
BMI Specific Complications Following Implant-Based Breast Reconstruction after Mastectomy


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Statistical Analysis
3. Results
3.1. Patient Characteristics
3.2. Complications
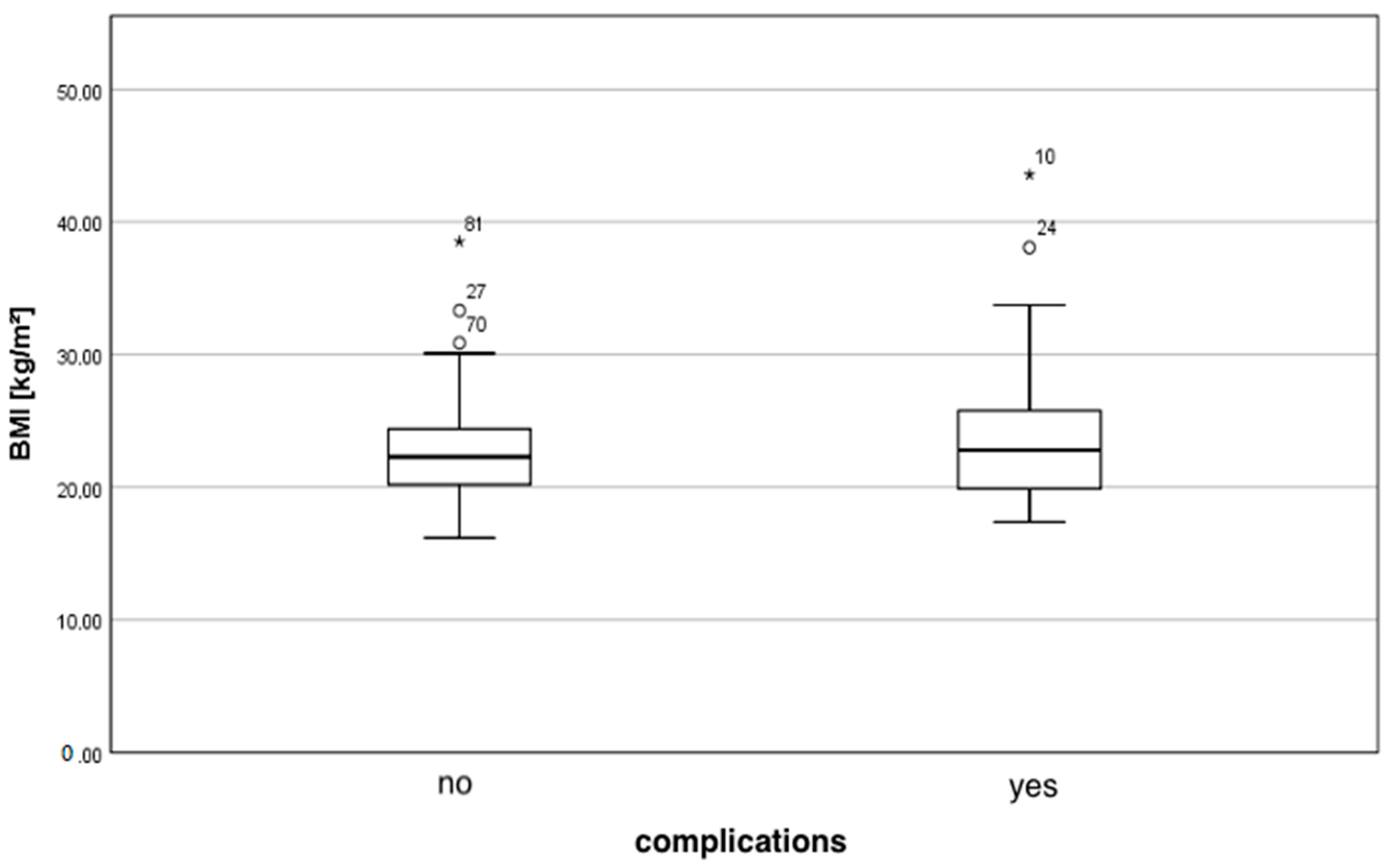
3.3. Body Mass Index (BMI)
3.4. Comorbidities and Other Risk Factors
3.5. Surgical Details
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
Appendix A

{kind=link}
| Parameters | Complications | p | |
|---|---|---|---|
| Yes (n = 40; 30.5%) | No (n = 91; 69.5%) | ||
| Implant type | (n = 39; 29.1%) | (n = 91; 69.5%) | 0.009 |
| Silicone | 19 (47.5%) | 23 (25.3%) | |
| Expander | 20 (50.0%) | 68 (74.7%) | |
| Age (y) | 0.717 | ||
| M ± SD | 47.7 ± 10.7 | 46.5 ± 10.7 | |
| Md (min—max) | 47 (30–73) | 46 (27–76) | |
| BMI (kg/m²) | 0.646 | ||
| M ± SD | 23.9 ± 5.7 | 22.8 ± 3.7 | |
| Md (min—max) | 22.8 (17.4–43.6) | 22.3 (16.1–38.5) | |
| Underweight | 4 (10.0%) | 7 (7.7%) | 0.284 |
| Normal weight | 23 (57.5%) | 65 (71.4%) | |
| Overweight | 13 (32.5%) | 19 (20.9%) | |
| (n = 40; 30.5%) | (n = 91; 69.5%) | 0.198 | |
| Obese | 4 (10.0%) | 4 (4.4%) | |
| Non-obese | 36 (90.0%) | 87 (95.6%) | |
| Comorbidities | (n = 21; 16.0%) | (n = 41; 31.3%) | |
| Arterial hypertension | 7 | 13 | 0.638 |
| Diabetes mellitus | 2 | 2 | 0.585 |
| Smokers | 12 | 26 | 0.868 |
| Timing of reconstruction | (n = 40; 30.5%) | (n = 91; 69.5%) | 0.198 |
| Immediate | 33 (82.5%) | 65 (71.4%) | |
| Delayed | 7 (17.5%) | 26 (28.6%) | |
| Surgery time (min) | <0.001 | ||
| M ± SD | 229.4 ± 78.5 | 176.4 ± 70.1 | |
| Md (min-max) | 235 (60–400) | 180 (45–335) | |
| Implant volume (cm3) | 0.984 | ||
| M ± SD | 325.8 ± 114.4 | 318.1 ± 96.4 | |
| Md (min-max) | 300 (120–685) | 315 (120–685) | |
| Implant position | (n = 40; 30.5%) | (n = 91; 69.5%) | 1 |
| Submuscular | 38 (95%) | 86 (94.5%) | |
| Prepectoral | 2 (5%) | 5 (5.5%) | |
| LD-flap | (n = 40; 100%) | (n = 91; 100%) | 0.309 |
| With | 5 (12.5%) | 6 (6.6%) | |
| Without | 35 (87.5%) | 85 (93.4%) | |
| Length of stay | 0.002 | ||
| M ± SD | 11.3 ± 4.6 | 9.2 ± 3.8 | |
| Md (min-max) | 10 (5–29) | 9 (4–38) | |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Rojas, K.; Stuckey, A. Breast Cancer Epidemiology and Risk Factors. Clin. Obstet. Gynecol. 2016, 59, 651–672. [Google Scholar] [CrossRef] [PubMed]
- Hindle, W. Breast cancer: Introduction. Clin. Obstet. Gynecol. 2002, 45, 738–745. [Google Scholar] [CrossRef] [PubMed]
- Waks, A.G.; Winer, E.P. Breast Cancer Treatment: A Review. JAMA 2019, 321, 288–300. [Google Scholar] [CrossRef]
- Brackstone, M.; Fletcher, G.G.; Dayes, I.S.; Madarnas, Y.; Sen Gupta, S.K.; Verma, S.; Eisen, A.; Gandhi, S.; Holloway, C.; Trudeau, M.; et al. Locoregional therapy of locally advanced breast cancer: A clinical practice guideline. Curr. Oncol. 2015, 22 (Suppl. 1), S54–S66. [Google Scholar] [CrossRef] [Green Version]
- Voogd, A.C.; Nielsen, M.; Peterse, J.L.; Blichert-Toft, M.; Bartelink, H.; Overgaard, M.; van Tienhoven, G.; Andersen, K.W.; Sylvester, R.J.; van Dongen, J.A. Differences in risk factors for local and distant recurrence after breast-conserving therapy or mastectomy for stage I and II breast cancer: Pooled results of two large European randomized trials. J. Clin. Oncol. 2001, 19, 1688–1697. [Google Scholar] [CrossRef]
- Fisher, B.; Anderson, S. Conservative surgery for the management of invasive and noninvasive carcinoma of the breast: NSABP trials. National Surgical Adjuvant Breast and Bowel Project. World J. Surg. 1994, 18, 63–69. [Google Scholar] [CrossRef]
- New Zealand Guidelines Group. Management of Early Breast Cancer—Evidence-Based Best Practice Guideline; New Zealand Guidelines Group: Wellington, New Zealand, 2009. [Google Scholar]
- Serletti, J.M.; Fosnot, J.; Nelson, J.A.; Disa, J.J.; Bucky, L.P. Breast reconstruction after breast cancer. Plast. Reconstr. Surg. 2011, 127, 124e–135e. [Google Scholar] [CrossRef]
- Toyserkani, N.M.; Jørgensen, M.G.; Tabatabaeifar, S.; Damsgaard, T.; Sørensen, J.A. Autologous versus implant-based breast reconstruction: A systematic review and meta-analysis of Breast-Q patient-reported outcomes. J. Plast. Reconstr. Aesthet. Surg. 2020, 73, 278–285. [Google Scholar] [CrossRef]
- Guyomard, V.; Leinster, S.; Wilkinson, M. Systematic review of studies of patients’ satisfaction with breast reconstruction after mastectomy. Breast 2007, 16, 547–567. [Google Scholar] [CrossRef]
- Goodwin, S.J.; McCarthy, C.M.; Pusic, A.L.; Bui, D.; Howard, M.; Disa, J.J.; Cordeiro, P.G.; Mehrara, B.J. Complications in smokers after postmastectomy tissue expander/implant breast reconstruction. Ann. Plast. Surg. 2005, 55, 16–20. [Google Scholar] [CrossRef]
- McCarthy, C.M.; Mehrara, B.J.; Riedel, E.; Davidge, K.; Hinson, A.; Disa, J.J.; Cordeiro, P.G.; Pusic, A.L. Predicting complications following expander/implant breast reconstruction: An outcomes analysis based on preoperative clinical risk. Plast. Reconstr. Surg. 2008, 121, 1886–1892. [Google Scholar] [CrossRef] [PubMed]
- Woerdeman, L.A.E.; Hage, J.J.; Hofland, M.M.I.; Rutgers, E.J.T. A prospective assessment of surgical risk factors in 400 cases of skin-sparing mastectomy and immediate breast reconstruction with implants to establish selection criteria. Plast. Reconstr. Surg. 2007, 119, 455–463. [Google Scholar] [CrossRef] [PubMed]
- Alderman, A.; Gutowski, K.; Ahuja, A.; Gray, D. ASPS clinical practice guideline summary on breast reconstruction with expanders and implants. Plast. Reconstr. Surg. 2014, 134, 648e–655e. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Doyle, S.L.; Lysaght, J.; Reynolds, J.V. Obesity and post-operative complications in patients undergoing non-bariatric surgery. Obes. Rev. Off. J. Int. Assoc. Study Obes. 2010, 11, 875–886. [Google Scholar] [CrossRef] [PubMed]
- Haslam, D.W.; James, W.P.T. Obesity. Lancet 2005, 366, 1197–1209. [Google Scholar] [CrossRef]
- Kopelman, P.G. Obesity as a medical problem. Nature 2000, 404, 635–643. [Google Scholar] [CrossRef]
- Gupta, V.; Winocour, J.; Rodriguez-Feo, C.; Bamba, R.; Shack, R.B.; Grotting, J.C.; Higdon, K.K. Safety of Aesthetic Surgery in the Overweight Patient: Analysis of 127,961 Patients. Aesthetic Surg. J. 2016, 36, 718–729. [Google Scholar] [CrossRef] [Green Version]
- Nguyen, K.T.; Hanwright, P.J.; Smetona, J.T.; Hirsch, E.M.; Seth, A.K.; Kim, J.Y.S. Body mass index as a continuous predictor of outcomes after expander-implant breast reconstruction. Ann. Plast. Surg. 2014, 73, 19–24. [Google Scholar] [CrossRef]
- Fischer, J.P.; Nelson, J.A.; Kovach, S.J.; Serletti, J.M.; Wu, L.C.; Kanchwala, S. Impact of obesity on outcomes in breast reconstruction: Analysis of 15,937 patients from the ACS-NSQIP datasets. J. Am. Coll. Surg. 2013, 217, 656–664. [Google Scholar] [CrossRef] [PubMed]
- Srinivasa, D.R.; Clemens, M.W.; Qi, J.; Hamill, J.B.; Kim, H.M.; Pusic, A.L.; Wilkins, E.G.; Butler, C.E.; Garvey, P.B. Obesity and Breast Reconstruction: Complications and Patient-Reported Outcomes in a Multicenter, Prospective Study. Plast. Reconstr. Surg. 2020, 145, 481E–490E. [Google Scholar] [CrossRef] [PubMed]
- Viscardi, J.A.; Oranges, C.M.; Schaefer, D.J.; Kalbermatten, D.F. Reduction Mammoplasty: A Ten-Year Retrospective Review of the Omega Resection Pattern Technique. J. Clin. Med. 2021, 10, 4418. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. “WHO/Europe|Nutrition—Body Mass Index—BMI,” World Health Organization. 2021. Available online: https://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi (accessed on 21 August 2021).
- Hanwright, P.J.; Davila, A.A.; Hirsch, E.M.; Khan, S.A.; Fine, N.A.; Bilimoria, K.Y.; Kim, J.Y.S. The differential effect of BMI on prosthetic versus autogenous breast reconstruction: A multivariate analysis of 12,986 patients. Breast 2013, 22, 938–945. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, A.; Sigalove, S.; Sigalove, N.M.; Storm-Dickerson, T.L.; Pope, N.; Rice, J.; Maxwell, G.P. Effect of Body Mass Index on Outcomes after Prepectoral Breast Reconstruction. Plast. Reconstr. Surg. 2019, 144, 550–558. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, A.; Sigalove, S.; Storm-Dickerson, T.L.; Sigalove, N.M.; Pope, N.; Rice, J.; Maxwell, G.P. Dual-Plane versus Prepectoral Breast Reconstruction in High-Body Mass Index Patients. Plast. Reconstr. Surg. 2020, 145, 1357–1365. [Google Scholar] [CrossRef] [PubMed]
- Hubert, H.B.; Feinleib, M.; McNamara, P.M.; Castelli, W.P. Obesity as an independent risk factor for cardiovascular disease: A 26-year follow-up of participants in the Framingham Heart Study. Circulation 1983, 67, 968–977. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nguyen, N.T.; Magno, C.P.; Lane, K.T.; Hinojosa, M.W.; Lane, J.S. Association of Hypertension, Diabetes, Dyslipidemia, and Metabolic Syndrome with Obesity: Findings from the National Health and Nutrition Examination Survey, 1999 to 2004. J. Am. Coll. Surg. 2008, 207, 928–934. [Google Scholar] [CrossRef]
- Hart, A.; Funderburk, C.D.; Chu, C.K.; Pinell-White, X.; Halgopian, T.; Manning-Geist, B.; Carlson, G.; Losken, A. The Impact of Diabetes Mellitus on Wound Healing in Breast Reconstruction. Ann. Plast. Surg. 2017, 78, 260–263. [Google Scholar] [CrossRef]
- Ottesen, T.D.; Malpani, R.; Galivanche, A.R.; Zogg, C.K.; Varthi, A.G.; Grauer, J.N. Underweight patients are at just as much risk as super morbidly obese patients when undergoing anterior cervical spine surgery. Spine J. 2020, 20, 1085–1095. [Google Scholar] [CrossRef]
- Shida, A.; Ida, M.; Ueda, M.; Kirita, T.; Kawaguchi, M. Preoperative underweight is associated with adverse postoperative events in patients undergoing microvascular reconstruction surgery for oral and maxillofacial cancer. Int. J. Oral Maxillofac. Surg. 2021, 50, 598–603. [Google Scholar] [CrossRef]
- Weichman, K.E.; Broer, P.N.; Thanik, V.D.; Wilson, S.C.; Tanna, N.; Levine, J.P.; Choi, M.; Karp, N.S.; Hazen, A. Patient-reported satisfaction and quality of life following breast reconstruction in thin patients: A comparison between microsurgical and prosthetic implant recipients. Plast. Reconstr. Surg. 2015, 136, 213–220. [Google Scholar] [CrossRef] [PubMed]
- Yang, C.-E.; Chung, S.W.; Lee, D.W.; Lew, D.H.; Song, S.Y. Evaluation of the Relationship Between Flap Tension and Tissue Perfusion in Implant-Based Breast Reconstruction Using Laser-Assisted Indocyanine Green Angiography. Ann. Surg. Oncol. 2018, 25, 2235–2240. [Google Scholar] [CrossRef] [PubMed]
- Gabriel, A.; Maxwell, G.P. Prepectoral Breast Reconstruction in Challenging Patients. Plast. Reconstr. Surg. 2017, 140, 14S–21S. [Google Scholar] [CrossRef] [PubMed]
| Complications | Major | Minor | Total (n = 131) |
|---|---|---|---|
| Impaired wound healing | 12 (9.15%) | 12 (9.15%) | 24 (18.3%) |
| Hematoma | 5 (3.8%) | 1 (0.8%) | 6 (4.6%) |
| Seroma | 2 (1.5%) | 6 (4.6%) | 8 (6.1%) |
| Capsular fibrosis | 6 (4.6%) | 0 | 6 (4.6%) |
| Rupture | 2 (1.5%) | 0 | 2 (1.5%) |
| Infection | 5 (3.8%) | 0 | 5 (3.8%) |
| BMI | Nutritional Status | Number of Patients |
|---|---|---|
| <8.5 | Underweight | 11 (8.2%) |
| 18.5–24.9 | Normal weight | 90 (67.2%) |
| 25.0–29.9 | Pre-obesity | 25 (18.7%) |
| 30.0–34.9 | Obesity class I | 5 (3.7%) |
| 35.0–39.9 | Obesity class II | 2 (1.5%) |
| ≥40 | Obesity class III | 1 (0.7%) |
| Total | 134 (100 %) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Leitner, H.S.; Pauzenberger, R.; Ederer, I.A.; Radtke, C.; Hacker, S. BMI Specific Complications Following Implant-Based Breast Reconstruction after Mastectomy. J. Clin. Med. 2021, 10, 5665. https://doi.org/10.3390/jcm10235665
Leitner HS, Pauzenberger R, Ederer IA, Radtke C, Hacker S. BMI Specific Complications Following Implant-Based Breast Reconstruction after Mastectomy. Journal of Clinical Medicine. 2021; 10(23):5665. https://doi.org/10.3390/jcm10235665
Chicago/Turabian StyleLeitner, Helena Sophie, Reinhard Pauzenberger, Ines Ana Ederer, Christine Radtke, and Stefan Hacker. 2021. "BMI Specific Complications Following Implant-Based Breast Reconstruction after Mastectomy" Journal of Clinical Medicine 10, no. 23: 5665. https://doi.org/10.3390/jcm10235665
APA StyleLeitner, H. S., Pauzenberger, R., Ederer, I. A., Radtke, C., & Hacker, S. (2021). BMI Specific Complications Following Implant-Based Breast Reconstruction after Mastectomy. Journal of Clinical Medicine, 10(23), 5665. https://doi.org/10.3390/jcm10235665