
Projections of Primary and Revision Shoulder Arthroplasty until 2040: Facing a Massive Rise in Fracture-Related Procedures



Abstract
:1. Introduction
2. Materials and Methods
2.1. Data Collection
2.2. Data Analysis
3. Results
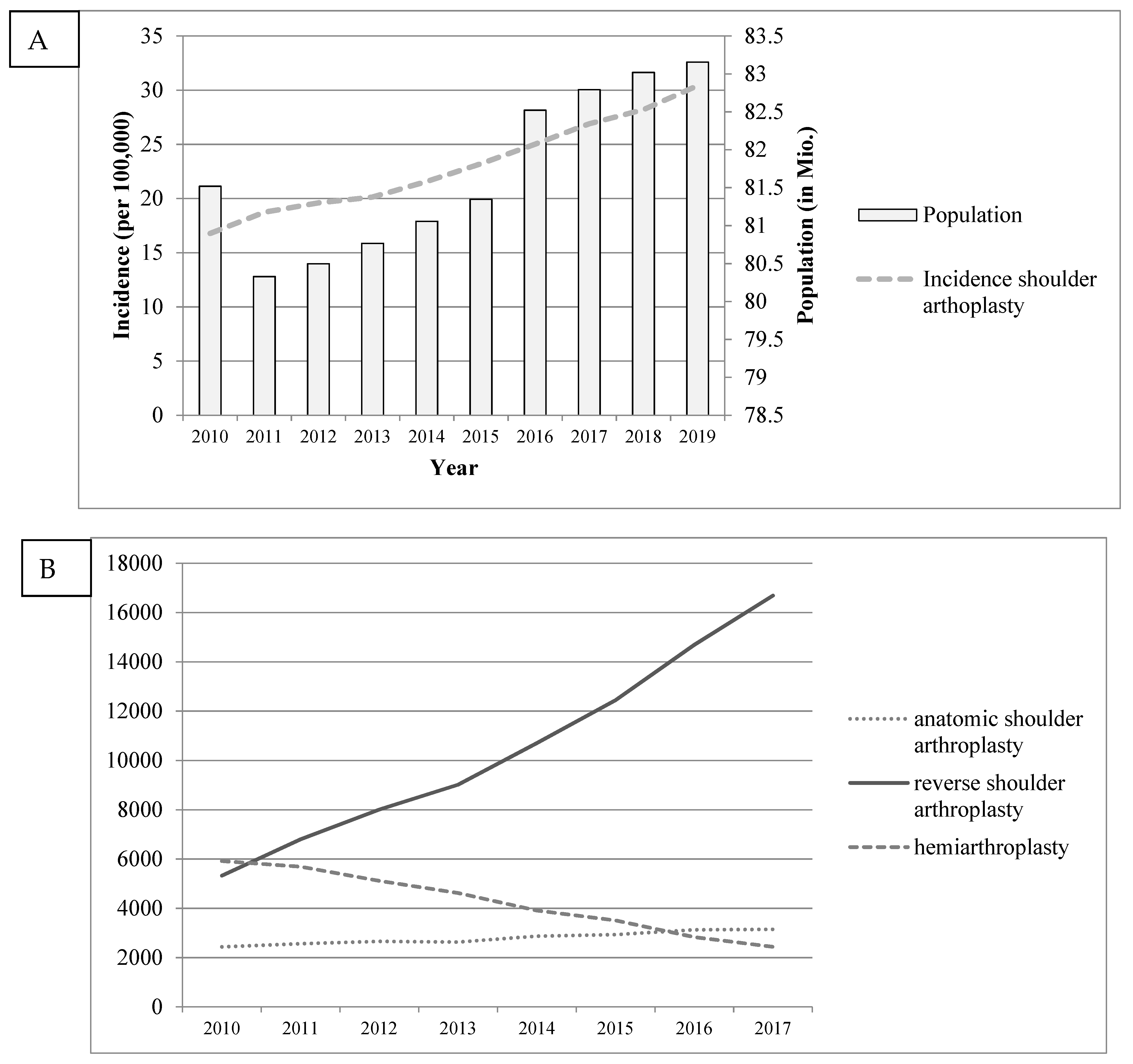
3.1. Historical Data: Baseline Years 2010–2019
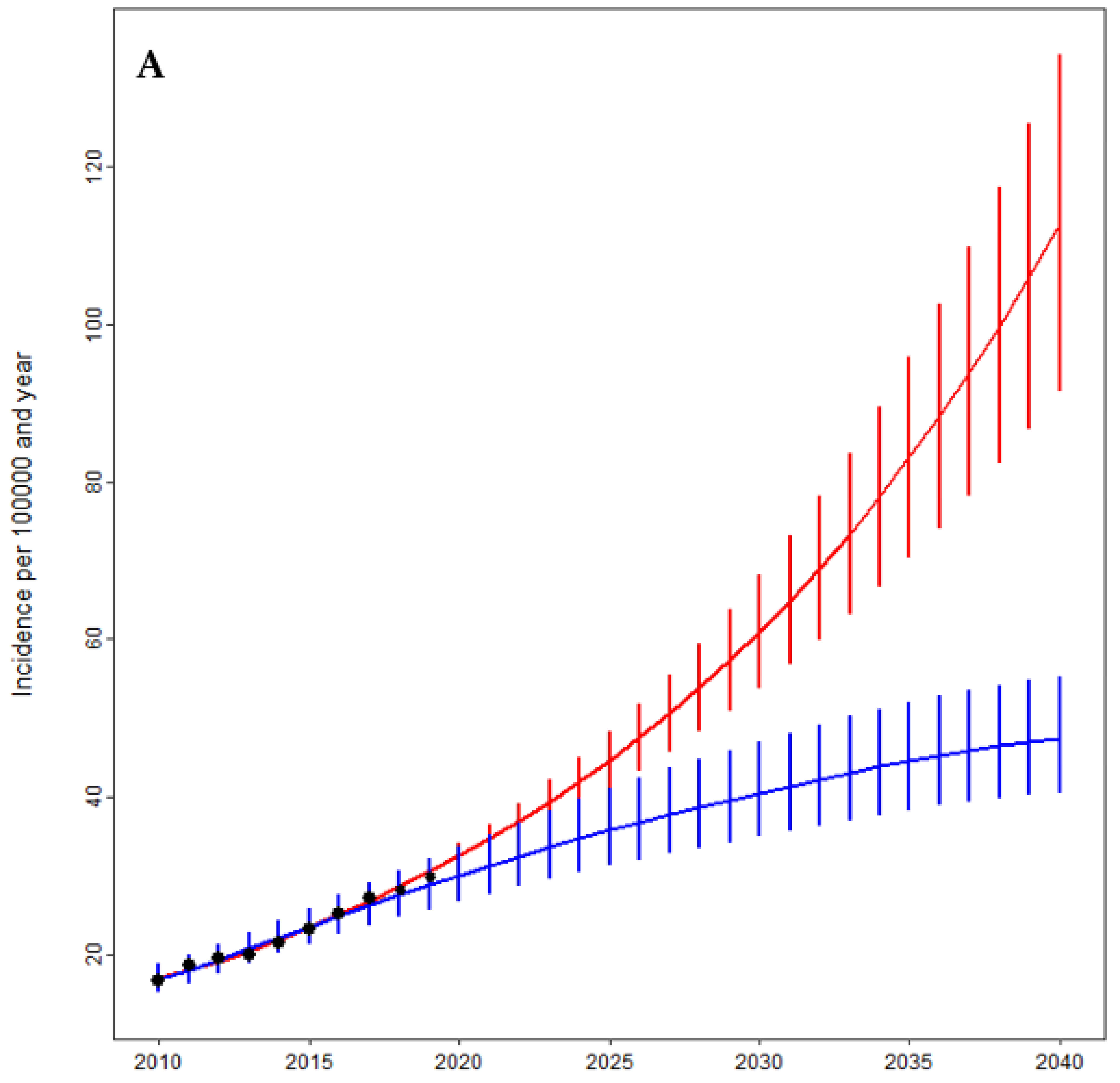
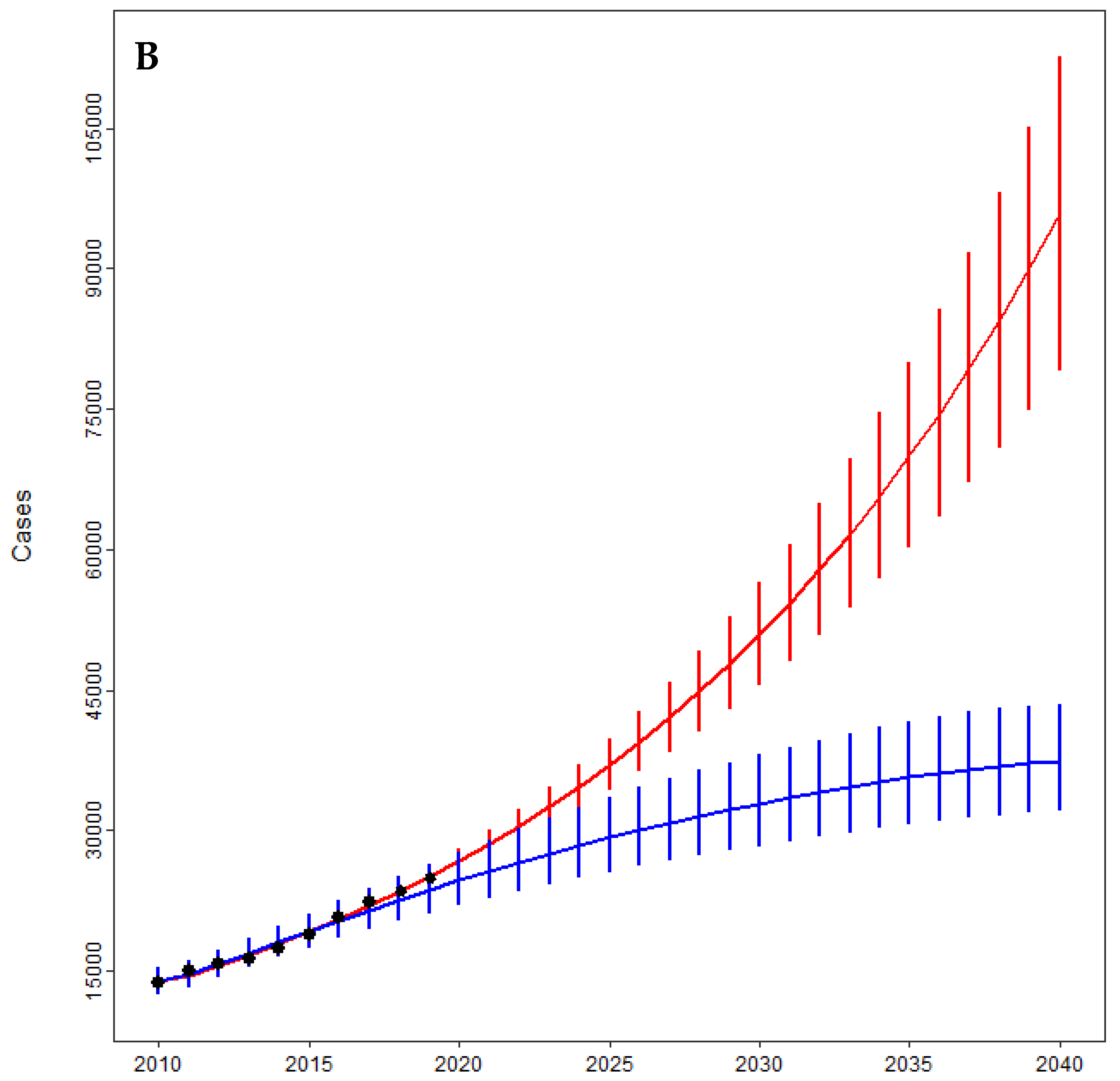
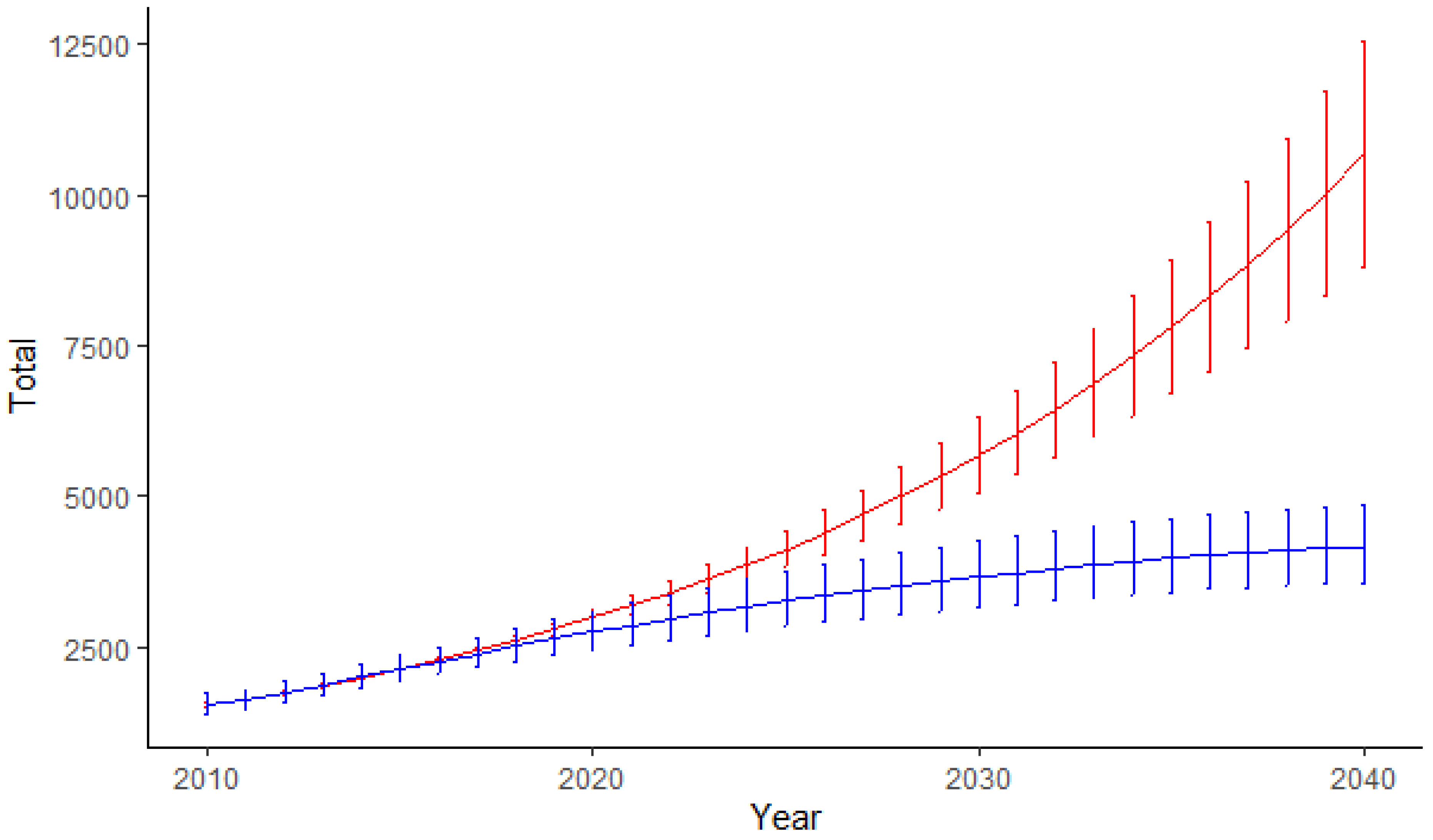
3.2. Projection of Primary Shoulder Arthroplasty: Years 2020–2040
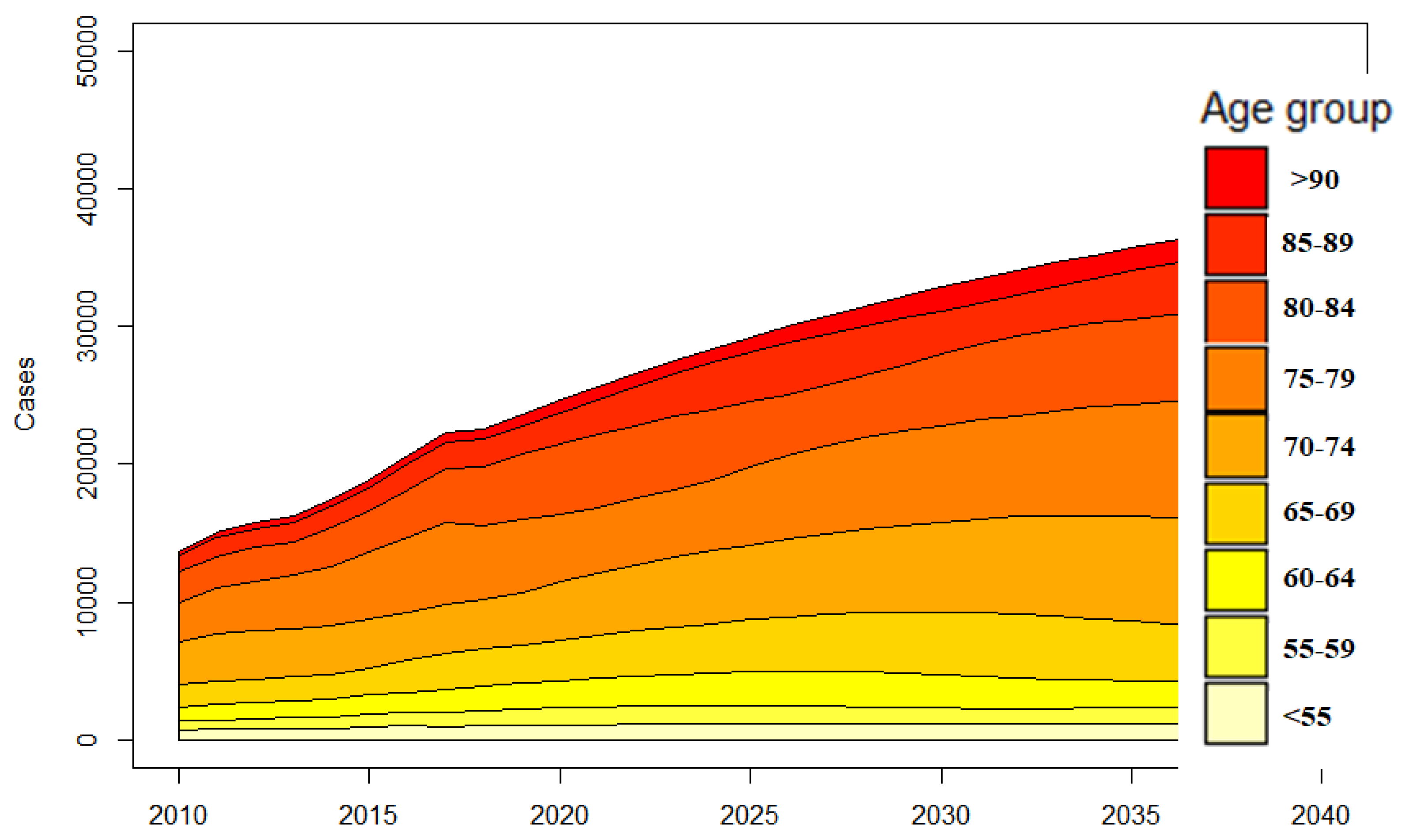
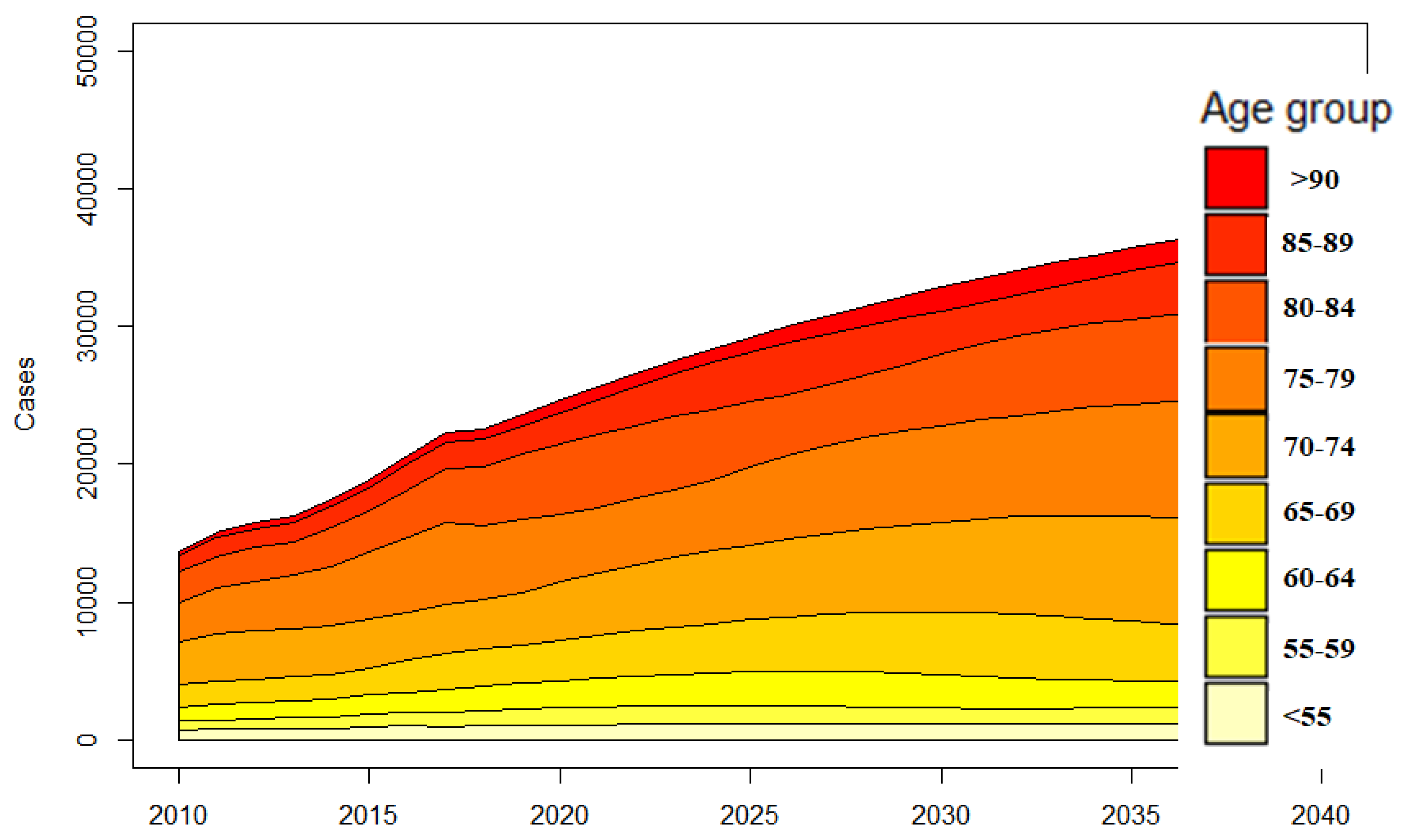
3.3. Projections of Shoulder Arthroplasty as a Function of Age
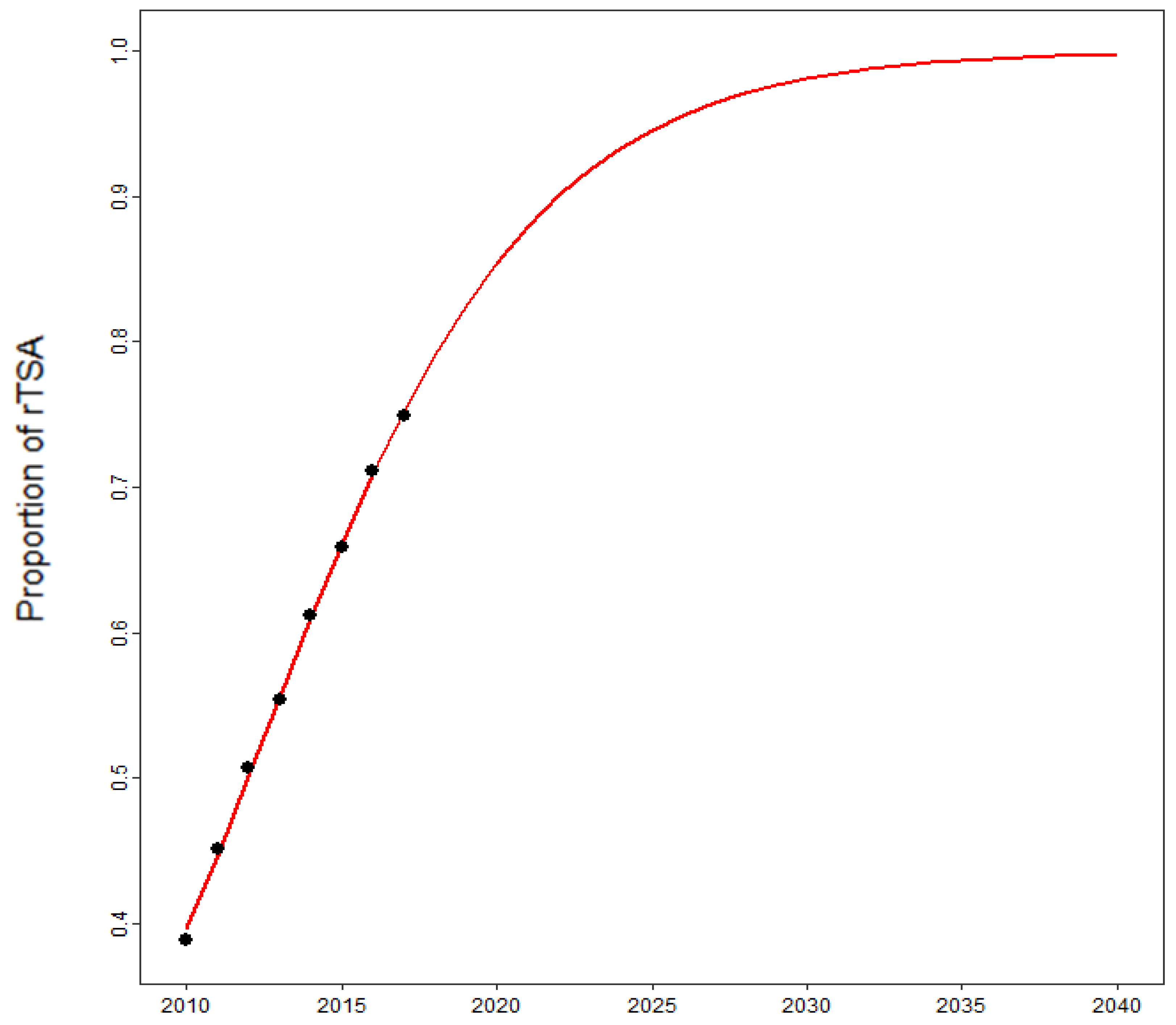
3.4. Projections of Revision Shoulder Arthroplasty
4. Discussion
4.1. Projections of Shoulder Arthroplasty and International Comparison
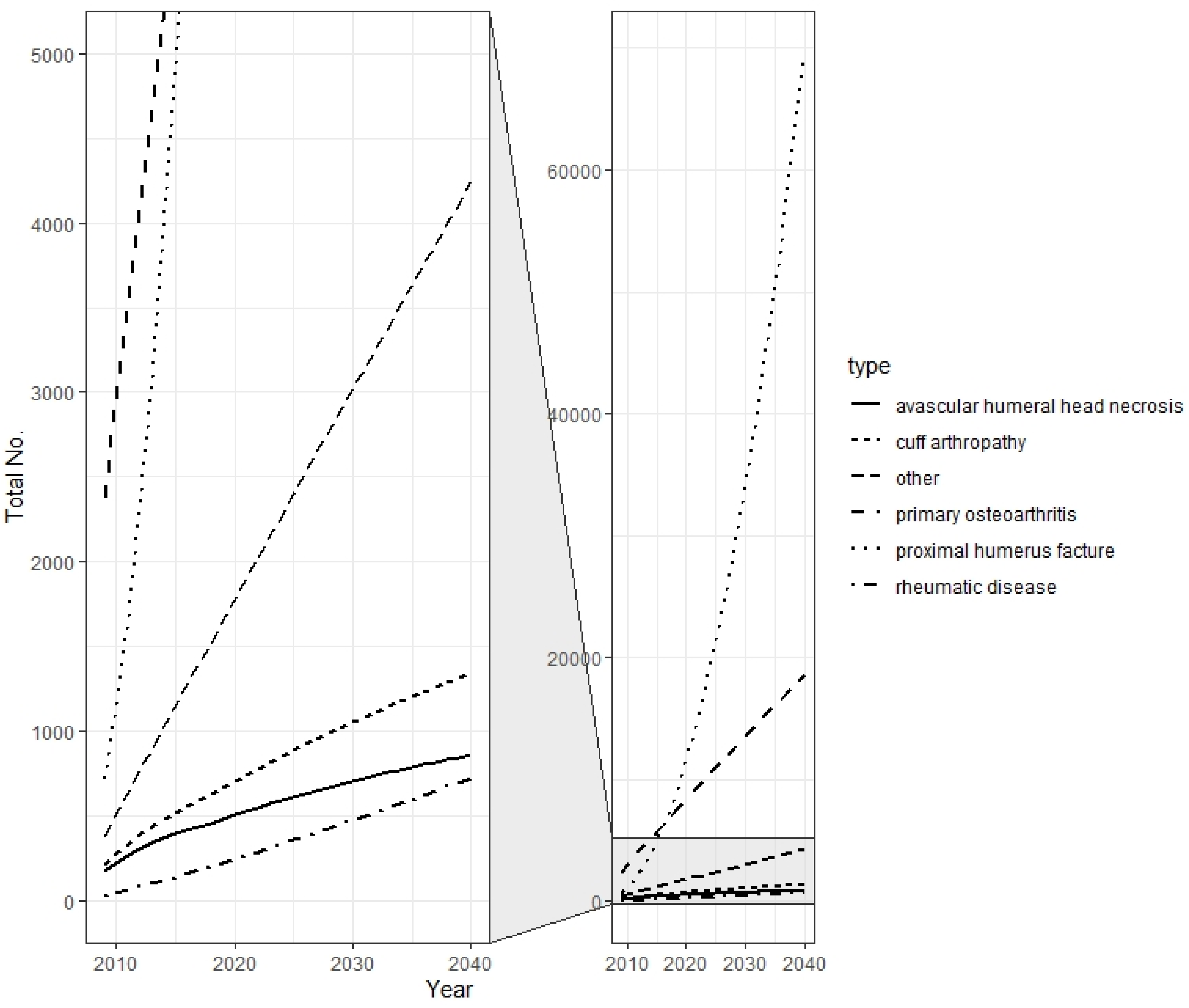
4.2. Projections as a Function of Age and Indication
4.3. Projections of Revision Shoulder Arthroplasty
4.4. Study Limitations
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Acknowledgments
Conflicts of Interest
References
- Nowossadeck, E. Population aging and hospitalization for chronic disease in Germany. Dtsch. Arztebl. Int. 2012, 109, 151–157. [Google Scholar] [CrossRef]
- Pilz, V.; Hanstein, T.; Skripitz, R. Projections of primary hip arthroplasty in Germany until 2040. Acta Orthop. 2018, 89, 308–313. [Google Scholar] [CrossRef] [Green Version]
- Inacio, M.C.S.; Graves, S.E.; Pratt, N.L.; Roughead, E.E.; Nemes, S. Increase in Total Joint Arthroplasty Projected from 2014 to 2046 in Australia: A Conservative Local Model with International Implications. Clin. Orthop. Relat. Res. 2017, 475, 2130–2137. [Google Scholar] [CrossRef] [Green Version]
- Nemes, S.; Gordon, M.; Rogmark, C.; Rolfson, O. Projections of total hip replacement in Sweden from 2013 to 2030. Acta Orthop. 2014, 85, 238–243. [Google Scholar] [CrossRef] [Green Version]
- Kurtz, S.M.; Lau, E.; Ong, K.; Zhao, K.; Kelly, M.; Bozic, K.J. Future young patient demand for primary and revision joint replacement: National projections from 2010 to 2030. Clin. Orthop. Relat. Res. 2009, 467, 2606–2612. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sloan, M.; Premkumar, A.; Sheth, N.P. Projected Volume of Primary Total Joint Arthroplasty in the U.S., 2014 to 2030. J. Bone Jt. Surg. Am. 2018, 100, 1455–1460. [Google Scholar] [CrossRef] [PubMed]
- Rupp, M.; Lau, E.; Kurtz, S.M.; Alt, V. Projections of Primary TKA and THA in Germany from 2016 through 2040. Clin. Orthop. Relat. Res. 2020, 478, 1622–1633. [Google Scholar] [CrossRef]
- Day, J.S.; Lau, E.; Ong, K.L.; Williams, G.R.; Ramsey, M.L.; Kurtz, S.M. Prevalence and projections of total shoulder and elbow arthroplasty in the United States to 2015. J. Shoulder Elbow Surg. 2010, 19, 1115–1120. [Google Scholar] [CrossRef] [PubMed]
- Padegimas, E.M.; Maltenfort, M.; Lazarus, M.D.; Ramsey, M.L.; Williams, G.R.; Namdari, S. Future patient demand for shoulder arthroplasty by younger patients: National projections. Clin. Orthop. Relat. Res. 2015, 473, 1860–1867. [Google Scholar] [CrossRef] [Green Version]
- Kim, S.H.; Wise, B.L.; Zhang, Y.; Szabo, R.M. Increasing incidence of shoulder arthroplasty in the United States. J. Bone Jt. Surg. Am. 2011, 93, 2249–2254. [Google Scholar] [CrossRef] [PubMed]
- Coleman, D.; Rowthorn, R. Who’s afraid of population decline? A critical examination of its consequences. Popul. Dev. Rev. 2011, 37, 217–248. [Google Scholar] [CrossRef]
- Bengtsson, T.; Scott, K. Population aging and the future of the welfare state: The example of Sweden. Popul. Dev. Rev. 2011, 37, 158–170. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lübbeke, A.; Rees, J.L.; Barea, C.; Combescure, C.; Carr, A.J.; Silman, A.J. International variation in shoulder arthroplasty. Acta Orthop. 2017, 88, 592–599. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Klug, A.; Gramlich, Y.; Wincheringer, D.; Schmidt-Horlohé, K.; Hoffmann, R. Trends in surgical management of proximal humeral fractures in adults: A nationwide study of records in Germany from 2007 to 2016. Arch. Orthop. Trauma Surg. 2019, 139, 1713–1721. [Google Scholar] [CrossRef] [PubMed]
- Luciani, P.; Farinelli, L.; Procaccini, R.; Verducci, C.; Gigante, A. Primary reverse shoulder arthroplasty for acute proximal humerus fractures: A 5-year long term retrospective study of elderly patients. Injury 2019, 50, 1974–1977. [Google Scholar] [CrossRef]
- Ferrel, J.R.; Trinh, T.Q.; Fischer, R.A. Reverse total shoulder arthroplasty versus hemiarthroplasty for proximal humeral fractures: A systematic review. J. Orthop. Trauma 2015, 29, 60–68. [Google Scholar] [CrossRef] [PubMed]
- Jonsson, E.Ö.; Ekholm, C.; Salomonsson, B.; Demir, Y.; Olerud, P. Reverse total shoulder arthroplasty provides better shoulder function than hemiarthroplasty for displaced 3- and 4-part proximal humeral fractures in patients aged 70 years or older: A multicenter randomized controlled trial. J. Shoulder Elbow Surg. 2021, 30, 994–1006. [Google Scholar] [CrossRef]
- Gauci, M.-O.; Cavalier, M.; Gonzalez, J.-F.; Holzer, N.; Baring, T.; Walch, G.; Boileau, P. Revision of failed shoulder arthroplasty: Epidemiology, etiology, and surgical options. J. Shoulder Elbow Surg. 2020, 29, 541–549. [Google Scholar] [CrossRef]
- DIMDI. Systematisches Verzeichnis—Operationen-und Prozedurenschlüssel—Internationale Klassifikation der Prozeduren in der Medizin (OPS); DIMDI unter Beteiligung der Arbeitsgruppe OPS des Kuratoriums für Fragen der Klassifikation im Gesundheitswesen (KKG): Cologne, Germany, 2010–2019.
- Pötzsch, O.R.F. Demographic Analyses, Methods and Projections, Births and Deaths: Germany’s Population by 2060—Results of the 13th Coordinated Population Projection; Federal Statistical Office of Germany: Wiesbaden, Germany, 2015.
- Bliemel, F. Theil’s Forecast Accuracy Coefficient: A Clarification. J. Mark. Res. 1973, 10, 444. [Google Scholar] [CrossRef]
- Hollatz, M.F.; Stang, A. Nationwide shoulder arthroplasty rates and revision burden in Germany: Analysis of the national hospitalization data 2005 to 2006. J. Shoulder Elbow Surg. 2014, 23, e267–e274. [Google Scholar] [CrossRef]
- Harjula, J.N.E.; Paloneva, J.; Haapakoski, J.; Kukkonen, J.; Äärimaa, V. Increasing incidence of primary shoulder arthroplasty in Finland—A nationwide registry study. BMC Musculoskelet. Disord. 2018, 19, 245. [Google Scholar] [CrossRef] [Green Version]
- Schwartz, B.E.; Savin, D.D.; Youderian, A.R.; Mossad, D.; Goldberg, B.A. National trends and perioperative outcomes in primary and revision total shoulder arthroplasty: Trends in total shoulder arthroplasty. Int. Orthop. 2015, 39, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Wagner, E.R.; Farley, K.X.; Higgins, I.; Wilson, J.M.; Daly, C.A.; Gottschalk, M.B. The incidence of shoulder arthroplasty: Rise and future projections compared with hip and knee arthroplasty. J. Shoulder Elbow Surg. 2020, 29, 2601–2609. [Google Scholar] [CrossRef] [PubMed]
- Nemes, S.; Rolfson, O.; W-Dahl, A.; Garellick, G.; Sundberg, M.; Kärrholm, J.; Robertsson, O. Historical view and future demand for knee arthroplasty in Sweden. Acta Orthop. 2015, 86, 426–431. [Google Scholar] [CrossRef] [Green Version]
- Villatte, G.; Erivan, R.; Barth, J.; Bonnevialle, N.; Descamps, S.; Boisgard, S. Progression and projection for shoulder surgery in France, 2012-2070: Epidemiologic study with trend and projection analysis. Orthop. Traumatol. Surg. Res. 2020, 106, 1067–1077. [Google Scholar] [CrossRef] [PubMed]
- Bayona, C.E.A.; Somerson, J.S.; Matsen, F.A. The utility of international shoulder joint replacement registries and databases: A comparative analytic review of two hundred and sixty one thousand, four hundred and eighty four cases. Int. Orthop. 2018, 42, 351–358. [Google Scholar] [CrossRef]
- García-Fernández, C.; Lopiz, Y.; Rizo, B.; Serrano-Mateo, L.; Alcobía-Díaz, B.; Rodríguez-González, A.; Marco, F. Reverse total shoulder arhroplasty for the treatment of failed fixation in proximal humeral fractures. Injury 2018, 49 (Suppl. 2), S22–S26. [Google Scholar] [CrossRef]
- Court-Brown, C.M.; Garg, A.; McQueen, M.M. The epidemiology of proximal humeral fractures. Acta Orthop. Scand. 2001, 72, 365–371. [Google Scholar] [CrossRef] [Green Version]
- Gallinet, D.; Ohl, X.; Decroocq, L.; Dib, C.; Valenti, P.; Boileau, P. Is reverse total shoulder arthroplasty more effective than hemiarthroplasty for treating displaced proximal humerus fractures in older adults? A systematic review and meta-analysis. Orthop. Traumatol. Surg. Res. 2018, 104, 759–766. [Google Scholar] [CrossRef]
- Noguera, L.; Trigo, L.; Melero, V.; Santana, F.; Torrens, C. Reverse shoulder arthroplasty for acute proximal humeral fractures: Postoperative complications at 7 days, 90 days and 1 year. Injury 2019, 50, 371–375. [Google Scholar] [CrossRef]
- Lindbloom, B.J.; Christmas, K.N.; Downes, K.; Simon, P.; McLendon, P.B.; Hess, A.V.; Mighell, M.A.; Frankle, M.A. Is there a relationship between preoperative diagnosis and clinical outcomes in reverse shoulder arthroplasty? An experience in 699 shoulders. J. Shoulder Elbow Surg. 2019, 28, S110–S117. [Google Scholar] [CrossRef] [PubMed]
- Coscia, A.C.; Matar, R.N.; Espinal, E.E.; Shah, N.S.; Grawe, B.M. Does Preoperative Diagnosis Impact Patient Outcomes Following Reverse Total Shoulder Arthroplasty? A Systematic Review. J. Shoulder Elbow Surg. 2020, 30, 1458–1470. [Google Scholar] [CrossRef] [PubMed]
- Lung, B.E.; Kanjiya, S.; Bisogno, M.; Komatsu, D.E.; Wang, E.D. Preoperative indications for total shoulder arthroplasty predict adverse postoperative complications. JSES Open Access 2019, 3, 99–107. [Google Scholar] [CrossRef] [Green Version]
- Malik, A.T.; Bishop, J.Y.; Neviaser, A.S.; Beals, C.T.; Jain, N.; Khan, S.N. Shoulder Arthroplasty for a Fracture Is Not the Same as Shoulder Arthroplasty for Osteoarthritis: Implications for a Bundled Payment Model. J. Am. Acad. Orthop. Surg. 2019, 27, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Fu, B.-S.; Jia, H.-L.; Zhou, D.-S.; Liu, F.-X. Surgical and Non-Surgical Treatment for 3-Part and 4-Part Fractures of the Proximal Humerus: A Systematic Review of Overlapping Meta-Analyses. Orthop. Surg. 2019, 11, 356–365. [Google Scholar] [CrossRef] [PubMed]
- Soler-Peiro, M.; García-Martínez, L.; Aguilella, L.; Perez-Bermejo, M. Conservative treatment of 3-part and 4-part proximal humeral fractures: A systematic review. J. Orthop. Surg. Res. 2020, 15, 347. [Google Scholar] [CrossRef] [PubMed]
- Hemmann, P.; Ziegler, P.; Konrads, C.; Ellmerer, A.; Klopfer, T.; Schreiner, A.J.; Bahrs, C. Trends in fracture development of the upper extremity in Germany-a population-based description of the past 15 years. J. Orthop. Surg. Res. 2020, 15, 65. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Martinez-Huedo, M.A.; Jiménez-García, R.; Mora-Zamorano, E.; Hernández-Barrera, V.; Villanueva-Martinez, M.; Lopez-de-Andres, A. Trends in incidence of proximal humerus fractures, surgical procedures and outcomes among elderly hospitalized patients with and without type 2 diabetes in Spain (2001-2013). BMC Musculoskelet. Disord. 2017, 18, 522. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Baertl, S.; Alt, V.; Rupp, M. Surgical enhancement of fracture healing—Operative vs. nonoperative treatment. Injury 2020, 52, S12–S17. [Google Scholar] [CrossRef]
- Gomberawalla, M.M.; Miller, B.S.; Coale, R.M.; Bedi, A.; Gagnier, J.J. Meta-analysis of joint preservation versus arthroplasty for the treatment of displaced 3- and 4-part fractures of the proximal humerus. Injury 2013, 44, 1532–1539. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Model | MSE | RMSE | MAPE | U1 | U2 |
|---|---|---|---|---|---|
| Poisson | 48,816.735 | 220.945 | 6.595 | 0.018 | 0.009 |
| B-spline | 19,724.682 | 140.445 | 3.108 | 0.012 | 0.006 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Klug, A.; Herrmann, E.; Fischer, S.; Hoffmann, R.; Gramlich, Y. Projections of Primary and Revision Shoulder Arthroplasty until 2040: Facing a Massive Rise in Fracture-Related Procedures. J. Clin. Med. 2021, 10, 5123. https://doi.org/10.3390/jcm10215123
Klug A, Herrmann E, Fischer S, Hoffmann R, Gramlich Y. Projections of Primary and Revision Shoulder Arthroplasty until 2040: Facing a Massive Rise in Fracture-Related Procedures. Journal of Clinical Medicine. 2021; 10(21):5123. https://doi.org/10.3390/jcm10215123
Chicago/Turabian StyleKlug, Alexander, Eva Herrmann, Sebastian Fischer, Reinhard Hoffmann, and Yves Gramlich. 2021. "Projections of Primary and Revision Shoulder Arthroplasty until 2040: Facing a Massive Rise in Fracture-Related Procedures" Journal of Clinical Medicine 10, no. 21: 5123. https://doi.org/10.3390/jcm10215123
APA StyleKlug, A., Herrmann, E., Fischer, S., Hoffmann, R., & Gramlich, Y. (2021). Projections of Primary and Revision Shoulder Arthroplasty until 2040: Facing a Massive Rise in Fracture-Related Procedures. Journal of Clinical Medicine, 10(21), 5123. https://doi.org/10.3390/jcm10215123