Abstract
The clinical indications and added value of obtaining MRI in the acute phase of spinal cord injury (SCI) remain controversial. This review aims to critically evaluate evidence regarding the role of MRI to influence decision-making and outcomes in acute SCI. A systematic review and meta-analysis were performed according to PRISMA methodology to identify studies that address six key questions (KQs) regarding diagnostic accuracy, frequency of abnormal findings, frequency of altered decision-making, optimal timing, and differences in outcomes related to obtaining an MRI in acute SCI. A total of 32 studies were identified that addressed one or more KQs. MRI showed no adverse events in 156 patients (five studies) and frequently identified cord compression (70%, 12 studies), disc herniation (43%, 16 studies), ligamentous injury (39%, 13 studies), and epidural hematoma (10%, two studies), with good diagnostic accuracy (seven comparative studies) except for fracture detection. MRI findings often altered management, including timing of surgery (78%, three studies), decision to operate (36%, 15 studies), and surgical approach (29%, nine studies). MRI may also be useful to determine the need for instrumentation (100%, one study), which levels to decompress (100%, one study), and if reoperation is needed (34%, two studies). The available literature consistently concluded that MRI was useful prior to surgical treatment (13 studies) and after surgery to assess decompression (two studies), but utility before/after closed reduction of cervical dislocations was unclear (three studies). One study showed improved outcomes with an MRI-based protocol but had a high risk of bias. Heterogeneity was high for most findings (I2 > 0.75). MRI is safe and frequently identifies findings alter clinical management in acute SCI, although direct evidence of its impact on outcomes is lacking. MRI should be performed before and after surgery, when feasible, to facilitate improved clinical decision-making. However, further research is needed to determine its optimal timing, effect on outcomes, cost-effectiveness, and utility before and after closed reduction.
1. Introduction
Traumatic injury to the spine is common and can have devastating consequences when resulting in spinal cord injury (SCI). Acute SCI has an estimated incidence of 750 cases per million annually, often affecting younger individuals and resulting in a substantial impact upon families and society [1]. Evidence-based management of SCI is primarily focused on the acute period, including careful immobilization and transport, avoidance of hypotension and hypoxia, and early surgical decompression [2,3,4,5].
Imaging plays a critical role in the initial evaluation of spinal trauma, and computed tomography (CT) has largely supplanted radiography in modern clinical algorithms [6]. CT is widely available and can quickly screen trauma patients for numerous injuries (head, spine, thorax, and abdomen), but the visualization of the spinal soft tissues is poor, including the spinal cord, intervertebral discs, and ligaments. In contrast, magnetic resonance imaging (MRI) provides detailed views of these structures, allowing detection of spinal cord compression, acute disc herniation, ligamentous injury, and epidural hemorrhage. However, MRI has not been widely incorporated into trauma protocols due to concerns over safety, availability, inconvenience, cost, time required, and the argument that MRI findings rarely change clinical decision-making. Surprisingly, in spite of numerous manuscripts investigating MRI in spinal trauma and SCI, high-quality studies that compare clinical decision-making with and without MRI are lacking [6,7,8]. The American Association of Neurological Surgeons (AANS) and Congress of Neurological Surgeons (CNS) published guidelines for acute cervical spine trauma and SCI in 2002 and updated these in 2013, but offered limited recommendations regarding the use of MRI beyond its utility for cervical collar clearance—no recommendations on the use of MRI in adult patients with SCI were offered [6]. A systematic review performed by Bozzo et al. (2011) [8] took a broader approach in evaluating the clinical utility of MRI, by considering various indirect lines of evidence; based on low-quality evidence, the authors offered a weak recommendation that MRI be performed in all patients with SCI when feasible, to direct management [8]. More recently, a multi-disciplinary group sponsored by AOSpine, AANS/CNS, and Ontario Neurotrauma Foundation developed clinical practice guidelines (CPGs) on five controversial topics in SCI that included a similarly weak recommendation based on very weak evidence that MRI should be used when feasible, to guide clinical decision-making in SCI [9]. However, this CPG was primarily based on expert opinion, as the systematic review that formed its evidentiary basis found only one study that examined MRI for clinical decision-making, and it had a high risk of bias due to methodological issues [7,10]. Overall, the efforts to synthesize the evidence have not provided sufficient guidance on the routine use of MRI in acute SCI; as a result, clinical practice among spinal surgeons and other clinicians remains highly variable.
The overarching aim of this review was to determine if performing an MRI in the acute phase of SCI yields useful clinical information, leading to improvements in patient care and outcomes. However, in view of previous reviews that revealed the paucity of literature directly addressing this question, we aimed to perform a more inclusive review seeking indirect evidence that answers the key questions (KQs) listed in Table 1. Hence, our review aims to synthesize the available direct and indirect evidence regarding the utility of MRI, to guide decision-making in the acute phase of SCI.

Table 1.
Key Questions of Systematic Review.
2. Materials and Methods
The systematic review was designed in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) and the Cochrane Handbook of Systematic Reviews of Interventions [11,12,13].
Only studies with human subjects published in the English language were included, with the search confined to randomized controlled trials (RCTs), cohort studies, case series, and case-control studies. Reviews, opinion articles, case reports, and case series with less than ten patients were excluded. A summary of the study’s design in PICO format (population, intervention, comparison, outcome), including inclusion and exclusion criteria, is found in Table 2. Studies of interest were those that included adults (16 years or older) with SCI in the acute phase (within 7 days of injury). Relevant studies that also included a small proportion of pediatric patients (<20%) were allowed after consideration by the authors, but were marked with an asterisk (*) in all tables. Relevant studies were required to utilize MRI in the acute phase (within 7 days) for the purpose of clinical decision-making (Table 1). Investigations that only examined the role of MRI for prognostication were excluded. The outcomes of interest were selected a priori based on previous studies, and are specified as KQs 1–6 listed in Table 1.
Table 2.
PICO Summary of Inclusion and Exclusion Criteria.
For KQ1, studies were only included if they calculated the diagnostic accuracy of MRI in reference to a gold standard measure (e.g., intraoperative findings) for the detection of specific pathological entities (spinal cord compression, disc herniation, ligamentous injury, epidural hematoma, fracture, or a spinal cord lesion/edema/contusion in the context of SCI without radiologic abnormality [SCIWORA]). For KQ2, studies were included that simply reported the frequency of abnormal MRI findings among the entities included in KQ1. For KQ3, studies were included if they examined how often obtaining an MRI alters clinical decision-making in SCI, including if surgery is required, when to operate, surgical approach, the need for instrumentation, which levels to decompress, or the need for reoperation after surgery. Comparative studies were also included that evaluated differences in decision-making between groups that did and did not undergo MRI. For KQ4, studies were included that reported data on the optimal timing of MRI in acute SCI, including before or after closed reduction, before or after surgery, within a certain time period, or studies that compared differences in timing of MRI between groups. Regarding KQ5, studies that reported the frequency of adverse events when performing MRI in SCI were included. Finally, for KQ6, comparative studies were included that evaluated differences in outcomes (neurological, functional, health-related quality of life) between patients that received an MRI versus those that did not.
Medical subheadings (MeSH) and text words related to acute spinal cord injury and magnetic resonance imaging were utilized for the search strategy. Medline, Embase, and Cochrane Central Register for Controlled Trials (CENTRAL, Wiley interface) were searched. A first search was performed between 1 January 1980 to 30 April 2016. The project was subsequently postponed, and a second search from 1 January 2016 to 26 August 2020 was completed with some overlap in dates to ensure no relevant studies were missed. The starting year of 1980 for the search was based on the timing of the first clinical MRI manuscripts being published in the 1980s [14]. In relevant literature and reviews, references were manually searched for additional studies, while use of Embase ensured gray literature was also screened. Other than dates, no database search limitations were utilized. The Appendix A provides the search protocols, including keywords. Specific search strategies were developed under guidance of library/information scientists with expertise in systemic review searches. Search results were imported to EndNote (Clarivate Analytics, Philadelphia, PA, USA) for the first search and Covidence (Covidence A/S, Melbourne, Australia) for the second search, to reduce data entry errors and bias (i.e., deduplicating references). All investigation reports were assessed for inconsistencies (e.g., design description, outcome presentation, total patients analyzed).
Two authors independently screened all titles and abstracts based on the eligibility criteria. Two authors reviewed each manuscript in full-text for inclusion, to assess eligibility for final inclusion and data extraction. Any discordances between reviewers during the abstract screening, full-text screening, or data-extraction phases were resolved with discussion and review by a third author. In compliance with recommendations from the Cochrane Handbook for Systematic Reviews of Interventions, the following data were compiled into a Microsoft Excel spreadsheet: author, publication year, journal citation, setting, inclusion and exclusion criteria, study design, study population, KQs addressed, and outcomes.
Data were placed into tables stratified by the KQ, enabling qualitative assessment. For simplicity, studied populations were categorized as SCIWORA when CT or radiographs showed no evidence of traumatic injury; otherwise, they were labeled as SCI (i.e., including cases with fracture or malalignment). For quantitative outcome data that were similarly reported across studies and their populations, a meta-analysis was conducted to calculate pooled results. In these cases, a chi-squared test for heterogeneity was performed and the I2 statistic was calculated. Analysis was conducted using R v4.0.2 Statistical Software (R Foundation for Statistical Computing, Vienna, Austria) [15].
Two authors independently performed risk of bias assessment according to the National Institutes of Health (NIH) Quality Assessment Tool [16]. Studies appraised as good had minimally low risk of bias, studies appraised as fair had moderately low risk of bias, and those appraised as poor had high risk of bias.
3. Results
The two electronic database searches yielded a total of 21,323 unique citations (Figure 1). After title and abstract review, 268 manuscripts were selected. Following full-text review, 32 studies were identified that met eligibility criteria and were included in the qualitative synthesis in the form of Table 3, Table 4, Table 5, Table 6, Table 7 and Table 8. Three studies were prospective, while the remainder were retrospective case series, cohort studies, or case-control studies (Table 9). Risk of bias assessment found a high risk of bias in two studies, moderately low in 17, and minimally low in 13 (Table 9).
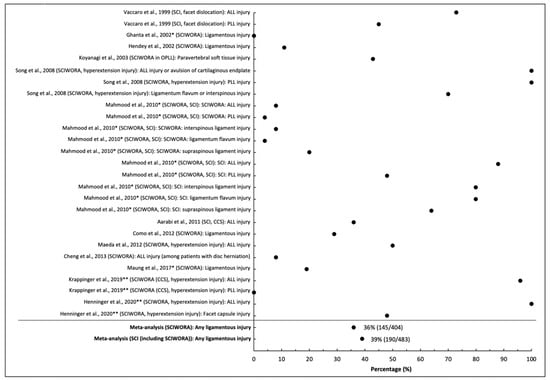
Figure 1.
Frequency of ligamentous injury on MRI in patients with acute spinal cord injury. * Studies that include pediatric patients (<16) or unspecified age range. ** Studies with overlapping cohorts.
Table 3.
Key Question 1: What is the diagnostic accuracy of MRI to detect specific features of spinal injury that are likely to alter clinical management in patients with acute SCI.
Table 4.
Key Question 2: What is the frequency of abnormal MRI findings of specific features of spinal injury that are likely to alter clinical management in patients with acute SCI?
Table 5.
Key Question 3: How often does obtaining an MRI alter clinical decision-making in acute SCI.
Table 6.
Key Question 4: When should MRI be performed in acute spinal cord injury?
Table 7.
Key Question 5: What is the frequency of adverse events when performing MRI in acute SCI patients?
Table 8.
Key Question 6: How does obtaining an MRI (compared with not obtaining MRI) affect neurological, functional, and health-related quality of life outcomes? (Differences in outcome between patients receiving MRI and those not receiving MRI.).
Table 9.
Risk of bias assessment. Studies arranged alphabetically by the last name of the first author. Risk of bias assessment was performed according to the National Institutes of Health (NIH) Quality Assessment Tool. Studies appraised as good had minimally low risk of bias, studies appraised as fair had moderately low risk of bias, and those appraised as poor had high risk of bias.
3.1. KQ1: Diagnostic Accuracy of MRI
Seven studies involving SCI were identified that addressed KQ1 (Table 3) [17,18,19,20,21,22,23]. Five studies calculated the diagnostic accuracy of MRI in relation to intraoperative findings [17,18,19,22,23], one compared against flexion/extension radiographs [20], and one against CT myelography [21]. Two studies with overlapping cohorts focused on hyperextension injuries and central cord syndrome [17,18]; both studies investigated detection of ALL injury, demonstrating superior sensitivity of STIR over T2-weighted (T2w) images (88% vs. 61%) [18] and a specialized MRI radiologist over a general radiologist (86% vs. 68%) [17]. In addition, one study also reported improved sensitivity of STIR over T2w images (82% vs. 61%) to identify intervertebral disc injury/herniation [18]. Two studies found 2 and 5 cases, respectively, of acute disc herniation on MRI that were verified by intraoperative findings [22,23]. Another study investigated the diagnostic accuracy of T2w images to detect intramedullary hemorrhage/contusion/edema in patients with SCIWORA compared with direct visualization of the spinal cord, reporting a sensitivity of 100% [19]. One study compared MRI against flexion/extension radiographs for segmental instability [20]; the MRI finding of ALL injury was present in 23/28 patients with instability (sensitivity: 0.82) and absent in 39/60 patients without instability (specificity: 0.65), while the finding of disc injury was present in 18/28 patients with instability (sensitivity: 0.64) and absent in 41/60 patients without instability (specificity: 0.68). One study found that MRI had only 40% (2/5) sensitivity to detect fracture, but 100% specificity (14/14) compared with CT myelography [21]. Meta-analysis was not possible for KQ1 findings due to the limited data available.
3.2. KQ2: Frequency of Abnormal Findings
Overall, 28 studies relevant to KQ2 were identified, reporting the frequency of certain pathological MRI findings in various types of SCI (Table 4) [17,18,19,20,21,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45].
3.2.1. Ligamentous Injury
Thirteen studies provided data on the frequency of ligamentous injury, all in patients with cervical SCI [17,18,20,24,25,26,27,28,29,34,37,41,43]. Among these studies, nine focused on patients with SCIWORA, in which the frequency of ligamentous injury ranged from 0 to 100% [20,24,25,26,27,28,34,37,41]. The pooled frequency of ligamentous injury in SCIWORA was 36% (145/404 across eight studies excluding [18] due to overlapping cohort with [17]), but heterogeneity across studies was high (I2 = 0.94, p < 0.001). Similarly, the pooled frequency of ligamentous injury was 39% in all patients with SCI (190/483 across 12 studies), with high heterogeneity (I2 = 0.93, p < 0.001; Figure 1).
3.2.2. Disc Injury/Herniation
Sixteen studies provided data on the frequency of disc herniation and/or injury in SCI, including 15 in cervical injuries and one including all spinal levels [20,21,23,25,26,27,28,30,31,32,33,37,41,42,43,44]. The rate of disc injury ranged from 4% to 42% in studies involving cervical SCIWORA, whereas it was 40% to 88% in other SCI studies [20,21,23,25,26,27,28,30,31,32,33,37,41,42,43,44]. Disc herniation was present in 37% to 100% of patients with SCIWORA, whereas it was present in 24% to 100% in SCI [20,21,23,25,26,27,28,30,31,32,33,37,41,42,43,44]. Disc herniation causing cord compression varied from 3% to 83% in two studies involving SCI [23,30]. In SCIWORA, the aggregate rate of disc injury was 20% (46/230), while disc herniation was more frequent at 45% (102/229); both results showed high heterogeneity across studies (I2 = 0.96, 0.84, respectively, both p < 0.001). The pooled frequency of disc injury, disc herniation, and disc herniation causing cord compression across all studies (SCIWORA and SCI) was 26% (71/278), 43% (159/370), and 16% (12/74), respectively, while heterogeneity was high for all analyses (I2 = 0.95, 0.83, and 0.98, respectively, all p < 0.001; Figure 2).
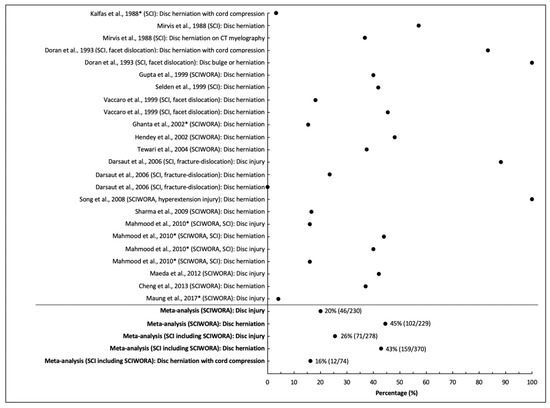
Figure 2.
Frequency of disc injury or herniation on MRI in patients with acute spinal cord injury. * Studies that include pediatric patients (<16) or unspecified age range.
3.2.3. Cord Compression
Twelve studies reported the frequency of ongoing spinal cord compression in SCI, including nine that included only cervical injuries, two that had sub-axial injuries (C3-T1), and one that included all levels [23,24,25,29,30,31,33,34,38,39,41,44]. A cohort examining sub-axial SCI found cord compression frequency at 89% (63/71) with a T1w sagittal sequence, but 92% (65/71) with T2w sagittal and 96% (68/71) when either result was positive [38]. In SCIWORA, cord compression was identified in 0% to 100% of patients in five studies [24,25,33,34,41]. In two studies involving cervical dislocations, cord compression was noted in 65% to 83% [30,31]. For fracture-dislocation patients, cord compression frequency was 65% (11/17) pre-traction, but 12% (2/17) post-traction according to one study [31]. The pooled frequency of cord compression across studies in patients with SCIWORA was 41% (47/116), whereas it was 70% (413/589) among all cases of SCI; heterogeneity across studies was high in both groups (I2 = 0.94, 0.95, respectively, both p < 0.001; Figure 3).
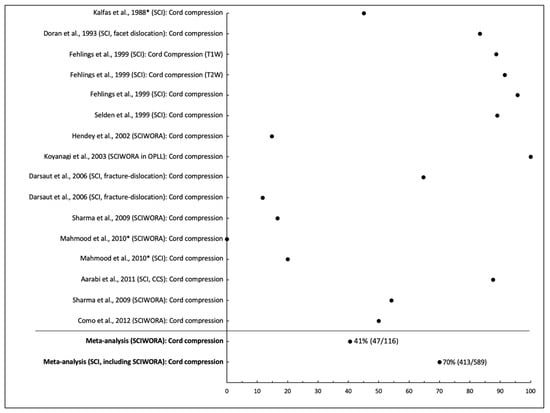
Figure 3.
Frequency of cord compression on MRI in patients with acute spinal cord injury. * Studies that include pediatric patients (<16) or unspecified age range.
3.2.4. Epidural Hematoma
Three investigations in cervical SCI reported epidural hematoma in 3% to 27% of patients, resulting in a pooled frequency of 10% (20/198) [26,39,44]; the results showed high heterogeneity (I2 = 0.92, p < 0.001; Figure 4).
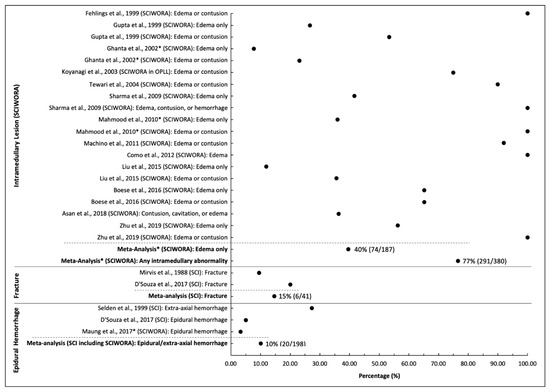
Figure 4.
Frequency of Epidural Hemorrhage, Fracture, and Intramedullary Lesions (SCIWORA) on MRI in patients with acute spinal cord injury. * Studies that include pediatric patients (<16) or unspecified age range.
3.2.5. Fracture
Two small studies provided data on the frequency of identifying fractures in patients with SCI, with a range of 10% to 20% and a pooled frequency of 15% (6/41) [21,39]; the results were homogeneous across these two studies, with I2 = 0, p = 0.61 (Figure 4).
3.2.6. Intramedullary Lesions in SCIWORA
Thirteen studies provided data on the frequency of intramedullary signal change in patients with SCIWORA, including 336 cervical injuries and 44 thoracic injuries [19,24,32,33,34,35,36,37,38,40,41,42,45]. The pooled frequency of simple edema was 40% (74/187), while the rate of any intramedullary lesion (including edema, contusion, hemorrhage, or cavitation) was 77% (291/380) [19,24,32,33,34,35,36,37,38,40,41,42,45]; heterogeneity between studies was high (I2 = 0.90, 0.91 respectively, both p < 0.001; Figure 4).
3.3. KQ3: Influence of MRI on Clinical Decision-Making
Twenty studies provided data relevant to KQ3, regarding if surgery is required, surgical approach, when to operate, determining the need for instrumentation, which levels to decompress, and the need for reoperation after surgery, based upon MRI findings in acute SCI (Table 5) [10,17,21,22,23,24,26,28,29,30,31,32,33,37,40,42,44,45,46,47].
3.3.1. If Surgery Is Required
Fifteen studies reported that MRI results directly influenced the decision of whether surgery was required in acute SCI [10,21,22,23,24,26,30,32,33,37,40,42,44,45,46]. Specific MRI findings that reportedly led to the decision for surgical treatment included cord compression, disc herniation, ligamentous injury, instability, and intramedullary edema (in conjunction with cord compression in SCIWORA). The frequency of MRI results reportedly leading to a decision to operate ranged from 3% to 100% across studies, with a pooled average of 36% (223/611) and high heterogeneity across studies (I2 = 0.96, p < 0.001).
3.3.2. Surgical Approach
Nine studies reported on the influence of MRI findings on surgical approach [21,23,28,29,30,33,37,42,44]. Seven studies cited acute disc herniations with cord compression as the rationale for performing anterior surgery, at a rate of 3% to 83% of cases across studies [21,23,30,33,37,42,44]. Two additional studies of SCIWORA noted that MRI dictated surgical approach in all patients requiring surgery (42/211 and 70/70 patients, respectively), listing anterior compression, anterior compression limited to 1–3 segments, and kyphosis as reasons for selecting anterior surgery [28,29]. Overall, MRI was reported to affect the surgical approach in 29% (143/500) of patients in the included studies, with high heterogeneity (I2 = 0.97, p < 0.001).
3.3.3. When to Operate
Three investigations examined the role of MRI in determining when to operate [10,31,44]. In two studies with overlapping datasets, 49% to 52% of patients required emergent surgery due to MRI-documented cord compression [10,44]. Two studies found that after traction/closed reduction, 33% to 82% of patients had good decompression and could undergo delayed surgery to perform definitive fixation [10,31]. Meta-analysis found that MRI affected surgical timing in 78% (65/83) of patients, with high heterogeneity (I2 = 0.84, p = 0.01).
3.3.4. Need for Instrumentation
One study reported on the need for instrumented fusion due to the finding of segmental instability [17]. This study reported that the level of injury in SCIWORA (showing edema on MRI) and any levels showing ligamentous injury on MRI (19/23 patients) or segmental instability intraoperatively (22/23 patients) would be decompressed and fused.
3.3.5. Which Levels to Decompress
A single study reported that MRI findings of edema and ligamentous injury, and intraoperative findings of instability, dictated which level(s) would be decompressed and fused [17].
3.3.6. Need for Re-Operation after Surgery
Two studies reported the use of post-operative MRI to determine if adequate cord compression had been achieved after SCI [29,47]. One study found that 11/28 patients undergoing anterior surgery had residual cord compression, and this finding led to additional posterior surgical decompression [29]. Another study found that 63/184 patients had inadequate decompression following surgery for acute SCI, highlighting the role of cord swelling and the possible need for multi-level laminectomy and expansile duraplasty [47].
3.4. KQ4: When to Perform MRI
Sixteen studies provided data addressing KQ4 (Table 6) [10,22,23,24,26,28,29,30,31,32,33,43,44,45,46,47]. Fourteen studies concluded that MRI was useful during the initial assessment for the purpose of decision-making (related to one or more aspects of KQ3) [10,22,23,24,26,28,29,30,32,33,44,45,46,47]. However, two studies found that MRI prior to closed reduction of cervical facet dislocation was of unclear utility, with one study finding that two patients with pre-reduction disc herniation did not deteriorate after closed reduction [43], while another study similarly reported that 11 patients with pre-reduction cord compression did not deteriorate during closed reduction [31]. In contrast, Selden et al. found acute disc herniation in 10/18 patients with cervical dislocations, prompting a decision for immediate anterior surgery as the authors felt that closed reduction was unsafe [44]. Furthermore, Doran et al. reported neurological complications in three patients undergoing closed reduction of cervical dislocations that did not have pre-reduction MRI, and subsequent MRI showed disc herniations in all cases [30]. Three studies yielded data on MRI after closed-reduction, with two finding that it was helpful to identify ongoing spinal cord compression [31,44], whereas the third study found no neurological deterioration in spite of disc herniations in five of nine patients [43]. Two studies with overlapping cohorts reported that post-operative MRI was useful to identify inadequate decompression of the cord for consideration of re-operation [29,47]. No studies specifically recommended MRI within a set time period, but one study found no difference in the time interval from injury to pre-operative MRI between patients that were completely and incompletely decompressed [47].
3.5. KQ5: Frequency of Adverse Events When Performing MRI
Five investigations reported on frequency of adverse events when performing an MRI in patients with acute SCI (Table 7) [10,22,23,31,44]. Bao et al. examined patients receiving neutral, flexion, and extension MRIs for cervical SCI without fracture and dislocation, and amongst the cohort of 16 patients found no deterioration of neurological functions [22]. Similarly, when closed reduction for cervical dislocation was performed during MRI, no patients (n = 12) experienced permanent neurological deterioration or burning sensations at pin sites [31]. Pooled results found a 0% rate of adverse events (0/156 patients, 95% CI: 0% to 2.4%), with homogeneity across studies (I2 = 0, p = 1).
3.6. KQ6: Effect of MRI on Outcomes
One investigation addressed KQ6, evaluating differences in outcome between 66 patients assigned to an MRI-based treatment protocol (including urgent surgery) and 25 who were not assigned (due to a “contraindication to MRI, the need for an emergent surgical procedure, or the bias of specific admitting attending neurosurgeons regarding the ‘futility’ of emergent surgical treatment”) [10]. In patients assigned to the protocol group, Frankel grade improved from admission in 50%, relative to 24% in the non-protocol group (p < 0.006). Furthermore, eight of 50 patients from the protocol group presenting with complete motor quadriplegia (grade A or B) improved to independent ambulation (grade D or E), compared with none of the 20 reference patients (p = 0.09, Fisher exact test, not reported in original manuscript). MRI protocol patients also had shorter ICU stay (9.9 ± 1.7 days vs. 23.8 ± 3.7 days, p < 0.001) and total length of stay (71.4 ± 5.9 days vs. 99.9 ± 13.1 days, p = 0.02) [10]. Unfortunately, this study was deemed to have a high risk of bias due to non-random assignment to treatment groups and the confounding effect of more urgent spinal cord decompression in the protocol group compared with the reference group.
4. Discussion
This systematic review and meta-analysis addressed the role of MRI to inform clinical decision-making for patients with acute SCI, offering several lines of evidence supporting its use in routine practice. First, obtaining an MRI in the acute phase of SCI appears to be safe, with no adverse events reported in greater than 150 patients across five studies. This finding confirms the safety of obtaining an MRI in acute SCI, in spite of limited monitoring, additional transfers, and positioning the patient flat and supine for 30 to 45 min. MRI also demonstrates good diagnostic accuracy for ligamentous injury, instability, disc injury, disc herniation, and intramedullary tissue changes, albeit in a small number of comparative studies. Despite substantial heterogeneity between manuscripts, it is clear based on the large number of subjects and studies included in this meta-analysis that MRI frequently identified important pathological findings in patients with SCI, including spinal cord compression in 70%, disc herniation in 43%, ligamentous injury in 39%, and epidural hematoma in 10%. In patients with SCIWORA, MRI demonstrated intramedullary signal change in 77%, disc herniation in 45%, cord compression in 41%, and ligamentous injury in 36%. In contrast, evidence for the utility of MRI in detecting fractures in acute SCI was limited, with a low frequency of positive findings (15%) and poor diagnostic accuracy.
In terms of clinical decision-making, a large number of studies were identified that consistently reported evidence of clinical utility, influencing the decision to operate in 36% of patients, surgical approach in 29%, and the timing of surgery in 78%. Limited evidence also suggested that MRI is useful to determine the need for instrumentation, which levels to decompress, and if re-operation is needed for inadequate decompression. In terms of timing of MRI, most studies concluded that MRI should be performed on initial evaluation, prior to surgery. However, in cases of cervical dislocations, the utility of MRI prior to and after closed reduction remained unclear, due to conflicting results between studies regarding both the frequency and clinical significance of disc herniations; some reports suggest that MRI may be useful to avoid secondary injury due to a large disc herniation, but this area requires further study to draw conclusions. Finally, the results of this review confirm that evidence is lacking to directly show if obtaining an MRI improves outcomes; the only study addressing this topic had a high risk of bias due to non-randomized selection and a confounding effect of earlier spinal cord decompression in patients in the MRI-protocol group. Overall, the body of literature offers moderate evidence that (1) MRI is safe in the acute phase of SCI, (2) MRI has good diagnostic accuracy to detect certain features that are potentially useful for decision-making, (3) these features occur frequently, (4) these features often affect clinical decision-making, and (5) MRI should be performed prior to surgical treatment, whenever possible. However, further studies that investigate management decisions and clinical outcomes with and without MRI, the role of MRI in cervical dislocations, the time delay incurred by obtaining an MRI, and the cost-effectiveness of MRI are required to fully define its utility in acute SCI.
The novelty of the current study is that the review was broadly inclusive, looking for both direct and indirect evidence, while focusing narrowly on the topic of the role of MRI to facilitate clinical decision-making in patients with acute SCI. This review involved a comprehensive search of the literature that considered a large number of citations and full-text articles, and was designed to directly answer a common question that faces surgeons when a patient presents with acute SCI: should I get an MRI first, or just proceed directly to the operating room? The 2002 and 2013 AANS/CNS guidelines for the management of SCI also attempted to address the utility of MRI, but circumvented the main topic with only peripheral recommendations that MRI should be used in pediatric patients to assess SCI, or in adults for collar clearance, for the diagnosis of vertebral artery injury, or to assess patients with ankylosing spondylitis or SCIWORA [6]. Subsequently, AOSpine sponsored an effort to develop five guidelines for controversial topics in SCI, including one on the role of MRI in acute SCI, which provided a weak recommendation that MRI should be used in acute SCI to facilitate improved decision-making and prognostication [9]. These recommendations were based on a systematic review by Kurpad et al. (2017), which was unfortunately hampered by restrictive inclusion criteria yielding only one relevant study (which was deemed to have a high risk of bias) regarding the utility of MRI to guide acute SCI management, thus resulting in a vacuum of relevant evidence [7]. Conversely, Bozzo et al. (2011) utilized liberal inclusion criteria, involving the broader population of all spinal trauma, but was less focused and potentially lacked external validity. Furthermore, the review did not explore how individual studies reported changes in management based on MRI results, nor did it explore the importance of MRI in detection of spinal cord compression, which was the most common entity cited in the current review to affect management. In addition, the vast majority of studies included in both Bozzo et al. (2011) and Kurpad et al. (2017) investigated the use of MRI for prognostication, which we feel is of secondary importance, compared to the imperative task of deciding upon and planning surgical treatment. As a result, a knowledge gap currently exists regarding the optimal use of MRI, with highly variable practice patterns between surgeons. In summary, this systematic review provides a focused synthesis of the literature that clarifies the utility of MRI, while highlighting several areas that require further investigation.
SCI is an inherently difficult condition to study, due to profound heterogeneity in demographics, patterns of injury, timing after injury, neurological presentation, biomechanical stability, comorbidities, concomitant injuries, treatments performed, outcome measures, and MRI methods. The current study performed meta-analyses that clearly reflected this heterogeneity, providing aggregate results that may be helpful to provide general insights, but must be interpreted with caution as the frequency of findings varied with several factors. Complicating matters, the literature uses inconsistent definitions of terms such as SCIWORA, which was originally described in the pediatric population based on radiographs, but has increasingly been used to describe adult SCI without CT evidence of trauma (sometimes dubbed SCIWOCTET). Adult SCIWORA is widely felt to be considerably different than pediatric SCIWORA, with the former frequently involving degenerative spondylosis, ossification of posterior longitudinal ligament, and disc herniations, whereas the latter typically involves ligamentous laxity; therefore, it was not surprising that the SCIWORA results presented in this study also showed high heterogeneity. Furthermore, patients presenting with acute SCI frequently have concomitant injuries, hemodynamic instability, altered mental status, and/or undefined neurological deficits, making it difficult to develop recommendations that are universally applicable. However, the findings of this study are sufficiently compelling to suggest that MRI should be obtained during initial assessment of most patients with acute SCI, in the absence of a contraindication.
Looking ahead, further investigations should focus on several areas to elucidate the role of MRI in acute SCI. First, studies are needed that directly compare outcomes with and without MRI, while implementing similar management otherwise. However, it is doubtful that a randomized study can be ethically performed, as there was a perceived lack of equipoise expressed by expert clinicians in a recent guidelines effort [9]. Furthermore, emerging evidence suggests that earlier decompression has an hour-by-hour benefit on outcomes for the first 36 h after injury [48], suggesting that delays incurred in obtaining an MRI may counteract the benefits. Thus, future studies should include an analysis of the timing of surgery and the related impact of obtaining an MRI. On this topic, institutional protocols such as a “Code SCI” that streamline the care of SCI patients to minimize delays in imaging and definitive treatment should be developed [10,49], akin to “Code Stroke” protocols that have transformed stroke care. Future research is required that prospectively investigates the utility of MRI to make specific decisions on the need for surgery, surgical approach, the number of levels of decompression, and the need for instrumentation. Aarabi et al. (2019) demonstrated that decompressing more levels (up to five) with laminectomy showed higher rates of complete spinal cord decompression, likely due to greater alleviation of spinal cord swelling and secondary injury [47]; identifying pre-operative MRI features that predict spinal cord swelling could inform the need for additional levels of decompression and/or expansile duraplasty. In addition, the vast majority of previous studies have focused on cervical SCI, while the utility of MRI in thoracolumbar injuries is poorly defined, such as burst fractures with SCI. Evaluation of the cost-effectiveness of MRI is also needed to justify its widespread use, particularly in health systems and regions with scarce resources. Finally, emerging microstructural MRI techniques that measure specific physical properties such as axonal injury, demyelination, and perfusion should be studied for their potential value in prognostication [50].
This study is subject to several limitations. The systematic review involved two separate literature searches that were conducted using different interfaces and software tools, which occurred because the authors paused the initial project; this could have resulted in missed citations, although the literature search was comprehensive and overlapping dates were used to mitigate this risk. The large number of citations and full-text articles that were reviewed could also lead to errors, but we had multiple authors reviewing at each step to avoid errors. After careful consideration, we also modified the original inclusion criteria to allow studies with a small number of pediatric patients, as we felt that exclusion of certain key studies would result in a failure to identify important evidence; however, this decision potentially degrades the internal validity, as the small number of pediatric patients could mildly influence the overall results. There also exists the possibility of publication bias, which may have influenced our results. Our approach also excluded studies of spinal trauma without SCI or those that did not perform subgroup analyses with and without SCI; this approach omitted a large number of studies that offered substantial data on the diagnostic accuracy of MRI to detect ligamentous injury and fractures; however, we felt that it was essential to focus the current study on the specific clinical population of acute SCI.
5. Conclusions
MRI is safe and frequently identifies important findings with good diagnostic accuracy that alter clinical management in patients with acute SCI of all presentations, and thus, should be utilized when feasible. Therefore, pessimism that some surgeons feel toward obtaining MRI for the purpose of informing decision-making in acute SCI appears to be unjustified. Although the evidence is imperfect and indirect, it confirms the prior CPG recommendation “that MRI be performed in adult patients with acute SCI prior to surgical intervention, when feasible, to facilitate improved clinical decision-making”. Future prospective studies are needed to fully define the utility and cost-effectiveness of MRI in specific types of SCI, to allow for stronger recommendations that improve and standardize clinical practice.
Author Contributions
Conceptualization, A.R.M., N.T. and M.G.F.; Methodology, A.R.M. and L.T.; Formal analysis, A.R.M. and A.G.-R.; Investigation, A.G.-R., J.E.L.-R., C.P., N.T., S.F.L. and M.K.; Data curation, A.G.-R., J.E.L.-R., C.P., N.T., S.F.L., M.K. and A.R.M.; Writing—original draft preparation, A.R.M. and A.G.-R.; Writing—review and editing, A.R.M., A.G.-R. and M.G.F.; Supervision, A.R.M.; Project administration, A.R.M. All authors have read and agreed to the published version of the manuscript.
Funding
Martin received support from Canadian Institutes of Health Research (CIHR) Fellowship (2016–2017) and Neurosurgery Research and Education Foundation (NREF) Clinical Fellowship (2019–2020). Fehlings was supported by the Halbert Chair in Neural Repair and Regeneration (MGF).
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
All data supporting reported results can be found within the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
Pubmed (MEDLINE) Search Strategy
(((magnetic resonance imaging) OR (MRI)) AND (((((((SCI) OR (spinal cord injury)) OR (spinal trauma)) OR (spine fracture)) OR (spine trauma)) OR (cervical fracture)) OR (cervical trauma))) AND ((((((((outcome) OR (recovery)) OR (management)) OR (decision-making)) OR (decision)) OR (surgery)) OR (surgical)) OR (treatment))
Embase Ovid Search Strategy
(magnetic AND resonance AND imaging OR mri) AND (((((((sci OR spinal) AND cord AND injury OR spinal) AND trauma OR spine) AND fracture OR spine) AND trauma OR cervical) AND fracture OR cervical) AND trauma) AND ((outcome OR recovery OR management OR decision) AND making OR decision OR surgery OR surgical OR treatment)
CENTRAL Search Strategy
[Magnetic Resonance Imaging] explode all trees OR MRI AND [Spinal Cord Injuries] explode all trees OR spinal cord injury OR SCI OR spinal trauma OR spine trauma OR spine fracture OR cervical fracture OR cervical trauma AND [Outcome Assessment, Health Care] explode all trees OR outcome OR recovery OR management OR MeSH descriptor: [Clinical Decision-Making] explode all trees OR decision-making OR decision OR MeSH descriptor: [General Surgery] explode all trees OR surgery OR surgical OR treatment OR MeSH descriptor: [Therapeutics] explode all trees.
References
- Wyndaele, M.; Wyndaele, J.J. Incidence, prevalence and epidemiology of spinal cord injury: What learns a worldwide literature survey? Spinal Cord 2006, 44, 523–529. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Vaccaro, A.; Wilson, J.R.; Singh, A.; Cadotte, D.W.; Harrop, J.S.; Aarabi, B.; Shaffrey, C.; Dvorak, M.; Fisher, C.; et al. Early versus Delayed Decompression for Traumatic Cervical Spinal Cord Injury: Results of the Surgical Timing in Acute Spinal Cord Injury Study (STASCIS). PLoS ONE 2012, 7, e32037. [Google Scholar] [CrossRef]
- Fehlings, M.G.; Tetreault, L.A.; Wilson, J.R.; Kwon, B.K.; Burns, A.S.; Martin, A.R.; Hawryluk, G.; Harrop, J.S. A Clinical Practice Guideline for the Management of Acute Spinal Cord Injury: Introduction, Rationale, and Scope. Glob. Spine J. 2017, 7, 84s–94s. [Google Scholar] [CrossRef] [PubMed]
- Hadley, M.N.; Walters, B.C.; Grabb, P.A.; Oyesiku, N.M.; Przybylski, G.J.; Resnick, D.K.; Ryken, T.C. Guidelines for management of acute cervical spinal injuries. Introduction. Neurosurgery 2002, 50, S1. [Google Scholar]
- Walters, B.C.; Hadley, M.N.; Hurlbert, R.J.; Aarabi, B.; Dhall, S.S.; Gelb, D.E.; Harrigan, M.R.; Rozelle, C.J.; Ryken, T.C.; Theodore, N. Guidelines for the management of acute cervical spine and spinal cord injuries: 2013 update. Neurosurgery 2013, 60, 82–91. [Google Scholar] [CrossRef]
- Ryken, T.C.; Hadley, M.N.; Walters, B.C.; Aarabi, B.; Dhall, S.S.; Gelb, D.E.; Hurlbert, R.J.; Rozzelle, C.J.; Theodore, N. Radiographic assessment. Neurosurgery 2013, 72 (Suppl. 2), 54–72. [Google Scholar] [CrossRef] [Green Version]
- Kurpad, S.N.; Martin, A.R.; Tetreault, L.A.; Fischer, D.J.; Skelly, A.C.; Mikulis, D.; Flanders, A.E.; Aarabi, B.; Mroz, T.; Tsai, E.C.; et al. Impact of baseline magnetic resonance imaging on neurologic, functional, and safety outcomes in patients with acute traumatic spinal cord injury. Glob. Spine J. 2017, 7, 151S–174S. [Google Scholar]
- Bozzo, A.; Marcoux, J.; Radhakrishna, M.; Pelletier, J.; Goulet, B. The role of magnetic resonance imaging in the management of acute spinal cord injury. J. Neurotrauma 2011, 28, 1401–1411. [Google Scholar] [PubMed] [Green Version]
- Fehlings, M.G.; Martin, A.R.; Tetreault, L.; Aarabi, B.; Anderson, P.; Arnold, P.M.; Broke, D.; Burns, A.; Chiba, K.; Hawryluk, G.; et al. A Clinical Practice Guideline for the Management of Patients with Acute Spinal Cord Injury: Recommendations on the Role of Baseline Magnetic Resonance Imaging in Clinical Decision Making and Outcome Prediction. Glob. Spine J. 2017, 7, 221S–230S. [Google Scholar]
- Papadopoulos, S.M.; Selden, N.R.; Quint, D.J.; Patel, N.; Gillespie, B.; Grube, S. Immediate spinal cord decompression for cervical spinal cord injury: Feasibility and outcome. J. Trauma 2002, 52, 323–332. [Google Scholar] [CrossRef] [PubMed]
- Moher, D.; Shamseer, L.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A.; PRISMA-P Group. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015 statement. Syst. Rev. 2015, 4, 1. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Shamseer, L.; Moher, D.; Clarke, M.; Ghersi, D.; Liberati, A.; Petticrew, M.; Shekelle, P.; Stewart, L.A. Preferred reporting items for systematic review and meta-analysis protocols (PRISMA-P) 2015: Elaboration and explanation. BMJ 2015, 349, g7647. [Google Scholar] [CrossRef] [Green Version]
- Higgins, J.P.T.; Thomas, J.; Chandler, J.; Cumpston, M.; Li, T.; Page, M.J.; Welch, V.A. (Eds.) Cochrane Handbook for Systematic Reviews of Interventions; Version 6.2; Cochrane: Oxford, UK, 2021. [Google Scholar]
- Edelman, R.R. The History of MR Imaging as Seen through the Pages of Radiology. Radiology 2014, 273, S181–S200. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- R Core Team. R: A Language and Environment for Statistical Computing; R Core Team: Vienna, Austria, 2013. [Google Scholar]
- National Heart, Lung, and Blood Institute. National Institute of Health: Quality Assessment Tool for Observational Cohort and Cross-Sectional Studies; National Heart, Lung, and Blood Institute: Bethesda, MD, USA, 2014.
- Krappinger, D.; Lindtner, R.A.; Zegg, M.J.; Henninger, B.; Kaser, V.; Spicher, A.; Schmid, R. Spondylotic traumatic central cord syndrome: A hidden discoligamentous injury? Eur. Spine J. 2019, 28, 434–441. [Google Scholar] [CrossRef] [Green Version]
- Henninger, B.; Kaser, V.; Ostermann, S.; Spicher, A.; Zegg, M.; Schmid, R.; Kremser, C.; Krappinger, D. Cervical Disc and Ligamentous Injury in Hyperextension Trauma: MRI and Intraoperative Correlation. J. Neuroimaging 2020, 30, 104–109. [Google Scholar] [CrossRef]
- Zhu, F.; Yao, S.; Ren, Z.; Telemacque, D.; Qu, Y.; Chen, K.; Yang, F.; Zeng, L.; Guo, X. Early durotomy with duroplasty for severe adult spinal cord injury without radiographic abnormality: A novel concept and method of surgical decompression. Eur. Spine J. 2019, 28, 2275–2282. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Maeda, T.; Ueta, T.; Mori, E.; Yugue, I.; Kawano, O.; Takao, T.; Sakai, H.; Okada, S.; Shiba, K. Soft-tissue damage and segmental instability in adult patients with cervical spinal cord injury without major bone injury. Spine 2012, 37, E1560–E1566. [Google Scholar] [CrossRef]
- Mirvis, S.E.; Geisler, F.H.; Jelinek, J.J.; Joslyn, J.N.; Gellad, F. Acute cervical spine trauma: Evaluation with 1.5-T MR imaging. Radiology 1988, 166, 807–816. [Google Scholar]
- Bao, Y.; Zhong, X.; Zhu, W.; Chen, Y.; Zhou, L.; Dai, X.; Liao, J.; Li, Z.; Hu, K.; Bei, K.; et al. Feasibility and Safety of Cervical Kinematic Magnetic Resonance Imaging in Patients with Cervical Spinal Cord Injury without Fracture and Dislocation. Orthop. Surg. 2020, 12, 570–581. [Google Scholar] [CrossRef] [PubMed]
- Kalfas, I.; Wilberger, J.; Goldberg, A.; Prostko, E.R. Magnetic resonance imaging in acute spinal cord trauma. Neurosurgery 1988, 23, 295–299. [Google Scholar] [CrossRef]
- Como, J.J.; Samia, H.; Nemunaitis, G.A.; Jain, V.; Anderson, J.S.; Malangoni, M.A.; Claridge, J.A. The misapplication of the term spinal cord injury without radiographic abnormality (SCIWORA) in adults. J. Trauma Acute Care Surg. 2012, 73, 1261–1266. [Google Scholar] [CrossRef] [PubMed]
- Hendey, G.W.; Wolfson, A.B.; Mower, W.R.; Hoffman, J.R. Spinal cord injury without radiographic abnormality: Results of the National Emergency X-Radiography Utilization Study in blunt cervical trauma. J. Trauma 2002, 53, 1–4. [Google Scholar] [CrossRef] [Green Version]
- Maung, A.A.; Johnson, D.C.; Barre, K.; Peponis, T.; Mesar, T.; Velmahos, G.C.; McGrail, D.; Kasotakis, G.; Gross, R.I.; Rosenblatt, M.S.; et al. Cervical spine MRI in patients with negative CT: A prospective, multicenter study of the Research Consortium of New England Centers for Trauma (ReCONECT). J. Trauma Acute Care Surg. 2017, 82, 263–269. [Google Scholar] [CrossRef] [PubMed]
- Song, K.J.; Kim, G.H.; Lee, K.B. The efficacy of the modified classification system of soft tissue injury in extension injury of the lower cervical spine. Spine 2008, 33, E488–E493. [Google Scholar] [CrossRef]
- Cheng, X.; Ni, B.; Liu, Q.; Chen, J.; Guan, H.; Guo, Q. Clinical and radiological outcomes of spinal cord injury without radiologic evidence of trauma with cervical disc herniation. Arch. Orthop. Trauma Surg. 2013, 133, 193–198. [Google Scholar] [CrossRef] [PubMed]
- Aarabi, B.; Alexander, M.; Mirvis, S.E.; Shanmuganathan, K.; Chesler, D.; Maulucci, C.; Iguchi, M.; Aresco, C.; Blacklock, T. Predictors of outcome in acute traumatic central cord syndrome due to spinal stenosis. J. Neurosurg. Spine 2011, 14, 122–130. [Google Scholar] [CrossRef]
- Doran, S.E.; Papadopoulos, S.M.; Ducker, T.B.; Lillehei, K.O. Magnetic resonance imaging documentation of coexistent traumatic locked facets of the cervical spine and disc herniation. J. Neurosurg. 1993, 79, 341–345. [Google Scholar] [PubMed]
- Darsaut, T.E.; Ashforth, R.; Bhargava, R.; Broad, R.; Emery, D.; Kortbeek, F.; Lambert, R.; Lavoie, M.; Mahood, J.; MacDowell, I.; et al. A pilot study of magnetic resonance imaging-guided closed reduction of cervical spine fractures. Spine 2006, 31, 2085–2090. [Google Scholar] [CrossRef]
- Gupta, S.K.; Rajeev, K.; Khosla, V.K.; Sharma, B.S.; Paramjit; Mathuriya, S.N.; Pathak, A.; Tewari, M.K.; Kumar, A. Spinal cord injury without radiographic abnormality in adults. Spinal Cord 1999, 37, 726–729. [Google Scholar] [PubMed]
- Sharma, S.; Singh, M.; Wani, I.H.; Sharma, S.; Sharma, N.; Singh, D. Adult Spinal Cord Injury without Radiographic Abnormalities (SCIWORA): Clinical and Radiological Correlations. J. Clin. Med. Res. 2009, 1, 165–172. [Google Scholar] [CrossRef] [Green Version]
- Koyanagi, I.; Iwasaki, Y.; Hida, K.; Imamura, H.; Fujimoto, S.; Akino, M. Acute cervical cord injury associated with ossification of the posterior longitudinal ligament. Neurosurgery 2003, 53, 887–891. [Google Scholar] [CrossRef] [PubMed]
- Asan, Z. Spinal Cord Injury without Radiological Abnormality in Adults: Clinical and Radiological Discordance. World Neurosurg. 2018, 114, e1147–e1151. [Google Scholar] [CrossRef] [PubMed]
- Liu, Q.; Liu, Q.; Zhao, J.; Yu, H.; Ma, X.; Wang, L. Early MRI finding in adult spinal cord injury without radiologic abnormalities does not correlate with the neurological outcome: A retrospective study. Spinal Cord 2015, 53, 750–753. [Google Scholar] [CrossRef] [Green Version]
- Ghanta, M.K.; Smith, L.M.; Polin, R.S.; Marr, A.B.; Spires, W.V. An analysis of Eastern Association for the Surgery of Trauma practice guidelines for cervical spine evaluation in a series of patients with multiple imaging techniques. Am. Surg. 2002, 68, 563–567. [Google Scholar] [PubMed]
- Fehlings, M.G.; Rao, S.C.; Tator, C.H.; Skaf, G.; Arnold, P.; Benzel, E.; Dickman, C.; Cuddy, B.; Green, B.; Hitchon, P.; et al. The optimal radiologic method for assessing spinal canal compromise and cord compression in patients with cervical spinal cord injury. Part II: Results of a multicenter study. Spine 1999, 24, 605–613. [Google Scholar] [CrossRef]
- D’Souza, M.M.; Choudhary, A.; Poonia, M.; Kumar, P.; Khushu, S. Diffusion tensor MR imaging in spinal cord injury. Injury 2017, 48, 880–884. [Google Scholar] [CrossRef]
- Machino, M.; Yukawa, Y.; Ito, K.; Nakashima, H.; Kanbara, S.; Morita, D.; Kato, F. Can magnetic resonance imaging reflect the prognosis in patients of cervical spinal cord injury without radiographic abnormality? Spine 2011, 36, E1568–E1572. [Google Scholar] [CrossRef] [PubMed]
- Mahmood, N.; Rajagopal, K.; Ramesh, A. Cervical spinal cord injury with and without the radiographical evidence of trauma–A retrospective comparative study in adults. J. Clin. Diagn. Res. 2010, 4, 2183–2189. [Google Scholar]
- Tewari, M.K.; Gifti, D.S.; Singh, P.; Khosla, V.K.; Mathuriya, S.N.; Gupta, S.K.; Pathak, A. Diagnosis and prognostication of adult spinal cord injury without radiographic abnormality using magnetic resonance imaging: Analysis of 40 patients. Surg. Neurol. 2005, 63, 204–209. [Google Scholar] [CrossRef]
- Vaccaro, A.R.; Falatyn, S.P.; Flanders, A.E.; Balderston, R.A.; Northrup, B.E.; Cotler, J.M. Magnetic resonance evaluation of the intervertebral disc, spinal ligaments, and spinal cord before and after closed traction reduction of cervical spine dislocations. Spine 1999, 24, 1210–1217. [Google Scholar] [CrossRef] [PubMed]
- Selden, N.R.; Quint, D.J.; Patel, N.; d’Arcy, H.S.; Papadopoulos, S.M. Emergency magnetic resonance imaging of cervical spinal cord injuries: Clinical correlation and prognosis. Neurosurgery 1999, 44, 785–792. [Google Scholar] [CrossRef] [PubMed]
- Boese, C.K.; Müller, D.; Bröer, R.; Eysel, P.; Krischek, B.; Lehmann, H.C.; Lechler, P. Spinal cord injury without radiographic abnormality (SCIWORA) in adults: MRI type predicts early neurologic outcome. Spinal Cord 2016, 54, 878–883. [Google Scholar] [CrossRef] [PubMed]
- Huang, R.; Ryu, R.C.; Kim, T.T.; Alban, R.F.; Margulies, D.R.; Ley, E.J.; Barmparas, G. Is magnetic resonance imaging becoming the new computed tomography for cervical spine clearance? Trends in magnetic resonance imaging utilization at a Level I trauma center. J. Trauma Acute Care Surg. 2020, 89, 365–370. [Google Scholar] [CrossRef] [PubMed]
- Aarabi, B.; Olexa, J.; Chryssikos, T.; Galvagno, S.M.; Hersh, D.S.; Wessell, A.; Sansur, C.; Schwartzbauer, G.; Crandall, K.; Shanmuganathan, K.; et al. Extent of Spinal Cord Decompression in Motor Complete (American Spinal Injury Association Impairment Scale Grades A and B) Traumatic Spinal Cord Injury Patients: Post-Operative Magnetic Resonance Imaging Analysis of Standard Operative Approaches. J. Neurotrauma 2019, 36, 862–876. [Google Scholar] [CrossRef]
- Badhiwala, J.H.; Wilson, J.R.; Witiw, C.D.; Harrop, J.S.; Vaccaro, A.R.; Aarabi, B.; Grossman, R.G.; Geisler, F.H.; Fehlings, M.G. The influence of timing of surgical decompression for acute spinal cord injury: A pooled analysis of individual patient data. Lancet Neurol. 2021, 20, 117–126. [Google Scholar] [CrossRef]
- Masterson, K. A New Spinal Cord Injury Treatment is Getting Patients Back on Their Feet. 2018. Available online: https://www.ucsf.edu/news/2018/09/411471/new-spinal-cord-injury-treatment-getting-patients-back-their-feet (accessed on 10 October 2021).
- Martin, A.R.; Aleksanderek, I.; Cohen-Adad, J.; Tarmohamed, Z.; Tetreault, L.; Smith, N.; Cadotte, D.W.; Crawley, A.; Ginsberg, H.; Mikulis, D.J.; et al. Translating state-of-the-art spinal cord MRI techniques to clinical use: A systematic review of clinical studies utilizing DTI, MT, MWF, MRS, and fMRI. NeuroImage 2016, 10, 192–238. [Google Scholar] [CrossRef] [Green Version]
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).