
Effects of Albumin on Survival after a Hepatic Encephalopathy Episode: Randomized Double-Blind Trial and Meta-Analysis

 , , , , , and
, , , , , and
Abstract
:1. Introduction
2. Materials and Methods
2.1. Albumin Infusion Effect in Hepatic Encephalopathy (BETA)
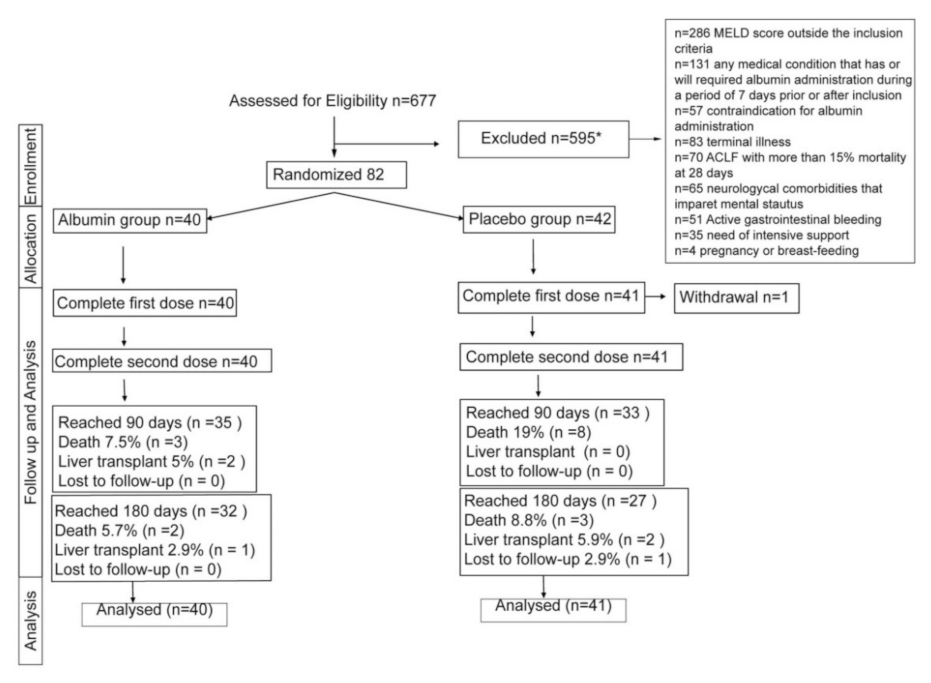
2.2. Patient Selection
2.3. Study Protocol
2.4. Outcome
2.5. Statistics
2.6. Metanalysis: Albumin Infusion Effect in Hepatic Encephalopathy (BETA) and Effects of Intravenous Albumin in Patients with Cirrhosis and Episodic Hepatic Encephalopathy (ALFAE)
2.7. Statistics
3. Results
3.1. Basal Clinical Characteristics
3.2. Complications during Follow-Up
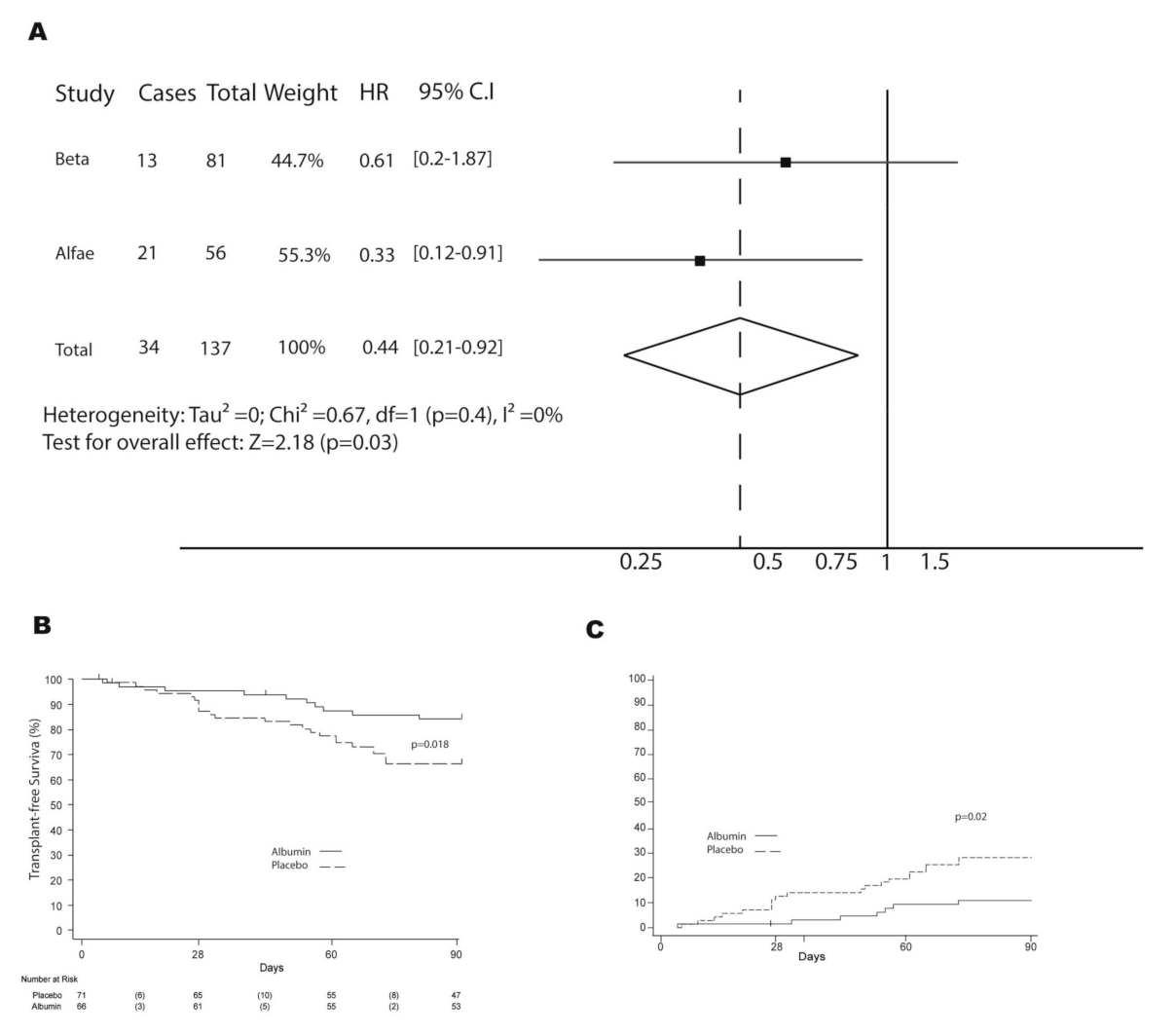
3.3. Survival
3.4. Safety and Tolerability
3.5. Meta-Analysis Results: BETA and ALFAE Studies
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Cordoba, J.; Ventura-Cots, M.; Simón-Talero, M.; Amorós, À.; Pavesi, M.; Vilstrup, H.; Angeli, P.; Domenicali, M.; Ginès, P.; Bernardi, M.; et al. Characteristics, risk factors, and mortality of cirrhotic patients hospitalized for hepatic encephalopathy with and without acute-on-chronic liver failure (ACLF). J. Hepatol. 2014, 60, 275–281. [Google Scholar] [CrossRef]
- Bass, N.M.; Mullen, K.D.; Sanyal, A.; Poordad, F.; Neff, G.; Leevy, C.B.; Sigal, S.; Sheikh, M.Y.; Beavers, K.; Frederick, T.; et al. Rifaximin Treatment in Hepatic Encephalopathy. N. Engl. J. Med. 2010, 362, 1071–1081. [Google Scholar] [CrossRef] [Green Version]
- Vilstrup, H.; Amodio, P.; Bajaj, J.; Cordoba, J.; Ferenci, P.; Mullen, K.D.; Weissenborn, K.; Wong, P. Hepatic encephalopathy in chronic liver disease: 2014 Practice Guideline by the American Association for the Study Of Liver Diseases and the European Association for the Study of the Liver. Hepatology 2014, 60, 715–735. [Google Scholar] [CrossRef]
- Fernández, J.; Clària, J.; Amorós, A.; Aguilar, F.; Castro, M.; Casulleras, M.; Acevedo, J.; Duran-Güell, M.; Nuñez, L.; Costa, M.; et al. Effects of Albumin Treatment on Systemic and Portal Hemodynamics and Systemic Inflammation in Patients With Decompensated Cirrhosis. Gastroenterology 2019, 157, 149–162. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sort, P.; Navasa, M.; Arroyo, V.; Aldeguer, X.; Planas, R.; Ruiz-Del-Arbol, L.; Castells, L.; Vargas, V.; Soriano, G.; Guevara, M.; et al. Effect of Intravenous Albumin on Renal Impairment and Mortality in Patients with Cirrhosis and Spontaneous Bacterial Peritonitis. N. Engl. J. Med. 1999, 341, 403–409. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Wong, F.; Pappas, S.C.; Curry, M.P.; Reddy, K.R.; Rubin, R.A.; Porayko, M.K.; Gonzalez, S.A.; Mumtaz, K.; Lim, N.; Simonetto, D.A.; et al. Terlipressin plus Albumin for the Treatment of Type 1 Hepatorenal Syndrome. N. Engl. J. Med. 2021, 384, 818–828. [Google Scholar] [CrossRef] [PubMed]
- Gines, A.; Fernandez-Esparrach, G.; Monescillo, A.; Vila, C.; Domenech, E.; Abecasis, R.; Angeli, P.; Ruiz-Del-Arbol, L.; Planas, R.; Sola, R.; et al. Randomized trial comparing albumin, dextran 70, and polygeline in cirrhotic patients with ascites treated by paracentesis. Gastroenterology 1996, 111, 1002–1010. [Google Scholar] [CrossRef]
- Angeli, P.; Bernardi, M.; Villanueva, C.; Francoz, C.; Mookerjee, R.; Trebicka, J.; Krag, A.; Laleman, W.; Gines, P. EASL Clinical Practice Guidelines for the management of patients with decompensated cirrhosis. J. Hepatol. 2018, 69, 406–460. [Google Scholar] [CrossRef] [Green Version]
- Solà, E.; Solé, C.; Simón-Talero, M.; Martín-Llahí, M.; Castellote, J.; Martinez, R.G.; Moreira, R.; Torrens, M.; Márquez, F.; Fabrellas, N.; et al. Midodrine and albumin for prevention of complications in patients with cirrhosis awaiting liver transplantation. A randomized placebo-controlled trial. J. Hepatol. 2018, 69, 1250–1259. [Google Scholar] [CrossRef] [PubMed]
- Guevara, M.; Terra, C.; Nazar, A.; Solà, E.; Fernández, J.; Pavesi, M.; Arroyo, V.; Ginès, P. Albumin for bacterial infections other than spontaneous bacterial peritonitis in cirrhosis. A randomized, controlled study. J. Hepatol. 2012, 57, 759–765. [Google Scholar] [CrossRef] [PubMed]
- Simón-Talero, M.; García-Martínez, R.; Torrens, M.; Augustin, S.; Gómez, S.; Pereira, G.; Guevara, M.; Ginés, P.; Soriano, G.; Román, E.; et al. Effects of intravenous albumin in patients with cirrhosis and episodic hepatic encephalopathy: A randomized double-blind study. J. Hepatol. 2013, 59, 1184–1192. [Google Scholar] [CrossRef] [PubMed]
- Fernández, J.; Angeli, P.; Trebicka, J.; Merli, M.; Gustot, T.; Alessandria, C.; Aagaard, N.K.; de Gottardi, A.; Welzel, T.M.; Gerbes, A.; et al. Efficacy of Albumin Treatment for Patients with Cirrhosis and Infections Unrelated to Spontaneous Bacterial Peritonitis. Clin. Gastroenterol. Hepatol. 2020, 18, 963–973.e14. [Google Scholar] [CrossRef] [PubMed]
- China, L.; Freemantle, N.; Forrest, E.; Kallis, Y.; Ryder, S.D.; Wright, G.; Portal, A.J.; Salles, N.B.; Gilroy, D.W.; O’Brien, A. A Randomized Trial of Albumin Infusions in Hospitalized Patients with Cirrhosis. N. Engl. J. Med. 2021, 384, 808–817. [Google Scholar] [CrossRef] [PubMed]
- Caraceni, P.; Riggio, O.; Angeli, P.; Alessandria, C.; Neri, S.; Foschi, F.G.; Levantesi, F.; Airoldi, A.; Boccia, S.; Svegliati-Baroni, G.; et al. Long-term albumin administration in decompensated cirrhosis (ANSWER): An open-label randomised trial. Lancet 2018, 391, 2417–2429. [Google Scholar] [CrossRef]
- Moreau, R.; Jalan, R.; Gines, P.; Pavesi, M.; Angeli, P.; Cordoba, J.; Durand, F.; Gustot, T.; Saliba, F.; Domenicali, M.; et al. Acute-on-Chronic Liver Failure Is a Distinct Syndrome That Develops in Patients With Acute Decompensation of Cirrhosis. Gastroenterology 2013, 144, 1426–1437.e9. [Google Scholar] [CrossRef] [PubMed]
- Martinez, R.G.; Caraceni, P.; Bernardi, M.; Ginès, P.; Arroyo, V.; Jalan, R. Albumin: Pathophysiologic basis of its role in the treatment of cirrhosis and its complications. Hepatology 2013, 58, 1836–1846. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
{kind=link}
{kind=link}
| Placebo Group | Albumin Group | |
|---|---|---|
| n = 42 | n = 40 | |
| Male, n (%) | 26(61.9) | 29(72.5) |
| Age, median (IQR) | 69.1(63.3–75.3) | 66.5(59.9–73.6) |
| BMI, median (IQR) | 24.5(23.2–26.5) | 24.2(23.2–26.8) |
| Etiology, n (%) | ||
| Alcohol related | 22(57.7) | 19(47.5) |
| MAFLD | 2(4.9) | 4(10) |
| Alcohol and HCV | 4(9.8) | 6(15) |
| HCV | 5(12.2) | 6(15) |
| Alcohol and MAFL | 2(4.9) | -- |
| Other * | 7(8.8) | 5(6.1) |
| Previous decompensations, n (%) | ||
| Ascites | 35(83.3) | 30(75) |
| Hepatic encephalopathy | 27(64.3) | 26(65) |
| Spontaneous bacterial peritonitis | 7(16.7) | 7(17.5) |
| Gastrointestinal bleeding | 11(26.2) | 11(27.6) |
| Hepatorenal syndrome | 2(4.8) | 3(7.5) |
| Hepatocellular carcinoma | 5(11.9) | 4(10) |
| Other comorbidities, n (%) | ||
| Hypertension | 26(66.7) | 23(59) |
| Dyslipidemia | 9(23.1) | 7(17.9) |
| Diabetes | 20(51.3) | 14(35.9) |
| Severity score, median (IQR) | ||
| MELD | 17(16–20) | 17(15–20) |
| Treatment at inclusion, n (%) | ||
| Rifaximin and/or lactulose | 35(83.3) | 31(77.5) |
| Laboratory parameters, median (IQR) | ||
| Hemoglobin g/dL | 10.6(9.9–13) | 10.9(9.3–11.8) |
| Leukocytes x109/L | 5.06(3.8–7.4) | 5.09(4.06–6.6) |
| Platelets x10E9/L | 82.5(64–109) | 76.5(57.5–106.5) |
| Sodium mEq/L | 135.8(132.8–138.6) | 136.2(134–139) |
| AST IU/L | 44(31–64) | 51(36–75) |
| ALT IU/L | 26(18–35) | 32.5(22–43.5) |
| Bilirubin mg/dL | 3.2(1.7–4.6) | 2.97(1.91–5) |
| Albumin g/dL | 2.85(2.35–3.01) | 2.6(2.41–2.93) |
| INR | 1.53(1.37–1.71) | 1.55(1.35–1.83) |
| Creatinine (mg/dL) | 1.08(0.77–1.53) | 0.99(0.7–1.32) |
| Mean Arterial Pressure (mmHg) | 82.6(76–94.3) | 78.7(72.5–89.3) |
| Current liver-related decompensations, n (%) ♦ | ||
| Ascites | 19(45.2) | 17(42.5) |
| Hepatorenal syndrome | 1(2.4) | -- |
| Precipitant factors, n (%) | ||
| Infection | 11(26.1) | 12(30) |
| Constipation | 9(21.4) | 9(22.5) |
| Dehydration | 4(9.5) | 3(7.5) |
| Diuretics | 14(33.3) | 23(59) ** |
| West Haven at screening, n (%) | ||
| II | 30(71.4) | 31(77.5) |
| III | 11(26.2) | 9(22.5) |
| IV | 1(2.4) | -- |
| CHESS scale | 2.5 (1–6) | 2(1–4) |
| Time Point | Placebo Number of Patients with MHE/Number of Total Evaluated Patients and Percentage | Albumin Number of Patients with MHE/Number of Total Evaluated Patients and Percentage |
|---|---|---|
| Day 2–3 | 6/9 (66.6) | 5/13(38.5) |
| Day 7 | 7/12(58.3) | 4/17(23.5) |
| Day 30 | 4/10(40) | 5/16(31.3) |
| Day 60 | 1/4(25) | 5/14(35.7) |
| Day 90 | 6/12(50) | 4/16(25) |
| Day 180 | 2/6(33.3) | 3/13(7.7) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Ventura-Cots, M.; Simón-Talero, M.; Poca, M.; Ariza, X.; Masnou, H.; Sanchez, J.; Llop, E.; Cañete, N.; Martín-Llahí, M.; Amador, A.; et al. Effects of Albumin on Survival after a Hepatic Encephalopathy Episode: Randomized Double-Blind Trial and Meta-Analysis. J. Clin. Med. 2021, 10, 4885. https://doi.org/10.3390/jcm10214885
Ventura-Cots M, Simón-Talero M, Poca M, Ariza X, Masnou H, Sanchez J, Llop E, Cañete N, Martín-Llahí M, Amador A, et al. Effects of Albumin on Survival after a Hepatic Encephalopathy Episode: Randomized Double-Blind Trial and Meta-Analysis. Journal of Clinical Medicine. 2021; 10(21):4885. https://doi.org/10.3390/jcm10214885
Chicago/Turabian StyleVentura-Cots, Meritxell, Macarena Simón-Talero, Maria Poca, Xavier Ariza, Helena Masnou, Jordi Sanchez, Elba Llop, Núria Cañete, Marta Martín-Llahí, Alberto Amador, and et al. 2021. "Effects of Albumin on Survival after a Hepatic Encephalopathy Episode: Randomized Double-Blind Trial and Meta-Analysis" Journal of Clinical Medicine 10, no. 21: 4885. https://doi.org/10.3390/jcm10214885
APA StyleVentura-Cots, M., Simón-Talero, M., Poca, M., Ariza, X., Masnou, H., Sanchez, J., Llop, E., Cañete, N., Martín-Llahí, M., Amador, A., Martínez, J., Clemente-Sanchez, A., Puente, A., Torrens, M., Alvarado-Tapias, E., Napoleone, L., Miquel-Planas, M., Ardèvol, A., Casas Rodrigo, M., ... Genescà, J. (2021). Effects of Albumin on Survival after a Hepatic Encephalopathy Episode: Randomized Double-Blind Trial and Meta-Analysis. Journal of Clinical Medicine, 10(21), 4885. https://doi.org/10.3390/jcm10214885