
Renal Recovery after the Implementation of an Electronic Alert and Biomarker-Guided Kidney-Protection Strategy following Major Surgery

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Patients and Study Design
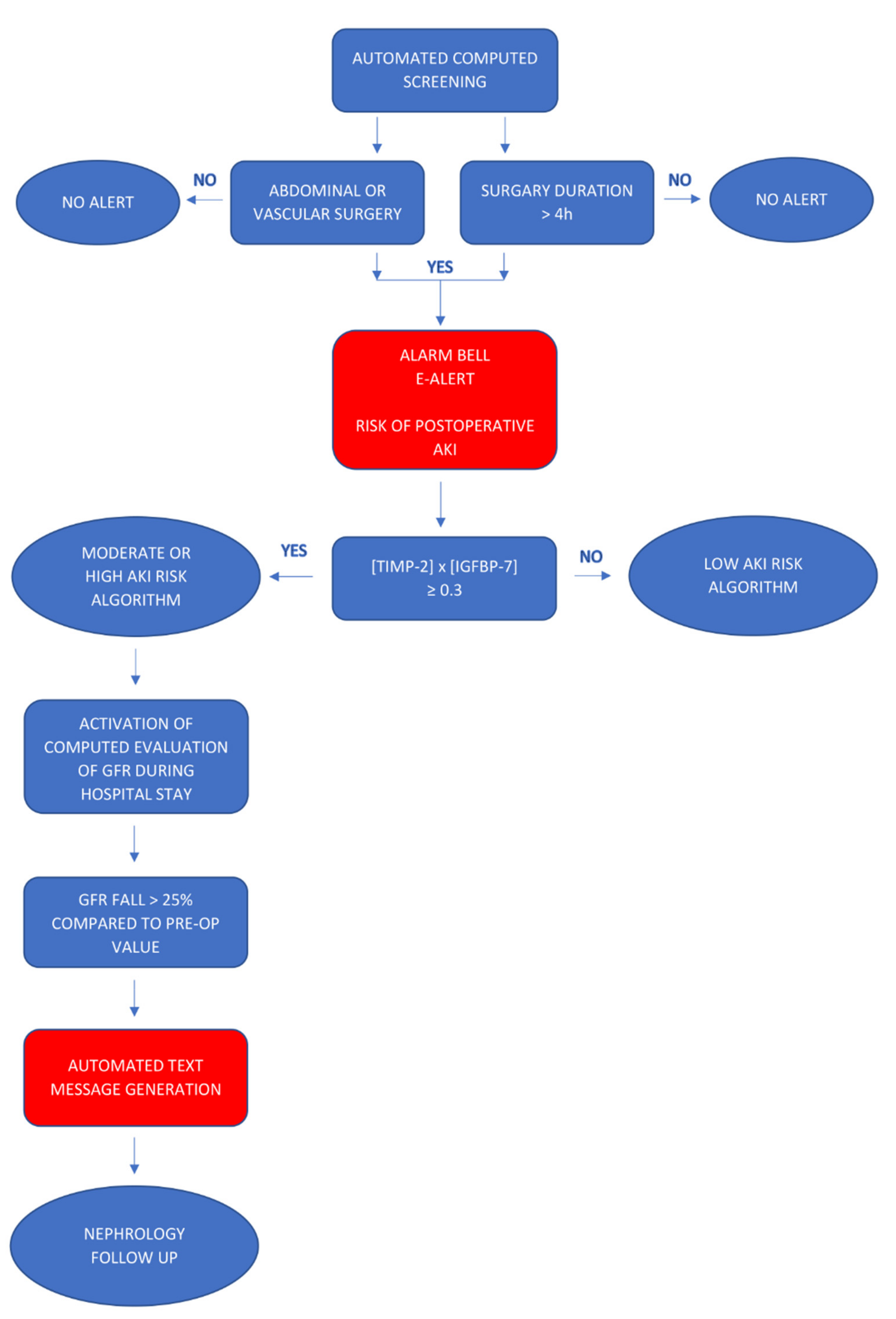
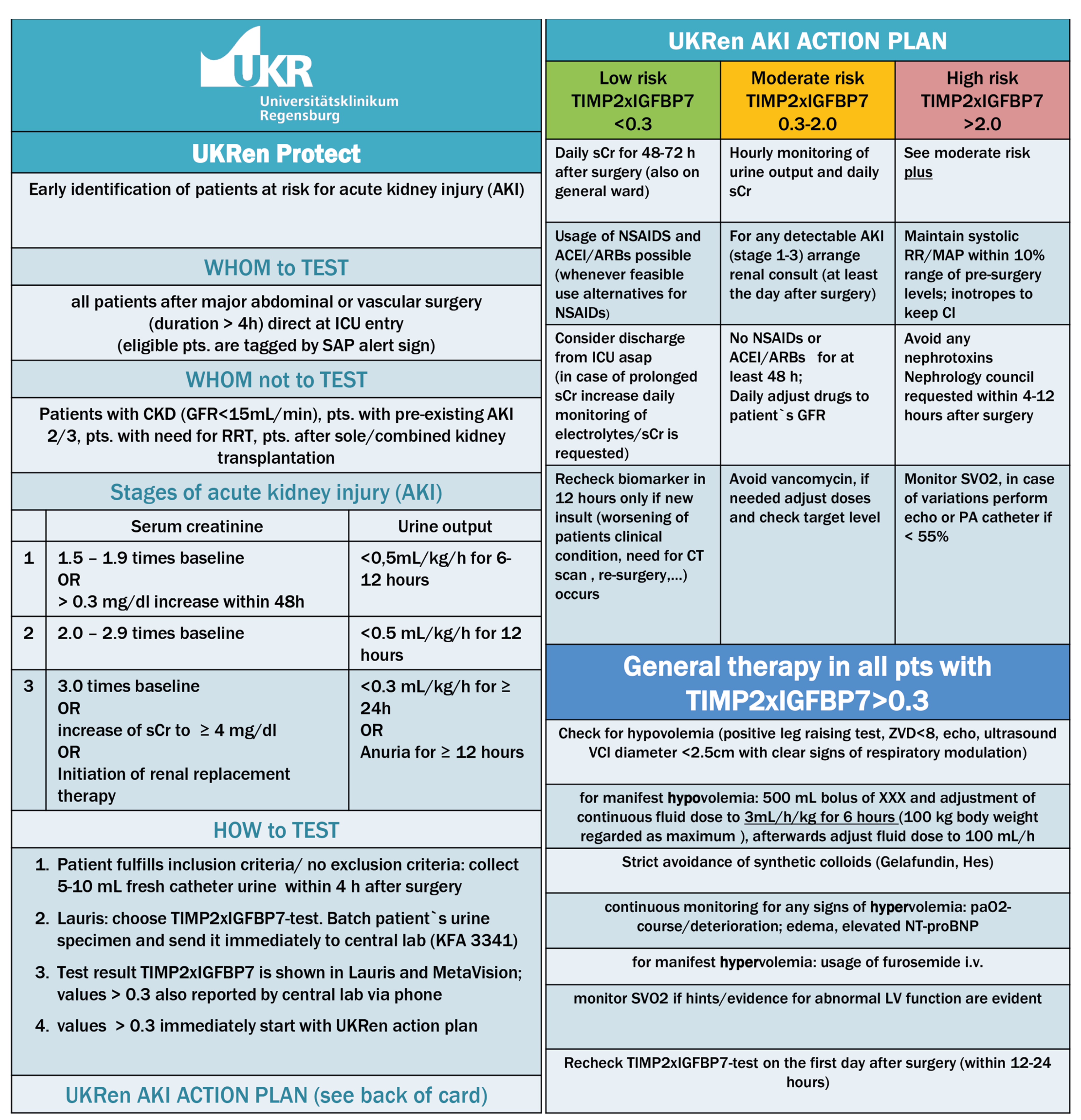
2.2. Electronic Alert and Biomarker-Guided Kidney-Protection Protocol
2.3. Outcomes
2.4. Statistical Analyses
3. Results
3.1. Patient Characteristics
3.2. Clinical Outcomes
3.2.1. Primary Endpoint
3.2.2. Secondary Endpoints
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- O’Connor, M.E.; Hewson, R.W.; Kirwan, C.J.; Ackland, G.L.; Pearse, R.; Prowle, J.R. Acute kidney injury and mortality 1 year after major non-cardiac surgery. BJS 2017, 104, 868–876. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.A.J.; Bagshaw, S.M.; Bellomo, R.; Cely, C.M.; Colman, R.; Cruz, D.N.; Edipidis, K.; Forni, L.G.; Gomersall, C.D.; Govil, D.; et al. Epidemiology of acute kidney injury in critically ill patients: The multinational AKI-EPI study. Intensiv. Care Med. 2015, 41, 1411–1423. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Ozrazgat-Baslanti, T.; Thottakkara, P.; Scali, S.T.; Bihorac, A.; Hobson, C. Cardiovascular-Specific Mortality and Kidney Disease in Patients Undergoing Vascular Surgery. JAMA Surg. 2016, 151, 441–450. [Google Scholar] [CrossRef]
- Vaara, S.T.; Pettilä, V.; Reinikainen, M.; Kaukonen, K.-M.; The Finnish Intensive Care Consortium. Population-based incidence, mortality and quality of life in critically ill patients treated with renal replacement therapy: A nationwide retrospective cohort study in finnish intensive care units. Crit. Care 2012, 16, R13. [Google Scholar] [CrossRef]
- Long, T.E.; Helgason, D.; Helgadottir, S.; Palsson, R.; Gudbjartsson, T.; Sigurdsson, G.H.; Indridason, O.S.; Sigurdsson, M.I. Acute Kidney Injury After Abdominal Surgery: Incidence, Risk Factors, and Outcome. Anesth Analg. 2016, 122, 1912–1920. [Google Scholar] [CrossRef] [PubMed]
- Apel, M.; Maia, V.P.; Zeidan, M.; Schinkoethe, C.; Wolf, G.; Reinhart, K.; Sakr, Y. End-stage renal disease and outcome in a surgical intensive care unit. Crit. Care 2013, 17, R298. [Google Scholar] [CrossRef]
- Iwagami, M.; Yasunaga, H.; Matsui, H.; Horiguchi, H.; Fushimi, K.; Noiri, E.; Nangaku, M.; Doi, K. Impact of end-stage renal disease on hospital outcomes among patients admitted to intensive care units: A retrospective matched-pair cohort study. Nephrology 2016, 22, 617–623. [Google Scholar] [CrossRef]
- Hofhuis, J.G.; Van Stel, H.F.; Schrijvers, A.J.; Rommes, J.H.; Spronk, P.E. The effect of acute kidney injury on long-term health-related quality of life: A prospective follow-up study. Crit. Care 2013, 17, R17. [Google Scholar] [CrossRef]
- Hobson, C.; Ozrazgat-Baslanti, T.; Kuxhausen, A.; Thottakkara, P.; Efron, P.A.; Moore, F.A.; Moldawer, L.L.; Segal, M.S.; Bihorac, A. Cost and Mortality Associated with Postoperative Acute Kidney Injury. Ann. Surg. 2015, 261, 1207–1214. [Google Scholar] [CrossRef]
- Bihorac, A.; Chawla, L.S.; Shaw, A.D.; Al-Khafaji, A.; Davison, D.L.; Demuth, G.E.; Fitzgerald, R.; Gong, M.N.; Graham, D.D.; Gunnerson, K.; et al. Validation of cell-cycle arrest biomarkers for acute kidney injury using clinical adjudication. Am. J. Respir. Crit. Care Med. 2014, 189, 932–939. [Google Scholar] [CrossRef]
- Meersch, M.; Schmidt, C.; Van Aken, H.; Martens, S.; Rossaint, J.; Singbartl, K.; Görlich, D.; Kellum, J.A.; Zarbock, A. Urinary TIMP-2 and IGFBP7 as Early Biomarkers of Acute Kidney Injury and Renal Recovery following Cardiac Surgery. PLoS ONE 2014, 9, e93460. [Google Scholar] [CrossRef]
- Kashani, K.; Al-Khafaji, A.; Ardiles, T.; Artigas, A.; Bagshaw, S.M.; Bell, M.; Bihorac, A.; Birkhahn, R.; Cely, C.M.; Chawla, L.S.; et al. Discovery and validation of cell cycle arrest biomarkers in human acute kidney injury. Crit. Care 2013, 17, R25. [Google Scholar] [CrossRef]
- Johnson, A.C.; Zager, R.A. Mechanisms Underlying Increased TIMP2 and IGFBP7 Urinary Excretion in Experimental AKI. J. Am. Soc. Nephrol. 2018, 29, 2157–2167. [Google Scholar] [CrossRef] [PubMed]
- Lieske, J.C.; Kashani, K.; Kellum, J.; Koyner, J.; Mehta, R.; Parikh, C. Use of Biomarkers to Detect and Manage Acute Kidney Injury: Has Progress Stalled? Clin. Chem. 2020, 66, 271–276. [Google Scholar] [CrossRef] [PubMed]
- Göcze, I.; Jauch, D.; Götz, N.; Kennedy, P.; Jung, B.; Zeman, F.; Gnewuch, C.; Graf, B.M.; Gnann, W.; Banas, B.; et al. Biomarker-guided Intervention to Prevent Acute Kidney Injury after Major Surgery: The Prospective Randomized BigpAK Study. Ann Surg. 2018, 267, 1013–1020. [Google Scholar] [CrossRef] [PubMed]
- Forni, L.G.; Darmon, M.; Ostermann, M.; Straaten, H.M.O.-V.; Pettilä, V.; Prowle, J.; Schetz, M.; Joannidis, M. Renal recovery after acute kidney injury. Intensiv. Care Med. 2017, 43, 855–866. [Google Scholar] [CrossRef]
- Wilson, F.P.; Shashaty, M.; Testani, J.; Aqeel, I.; Borovskiy, Y.; Ellenberg, S.S.; Feldman, H.I.; Fernandez, H.; Gitelman, Y.; Lin, J.; et al. Automated, electronic alerts for acute kidney injury: A single-blind, parallel-group, randomised controlled trial. Lancet 2015, 385, 1966–1974. [Google Scholar] [CrossRef]
- Selby, N.M.; Casula, A.; Lamming, L.; Stoves, J.; Samarasinghe, Y.; Lewington, A.J.; Roberts, R.; Shah, N.; Johnson, M.; Jackson, N.; et al. An Organizational-Level Program of Interventionfor AKI: A Pragmatic Stepped Wedge Cluster Randomized Trial. J. Am. Soc. Nephrol. 2019, 30, 505–515. [Google Scholar] [CrossRef]
- Hobson, C.; Singhania, G.; Bihorac, A. Acute Kidney Injury in the Surgical Patient. Crit. Care Clin. 2015, 31, 705–723. [Google Scholar] [CrossRef]
- Martin, D.; The ESA Study Group; Mantziari, S.; Demartines, N.; Hübner, M. Defining Major Surgery: A Delphi Consensus Among European Surgical Association (ESA) Members. World J. Surg. 2020, 44, 2211–2219. [Google Scholar] [CrossRef]
- Khwaja, A. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. 2012, 120, c179–c184. [Google Scholar] [CrossRef] [PubMed]
- Hoste, E.; McCullough, P.A.; Kashani, K.; Chawla, L.; Joannidis, M.; Shaw, A.D.; Feldkamp, T.; Uettwiller-Geiger, D.L.; McCarthy, P.; Shi, J.; et al. Derivation and validation of cutoffs for clinical use of cell cycle arrest biomarkers. Nephrol. Dial. Transplant. 2014, 29, 2054–2061. [Google Scholar] [CrossRef]
- Guzzi, L.M.; Bergler, T.; Binnall, B.; Engelman, D.T.; Forni, L.; Germain, M.J.; Gluck, E.; Göcze, I.; Joannidis, M.; Koyner, J.L.; et al. Clinical use of [TIMP-2]•[IGFBP7] biomarker testing to assess risk of acute kidney injury in critical care: Guidance from an expert panel. Crit. Care 2019, 23, 1–9. [Google Scholar] [CrossRef]
- Ricci, Z.; Cruz, D.; Ronco, C. TheRifle criteria and mortality in acute kidney injury: A systematic review. Kidney Int. 2008, 73, 538–546. [Google Scholar] [CrossRef]
- Kidney Disease: Improving Global Outcomes (KDIGO) Acute Kidney Injury Work Group. KDIGO Clinical Practice Guideline for Acute Kidney Injury. Kidney Int. Suppl. 2012, 2, 1–138. [Google Scholar]
- Wilson, F.P.; Martin, M.; Yamamoto, Y.; Partridge, C.; Moreira, E.; Arora, T.; Biswas, A.; Feldman, H.; Garg, A.X.; Greenberg, J.H.; et al. Electronic health record alerts for acute kidney injury: Multicenter, randomized clinical trial. BMJ 2021, 372, m4786. [Google Scholar] [CrossRef] [PubMed]
- Ostermann, M.; Zarbock, A.; Goldstein, S.; Kashani, K.; Macedo, E.; Murugan, R.; Bell, M.; Forni, L.; Guzzi, L.; Joannidis, M.; et al. Recommendations on Acute Kidney Injury Biomarkers from the Acute Disease Quality Initiative Consensus Conference A Consensus Statement. JAMA Network Open 2020, 3, e2019209. [Google Scholar] [CrossRef] [PubMed]
- Ugwuowo, U.; Yamamoto, Y.; Arora, T.; Saran, I.; Partridge, C.; Biswas, A.; Martin, M.; Moledina, D.G.; Greenberg, J.H.; Simonov, M.; et al. Real-time prediction of acute kid-ney injury in hospitalized adults: Implementation and proof of concept. Am. J. Kidney Dis. 2020, 76, 806–814.e41. [Google Scholar] [CrossRef]
- Park, S.; Baek, S.H.; Ahn, S.; Lee, K.-H.; Hwang, H.; Ryu, J.; Ahn, S.Y.; Chin, H.J.; Na, K.Y.; Chae, D.-W.; et al. Impact of Electronic Acute Kidney Injury (AKI) Alerts with Automated Nephrologist Consultation on Detection and Severity of AKI: A Quality Improvement Study. Am. J. Kidney Dis. 2018, 71, 9–19. [Google Scholar] [CrossRef] [PubMed]
- Meersch, M.; Schmidt, C.; Hoffmeier, A.; Van Aken, H.; Wempe, C.; Gerss, J.; Zarbock, A. Prevention of cardiac surgery-associated AKI by implementing the KDIGOguidelines in high risk patients identified by biomarkers: The PrevAKI randomized controlled trial. Intensive Care Med. 2017, 43, 1551–1561. [Google Scholar] [CrossRef]
- Kellum, J.A.; Sileanu, F.E.; Bihorac, A.; Hoste, E.A.J.; Chawla, L.S. Recovery after acute kidney injury. Am. J. Respir. Crit. Care Med. 2017, 195, 784–791. [Google Scholar] [CrossRef] [PubMed]
- Gameiro, J.; Duarte, M.; Marques, F.; Fonseca, J.A.; Jorge, S.; Rosa, R.; Lopes, J.A. Transient and Persistent AKI and Outcomes in Patients Undergoing Major Abdominal Surgery. Nephron 2020, 144, 236–244. [Google Scholar] [CrossRef] [PubMed]
- Heung, M.; Steffick, D.E.; Zivin, K.; Gillespie, B.W.; Banerjee, T.; Hsu, C.-Y.; Powe, N.R.; Pavkov, M.E.; Williams, D.E.; Saran, R.; et al. Acute Kidney Injury Recovery Pattern and Subsequent Risk of CKD: An Analysis of Veterans Health Administration Data. Am. J. Kidney Dis. 2016, 67, 742–752. [Google Scholar] [CrossRef]
- Chawla, L.S.; Bellomo, R.; Bihorac, A.; Goldstein, S.L.; Siew, E.D.; Bagshaw, S.M.; Fitzgerald, D.B.R.L.; Fitzgerald, D.B.R.L.; Mehta, D.C.E.M.R.; Mehta, D.C.E.M.R.; et al. Acute kidney disease and renal recovery: Consensus report of the Acute Disease Quality Initiative (ADQI) 16 Workgroup. Nat. Rev. Nephrol. 2017, 13, 241–257. [Google Scholar] [CrossRef]
- Ferenbach, D.; Bonventre, J.V. Mechanisms of maladaptive repair after AKI leading to accelerated kidney ageing and CKD. Nat. Rev. Nephrol. 2015, 11, 264–276. [Google Scholar] [CrossRef]
- Xie, Y.; Ankawi, G.; Yang, B.; Garzotto, F.; Passannante, A.; Breglia, A.; Digvijay, K.; Ferrari, F.; Brendolan, A.; Raffaele, B.; et al. Tissue inhibitor metalloproteinase-2 (TIMP-2) • IGF-binding protein-7 (IGFBP7) levels are associated with adverse outcomes in patients in the intensive care unit with acute kidney injury. Kidney Int. 2019, 95, 1486–1493. [Google Scholar] [CrossRef]
- Koyner, J.L.; Shaw, A.D.; Chawla, L.; Hoste, E.; Bihorac, A.; Kashani, K.; Haase, M.; Shi, J.; Kellum, J.A. Tissue Inhibitor Metalloproteinase-2 (TIMP-2)⋅IGF-Binding Protein-7 (IGFBP7) Levels Are Associated with Adverse Long-Term Outcomes in Patients with AKI. J. Am. Soc. Nephrol. 2014, 26, 1747–1754. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, M.; Kirwan, C.; Pearse, R.; Prowle, J.R. Incidence and associations of acute kidney injury after major abdominal surgery. Intensive Care Med. 2016, 42, 521–530. [Google Scholar] [CrossRef]
- Schefold, J.C.; Filippatos, G.; Hasenfuss, G.; Anker, S.D.; Von Haehling, S. Heart failure and kidney dysfunction: Epidemiology, mechanisms and management. Nat. Rev. Nephrol. 2016, 12, 610–623. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
| Protocol Implementation n = 143 | Historical Control n = 151 | p-Value | |||
|---|---|---|---|---|---|
| Age, median (IQR) | 64 (55–74) | 65 (56–73) | 0.85 | ||
| Sex (%) | Female | Male | Female | Male | |
| 58 (41%) | 85 (59%) | 45 (30%) | 106 (70%) | 0.053 | |
| BMI, median (IQR) | 25 (23–29) | 26 (23–29.5) | 0.365 | ||
| Weight, kg, median (IQR) | 76 (65–86) | 80 (69.5–90) | 0.089 | ||
| SAPS II, median (IQR) | 30 (23–38.5) | 30 (24.25–37.75) | 0.956 | ||
| Preoperative creatinine, mg/dL, median (IQR) | 0.84 (0.7–1.02) | 0.83 (IQR 0.7–0.97) | 0.898 | ||
| Preoperative eGFR (CKD-EPI), mL/min/1.73 qm, median (IQR) | 86 (71–99) | 90 (75–98) | 0.424 | ||
| Comorbidities | |||||
| Chronic cardiac disease | 24 (17%) | 26 (17%) | 0.921 | ||
| Chronic heart failure | 35 (24%) | 17 (11%) | 0.003 | ||
| Arterial hypertension | 70 (49%) | 74 (49%) | 0.992 | ||
| Diabetes mellitus | 29 (20%) | 20 (13%) | 0.106 | ||
| Chronic liver failure | 8 (6%) | 8 (5%) | 0.911 | ||
| Smoking | 16 (11%) | 23 (15%) | 0.307 | ||
| Chronic kidney disease eGFR < 60 mL/min | 37 (26%) | 19 (13%) | 0.004 | ||
| COPD | 8 (6%) | 6 (4%) | 0.514 | ||
| Peripheral vascular disease | 9 (6%) | 24 (16%) | 0.009 | ||
| Malignancy | 92 (64%) | 108 (72%) | 0.187 | ||
| Protocol Implementation n = 143 | Historical Control n = 151 | p-Value | |
|---|---|---|---|
| ASA score preoperative | 0.400 | ||
| ASA 1 | 8 (6%) | 6 (4%) | |
| ASA 2 | 45 (32%) | 46 (31%) | |
| ASA 3 | 85 (59%) | 86 (58%) | |
| ASA 4 | 5 (3%) | 11 (7%) | |
| Type of surgery | |||
| Hepatobiliary surgery | 55 (38%) | 53 (35%) | 0.550 |
| Transplantation | 4 (3%) | 2 (1%) | 0.449 |
| Pancreatic surgery | 21 (15%) | 22 (15%) | 0.978 |
| Upper-GI surgery | 8 (6%) | 6 (4%) | 0.514 |
| Colorectal surgery | 17 (12%) | 26 (17%) | 0.196 |
| Vascular aortic surgery | 11 (8%) | 16 (11%) | 0.389 |
| Vascular other surgery | 9 (6%) | 10 (7%) | 0.909 |
| Multivisceral resection and HIPEC | 12 (8%) | 5 (3%) | 0.062 |
| Multivisceral resection without HIPEC | 8 (6%) | 8 (5%) | 0.911 |
| Other surgery | 0 (0%) | 1 (1%) | 0.330 |
| Duration | |||
| Duration of surgery (minutes) | 295 (IQR 233.5–381) | 300 (IQR 219–384.5) | 0.741 |
| Duration of anesthesia (minutes) | 365 (IQR 310.5–463.5) | 380 (IQR 298.5–473) | 0.951 |
| Protocol Implementation n = 143 | Historical Control n = 151 | Effect Estimate (95% CI) * | p-Value | |
|---|---|---|---|---|
| Primary outcome | ||||
| Recovery of kidney function in 7 days | 36/46 (78%) | 27/48 (56%) | 0.36 (0.14, 0.86) | 0.025 |
| Secondary outcomes | ||||
| Overall AKI (%) in 7 days | 46 (32%) | 48 (32%) | 0.98 (0.6, 1.61) | 0.944 |
| AKI stage 2 and 3 in 7 days | 12 (8%) | 18 (12%) | 1.48 (0.69, 3.26) | 0.320 |
| AKI stage 3 and dialysis in 7 days | 2 (1%) | 7 (5%) | 3.43 (0.70, 16.8) | 0.129 |
| ICU length of stay, median (IQR) days | 3 (1–4.5) | 3 (2–6) | 0.30 (0.16, 0.42) | <0.001 |
| Hospital length of stay, median (IQR) days | 14 (11–22) | 13 (9–18.5) | −0.12 (−0.24, 0.02) | 0.083 |
| RRT-free days (SD) in 7 days ** | 6.91 (0.46) | 6.33 (1.7) | −0.58 (−1.09, −0.07) | 0.027 |
| In-hospital mortality | 6 (4%) | 10 (7%) | 1.62 (0.59, 4.87) | 0.363 |
| Any AKI > 7 days | 6 (4%) | 9 (6%) | 1.45 (0.51,4.42) | 0.494 |
| AKI stage 2 and 3 (%) > 7 days | 2 (1%) | 4 (3%) | 1.92 (0.37,13.99) | 0.456 |
| Any in-hospital AKI (%) | 48 (34%) | 57 (38%) | 1.20 (0.74, 1.94) | 0.455 |
| Any in-hospital AKI stage 2 and 3 (%) | 14 (10%) | 22 (15%) | 1.57 (0.77, 3.21) | 0.214 |
| Odds Ratio (95%-CI) | p-Value | |
|---|---|---|
| Primary outcome | ||
| Recovery of kidney function in 7 days | 0.35 (0.13, 0.90) | 0.029 |
| Secondary Outcomes | ||
| Overall AKI in 7 days | 1.11 (0.66, 1.87) | 0.697 |
| AKI stage 2 and 3 in 7 days | 1.79 (0.78, 4.07) | 0.167 |
| AKI stage 3 and dialysis in 7 days | 3.60 (0.62, 20.84) | 0.153 |
| In-hospital mortality | 2.22 (0.70, 7.00) | 0.175 |
| Any AKI stage > 7 days | 1.68 (0.54, 5.25) | 0.370 |
| AKI stage 2 and 3 > 7 days | 1.94 (0.29, 13.03) | 0.497 |
| Total in-hospital AKI | 1.32 (0.80, 2.20) | 0.283 |
| Total in-hospital AKI stage 2 and 3 | 2.08 (0.95, 4.54) | 0.066 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Halmy, L.; Riedel, J.; Zeman, F.; Tege, B.; Linder, V.; Gnewuch, C.; Graf, B.M.; Schlitt, H.J.; Bergler, T.; Göcze, I. Renal Recovery after the Implementation of an Electronic Alert and Biomarker-Guided Kidney-Protection Strategy following Major Surgery. J. Clin. Med. 2021, 10, 5122. https://doi.org/10.3390/jcm10215122
Halmy L, Riedel J, Zeman F, Tege B, Linder V, Gnewuch C, Graf BM, Schlitt HJ, Bergler T, Göcze I. Renal Recovery after the Implementation of an Electronic Alert and Biomarker-Guided Kidney-Protection Strategy following Major Surgery. Journal of Clinical Medicine. 2021; 10(21):5122. https://doi.org/10.3390/jcm10215122
Chicago/Turabian StyleHalmy, Laszlo, Joshua Riedel, Florian Zeman, Birgit Tege, Volker Linder, Carsten Gnewuch, Bernhard M. Graf, Hans J. Schlitt, Tobias Bergler, and Ivan Göcze. 2021. "Renal Recovery after the Implementation of an Electronic Alert and Biomarker-Guided Kidney-Protection Strategy following Major Surgery" Journal of Clinical Medicine 10, no. 21: 5122. https://doi.org/10.3390/jcm10215122
APA StyleHalmy, L., Riedel, J., Zeman, F., Tege, B., Linder, V., Gnewuch, C., Graf, B. M., Schlitt, H. J., Bergler, T., & Göcze, I. (2021). Renal Recovery after the Implementation of an Electronic Alert and Biomarker-Guided Kidney-Protection Strategy following Major Surgery. Journal of Clinical Medicine, 10(21), 5122. https://doi.org/10.3390/jcm10215122