast-enhanced transthoracic second-harmonic echo-Doppler. Circulation 1999, 99, 771–778. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Caiati, C.; Zedda, N.; Montaldo, C.; Montisci, R.; Iliceto, S. Contrast-enhanced transthoracic second harmonic echo Doppler with adenosine: A noninvasive, rapid and effective method for coronary flow reserve assessment. J. Am. Coll Cardiol. 1999, 34, 122–130. [Google Scholar] [CrossRef]
- Caiati, C.; Montaldo, C.; Zedda, N.; Montisci, R.; Ruscazio, M.; Lai, G.; Cadeddu, M.; Meloni, L.; Iliceto, S. Validation of a new noninvasive method (contrast-enhanced transthoracic second harmonic echo Doppler) for the evaluation of coronary flow reserve: Comparison with intracoronary Doppler flow wire. J. Am. Coll. Cardiol. 1999, 34, 1193–1200. [Google Scholar] [CrossRef]
- Daimon, M.; Watanabe, H.; Yamagishi, H.; Muro, T.; Akioka, K.; Hirata, K.; Takeuchi, K.; Yoshikawa, J. Physiologic Assessment of Coronary Artery Stenosis by Coronary Flow Reserve Measurements With Transthoracic Doppler Echocardiography: Comparison With Exercise Thallium-201Single-Photon Emission Computed Tomography. J. Am. Coll. Cardiol. 2001, 37, 1310–1315. [Google Scholar] [CrossRef]
- Picano, E. Stress Echocardiography, 6th ed.; Springer: Berlin/Heidelberg, Germany, 2015. [Google Scholar]
- Lim, H.E.; Shim, W.J.; Rhee, H.; Kim, S.M.; Hwang, G.S.; Kim, Y.H.; Seo, H.S.; Oh, D.J.; Ro, Y.M. Assessment of coronary flow reserve with transthoracic Doppler echocardiography: Comparison among adenosine, standard-dose dipyridamole, and high-dose dipyridamole. J. Am. Soc. Echocardiogr. 2000, 13, 264–270. [Google Scholar] [CrossRef] [PubMed]
- Hakeem, A.; Cilingiroglu, M.; Leesar, M.A. Hemodynamic and intravascular ultrasound assessment of myocardial bridging: Fractional flow reserve paradox with dobutamine versus adenosine. Catheter. Cardiovasc. Interv. 2010, 75, 229–236. [Google Scholar] [CrossRef] [PubMed]
- Escaned, J.; Cortés, J.; Flores, A.; Goicolea, J.; Alfonso, F.; Hernández, R.; Fernández-Ortiz, A.; Sabaté, M.; Bañuelos, C.; Macaya, C. Importance of diastolic fractional flow reserve and dobutamine challenge in physiologic assessment of myocardial bridging. J. Am. Coll. Cardiol. 2003, 42, 226–233. [Google Scholar] [CrossRef] [Green Version]
- Uusitalo, V.; Saraste, A.; Pietilä, M.; Kajander, S.; Bax, J.J.; Knuuti, J. The Functional effects of intramural course of coronary arteries and its relation to coronary atherosclerosis. JACC Cardiovasc. Imaging 2015, 8, 697–704. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Tarantini, G.; Barioli, A.; Fovino, L.N.; Fraccaro, C.; Masiero, G.; Iliceto, S.; Napodano, M. Unmasking Myocardial Bridge–Related Ischemia by Intracoronary Functional Evaluation. Circ. Cardiovasc. Interv. 2018, 11, e006247. [Google Scholar] [CrossRef]
- Aleksandric, S.; Djordjevic-Dikic, A.; Beleslin, B.; Parapid, B.; Teofilovski-Parapid, G.; Stepanovic, J.; Simic, D.; Nedeljkovic, I.; Petrovic, M.; Dobric, M.; et al. Noninvasive assessment of myocardial bridging by coronary flow velocity reserve with transthoracic Doppler echocardiography: Vasodilator vs. inotropic stimulation. Int. J. Cardiol. 2016, 225, 37–45. [Google Scholar] [CrossRef]
- Aleksandric, S.B.; Djordjevic-Dikic, A.D.; Dobric, M.R.; Giga, V.L.; Soldatovic, I.A.; Vukcevic, V.; Tomasevic, M.V.; Stojkovic, S.M.; Orlic, D.N.; Saponjski, J.D.; et al. Functional Assessment of Myocardial Bridging With Conventional and Diastolic Fractional Flow Reserve: Vasodilator Versus Inotropic Provocation. J. Am. Heart Assoc. 2021, 10, e020597. [Google Scholar] [CrossRef]
- Tarantini, G.; Migliore, F.; Cademartiri, F.; Fraccaro, C.; Iliceto, S. Left anterior descending artery myocardial bridging: A clinical approach. J. Am. Coll. Cardiol. 2016, 68, 2887–2899. [Google Scholar] [CrossRef]
- Corban, M.T.; Hung, O.Y.; Eshtehardi, P.; Rasoul-Arzrumly, E.; McDaniel, M.; Mekonnen, G.; Timmins, L.H.; Lutz, J.; Guyton, R.A.; Samady, H. Myocardial bridging: Contemporary understanding of pathophysiology with implications for diagnostic and therapeutic strategies. J. Am. Coll. Cardiol. 2014, 63, 2346–2355. [Google Scholar] [CrossRef] [Green Version]
- Alegria, J.R.; Herrmann, J.; Holmes, D.R., Jr.; Lerman, A.; Rihal, C.S. Myocardial bridging. Eur. Heart J. 2005, 26, 1159–1168. [Google Scholar] [CrossRef]
- Bourassa, M.G.; Butnaru, A.; Lesperance, J.; Tardif, J.C. Symptomatic myocardial bridges: Overview of ischemic mechanisms and current diagnostic and treatment strategies. J. Am. Coll. Cardiol. 2003, 41, 351–359. [Google Scholar] [CrossRef] [Green Version]
- Stoddard, F.M.; Prince, R.C.; Morris, T. Coronary flow reserve assessment by dobutamine transesophageal Doppler echocardiography. J. Am. Coll. Cardiol. 1995, 25, 325–332. [Google Scholar] [CrossRef] [Green Version]
- Ahmari, S.A.; Modesto, K.; Bunch, J.; Stussy, V.; Dichak, A.; Seward, J.; Pellikka, P.; Chandrasekaran, K. Doppler derived coronary flow reserve during dobutamine stress echocardiography further improves detection of myocardial ischemia. Eur. J. Echocardiography. 2006, 7, 134–140. [Google Scholar] [CrossRef]
- Takeuchi, M.; Miyazaki, C.; Yoshitani, H.; Otani, S.; Sakamoto, K.; Yoshikawa, J. Assessment of coronary flow velocity with transthoracic Doppler echocardiography during dobutamine stress echocardiography. J. Am. Coll. Cardiol. 2001, 38, 117–123. [Google Scholar] [CrossRef] [Green Version]
- Meimoun, P.; Benali, T.; Sayah, S.; Luycx-Bore, A.; Boulanger, J.; Zemir, H.; Tribouilloy, C. Evaluation of left anterior descending coronary artery stenosis of intermediate severity using transthoracic coronary flow reserve and dobutamine stress echocardiography. J. Am. Soc. Echocardiogr. 2005, 18, 1233–1240. [Google Scholar] [CrossRef] [PubMed]
- Meimoun, P.; Sayah, S.; Tcheuffa, J.C.; Benali, T.; Luycx-Bore, A.; Levy, F.; Tribouilloy, C. Transthoracic coronary flow velocity reserve assessment: Comparison between adenosine and dobutamine. J. Am. Soc. Echocardiogr. 2006, 19, 1220–1228. [Google Scholar] [CrossRef]
- Bartunek, J.; Wijns, W.; Heyndrickx, G.R.; de Bruyne, B. Effects of dobutamine on coronary stenosis physiology and morphology: Comparison with intracoronary adenosine. Circulation 1999, 100, 243–249. [Google Scholar] [CrossRef]
- Skopicki, H.A.; Abraham, S.A.; Picard, M.H.; Alpert, N.M.; Fischman, A.J.; Gewirtz, H. Effects of dobutamine at maximally tolerated dose on myocardial blood flow in humans with ischemic heart disease. Circulation 1997, 96, 3346–3352. [Google Scholar] [CrossRef]
- Severi, S.; Underwood, R.; Mohiaddin, R.H.; Boyd, H.; Paterni, M.; Camici, P.G. Dobutamine stress: Effects on regional myocardial blood flow and wall motion. J. Am. Coll. Cardiol. 1995, 26, 1187–1195. [Google Scholar] [CrossRef] [Green Version]
- Beleslin, B.D.; Ostojic, M.; Stepanovic, J.; Djordjevic-Dikic, A.; Stojkovic, S.; Nedeljkovic, M.; Stankovic, G.; Petrasinovic, Z.; Gojkovic, L.; Vasiljevic-Pokrajcic, Z. Stress-echocardiography in the detection of myocardial ischemia. Head-to-head comparison of exercise, dobutamine, and dipyridamole tests. Circulation 1994, 90, 1168–1176. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Pellikka, P.A.; Arruda-Olson, A.; Chaudhry, F.A.; Chen, M.H.; Marshall, J.E.; Porter, T.R.; Sawada, S.G. Guidelines for Performance, Interpretation, and Application of Stress Echocardiography in Ischemic Heart Disease: From the American Society of Echocardiography. J. Am. Soc. Echocardiogr. 2020, 33, 1–41.e8. [Google Scholar] [CrossRef] [Green Version]
- Lang, R.M.; Badano, L.P.; Mor-Avi, V.; Afilalo, J.; Armstrong, A.; Ernande, L.; Flachskampf, F.A.; Foster, E.; Goldstein, S.A.; Kuznetsova, T.; et al. Recommendations for cardiac chamber quantification by echocardiography in adults: An update from the American Society of Echocardiography and the European Association of Cardiovascular Imaging. J. Am. Soc. Echocardiogr. 2015, 28, 1–39. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, E.R.; Klues, H.G.; vom Dahl, J.; Klein, I.; Krebs, W.; Hanrath, P. Functional, angiographic and intracoronary Doppler flow characteristics in symptomatic patients with myocardial bridging: Effect of short-term intravenous beta-blocker medication. J. Am. Coll. Cardiol. 1996, 27, 1637–1645. [Google Scholar] [CrossRef] [Green Version]
- Forte, E.H.; Rousse, M.G.; Lowenstein, J.A. Target heart rate to determine the normal value of coronary flow reserve during dobutamine stress echocardiography. Cardiovasc Ultrasound 2011, 9, 10. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joye, J.D.; Schulman, D.S.; Lasorda, D.; Farah, T.; Donohue, B.C.; Reichek, N. Intracoronary Doppler guide wire versus stress single-photon emission computed tomographic thallium-201 imaging in assessment of intermediate coronary stenoses. J. Am. Coll. Cardiol. 1994, 24, 940–947. [Google Scholar] [CrossRef] [Green Version]
- Abe, M.; Tomiyama, H.; Yoshida, H.; Doba, N. Diastolic fractional flow reserve to assess the functional severity of moderate coronary stenoses. Comparison with fractional flow reserve and coronary flow velocity reserve. Circulation 2000, 102, 2365–2370. [Google Scholar] [CrossRef] [Green Version]
- Schwarz, E.R.; Gupta, R.; Haager, P.K.; vom Dahl, J.; Klues, H.G.; Minartz, J.; Uretsky, B.F. Myocardial bridging in absence of coronary artery disease: Proposal of a new classification based on clinical-angiographic data and long-term follow-up. Cardiology 2009, 112, 13–21. [Google Scholar] [CrossRef]
- Schwarz, E.R.; Klues, H.G.; vom Dahl, J.; Klein, I.; Krebs, W.; Hanrath, P. Functional characteristics of myocardial bridging: A combined angiographic and intracoronary Doppler flow study. Eur. Heart J. 1997, 18, 434–442. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klues, H.G.; Schwarz, E.R.; vom Dahl, J.; Reffelmann, T.; Reu Hl Potthast, K.; Schmitz, C.; Minartz, J.; Krebs, W.; Hanrath, P. Disturbed intracoronary hemodynamics in myocardial bridging: Early normalization by intracoronary stent placement. Circulation 1997, 96, 2905–2913. [Google Scholar] [CrossRef] [PubMed]
- Ge, J.; Erbel, R.; Rupprecht, H.J.; Koch, L.; Kearney, P.; Görge, G.; Haude, M.; Meyer, J. Comparison of intravascular ultrasound and angiography in the assessment of myocardial bridging. Circulation 1994, 89, 1725–1732. [Google Scholar] [CrossRef] [Green Version]
- Ge, J.; Jeremias, A.; Rupp, A.; Abels, M.; Baumgart, D.; Liu, F.; Haude, M.; Goorge, G.; von Birgelen, C.; Sack, S.; et al. New signs characteristic of myocardial bridging demonstrated by intracoronary ultrasound and Doppler. Eur. Heart J. 1999, 20, 1707–1716. [Google Scholar] [CrossRef]
- Sicari, R.; Cortigiani, L. The clinical use of stress echocardiography in ischemic heart disease. Cardiovasc. Ultrasound 2017, 15, 7. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Saraste, M.; Koskenvuo, J.; Knuuti, J.; Toikka, J.; Laine, H.; Niemi, P.; Sakuma, H.; Hartiala, J. Coronary flow reserve measurement with transthoracic Doppler echocardiography is reproducible and comparable with positron emission tomography. Clin. Physiol. 2001, 23, 114–122. [Google Scholar] [CrossRef]




{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Variable | All (n = 81) | SE − (n = 58) | SE + (n = 23) | p-Value |
|---|---|---|---|---|
| Age ± SD, years | 56 ± 10 | 55 ± 10 | 57 ± 9 | 0.275 |
| Gender, males (%) | 55 (68) | 38 (65) | 17 (74) | 0.466 |
| BMI ± SD, kg/m2 | 27.0 ± 3.9 | 27.1 ± 4.1 | 26.5 ± 3.5 | 0.526 |
| Hypertension, n (%) | 59 (73) | 45 (78) | 14 (61) | 0.127 |
| Diabetes, n (%) | 10 (12) | 7 (12) | 3 (13) | 0.904 |
| Smoking, n (%) | 37 (46) | 26 (45) | 11 (48) | 0.807 |
| Hyperlipidemia, n (%) | 59 (73) | 44 (76) | 15 (65) | 0.331 |
| Family history, n (%) | 49 (60) | 33 (57) | 16 (70) | 0.293 |
| LVEF ± SD, % | 64 ± 8 | 64 ± 8 | 62 ± 7 | 0.161 |
| Typical chest pain, n (%) | 44 (54) | 29 (50) | 15 (65) | 0.215 |
| Atypical chest pain, n (%) | 37 (46) | 29 (50) | 8 (35) | 0.215 |
| Variable | All (n = 81) | SE− (n = 58) | SE + (n = 23) | p-Value |
|---|---|---|---|---|
| RD (end-systole) ± SD, mm | 2.59 ± 0.39 | 2.64 ± 0.40 | 2.47 ± 0.33 | 0.126 |
| RD (end-diastole) ± SD, mm | 2.65 ± 0.40 * | 2.70 ± 0.40 * | 2.53 ± 0.36 * | 0.140 |
| MLD (end-systole) ± SD, mm | 0.98 ± 0.31 | 1.01 ± 0.29 | 0.89 ± 0.34 | 0.200 |
| MLD (end-diastole) ± SD, mm | 1.84 ± 0.39 * | 1.96 ± 0.36 * | 1.55 ± 0.31 * | <0.001 |
| DS (end-systole) ± SD, % | 62 ± 11 | 62 ± 10 | 64 ± 12 | 0.496 |
| DS (end-diastole) ± SD, % | 31 ± 10 * | 27 ± 8 * | 39 ± 8 * | <0.001 |
| All (n = 81) | SE− (n = 58) | SE + (n = 23) | p-Value | |
|---|---|---|---|---|
| HR, bpm (baseline) | 74 ± 11 | 75 ± 10 | 72 ± 11 | 0.240 |
| HR, bpm (DOBmax) | 139 ± 9 * | 140 ± 8 * | 136 ± 12 * | 0.093 |
| Mean systolic BP, mmHg (baseline) | 129 ± 13 | 130 ± 12 | 126 ± 13 | 0.253 |
| Mean systolic BP, mmHg (DOBmax) | 133 ± 17 | 134 ± 18 | 129 ± 14 | 0.264 |
| Mean diastolic BP, mmHg (baseline) | 82 ± 10 | 82 ± 10 | 82 ± 10 | 0.946 |
| Mean diastolic BP, mmHg (DOBmax) | 82 ± 9 | 83 ± 9 | 80 ± 7 | 0.141 |
| RPP, ×103 bpm∙mmHg (baseline) | 9.6 ± 2.0 | 9.7 ± 1.8 | 9.1 ± 2.2 | 0.186 |
| RPP, ×103 bpm∙mmHg (DOBmax) | 18.5 ± 2.6 * | 18.8 ± 2.4 * | 17.6 ± 2.9 * | 0.151 |
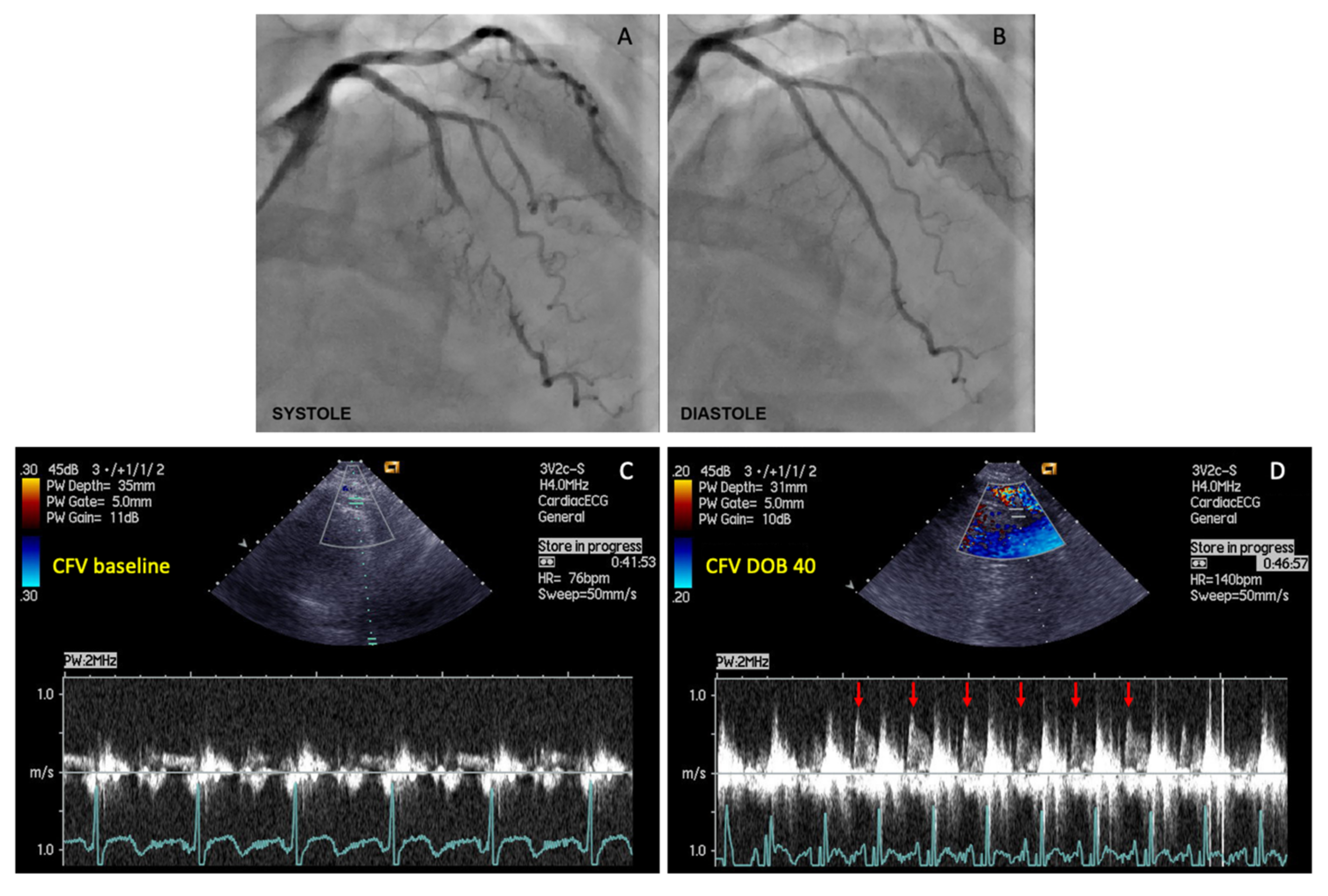
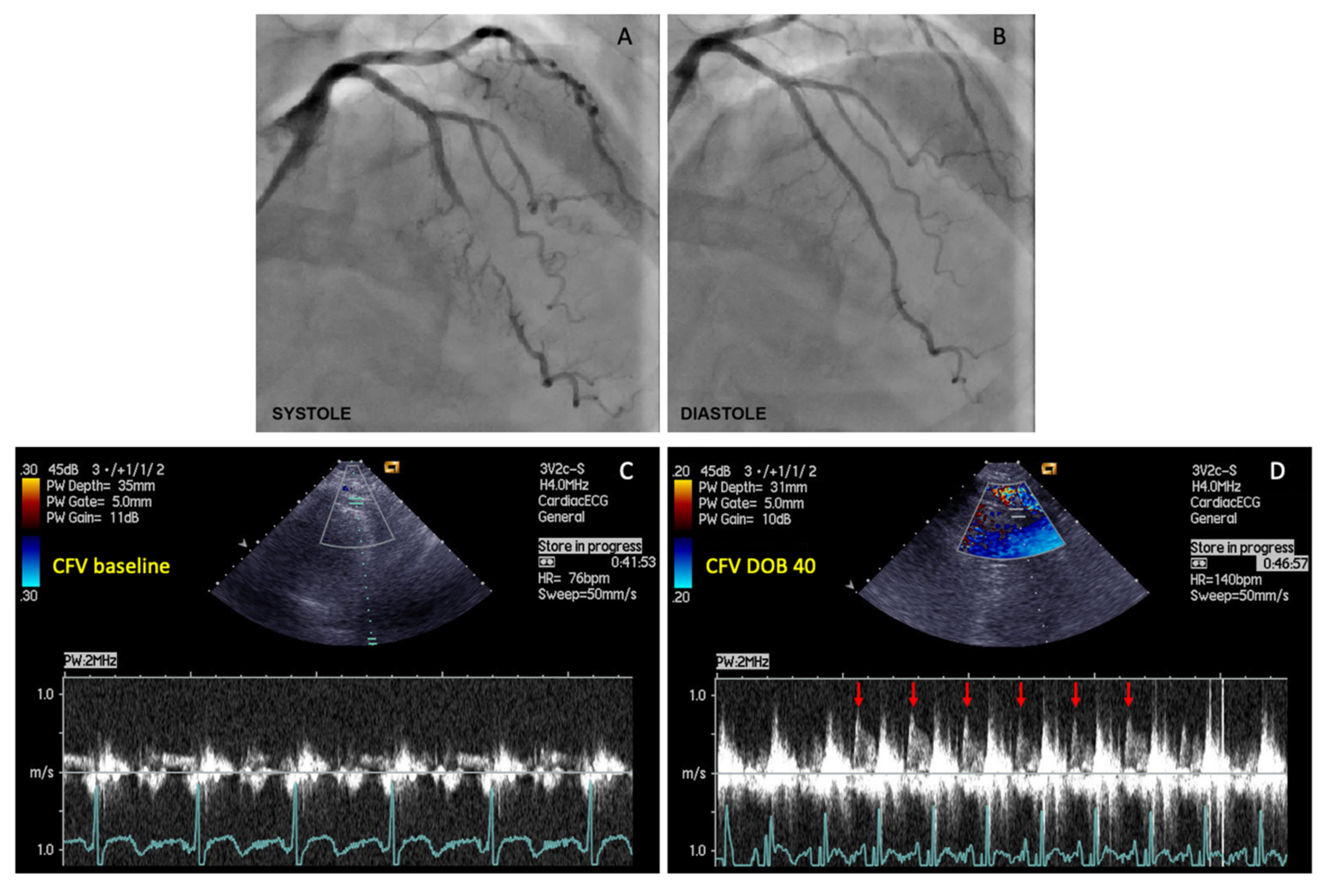
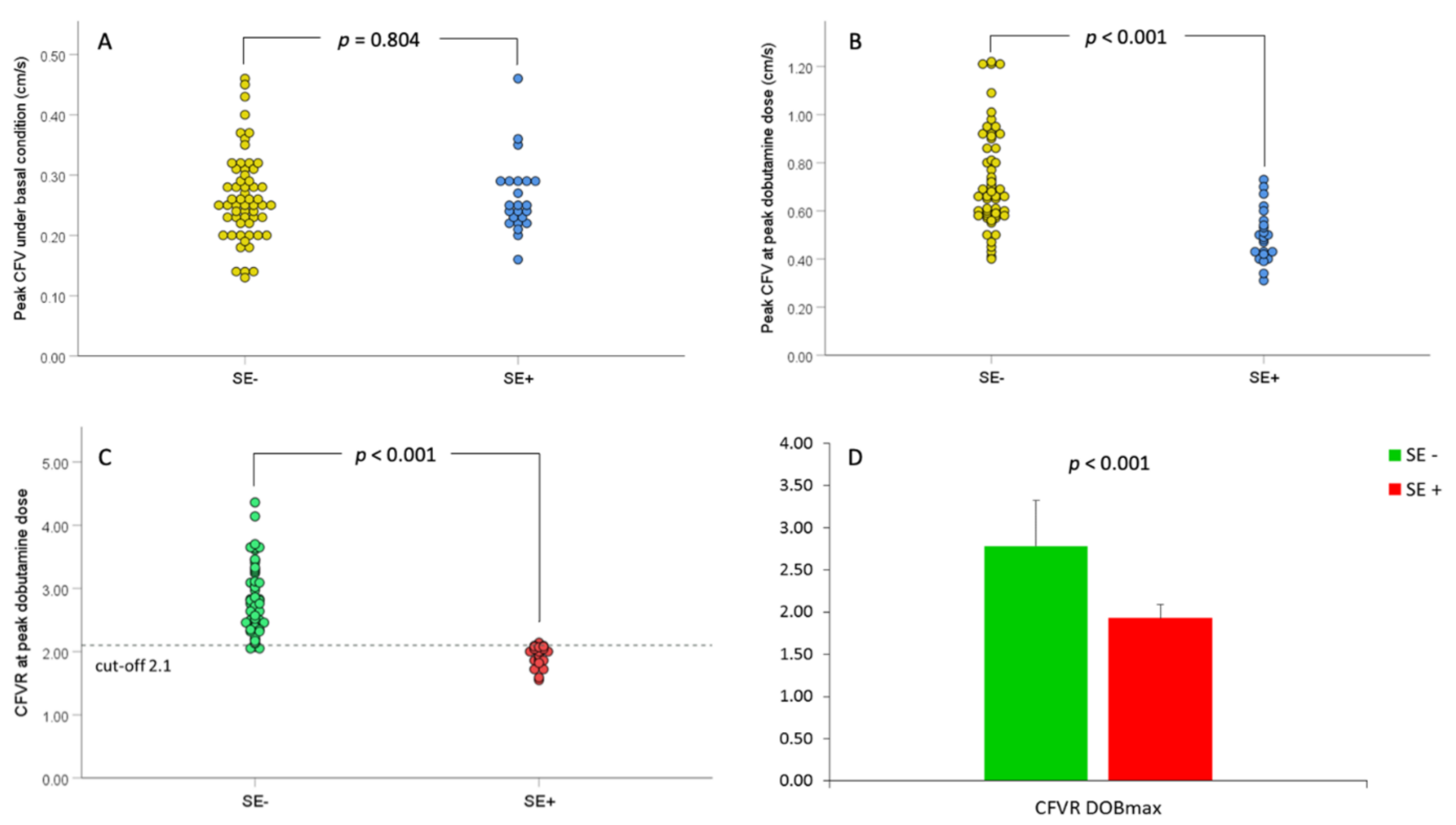
| CFV, cm/s (baseline) | 26.42 ± 6.97 | 26.47 ± 7.28 | 26.30 ± 6.28 | 0.804 |
| CFV, cm/s (DOBmax) | 67.44 ± 21.15 * | 72.62 ± 20.74 * | 50.78 ± 11.05 * | <0.001 |
| CFVR | 2.55 ± 0.61 | 2.78 ± 0.54 | 1.93 ± 0.16 | <0.001 |
| Univariate Analysis | OR (95% CI for OR) | p-Value | R2 | HL Test p-Value |
|---|---|---|---|---|
| Age, years | 1.037 (0.982–1.094) | 0.182 | 0.033 | 0.411 |
| Gender, males | 1.759 (0.604–5.120) | 0.300 | 0.019 | 1.000 |
| BMI, kg/m2 | 0.954 (0.841–1.082) | 0.461 | 0.010 | 0.975 |
| Hypertension | 0.537 (0.193–1.499) | 0.235 | 0.024 | 1.000 |
| Diabetes | 1.587 (0.406–6.209) | 0.507 | 0.007 | 1.000 |
| Smoking | 1.444 (0.561–3.722) | 0.446 | 0.010 | 1.000 |
| Heredity | 1.239 (0.467–3.284) | 0.667 | 0.003 | 1.000 |
| Hyperlipidemia | 0.537 (0.193–1.499) | 0.235 | 0.024 | 1.000 |
| LVEF, % | 0.950 (0.888–1.016) | 0.134 | 0.045 | 0.532 |
| Typical chest pain, % | 1.778 (0.674–4.691) | 0.245 | 0.024 | 1.000 |
| Atypical chest pain, % | 0.563 (0.213–1.484) | 0.245 | 0.024 | 1.000 |
| RD (end-systole), mm | 0.326 (0.073–1.454) | 0.142 | 0.054 | 0.666 |
| RD (end-diastole), mm | 0.340 (0.078–1.481) | 0.151 | 0.051 | 0.223 |
| MLD MB (end-systole), mm | 0.426 (0.074–2.465) | 0.341 | 0.022 | 0.080 |
| MLD MB (end-diastole), mm | 0.072 (0.012–0.459) | 0.005 | 0.218 | 0.931 |
| DS MB (end-systole), % | 1.009 (0.958–1.062) | 0.745 | 0.003 | 0.189 |
| DS MB (end-diastole), % | 1.145 (1.053–1.244) | 0.001 | 0.308 | 0.589 |
| Model 1. Backward Method with Age, LVEF, RD, and MLD MB at End-Diastole: | OR (95% CI for OR) | p-Value | R2 | HL Test p-Value |
| Age, years | 1.043 (0.970–1.122) | 0.252 | 0.314 | 0.224 |
| LVEF, % | 0.936 (0.856–1.024) | 0.152 | 0.314 | 0.224 |
| RD (end-diastole), mm | 5.321 (0.340–83.172) | 0.233 | 0.314 | 0.224 |
| MLD MB (end-diastole), mm a | 0.023 (0.001–0.534) | 0.019 | 0.314 | 0.224 |
| Model 2. Backward Method with Age, LVEF, RD, and %DS MB at End-diastole: | OR (95% CI for OR) | p-Value | R2 | HL Test p-Value |
| Age, years | 1.059 (0.978–1.146) | 0.161 | 0.395 | 0.533 |
| LVEF, % | 0.939 (0.853–1.033) | 0.197 | 0.395 | 0.533 |
| RD (end-diastole), mm | 0.438 (0.076–2.519) | 0.355 | 0.395 | 0.533 |
| DS MB (end-diastole), % a | 1.147 (1.042–1.263) | 0.005 | 0.395 | 0.533 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Aleksandric, S.B.; Djordjevic-Dikic, A.D.; Giga, V.L.; Tesic, M.B.; Soldatovic, I.A.; Banovic, M.D.; Dobric, M.R.; Vukcevic, V.; Tomasevic, M.V.; Orlic, D.N.; et al. Coronary Flow Velocity Reserve Using Dobutamine Test for Noninvasive Functional Assessment of Myocardial Bridging. J. Clin. Med. 2022, 11, 204. https://doi.org/10.3390/jcm11010204
Aleksandric SB, Djordjevic-Dikic AD, Giga VL, Tesic MB, Soldatovic IA, Banovic MD, Dobric MR, Vukcevic V, Tomasevic MV, Orlic DN, et al. Coronary Flow Velocity Reserve Using Dobutamine Test for Noninvasive Functional Assessment of Myocardial Bridging. Journal of Clinical Medicine. 2022; 11(1):204. https://doi.org/10.3390/jcm11010204
Chicago/Turabian StyleAleksandric, Srdjan B., Ana D. Djordjevic-Dikic, Vojislav L. Giga, Milorad B. Tesic, Ivan A. Soldatovic, Marko D. Banovic, Milan R. Dobric, Vladan Vukcevic, Miloje V. Tomasevic, Dejan N. Orlic, and et al. 2022. "Coronary Flow Velocity Reserve Using Dobutamine Test for Noninvasive Functional Assessment of Myocardial Bridging" Journal of Clinical Medicine 11, no. 1: 204. https://doi.org/10.3390/jcm11010204
APA StyleAleksandric, S. B., Djordjevic-Dikic, A. D., Giga, V. L., Tesic, M. B., Soldatovic, I. A., Banovic, M. D., Dobric, M. R., Vukcevic, V., Tomasevic, M. V., Orlic, D. N., Boskovic, N., Jovanovic, I., Nedeljkovic, M. A., Stankovic, G., Ostojic, M. C., & Beleslin, B. D. (2022). Coronary Flow Velocity Reserve Using Dobutamine Test for Noninvasive Functional Assessment of Myocardial Bridging. Journal of Clinical Medicine, 11(1), 204. https://doi.org/10.3390/jcm11010204