Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity

 ,
, 
 ,
,  and
and 
Abstract
1. Introduction
2. Materials and Methods
2.1. Design
2.2. Study Population
- Healthy volunteers were people who attended the Dermatology Service for common conditions, such as melanocytic nevi or seborrheic keratoses, and did not have previous personal or family history of any inflammatory skin disease.
- Patients with psoriasis were patients with an established clinical diagnosis of mild to severe plaque-type psoriasis [25] and had a psoriasis plaque on their elbows.
- Patients with AD were patients with established clinical diagnosis of mild to severe AD [26] and had an eczematous lesion on their volar forearms.
- Psoriasis patients currently having non-plaque forms of psoriasis, e.g., erythrodermic, guttate, or pustular psoriasis, or a drug-induced form of psoriasis.
- Healthy volunteers who had previous personal history of any inflammatory skin disease.
- Clinical infection on the measured area.
- History of cancer, including skin cancer.
- Subjects with intense sun exposure during the study.
- Not signing the informed consent form.
2.3. Study Variables
2.4. Outcome Measures
- To assess differences in TEWL, SCH, and temperature values between healthy skin, psoriatic skin, and AD skin.
- To evaluate TEWL and temperature values’ ability to discriminate mild psoriasis versus moderate/severe psoriasis.
- To evaluate TEWL and temperature values’ ability to discriminate mild AD versus moderate/severe AD.
- To assess differences in other homeostasis parameters between healthy skin, psoriatic skin, and AD skin: erythema, melanin, pH, and elasticity.
- To assess differences in homeostasis parameters between mild psoriasis and moderate/severe psoriasis: TEWL, SCH, temperature, erythema, melanin, pH, and elasticity.
- To assess differences in homeostasis parameters between mild AD and moderate/severe AD: TEWL, SCH, temperature, erythema, melanin, pH, and elasticity.
2.5. Statistical Analysis
3. Results
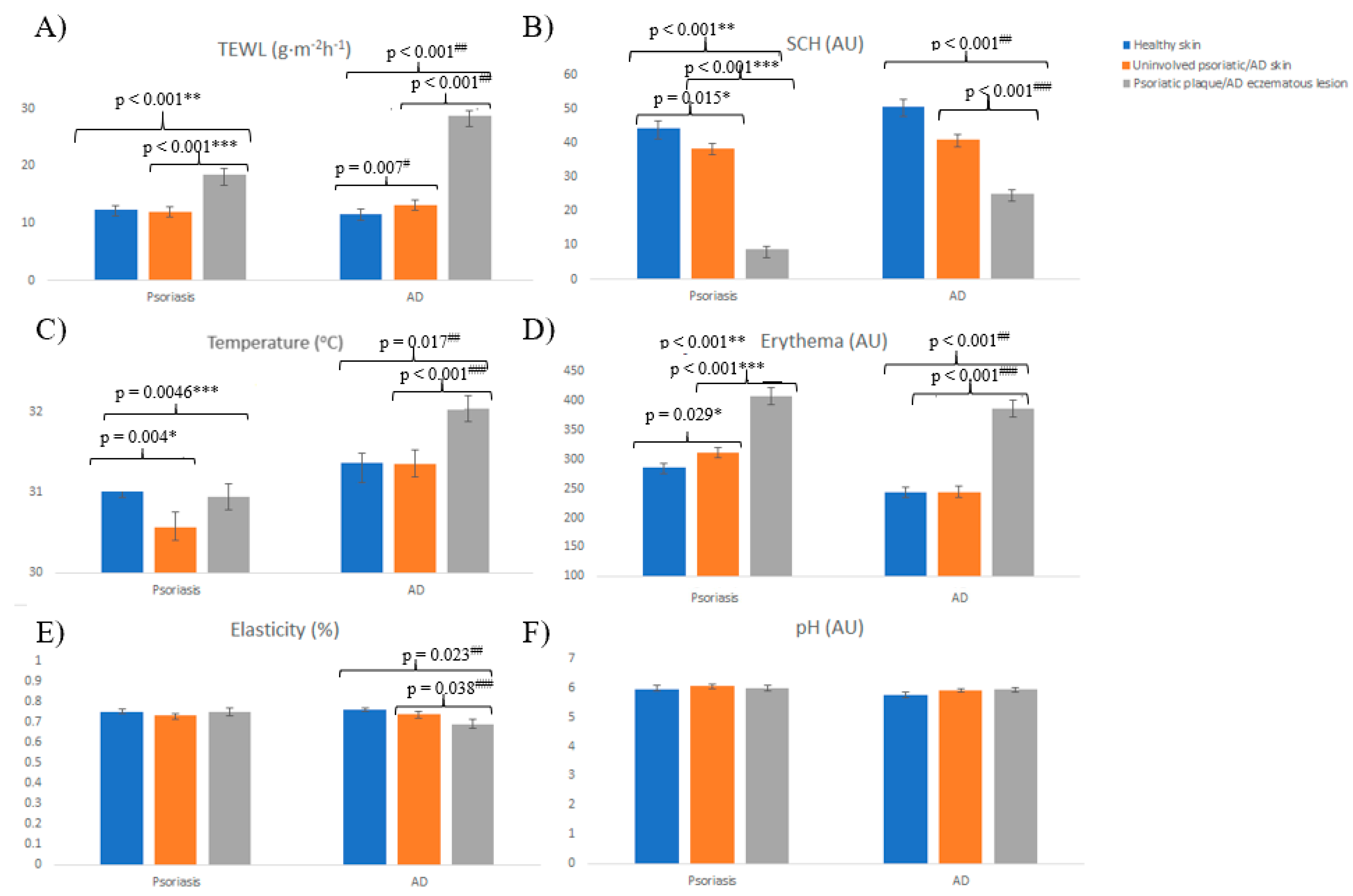
3.1. Skin Homeostasis in Psoriatic Patients
3.2. Skin Homeostasis in Atopic Dermatitis Patients
3.3. Skin Homeostasis Analysis between Psoriatic Patients and AD Patients
4. Discussion
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Clark, R.A.; Ghosh, K.; Tonnesen, M.G. Tissue engineering for cutaneous wounds. J. Investig. Dermatol. 2007, 127, 1018–1029. [Google Scholar] [CrossRef] [PubMed]
- Elias, P.M.; Choi, E.H. Interactions among stratum corneum defensive functions. Exp. Dermatol. 2005, 14, 719–726. [Google Scholar] [CrossRef]
- Kalia, Y.N.; Pirot, F.; Guy, R.H. Homogeneous transport in a heterogeneous membrane: Water diffusion across human stratum corneum in vivo. Biophys. J. 1996, 71, 2692–2700. [Google Scholar] [CrossRef]
- Fluhr, J.W.; Feingold, K.R.; Elias, P.M. Transepidermal water loss reflects permeability barrier status: Validation in human and rodent in vivo and ex vivo models. Exp. Dermatol. 2006, 15, 483–492. [Google Scholar] [CrossRef] [PubMed]
- Ye, L.; Wang, Z.; Li, Z.; Lv, C.; Man, M.Q. Validation of GPSkin Barrier((R)) for assessing epidermal permeability barrier function and stratum corneum hydration in humans. Skin Res. Technol. 2019, 25, 25–29. [Google Scholar] [CrossRef] [PubMed]
- Algiert-Zielinska, B.; Batory, M.; Skubalski, J.; Rotsztejn, H. Evaluation of the relation between lipid coat, transepidermal water loss, and skin pH. Int. J. Dermatol. 2017, 56, 1192–1197. [Google Scholar] [CrossRef] [PubMed]
- Denda, M.; Sokabe, T.; Fukumi-Tominaga, T.; Tominaga, M. Effects of skin surface temperature on epidermal permeability barrier homeostasis. J. Investig. Dermatol. 2007, 127, 654–659. [Google Scholar] [CrossRef]
- Nedelec, B.; Forget, N.J.; Hurtubise, T.; Cimino, S.; de Muszka, F.; Legault, A.; Liu, W.L.; de Oliveira, A.; Calva, V.; Correa, J.A. Skin characteristics: Normative data for elasticity, erythema, melanin, and thickness at 16 different anatomical locations. Skin Res. Technol. 2016, 22, 263–275. [Google Scholar] [CrossRef] [PubMed]
- Fajuyigbe, D.; Lwin, S.M.; Diffey, B.L.; Baker, R.; Tobin, D.J.; Sarkany, R.P.E.; Young, A.R. Melanin distribution in human epidermis affords localized protection against DNA photodamage and concurs with skin cancer incidence difference in extreme phototypes. FASEB J. 2018, 32, 3700–3706. [Google Scholar] [CrossRef]
- Khosrowpour, Z.; Ahmad Nasrollahi, S.; Ayatollahi, A.; Samadi, A.; Firooz, A. Effects of four soaps on skin trans-epidermal water loss and erythema index. J. Cosmet. Dermatol. 2019, 18, 857–861. [Google Scholar] [CrossRef]
- Yazdanparast, T.; Yazdani, K.; Humbert, P.; Khatami, A.; Ahmad Nasrollahi, S.; Hassanzadeh, H.; Ehsani, A.H.; Izadi Firouzabadi, L.; Firooz, A. Comparison of biophysical, biomechanical and ultrasonographic properties of skin in chronic dermatitis, psoriasis and lichen planus. Med. J. Islam. Repub. Iran. 2018, 32, 108. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Cerdeira, C.; Molares-Vila, A.; Sanchez-Blanco, E.; Sanchez-Blanco, B. Study on Certain Biomarkers of Inflammation in Psoriasis Through “OMICS” Platforms. Open Biochem. J. 2014, 8, 21–34. [Google Scholar] [CrossRef]
- Furue, M.; Chiba, T.; Tsuji, G.; Ulzii, D.; Kido-Nakahara, M.; Nakahara, T.; Kadono, T. Atopic dermatitis: Immune deviation, barrier dysfunction, IgE autoreactivity and new therapies. Allergol. Int 2017, 66, 398–403. [Google Scholar] [CrossRef] [PubMed]
- Jungersted, J.M.; Scheer, H.; Mempel, M.; Baurecht, H.; Cifuentes, L.; Hogh, J.K.; Hellgren, L.I.; Jemec, G.B.; Agner, T.; Weidinger, S. Stratum corneum lipids, skin barrier function and filaggrin mutations in patients with atopic eczema. Allergy 2010, 65, 911–918. [Google Scholar] [CrossRef] [PubMed]
- Cannavo, S.P.; Guarneri, F.; Giuffrida, R.; Aragona, E.; Guarneri, C. Evaluation of cutaneous surface parameters in psoriatic patients. Skin Res. Technol. 2017, 23, 41–47. [Google Scholar] [CrossRef] [PubMed]
- Chopra, R.; Silverberg, J.I. Assessing the severity of atopic dermatitis in clinical trials and practice. Clin. Dermatol. 2018, 36, 606–615. [Google Scholar] [CrossRef]
- Chalmers, R.J. Assessing psoriasis severity and outcomes for clinical trials and routine clinical practice. Dermatol. Clin. 2015, 33, 57–71. [Google Scholar] [CrossRef] [PubMed]
- Llamas-Velasco, M.; de la Cueva, P.; Notario, J.; Martinez-Pilar, L.; Martorell, A.; Moreno-Ramirez, D. Moderate Psoriasis: A Proposed Definition. Actas Dermosifiliogr. 2017, 108, 911–917. [Google Scholar] [CrossRef]
- Schmitt, J.; Wozel, G. The psoriasis area and severity index is the adequate criterion to define severity in chronic plaque-type psoriasis. Dermatology 2005, 210, 194–199. [Google Scholar] [CrossRef]
- Eichenfield, L.F.; Tom, W.L.; Chamlin, S.L.; Feldman, S.R.; Hanifin, J.M.; Simpson, E.L.; Berger, T.G.; Bergman, J.N.; Cohen, D.E.; Cooper, K.D.; et al. Guidelines of care for the management of atopic dermatitis: Section 1. Diagnosis and assessment of atopic dermatitis. J. Am. Acad. Dermatol. 2014, 70, 338–351. [Google Scholar] [CrossRef]
- Oranje, A.P.; Glazenburg, E.J.; Wolkerstorfer, A.; de Waard-van der Spek, F.B. Practical issues on interpretation of scoring atopic dermatitis: The SCORAD index, objective SCORAD and the three-item severity score. Br. J. Dermatol. 2007, 157, 645–648. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Kung, J.; Ng, W.G.; Tsang, K.; Cheng, N.S.; Leung, T.F. Are skin equipment for assessing childhood eczema any good? J. Dermatolog. Treat. 2018, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Fink, C.; Alt, C.; Uhlmann, L.; Klose, C.; Enk, A.; Haenssle, H.A. Intra- and interobserver variability of image-based PASI assessments in 120 patients suffering from plaque-type psoriasis. J. Eur. Acad. Dermatol. Venereol. 2018, 32, 1314–1319. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, M.M.; Dunn-Galvin, A.; Gray, C.; Murray, D.M.; Kiely, M.; Kenny, L.; McLean, W.H.I.; Irvine, A.D.; Hourihane, J.O. Skin barrier impairment at birth predicts food allergy at 2 years of age. J. Allergy Clin. Immunol. 2016, 137, 1111–1116.e8. [Google Scholar] [CrossRef] [PubMed]
- Boehncke, W.H.; Schon, M.P. Psoriasis. Lancet 2015, 386, 983–994. [Google Scholar] [CrossRef]
- Weidinger, S.; Novak, N. Atopic dermatitis. Lancet 2016, 387, 1109–1122. [Google Scholar] [CrossRef]
- Takahashi, H.; Tsuji, H.; Minami-Hori, M.; Miyauchi, Y.; Iizuka, H. Defective barrier function accompanied by structural changes of psoriatic stratum corneum. J. Dermatol. 2014, 41, 144–148. [Google Scholar] [CrossRef]
- Nikam, V.N.; Monteiro, R.C.; Dandakeri, S.; Bhat, R.M. Transepidermal Water Loss in Psoriasis: A Case-control Study. Indian Dermatol. Online J. 2019, 10, 267–271. [Google Scholar] [CrossRef]
- Lee, Y.; Je, Y.J.; Lee, S.S.; Li, Z.J.; Choi, D.K.; Kwon, Y.B.; Sohn, K.C.; Im, M.; Seo, Y.J.; Lee, J.H. Changes in transepidermal water loss and skin hydration according to expression of aquaporin-3 in psoriasis. Ann. Dermatol. 2012, 24, 168–174. [Google Scholar] [CrossRef]
- Delfino, M.; Russo, N.; Migliaccio, G.; Carraturo, N. Experimental study on efficacy of thermal muds of Ischia Island combined with balneotherapy in the treatment of psoriasis vulgaris with plaques. Clin. Ter. 2003, 154, 167–171. [Google Scholar]
- Gran, F.; Kerstan, A.; Serfling, E.; Goebeler, M.; Muhammad, K. Current Developments in the Immunology of Psoriasis. Yale J. Biol. Med. 2020, 93, 97–110. [Google Scholar] [PubMed]
- Bozek, A.; Reich, A. The reliability of three psoriasis assessment tools: Psoriasis area and severity index, body surface area and physician global assessment. Adv. Clin. Exp. Med. 2017, 26, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Yatagai, T.; Shimauchi, T.; Yamaguchi, H.; Sakabe, J.I.; Aoshima, M.; Ikeya, S.; Tatsuno, K.; Fujiyama, T.; Ito, T.; Ojima, T.; et al. Sensitive skin is highly frequent in extrinsic atopic dermatitis and correlates with disease severity markers but not necessarily with skin barrier impairment. J. Dermatol. Sci. 2018, 89, 33–39. [Google Scholar] [CrossRef]
- Laudanska, H.; Reduta, T.; Szmitkowska, D. Evaluation of skin barrier function in allergic contact dermatitis and atopic dermatitis using method of the continuous TEWL measurement. Rocz. Akad. Med. Bialymst. 2003, 48, 123–127. [Google Scholar] [PubMed]
- Gupta, J.; Grube, E.; Ericksen, M.B.; Stevenson, M.D.; Lucky, A.W.; Sheth, A.P.; Assa’ad, A.H.; Khurana Hershey, G.K. Intrinsically defective skin barrier function in children with atopic dermatitis correlates with disease severity. J. Allergy Clin. Immunol. 2008, 121, 725–730.e2. [Google Scholar] [CrossRef]
- Knor, T.; Meholjic-Fetahovic, A.; Mehmedagic, A. Stratum corneum hydration and skin surface pH in patients with atopic dermatitis. Acta Dermatovenerol. Croat. 2011, 19, 242–247. [Google Scholar]
- Thyssen, J.P.; Kezic, S. Causes of epidermal filaggrin reduction and their role in the pathogenesis of atopic dermatitis. J. Allergy Clin. Immunol. 2014, 134, 792–799. [Google Scholar] [CrossRef] [PubMed]
- Brunner, P.M.; Guttman-Yassky, E.; Leung, D.Y. The immunology of atopic dermatitis and its reversibility with broad-spectrum and targeted therapies. J. Allergy Clin. Immunol. 2017, 139, S65–S76. [Google Scholar] [CrossRef]
- Yazdanparast, T.; Yazdani, K.; Humbert, P.; Khatami, A.; Nasrollahi, S.A.; Firouzabadi, L.I.; Firooz, A. Biophysical Measurements and Ultrasonographic Findings in Chronic Dermatitis in Comparison with Uninvolved Skin. Indian J. Dermatol. 2019, 64, 90–96. [Google Scholar] [CrossRef]
- Van Doren, S.R. Matrix metalloproteinase interactions with collagen and elastin. Matrix Biol. 2015, 44-46, 224–231. [Google Scholar] [CrossRef]
- Hon, K.L.; Kung, J.S.C.; Tsang, K.Y.C.; Yu, J.W.S.; Cheng, N.S.; Leung, T.F. Do we need another symptom score for childhood eczema? J. Dermatolog. Treat. 2018, 29, 510–514. [Google Scholar] [CrossRef] [PubMed]
- Hon, K.L.; Lam, P.H.; Ng, W.G.; Kung, J.S.; Cheng, N.S.; Lin, Z.X.; Chow, C.M.; Leung, T.F. Age, sex, and disease status as determinants of skin hydration and transepidermal water loss among children with and without eczema. Hong Kong Med. J. 2020, 26, 19–26. [Google Scholar] [CrossRef] [PubMed]
- Rehbinder, E.M.; Advocaat Endre, K.M.; Lodrup Carlsen, K.C.; Asarnoj, A.; Stensby Bains, K.E.; Berents, T.L.; Carlsen, K.H.; Gudmundsdottir, H.K.; Haugen, G.; Hedlin, G.; et al. Predicting Skin Barrier Dysfunction and Atopic Dermatitis in Early Infancy. J. Allergy Clin. Immunol. Pract. 2020, 8, 664–673.e5. [Google Scholar] [CrossRef] [PubMed]
- Kelleher, M.; Dunn-Galvin, A.; Hourihane, J.O.; Murray, D.; Campbell, L.E.; McLean, W.H.; Irvine, A.D. Skin barrier dysfunction measured by transepidermal water loss at 2 days and 2 months predates and predicts atopic dermatitis at 1 year. J. Allergy Clin. Immunol. 2015, 135, 930–935.e1. [Google Scholar] [CrossRef] [PubMed]


{kind=link}
| Sociodemographic Features | Psoriatic Patients (n = 92) | Healthy Participants assessed on the Elbow (n = 92) | Atopic Dermatitis Patients (n = 65) | Healthy Participants assessed on the Volar Forearm (n = 65) |
|---|---|---|---|---|
| Age (years) | 48.63 (15.70) | 42.06 (18.59) | 28.14 (19.59) | 35.96 (19.03) |
| Sex (%) | ||||
| Female | 46 (50%) | 57 (62%) | 42 (64.6%) | 48 (73.8%) |
| Male | 46 (50%) | 35 (38%) | 23 (35.4%) | 17 (26.2%) |
| Smoking habit (yes) | 31 (33.7%) | 12 (13%) | 7 (10.8%) | 6 (9.23%) |
| Alcohol habit (yes) | 29 (31.5%) | 29 (31.5%) | 15 (23.1%) | 10 (15.4%) |
| Family history of psoriasis/atopic dermatitis (yes) | 43 (46.7%) | 12 (13%) | 32 (49.2%) | 7 (10.8%) |
| Emollients use (yes) | 51 (55.4%) | 35 (38%) | 51 (78.5%) | 28 (43.1%) |
| Treatment | ||||
| Topical treatment | 49 (53.26%) | 39 (60%) | ||
| Systemic treatment | 23 (25%) | 26 (40%) | ||
| Biologic drugs | 20 (21.7%) | 0 |
| Skin Homeostasis Parameters | Psoriatic Patients with PASI < 7 (n = 59) | Psoriatic Patients with PASI ≥ 7 (n = 33) | p Value | p Value | ||
|---|---|---|---|---|---|---|
| Uninvolved Psoriatic Skin | Psoriatic Plaques | Uninvolved Psoriatic Skin | Psoriatic Plaques | p * | p ** | |
| TEWL (g·m−2·h−1) | 12.18 (7.52) | 17.16 (9.58) | 11.86 (8.78) | 20.75 (11.22) | 0.855 | 0.109 |
| SCH (AU) | 37.76 (13.13) | 10.91 (9.76) | 39.63 (14.69) | 4.78 (5.24) | 0.531 | <0.001 ** |
| Temperature (°C) | 30.51 (2.00) | 30.62 (1.65) | 30.66 (1.09) | 31.56 (1.13) | 0.639 | 0.005 ** |
| Erythema (AU) | 311.78 (73.15) | 404.37 (73.76) | 311.34 (69.90) | 412.79 (67.91) | 0.981 | 0.648 |
| Melanin (AU) | 246.49 (81.63) | 193.65 (69.98) | 230.05 (75.64) | 188.36 (69.30) | 0.422 | 0.770 |
| pH | 6.01 (0.64) | 6.06 (1.01) | 6.12 (0.56) | 5.90 (0.87) | 0.422 | 0.468 |
| Elasticity (%) | 0.74 (0.13) | 0.77 (0.20) | 0.69 (0.15) | 0.72 (0.17) | 0.110 | 0.251 |
| Skin Homeostasis Parameters | Cut-off Value | Sensitivity | Specificity | OR | p |
|---|---|---|---|---|---|
| Temperature (°C) | 30.85 | 72.7% | 55.9% | 3.39 | 0.010 * |
| TEWL (g·m−2 h−1) | 13.85 | 81.8% | 50.8% | 4.66 | 0.003 * |
| SCH (AU) | 2.07 | 39.4% | 84.7% | 0.28 | 0.011 * |
| Two criteria (temperature > 30.85 + TEWL > 13.85) | - | 60.6% | 76.3% | 4.95 | 0.001 * |
| Skin Homeostasis Parameters | AD Patients with SCORAD < 37 (n = 26) | AD Patients with SCORAD ≥ 37 (n = 34) | p Value | p Value | ||
|---|---|---|---|---|---|---|
| Uninvolved AD Skin | AD Eczematous Lesion | Uninvolved AD Skin | AD Eczematous Lesion | p * | p ** | |
| TEWL (g·m−2 h−1) | 10.88 (8.04) | 26.33 (15.34) | 13.75 (6.62) | 31.67 (13.74) | 0.135 | 0.161 |
| SCH (AU) | 47.10 (17.01) | 30.68 (24.23) | 34.78 (13.55) | 19.90 (11.40) | 0.003 * | 0.044 ** |
| Temperature (°C) | 31.30 (1.04) | 31.74 (1.00) | 31.35 (1.46) | 32.45 (1.15) | 0.891 | 0.015 ** |
| Erythema (AU) | 201.05 (17.30) | 351.78 (102.64) | 254.93 (78.78) | 395.71 (77.71) | 0.004 * | 0.361 |
| Melanin (AU) | 168.91 (37.39) | 1990.04 (23.33) | 212.55 (82.57) | 215.24 (88.88) | 0.221 | 0.298 |
| pH | 5.79 (0.62) | 5.87 (0.61) | 6.04 (0.41) | 6.03 (0.47) | 0.97 | 0.274 |
| Elasticity (%) | 0.79 (0.11) | 0.75 (0.12) | 0.67 (0.16) | 0.63 (0.20) | 0.003 * | 0.01 ** |
| Skin Homeostasis Parameters | Cut-off Value | Sensitivity | Specificity | OR | p |
|---|---|---|---|---|---|
| Temperature (°C) | 31.75 | 81.8% | 57.7% | 6.14 | 0.003 * |
| TEWL (g·m−2 h−1) | 23.19 | 73.5% | 53.8% | 3.24 | 0.034 * |
| SCH (AU) | 14.54 | 71.9% | 23.1% | 0.77 | 0.663 |
| Two criteria (temperature > 31.75 + TEWL > 23.19) | - | 69.2% | 61.8% | 3.64 | 0.19 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Share and Cite
Montero-Vilchez, T.; Segura-Fernández-Nogueras, M.-V.; Pérez-Rodríguez, I.; Soler-Gongora, M.; Martinez-Lopez, A.; Fernández-González, A.; Molina-Leyva, A.; Arias-Santiago, S. Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity. J. Clin. Med. 2021, 10, 359. https://doi.org/10.3390/jcm10020359
Montero-Vilchez T, Segura-Fernández-Nogueras M-V, Pérez-Rodríguez I, Soler-Gongora M, Martinez-Lopez A, Fernández-González A, Molina-Leyva A, Arias-Santiago S. Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity. Journal of Clinical Medicine. 2021; 10(2):359. https://doi.org/10.3390/jcm10020359
Chicago/Turabian StyleMontero-Vilchez, Trinidad, María-Victoria Segura-Fernández-Nogueras, Isabel Pérez-Rodríguez, Miguel Soler-Gongora, Antonio Martinez-Lopez, Ana Fernández-González, Alejandro Molina-Leyva, and Salvador Arias-Santiago. 2021. "Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity" Journal of Clinical Medicine 10, no. 2: 359. https://doi.org/10.3390/jcm10020359
APA StyleMontero-Vilchez, T., Segura-Fernández-Nogueras, M.-V., Pérez-Rodríguez, I., Soler-Gongora, M., Martinez-Lopez, A., Fernández-González, A., Molina-Leyva, A., & Arias-Santiago, S. (2021). Skin Barrier Function in Psoriasis and Atopic Dermatitis: Transepidermal Water Loss and Temperature as Useful Tools to Assess Disease Severity. Journal of Clinical Medicine, 10(2), 359. https://doi.org/10.3390/jcm10020359