
Cessation of Nucleos(t)ide Analogue Therapy in Non-Cirrhotic Hepatitis B Patients with Prior Severe Acute Exacerbation


Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Design
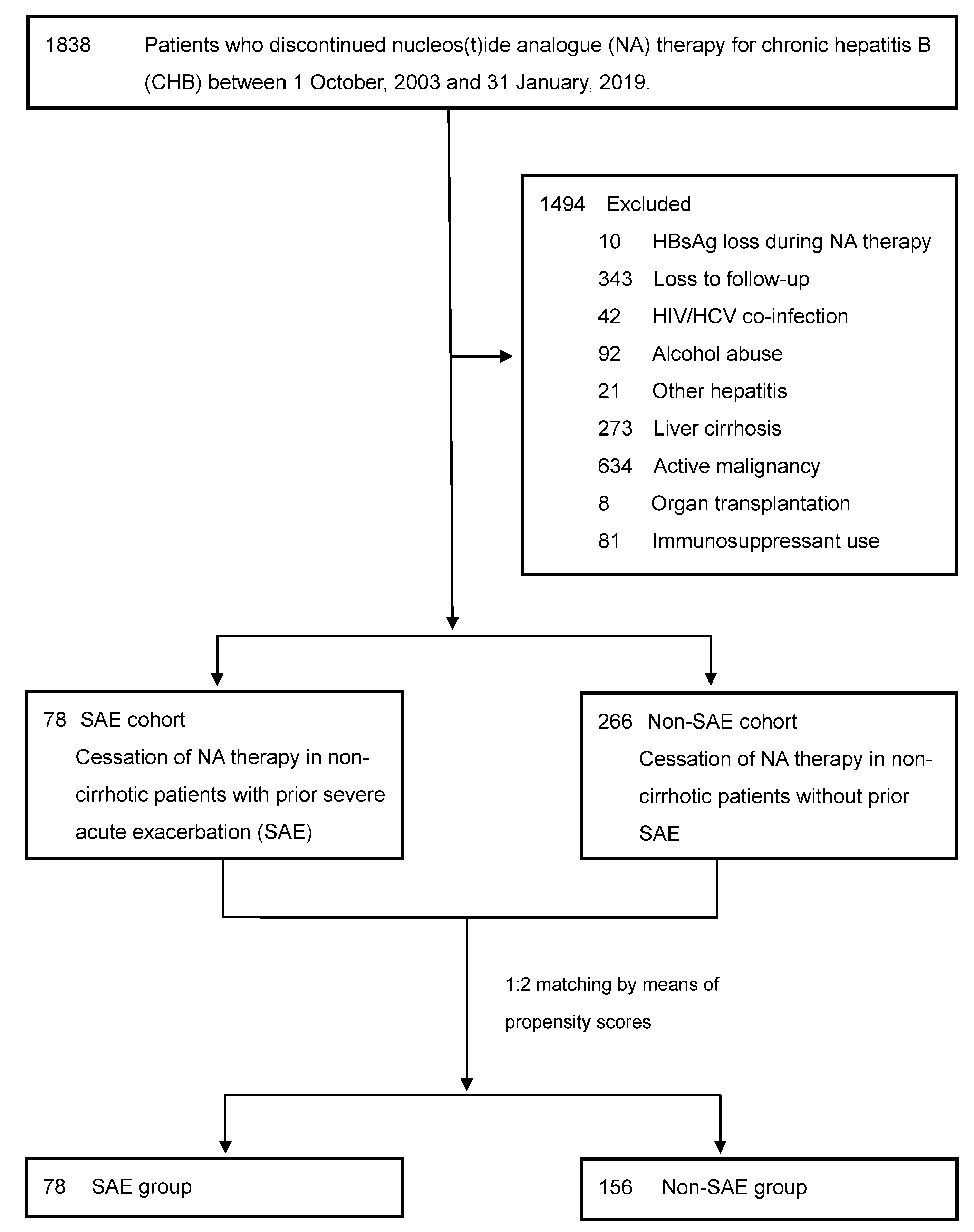
2.2. Study Cohort
2.3. Outcome Measurement
2.4. Statistical Analysis
3. Results
3.1. Study Subjects
3.2. Clinical Relapse and NA Retreatment
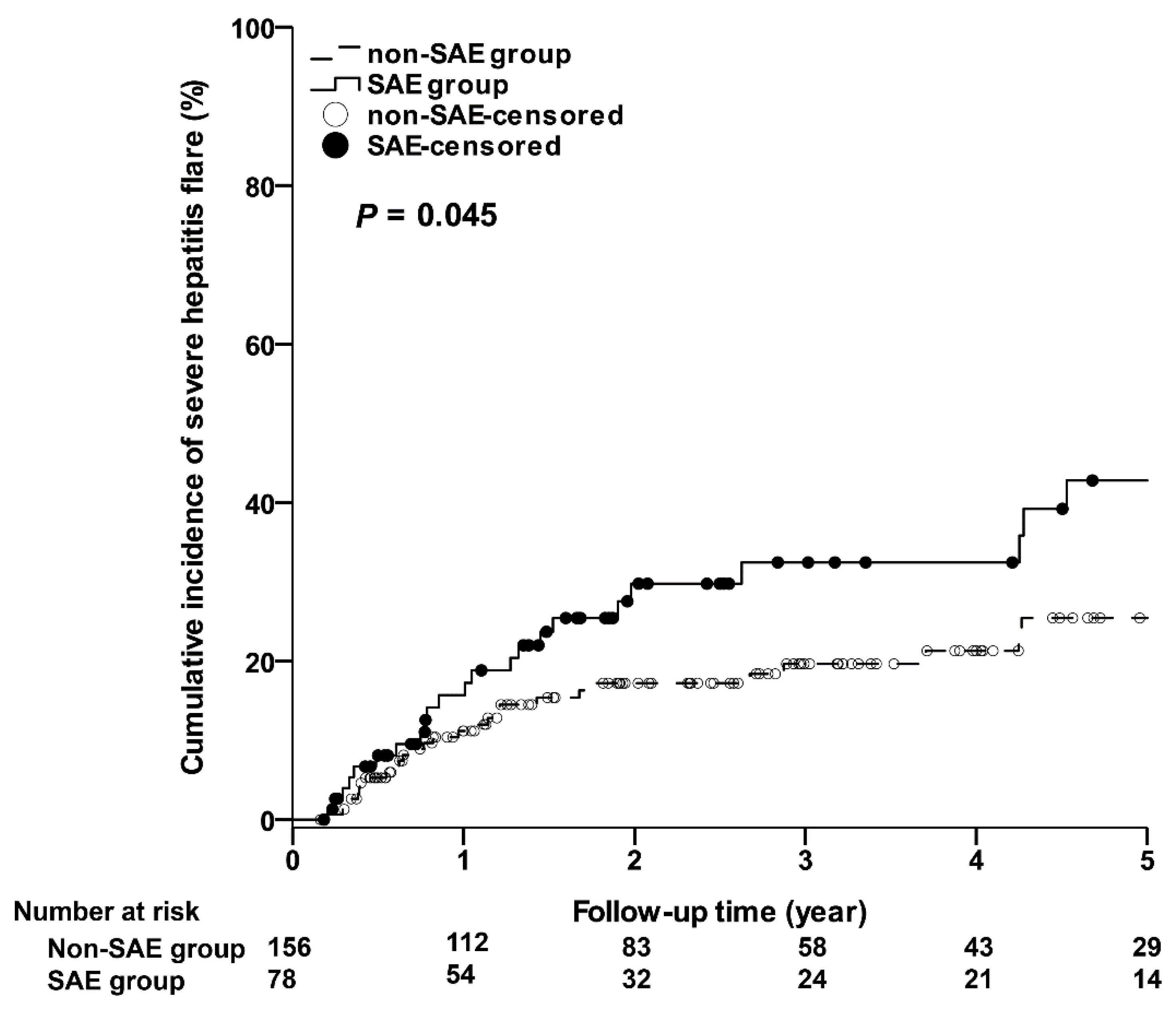
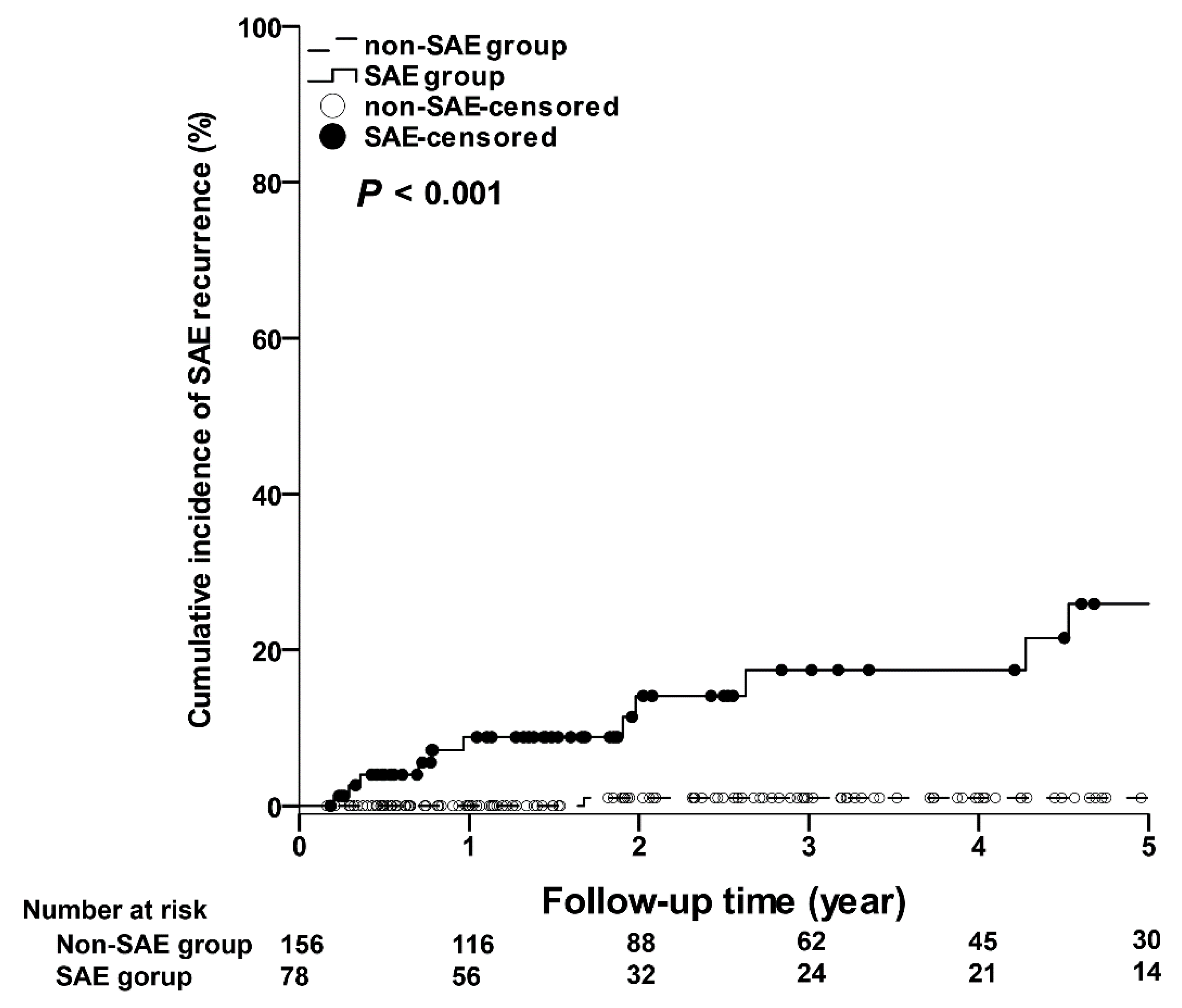
3.3. Severe Clinical Relapse and SAE Recurrence
3.4. Multivariable Regression Analysis for Severe Clinical Relapse
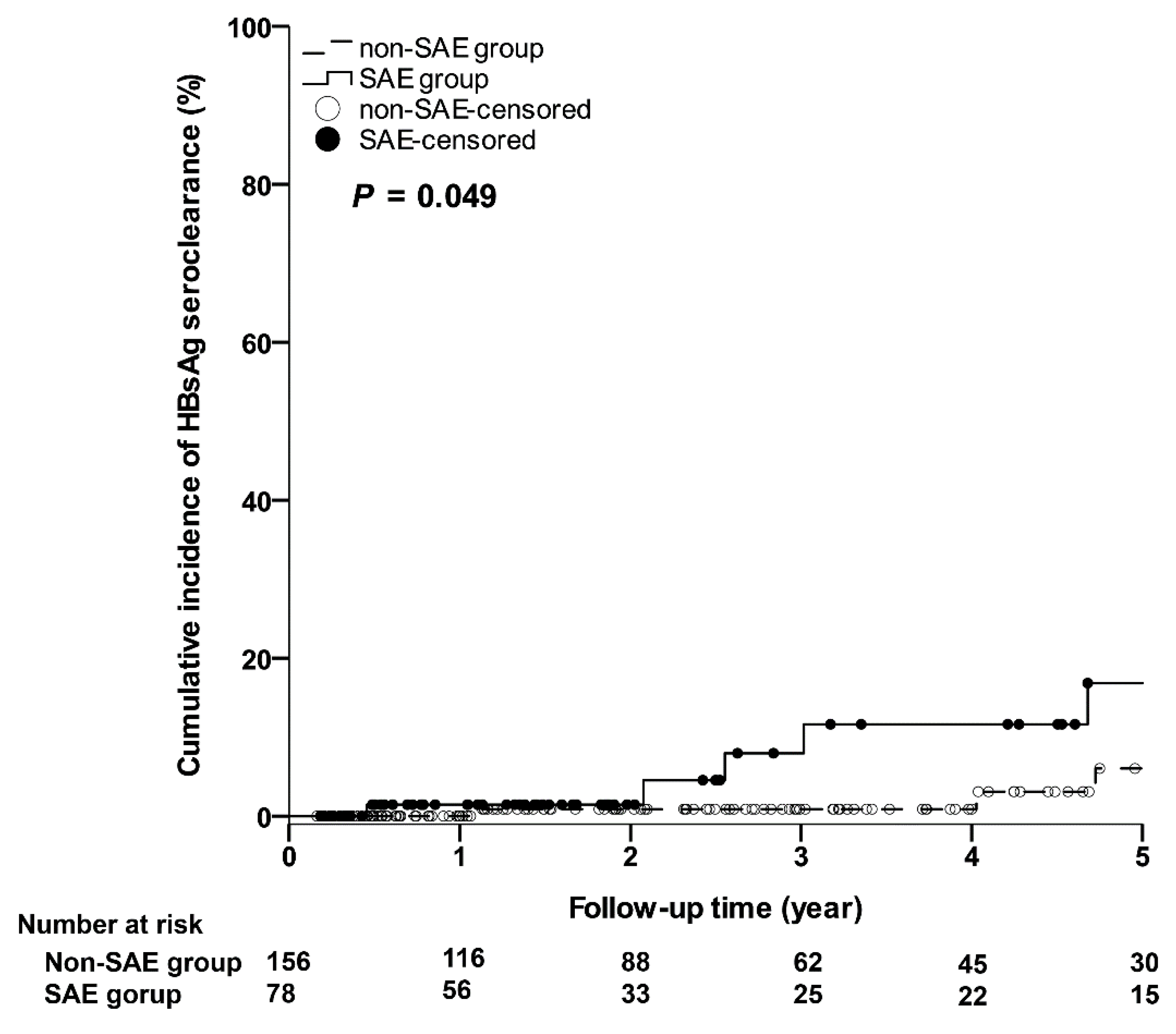
3.5. HBsAg Seroclearance
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- World Health Organization. Global Hepatitis Report 2017. Available online: https://www.who.int/publications/i/item/global-hepatitis-report-2017 (accessed on 16 November 2020).
- Hosaka, T.; Suzuki, F.; Kobayashi, M.; Seko, Y.; Kawamura, Y.; Sezaki, H.; Akuta, N.; Suzuki, Y.; Saitoh, S.; Arase, Y.; et al. Long-term entecavir treatment reduces hepatocellular carcinoma incidence in patients with hepatitis B virus infection. Hepatology 2013, 58, 98–107. [Google Scholar] [CrossRef] [PubMed]
- Lok, A.S.; Zoulim, F.; Dusheiko, G.; Ghany, M.G. Hepatitis B cure: From discovery to regulatory approval. J. Hepatol. 2017, 67, 847–861. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- EASL. Clinical Practice Guidelines on the management of hepatitis B virus infection. J. Hepatol. 2017, 67, 370–398. [Google Scholar] [CrossRef] [Green Version]
- Sarin, S.K.; Kumar, M.; Lau, G.K.; Abbas, Z.; Chan, H.L.; Chen, C.J.; Chen, D.S.; Chen, H.L.; Chen, P.J.; Chien, R.N.; et al. Asian-Pacific clinical practice guidelines on the management of hepatitis B: A 2015 update. Hepatol. Int. 2016, 10, 1–98. [Google Scholar] [CrossRef] [PubMed]
- Terrault, N.A.; Lok, A.S.F.; McMahon, B.J.; Chang, K.M.; Hwang, J.P.; Jonas, M.M.; Brown, R.S., Jr.; Bzowej, N.H.; Wong, J.B. Update on prevention, diagnosis, and treatment of chronic hepatitis B: AASLD 2018 hepatitis B guidance. Hepatology 2018, 67, 1560–1599. [Google Scholar] [CrossRef]
- Lampertico, P.; Berg, T. Less can be more: A finite treatment approach for HBeAg-negative chronic hepatitis B. Hepatology 2018, 68, 397–400. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Papatheodoridis, G.V.; Manolakopoulos, S.; Su, T.H.; Siakavellas, S.; Liu, C.J.; Kourikou, A.; Yang, H.C.; Kao, J.H. Significance of definitions of relapse after discontinuation of oral antivirals in HBeAg-negative chronic hepatitis B. Hepatology 2018, 68, 415–424. [Google Scholar] [CrossRef] [Green Version]
- Liaw, Y.-F.; Kao, J.-H.; Piratvisuth, T.; Chan, H.L.Y.; Chien, R.-N.; Liu, C.-J.; Gane, E.; Locarnini, S.; Lim, S.-G.; Han, K.-H.; et al. Asian-Pacific consensus statement on the management of chronic hepatitis B: A 2012 update. Hepatol. Int. 2012, 6, 531–561. [Google Scholar] [CrossRef]
- Chang, M.L.; Liaw, Y.F.; Hadziyannis, S.J. Systematic review: Cessation of long-term nucleos(t)ide analogue therapy in patients with hepatitis B e antigen-negative chronic hepatitis B. Aliment. Pharmacol. Ther. 2015, 42, 243–257. [Google Scholar] [CrossRef]
- Papatheodoridis, G.; Vlachogiannakos, I.; Cholongitas, E.; Wursthorn, K.; Thomadakis, C.; Touloumi, G.; Petersen, J. Discontinuation of oral antivirals in chronic hepatitis B: A systematic review. Hepatology 2016, 63, 1481–1492. [Google Scholar] [CrossRef]
- Jeng, W.J.; Chen, Y.C.; Chien, R.N.; Sheen, I.S.; Liaw, Y.F. Incidence and predictors of hepatitis B surface antigen seroclearance after cessation of nucleos(t)ide analogue therapy in hepatitis B e antigen-negative chronic hepatitis B. Hepatology 2018, 68, 425–434. [Google Scholar] [CrossRef]
- Chen, C.H.; Hung, C.H.; Wang, J.H.; Lu, S.N.; Lai, H.C.; Hu, T.H.; Lin, C.H.; Peng, C.Y. The Incidence of Hepatitis B Surface Antigen Loss Between Hepatitis B E Antigen-Negative Noncirrhotic Patients Who Discontinued or Continued Entecavir Therapy. J. Infect. Dis. 2019, 219, 1624–1633. [Google Scholar] [CrossRef]
- Wong, V.W.; Wong, G.L.; Yiu, K.K.; Chim, A.M.; Chu, S.H.; Chan, H.Y.; Sung, J.J.; Chan, H.L. Entecavir treatment in patients with severe acute exacerbation of chronic hepatitis B. J. Hepatol. 2011, 54, 236–242. [Google Scholar] [CrossRef]
- Peng, C.Y.; Chien, R.N.; Liaw, Y.F. Hepatitis B virus-related decompensated liver cirrhosis: Benefits of antiviral therapy. J. Hepatol. 2012, 57, 442–450. [Google Scholar] [CrossRef] [Green Version]
- Wong, V.W.; Chan, H.L. Severe acute exacerbation of chronic hepatitis B: A unique presentation of a common disease. J Gastroenterol. Hepatol. 2009, 24, 1179–1186. [Google Scholar] [CrossRef] [PubMed]
- Chang, M.L.; Jeng, W.J.; Liaw, Y.F. Clinical events after cessation of lamivudine therapy in patients recovered from hepatitis B flare with hepatic decompensation. Clin. Gastroenterol. Hepatol. 2015, 13, 979–986. [Google Scholar] [CrossRef] [PubMed]
- Tsai, W.L.; Chiang, P.H.; Chan, H.H.; Lin, H.S.; Lai, K.H.; Cheng, J.S.; Chen, W.C.; Tsay, F.W.; Wang, H.M.; Tsai, T.J.; et al. Early entecavir treatment for chronic hepatitis B with severe acute exacerbation. Antimicrob. Agents Chemother. 2014, 58, 1918–1921. [Google Scholar] [CrossRef] [Green Version]
- Hsu, C.; Tsou, H.H.; Lin, S.J.; Wang, M.C.; Yao, M.; Hwang, W.L.; Kao, W.Y.; Chiu, C.F.; Lin, S.F.; Lin, J.; et al. Chemotherapy-induced hepatitis B reactivation in lymphoma patients with resolved HBV infection: A prospective study. Hepatology 2014, 59, 2092–2100. [Google Scholar] [CrossRef]
- Facciorusso, A. The influence of diabetes in the pathogenesis and the clinical course of hepatocellular carcinoma: Recent findings and new perspectives. Curr. Diabetes Rev. 2013, 9, 382–386. [Google Scholar] [CrossRef] [PubMed]
- Sterling, R.K.; Lissen, E.; Clumeck, N.; Sola, R.; Correa, M.C.; Montaner, J.; Sulkowski, S.M.; Torriani, F.J.; Dieterich, D.T.; Thomas, D.L.; et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology 2006, 43, 1317–1325. [Google Scholar] [CrossRef]
- Chiang, C.H.; Huang, K.C. Association between metabolic factors and chronic hepatitis B virus infection. World J. Gastroenterol. 2014, 20, 7213–7216. [Google Scholar] [CrossRef] [PubMed]
- Fung, J.; Lai, C.L.; Tanaka, Y.; Mizokami, M.; Yuen, J.; Wong, D.K.; Yuen, M.F. The duration of lamivudine therapy for chronic hepatitis B: Cessation vs. continuation of treatment after HBeAg seroconversion. Am. J. Gastroenterol. 2009, 104, 1940–1946. [Google Scholar] [CrossRef]
- Van Hees, S.; Bourgeois, S.; Van Vlierberghe, H.; Sersté, T.; Francque, S.; Michielsen, P.; Sprengers, D.; Reynaert, H.; Henrion, J.; Negrin Dastis, S.; et al. Stopping nucleos(t)ide analogue treatment in Caucasian hepatitis B patients after HBeAg seroconversion is associated with high relapse rates and fatal outcomes. Aliment. Pharmacol. Ther. 2018, 47, 1170–1180. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Lee, I.C.; Sun, C.K.; Su, C.W.; Wang, Y.J.; Chang, H.C.; Huang, H.C.; Lee, K.C.; Huang, Y.S.; Perng, C.L.; Liu, Y.H.; et al. Durability of Nucleos(t)ide Analogues Treatment in Patients With Chronic Hepatitis B. Medicine (Baltimore) 2015, 94, e1341. [Google Scholar] [CrossRef] [PubMed]
- Jeng, W.J.; Chen, Y.C.; Sheen, I.S.; Lin, C.L.; Hu, T.H.; Chien, R.N.; Liaw, Y.F. Clinical Relapse After Cessation of Tenofovir Therapy in Hepatitis B e Antigen-Negative Patients. Clin. Gastroenterol. Hepatol. 2016, 14, 1813–1820.e1. [Google Scholar] [CrossRef]
- Kuo, M.T.; Hu, T.H.; Hung, C.H.; Wang, J.H.; Lu, S.N.; Tsai, K.L.; Chen, C.H. Hepatitis B virus relapse rates in chronic hepatitis B patients who discontinue either entecavir or tenofovir. Aliment. Pharmacol. Ther. 2019, 49, 218–228. [Google Scholar] [CrossRef]
- Seeff, L.B.; Koff, R.S. Evolving concepts of the clinical and serologic consequences of hepatitis B virus infection. Semin. Liver Dis. 1986, 6, 11–22. [Google Scholar] [CrossRef]
- Liu, C.J.; Kao, J.H.; Wang, H.Y.; Lai, M.Y.; Chen, T.C.; Chen, P.J.; Chen, D.S. Origin of serum hepatitis B virus in acute exacerbation: Comparison with HBV in the liver and from other exacerbation. Hepatology 2004, 40, 310–317. [Google Scholar] [CrossRef] [PubMed]
- Bertoletti, A.; Gehring, A.J. The immune response during hepatitis B virus infection. J. Gen. Virol. 2006, 87, 1439–1449. [Google Scholar] [CrossRef]
- Boni, C.; Laccabue, D.; Lampertico, P.; Giuberti, T.; Viganò, M.; Schivazappa, S.; Alfieri, A.; Pesci, M.; Gaeta, G.B.; Brancaccio, G.; et al. Restored function of HBV-specific T cells after long-term effective therapy with nucleos(t)ide analogues. Gastroenterology 2012, 143, 963–973.e9. [Google Scholar] [CrossRef]
- Liaw, Y.F. Finite nucleos(t)ide analog therapy in HBeAg-negative chronic hepatitis B: An emerging paradigm shift. Hepatol. Int. 2019, 13, 665–673. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Del Prete, V.; Antonino, M.; Crucinio, N.; Neve, V.; Di Leo, A.; Carr, B.I.; Barone, M. Post-recurrence survival in hepatocellular carcinoma after percutaneous radiofrequency ablation. Dig. Liver Dis. 2014, 46, 1014–1019. [Google Scholar] [CrossRef] [PubMed]
- Facciorusso, A.; Garcia Perdomo, H.A.; Muscatiello, N.; Buccino, R.V.; Wong, V.W.; Singh, S. Systematic review with meta-analysis: Change in liver stiffness during anti-viral therapy in patients with hepatitis B. Dig. Liver Dis. 2018, 50, 787–794. [Google Scholar] [CrossRef] [PubMed]





{kind=link}
{kind=link}
{kind=link}
{kind=link}
| Characteristics | Non-SAE Group | SAE Group | |
|---|---|---|---|
| n = 156 | n = 78 | p Value | |
| Age, years | 43 (35–53) | 42 (31–53) | 0.650 |
| Male, n (%) | 112 (71.8%) | 56 (71.8%) | 1.000 |
| BMI, kg/m2 | 24.5 (22.8–27.1) | 23.7 (22.1–25.8) | 0.114 |
| Diabetes, n (%) | 20 (12.8%) | 12 (15.4%) | 0.737 |
| Data when NA therapy initiation | |||
| HBV DNA, log10 IU/mL | 6.21 (5.11–7.36) | 6.68 (5.02–7.91) | 0.359 |
| Bilirubin, mg/dL | 0.8 (0.6–1.1) | 5.2 (2.7–10.1) | <0.001 ** |
| PT prolongation, second | 0 (0–0.3) | 2.4 (0.25–5.35) | <0.001 ** |
| AST, ULN | 3.7 (2.5–7.3) | 32.5 (14.8–49.5) | <0.001 ** |
| ALT, ULN | 8.5 (4.8–15.9) | 41.5 (22.9–67.9) | <0.001 ** |
| HBeAg positivity, n (%) | 62 (39.7%) | 25 (32.1%) | 0.315 |
| NA therapy duration, month | 36.0 (35.0–38.0) | 36.0 (22.9–36.0) | 0.454 |
| NA consolidation duration, month | 26.04 (14.46–30.51) | 24.95 (15.59–31.53) | 0.779 |
| NA therapy categories | 0.468 | ||
| Entecavir, n (%) | 67 (42.9%) | 31 (39.7%) | |
| Tenofovir, n (%) | 27 (17.3%) | 10 (12.8%) | |
| Lamivudine or telbivudine, n (%) | 62 (39.7%) | 37 (47.4%) | |
| Data when NA therapy cessation | |||
| Bilirubin, mg/dL | 0.7 (0.5–0.8) | 0.7 (0.5–0.9) | 0.117 |
| AST, ULN | 0.7 (0.6–0.9) | 0.7 (0.6–0.8) | 0.816 |
| ALT, ULN | 0.8 (0.6–1.1) | 0.7 (0.5–0.9) | 0.021 * |
| PLT, 109/L | 202.0 (177–249) | 206.0 (168–251) | 0.879 |
| FIB-4 | 1.1 (0.7–1.6) | 1.1 (0.7–1.4) | 0.843 |
| Follow-up duration, month | 24.87 (10.28–47.54) | 19.56 (9.2–37.17) | 0.229 |
| Variables | Univariable | Multivariable | ||
|---|---|---|---|---|
| HR (95% CI) | p Value | HR (95% CI) | p Value | |
| SAE vs. Non-SAE | 1.76 (1.03–3.01) | 0.040 * | 1.79 (1.04–3.06) | 0.034 * |
| Age, year | 1.01 (1.00–1.03) | 0.143 | ||
| Male vs. female | 2.27 (1.11–4.66) | 0.025 * | 2.31 (1.13–4.75) | 0.022 * |
| BMI, kg/m2 | 0.96 (0.87-1.05) | 0.369 | ||
| Overweight vs. non-overweight a | 0.96 (0.87-1.05) | 0.369 | ||
| Obesity vs. non-obesity b | 0.71 (0.37-1.37) | 0.309 | ||
| Diabetes vs. Non-diabetes | 1.66 (0.83–3.32) | 0.149 | ||
| Data when NA therapy initiation | ||||
| HBV DNA, log10 IU/mL | 1.15 (0.93–1.42) | 0.186 | ||
| Bilirubin, mg/dL | 1.03 (0.99–1.08) | 0.146 | ||
| PT prolongation, second | 1.05 (0.95–1.16) | 0.313 | ||
| AST, ULN | 1.00 (0.99–1.01) | 0.913 | ||
| ALT, ULN | 1.00 (0.99–1.01) | 0.602 | ||
| HBeAg positivity | 0.66 (0.37–1.17) | 0.154 | ||
| NA therapy duration, month NA consolidation duration, m NA consolidation > 36 months | 1.01 (1.00–1.02) 1.01 (0.99–1.03) 1.17 (0.36–3.82) | 0.143 0.524 0.794 | ||
| ETV vs. other NAs | 0.95 (0.55–1.66) | 0.869 | ||
| Data when NA therapy cessation | ||||
| Bilirubin, mg/dL | 2.31 (0.41–12.85) | 0.340 | ||
| AST, ULN | 0.69 (0.27–1.79) | 0.450 | ||
| ALT, ULN | 0.98 (0.71–1.36) | 0.904 | ||
| PLT, 109/L | 0.99 (0.99–1.00) | 0.095 | ||
| FIB-4 | 1.09 (0.73–1.63) | 0.682 | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Lai, C.-Y.; Yang, S.-S.; Lee, S.-W.; Tsai, H.-J.; Lee, T.-Y. Cessation of Nucleos(t)ide Analogue Therapy in Non-Cirrhotic Hepatitis B Patients with Prior Severe Acute Exacerbation. J. Clin. Med. 2021, 10, 4883. https://doi.org/10.3390/jcm10214883
Lai C-Y, Yang S-S, Lee S-W, Tsai H-J, Lee T-Y. Cessation of Nucleos(t)ide Analogue Therapy in Non-Cirrhotic Hepatitis B Patients with Prior Severe Acute Exacerbation. Journal of Clinical Medicine. 2021; 10(21):4883. https://doi.org/10.3390/jcm10214883
Chicago/Turabian StyleLai, Chia-Yeh, Sheng-Shun Yang, Shou-Wu Lee, Hsin-Ju Tsai, and Teng-Yu Lee. 2021. "Cessation of Nucleos(t)ide Analogue Therapy in Non-Cirrhotic Hepatitis B Patients with Prior Severe Acute Exacerbation" Journal of Clinical Medicine 10, no. 21: 4883. https://doi.org/10.3390/jcm10214883
APA StyleLai, C.-Y., Yang, S.-S., Lee, S.-W., Tsai, H.-J., & Lee, T.-Y. (2021). Cessation of Nucleos(t)ide Analogue Therapy in Non-Cirrhotic Hepatitis B Patients with Prior Severe Acute Exacerbation. Journal of Clinical Medicine, 10(21), 4883. https://doi.org/10.3390/jcm10214883