
Fertility-Sparing Surgery for Ovarian Cancer

Abstract
:1. Introduction
2. Materials and Methods
3. Borderline Ovarian Tumors
3.1. Modalities of Fertility-Sparing Surgery and Clinical Outcomes
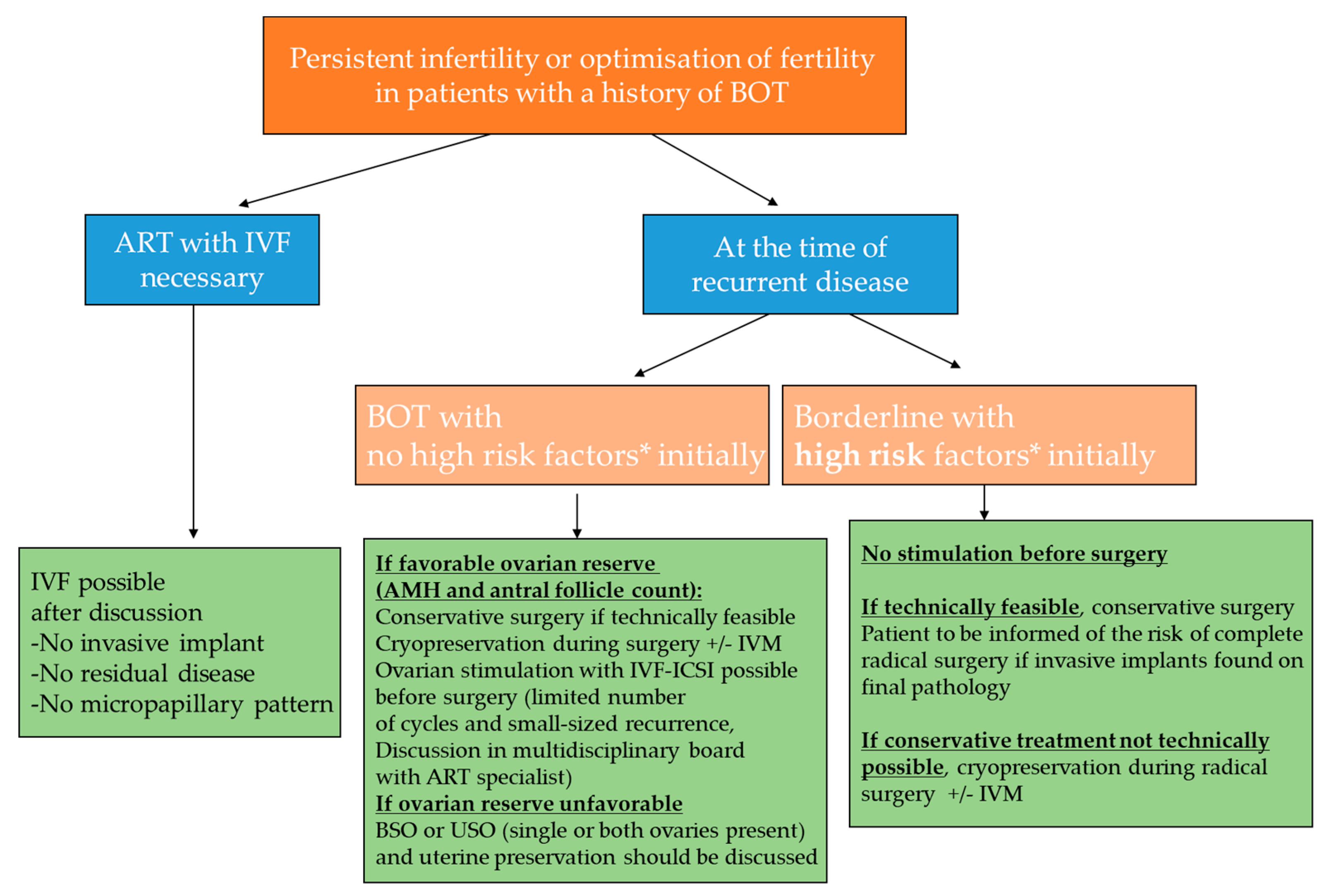
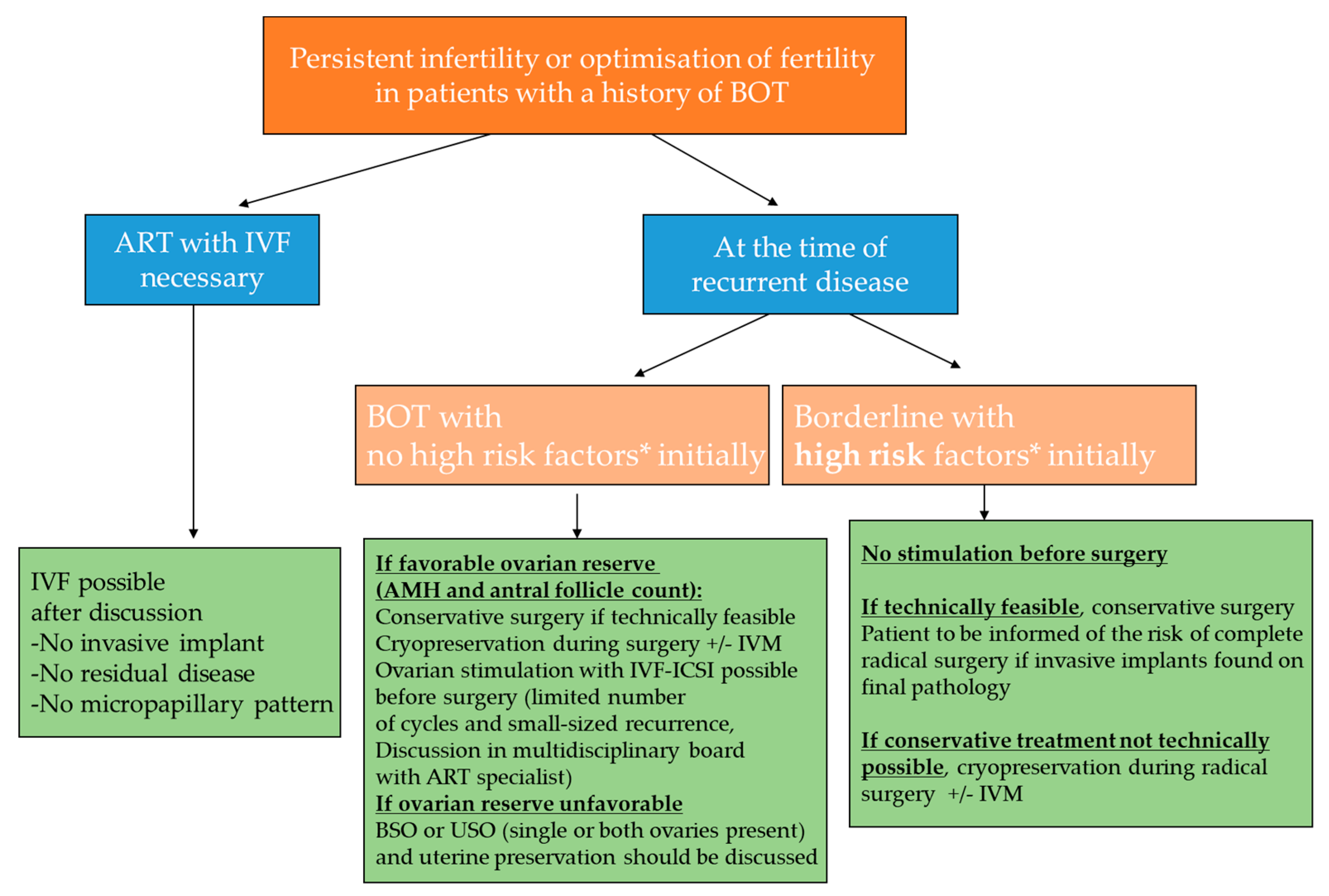
- (1)
- Magnetic resonance imaging (MRI) to assess possible healthy functional ovarian tissue.
- (2)
- An oncofertility consultation to discuss whether a preoperative fertility preservation technique could be performed.
3.2. Survival of Patients after Fertility-Sparing Surgery
3.3. Fertility Results after Fertility-Sparing Surgery
4. Epithelial Ovarian Cancer
4.1. Indications of Fertility-Sparing Surgery
4.2. Fertility Results
5. Non-Epithelial Ovarian Cancer
5.1. Malignant Ovarian Germ Cell Tumors
5.2. Sex Cord Stromal Tumors
6. Conclusions
Author Contributions
Funding
Conflicts of Interest
References
- La Rosa, V.L.; Garzon, S.; Gullo, G.; Fichera, M.; Sisti, G.; Gallo, P.; Riemma, G.; Schiattarella, A. Fertility preservation in women affected by gynaecological cancer: The importance of an integrated gynaecological and psychological approach. Ecancermedicalscience 2020, 14, 1035. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Wallberg, K.A.; Hao, X.; Marklund, A.; Johansen, G.; Borgström, B.; Lundberg, F.E. Hot Topics on Fertility Preservation for Women and Girls-Current Research, Knowledge Gaps, and Future Possibilities. J. Clin. Med. 2021, 10, 1650. [Google Scholar] [CrossRef]
- Ray-Coquard, I.; Morice, P.; Lorusso, D.; Prat, J.; Oaknin, A.; Pautier, P.; Colombo, N. Non-epithelial ovarian cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2018, 4, iv1–iv18. [Google Scholar] [CrossRef]
- Colombo, N.; Sessa, C.; du Bois, A.; Ledermann, J.; McCluggage, W.G.; McNeish, I.; Morice, P.; Pignata, S.; Ray-Coquard, I.; Vergote, I.; et al. ESMO-ESGO consensus conference recommendations on ovarian cancer: Pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Ann. Oncol. 2019, 30, 672–705. [Google Scholar] [CrossRef] [Green Version]
- Leary, A.; Petrella, M.C.; Pautier, P.; Duvillard, P.; Uzan, C.; Tazi, Y.; Ledoux, F.; Gouy, S.; Morice, P.; Lhommé, C. Adjuvant platinum-based chemotherapy for borderline serous ovarian tumors with invasive implants. Gynecol. Oncol. 2014, 132, 237. [Google Scholar] [CrossRef]
- Trimble, C.L.; Kosary, C.; Trimble, E.L. Long-term survival and patterns of care in women with ovarian tumors of low malignant potential. Gynecol. Oncol. 2002, 86, 34–37. [Google Scholar] [CrossRef]
- Daraï, E.; Fauvet, R.; Uzan, C.; Gouy, S.; Duvillard, P.; Morice, P. Fertility and borderline ovarian tumor: A systematic review of conservative management, risk of recurrence and alternative options. Hum. Reprod. Update 2013, 19, 151–166. [Google Scholar] [CrossRef] [PubMed]
- Palomba, S.; Zupi, E.; Russo, T.; Falbo, A.; Del Negro, S.; Manguso, F.; Marconi, D.; Tolino, A.; Zullo, F. Comparison of two fertility-sparing approaches for bilateral borderline ovarian tumours: A randomized controlled study. Hum. Reprod. 2007, 22, 578–585. [Google Scholar] [CrossRef] [Green Version]
- Palomba, S.; Falbo, A.; Del Negro, S.; Rocca, M.; Russo, T.; Cariati, F.; Annunziata, G.; Tolino, A.; Tagliaferri, P.; Zullo, F. Ultra-conservative fertility-sparing strategy for bilateral borderline ovarian tumours: An 11-year follow-up. Hum. Reprod. 2010, 25, 1966–1972. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Bendifallah, S.; Ballester, M.; Uzan, C.; Fauvet, R.; Morice, P.; Darai, E. Nomogram to predict recurrence in patients with early- and advanced-stage mucinous and serous borderline ovarian tumors. Am. J. Obstet. Gynecol. 2014, 211, 637.e1-6. [Google Scholar] [CrossRef] [PubMed]
- Morice, P.; Uzan, C.; Fauvet, R.; Gouy, S.; Duvillard, P.; Darai, E. Borderline ovarian tumour: Pathological diagnostic dilemma and risk factors for invasive or lethal recurrence. Lancet Oncol. 2012, 13, e103–e115. [Google Scholar] [CrossRef]
- Gouy, S.; Maria, S.; Faron, M.; Maulard, A.; Pautier, P.; Leary, A.; Chargari, C.; Genestie, C.; Morice, P. Results After Conservative Surgery of Stage II/III Serous Borderline Ovarian Tumors. Ann. Surg. Oncol. 2021, 28, 3597–3604. [Google Scholar] [CrossRef]
- Uzan, C.; Nikpayam, M.; Ribassin-Majed, L.; Gouy, S.; Bendifallah, S.; Cortez, A.; Rey, A.; Duvillard, P.; Darai, E.; Morice, P. Influence of histological subtypes on the risk of an invasive recurrence in a large series of stage I borderline ovarian tumor including 191 conservative treatments. Ann. Oncol. 2014, 25, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Jia, S.-Z.; Xiang, Y.; Yang, J.-J.; Shi, J.-H.; Jia, C.-W.; Leng, J.-H. Oncofertility outcomes after fertility-sparing treatment of bilateral serous borderline ovarian tumors: Results of a large retrospective study. Hum. Reprod. 2020, 35, 328–339. [Google Scholar] [CrossRef] [PubMed]
- du Bois, A.; Ewald-Riegler, N.; de Gregorio, N.; Reuss, A.; Mahner, S.; Fotopoulou, C.; Kommoss, F.; Schmalfeldt, B.; Hilpert, F.; Fehm, T.; et al. Borderline tumours of the ovary: A cohort study of the Arbeitsgmeinschaft Gynäkologische Onkologie (AGO) Study Group. Eur. J. Cancer 2013, 49, 1905–1914. [Google Scholar] [CrossRef] [PubMed]
- Boran, N.; Cil, A.P.; Tulunay, G.; Ozturkoglu, E.; Koc, S.; Bulbul, D.; Kose, M.F. Fertility and recurrence results of conservative surgery for borderline ovarian tumors. Gynecol. Oncol. 2005, 97, 845–851. [Google Scholar] [CrossRef]
- Fauvet, R.; Poncelet, C.; Boccara, J.; Descamps, P.; Fondrinier, E.; Daraï, E. Fertility after conservative treatment for borderline ovarian tumors: A French multicenter study. Fertil. Steril. 2005, 83, 284–290. [Google Scholar] [CrossRef]
- Park, J.-Y.; Kim, D.-Y.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Nam, J.-H. Surgical management of borderline ovarian tumors: The role of fertility-sparing surgery. Gynecol. Oncol. 2009, 113, 75–82. [Google Scholar] [CrossRef]
- Kanat-Pektas, M.; Ozat, M.; Gungor, T.; Dikici, T.; Yilmaz, B.; Mollamahmutoglu, L. Fertility outcome after conservative surgery for borderline ovarian tumors: A single center experience. Arch. Gynecol. Obstet. 2011, 284, 1253–1258. [Google Scholar] [CrossRef]
- Koskas, M.; Uzan, C.; Gouy, S.; Pautier, P.; Lhommé, C.; Haie-Meder, C.; Duvillard, P.; Morice, P. Fertility determinants after conservative surgery for mucinous borderline tumours of the ovary (excluding peritoneal pseudomyxoma). Hum. Reprod. 2011, 26, 808–814. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Song, T.; Choi, C.H.; Kim, H.J.; Lee, W.; Lee, Y.Y.; Kim, T.J.; Lee, J.W.; Bae, D.S.; Kim, B.G. Oncologic and reproductive outcomes in patients with advanced-stage borderline ovarian tumors. Eur. J. Obstet. Gynecol. Reprod. Biol. 2011, 156, 204–208. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.Y.; Choi, M.C.; Kwon, B.R.; Jung, S.G.; Park, H.; Joo, W.D.; Lee, C.; Lee, J.H.; Lee, J.M. Oncologic and obstetric outcomes of conservative surgery for borderline ovarian tumors in women of reproductive age. Obstet. Gynecol. Sci. 2017, 60, 289–295. [Google Scholar] [CrossRef] [PubMed]
- Delle Marchette, M.; Ceppi, L.; Andreano, A.; Bonazzi, C.M.; Buda, A.; Grassi, T.; Giuliani, D.; Sina, F.; Lamanna, M.; Bianchi, T.; et al. Oncologic and fertility impact of surgical approach for borderline ovarian tumours treated with fertility sparing surgery. Eur. J. Cancer 2019, 111, 61–68. [Google Scholar] [CrossRef] [PubMed]
- Lu, Z.; Li, B.; Gu, C. Outcomes of fertility-sparing surgery for stage II and III serous borderline ovarian tumors. J. Int. Med. Res. 2019, 47, 4895–4903. [Google Scholar] [CrossRef] [PubMed]
- Candotti, G.; Peiretti, M.; Mangili, G.; Bergamini, A.; Candiani, M.; Cioffi, R.; Mais, V.; Rabaiotti, E.; Bocciolone, L. What women want: Fertility sparing surgery in Borderline ovarian tumours patients and pregnancy outcome. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2020, 46, 888–892. [Google Scholar] [CrossRef] [PubMed]
- Chevrot, A.; Pouget, N.; Bats, A.S.; Huchon, C.; Guyon, F.; Chopin, N.; Rousset-Jablonski, C.; Beurrier, F.; Lambaudie, E.; Provansal, M.; et al. Fertility and prognosis of borderline ovarian tumor after conservative management: Results of the multicentric OPTIBOT study by the GINECO & TMRG group. Gynecol. Oncol. 2020, 157, 29–35. [Google Scholar] [PubMed]
- Plett, H.; Harter, P.; Ataseven, B.; Heitz, F.; Prader, S.; Schneider, S.; Heikaus, S.; Fisseler-Eckhoff, A.; Kommoss, F.; Lax, S.F.; et al. Fertility-sparing surgery and reproductive-outcomes in patients with borderline ovarian tumors. Gynecol. Oncol. 2020, 157, 411–417. [Google Scholar] [CrossRef] [PubMed]
- Trillsch, F.; Mahner, S.; Woelber, L.; Vettorazzi, E.; Reuss, A.; Ewald-Riegler, N.; de Gregorio, N.; Fotopoulou, C.; Schmalfeldt, B.; Burges, A.; et al. Age-dependent differences in borderline ovarian tumours (BOT) regarding clinical characteristics and outcome: Results from a sub-analysis of the Arbeitsgemeinschaft Gynaekologische Onkologie (AGO) ROBOT study. Ann. Oncol. 2014, 25, 1320–1327. [Google Scholar] [CrossRef]
- Fauvet, R.; Demblocque, E.; Morice, P.; Querleu, D.; Daraï, E. Behavior of serous borderline ovarian tumors with and without micropapillary patterns: Results of a French multicenter study. Ann. Surg. Oncol. 2012, 19, 941–947. [Google Scholar] [CrossRef]
- Ouldamer, L.; Bendifallah, S.; Naoura, I.; Body, G.; Uzan, C.; Morice, P.; Ballester, M.; Daraï, E. Nomogram to predict live birth rate after fertility-sparing surgery for borderline ovarian tumours. Hum. Reprod. 2016, 31, 1732–1737. [Google Scholar] [CrossRef]
- Jiao, X.; Hu, J.; Zhu, L. Prognostic Factors for Recurrence After Fertility-Preserving Surgery in Patients with Borderline Ovarian Tumors: A Systematic Review and Meta-analysis of Observational Studies. Int. J. Gynecol. Cancer 2017, 27, 1833–1841. [Google Scholar] [CrossRef]
- Rizzuto, I.; Behrens, R.F.; Smith, L.A. Risk of ovarian cancer in women treated with ovarian stimulating drugs for infertility. Cochrane Database Syst. Rev. 2013, 8, CD008215. [Google Scholar] [CrossRef] [PubMed]
- Basille, C.; Olivennes, F.; Le Calvez, J.; Beron-Gaillard, N.; Meduri, G.; Lhommé, C.; Duvillard, P.; Benard, J.; Morice, P. Impact of gonadotrophins and steroid hormones on tumour cells derived from borderline ovarian tumours. Hum. Reprod. 2006, 21, 3241–3245. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Nijman, H.W.; Burger, C.W.; Baak, J.P.; Schats, R.; Vermorken, J.B.; Kenemans, P. Borderline malignancy of the ovary and controlled hyperstimulation, a report of 2 cases. Eur. J. Cancer 1992, 28, 1971–1973. [Google Scholar] [CrossRef]
- Mantzavinos, T.; Kanakas, N.; Genatas, C.; Papadias, K.; Zourlas, P.A. Five years’ follow-up in two patients with borderline tumours of the ovary hyperstimulated by gonadotrophin therapy for in-vitro fertilization. Hum. Reprod. 1994, 9, 2032–2033. [Google Scholar] [CrossRef]
- Lawal, A.H.; B-Lynch, C. Borderline ovarian cancer, bilateral surgical castration, chemotherapy and a normal delivery after ovum donation and in vitro fertilisation-embryo transfer. Br. J. Obstet. Gynaecol. 1996, 103, 931–932. [Google Scholar] [CrossRef] [PubMed]
- Hoffman, J.S.; Laird, L.; Benadiva, C.; Dreiss, R. In vitro fertilization following conservative management of stage 3 serous borderline tumor of the ovary. Gynecol Oncol. 1999, 74, 515–518. [Google Scholar] [CrossRef]
- Gallot, D.; Pouly, J.L.; Janny, L.; Mage, G.; Canis, M.; Wattiez, A.; Bruhat, M.A. Successful transfer of frozen-thawed embryos obtained immediately before radical surgery for stage IIIa serous borderline ovarian tumour: Case report. Hum. Reprod. 2000, 15, 2347–2350. [Google Scholar] [CrossRef] [Green Version]
- Morris, R.T.; Gershenson, D.M.; Silva, E.G.; Follen, M.; Morris, M.; Wharton, J.T. Outcome and reproductive function after conservative surgery for borderline ovarian tumors. Obstet. Gynecol. 2000, 95, 541–547. [Google Scholar]
- Beiner, M.E.; Gotlieb, W.H.; Davidson, B.; Kopolovic, J.; Ben-Baruch, G. Infertility treatment after conservative management of borderline ovarian tumors. Cancer 2001, 92, 320–325. [Google Scholar] [CrossRef]
- Attar, E.; Berkman, S.; Topuz, S.; Baysal, B.; Akhan, S.; Chambers, J.T. Evolutive peritoneal disease after conservative management and the use of infertility drugs in a patient with stage IIIC borderline micro-papillary serous carcinoma (MPSC) of the ovary: Case report. Hum. Reprod. 2004, 19, 1472–1475. [Google Scholar] [CrossRef] [Green Version]
- Fasouliotis, S.J.; Davis, O.; Schattman, G.; Spandorfer, S.D.; Kligman, I.; Rosenwaks, Z. Safety and efficacy of infertility treatment after conservative management of borderline ovarian tumors: A preliminary report. Fertil. Steril. 2004, 82, 568–572. [Google Scholar] [CrossRef] [PubMed]
- Marcickiewicz, J.; Brännström, M. Fertility preserving surgical treatment of borderline ovarian tumour: Long-term consequence for fertility and recurrence. Acta. Obstet. Gynecol. Scand. 2006, 85, 1496–1500. [Google Scholar] [CrossRef] [PubMed]
- Fortin, A.; Morice, P.; Thoury, A.; Camatte, S.; Dhainaut, C.; Madelenat, P. Impact of infertility drugs after treatment of borderline ovarian tumors: Results of a retrospective multicenter study. Fertil. Steril. 2007, 87, 591–596. [Google Scholar] [CrossRef] [PubMed]
- Park, C.W.; Yang, K.M.; Kim, H.O.; Hong, S.R.; Kim, T.J.; Lim, K.T.; Lee, K.H.; Kang, I.S. Outcomes of controlled ovarian hyperstimulation/in vitro fertilization for infertile patients with borderline ovarian tumor after conservative treatment. J. Korean. Med. Sci. 2007, 22, S134–S138. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Yinon, Y.; Beiner, M.E.; Gotlieb, W.H.; Korach, Y.; Perri, T.; Ben-Baruch, G. Clinical outcome of cystectomy compared with unilateral salpingo-oophorectomy as fertility-sparing treatment of borderline ovarian tumors. Fertil. Steril. 2007, 88, 479–484. [Google Scholar] [CrossRef]
- Porcu, E.; Venturoli, S.; Damiano, G.; Ciotti, P.M.; Notarangelo, L.; Paradisi, R.; Moscarini, M.; Ambrosini, G. Healthy twins delivered after oocyte cryopreservation and bilateral ovariectomy for ovarian cancer. Reprod. Biomed. Online 2008, 17, 265–267. [Google Scholar] [CrossRef]
- Cabenda-Narain, N.E.; Jansen, F.W.; Dieben, S.W.M.; Verburg, H.J.; Gaarenstroom, K.N. Conservatively treated borderline ovarian tumours, followed by IVF treatment: A case series. J. Obstet. Gynaecol. 2011, 31, 327–329. [Google Scholar] [CrossRef]
- Childress, K.J.; Patil, N.M.; Muscal, J.A.; Dietrich, J.E.; Venkatramani, R. Borderline Ovarian Tumor in the Pediatric and Adolescent Population: A Case Series and Literature Review. J. Pediatr. Adolesc. Gynecol. 2018, 31, 48–54. [Google Scholar] [CrossRef]
- Nasioudis, D.; Alevizakos, M.; Holcomb, K.; Witkin, S.S. Malignant and borderline epithelial ovarian tumors in the pediatric and adolescent population. Maturitas 2017, 96, 45–50. [Google Scholar] [CrossRef]
- Zanetta, G.; Chiari, S.; Rota, S.; Bratina, G.; Maneo, A.; Torri, V.; Mangioni, C. Conservative surgery for stage I ovarian carcinoma in women of childbearing age. Br. J. Obstet. Gynaecol. 1997, 104, 1030–1035. [Google Scholar] [CrossRef] [PubMed]
- Schilder, J.M.; Thompson, A.M.; DePriest, P.D.; Ueland, F.R.; Cibull, M.L.; Kryscio, R.J.; Modesitt, S.C.; Lu, K.H.; Geisler, J.P.; Higgins, R.V.; et al. Outcome of reproductive age women with stage IA or IC invasive epithelial ovarian cancer treated with fertility-sparing therapy. Gynecol. Oncol. 2002, 87, 1–7. [Google Scholar] [CrossRef]
- Morice, P.; Leblanc, E.; Rey, A.; Baron, M.; Querleu, D.; Blanchot, J.; Duvillard, P.; Lhommé, C.; Castaigne, D.; Classe, J.M.; et al. Conservative treatment in epithelial ovarian cancer: Results of a multicentre study of the GCCLCC (Groupe des Chirurgiens de Centre de Lutte Contre le Cancer) and SFOG (Société Francaise d’Oncologie Gynécologique). Hum. Reprod. 2005, 20, 1379–1385. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Borgfeldt, C.; Iosif, C.; Måsbäck, A. Fertility-sparing surgery and outcome in fertile women with ovarian borderline tumors and epithelial invasive ovarian cancer. Eur. J. Obstet. Gynecol. Reprod. Biol. 2007, 134, 110–114. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Park, J.-Y.; Kim, D.-Y.; Suh, D.-S.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Nam, J.H. Outcomes of fertility-sparing surgery for invasive epithelial ovarian cancer: Oncologic safety and reproductive outcomes. Gynecol. Oncol. 2008, 110, 345–353. [Google Scholar] [CrossRef] [PubMed]
- Anchezar, J.P.; Sardi, J.; Soderini, A. Long-term follow-up results of fertility sparing surgery in patients with epithelial ovarian cancer. J. Surg. Oncol. 2009, 100, 55–58. [Google Scholar] [CrossRef]
- Schlaerth, A.C.; Chi, D.S.; Poynor, E.A.; Barakat, R.R.; Brown, C.L. Long-term survival after fertility-sparing surgery for epithelial ovarian cancer. Int. J. Gynecol. Cancer 2009, 19, 1199–1204. [Google Scholar] [CrossRef]
- Kwon, Y.-S.; Hahn, H.-S.; Kim, T.-J.; Lee, I.-H.; Lim, K.-T.; Lee, K.-H.; Shim, J.U.; Mok, J.E. Fertility preservation in patients with early epithelial ovarian cancer. J. Gynecol. Oncol. 2009, 20, 44–47. [Google Scholar] [CrossRef] [Green Version]
- Wright, J.D.; Shah, M.; Mathew, L.; Burke, W.M.; Culhane, J.; Goldman, N.; Schiff, P.B.; Herzog, T.J. Fertility preservation in young women with epithelial ovarian cancer. Cancer 2009, 115, 4118–4126. [Google Scholar] [CrossRef]
- Satoh, T.; Hatae, M.; Watanabe, Y.; Yaegashi, N.; Ishiko, O.; Kodama, S.; Yamaguchi, S.; Ochiai, K.; Takano, M.; Yokota, H.; et al. Outcomes of fertility-sparing surgery for stage I epithelial ovarian cancer: A proposal for patient selection. J. Clin. Oncol. 2010, 28, 1727–1732. [Google Scholar] [CrossRef]
- Kajiyama, H.; Shibata, K.; Suzuki, S.; Ino, K.; Nawa, A.; Kawai, M.; Nagasaka, T.; Kikkawa, F. Fertility-sparing surgery in young women with invasive epithelial ovarian cancer. Eur. J. Surg. Oncol. J. Eur. Soc. Surg. Oncol. Br. Assoc. Surg. Oncol. 2010, 36, 404–408. [Google Scholar] [CrossRef] [PubMed]
- Hu, J.; Zhu, L.R.; Liang, Z.Q.; Meng, Y.G.; Guo, H.Y.; Qu, P.P.; Ma, C.L.; Xu, C.J.; Yuan, B.B. Clinical outcomes of fertility-sparing treatments in young patients with epithelial ovarian carcinoma. J. Zhejiang Univ. Sci. B 2011, 12, 787–795. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajiyama, H.; Shibata, K.; Mizuno, M.; Umezu, T.; Suzuki, S.; Nawa, A.; Kawai, M.; Nagasaka, T.; Kikkawa, F. Long-term survival of young women receiving fertility-sparing surgery for ovarian cancer in comparison with those undergoing radical surgery. Br. J. Cancer 2011, 105, 1288–1294. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Cheng, X.; Cheng, B.; Wan, X.; Lu, W.; Xie, X. Outcomes of conservative surgery in early epithelial ovarian carcinoma. Eur. J. Gynaecol. Oncol. 2012, 33, 93–95. [Google Scholar] [CrossRef] [PubMed]
- Fruscio, R.; Corso, S.; Ceppi, L.; Garavaglia, D.; Garbi, A.; Floriani, I.; Franchi, D.; Cantù, M.G.; Bonazzi, C.M.; Milani, R.; et al. Conservative management of early-stage epithelial ovarian cancer: Results of a large retrospective series. Ann. Oncol. 2013, 24, 138–144. [Google Scholar] [CrossRef] [PubMed]
- Fruscio, R.; Ceppi, L.; Corso, S.; Galli, F.; Dell’Anna, T.; Dell’Orto, F.; Giuliani, D.; Garbi, A.; Chiari, S.; Mangioni, C.; et al. Long-term results of fertility-sparing treatment compared with standard radical surgery for early-stage epithelial ovarian cancer. Br. J. Cancer 2016, 115, 641–648. [Google Scholar] [CrossRef] [PubMed]
- Kashima, K.; Yahata, T.; Fujita, K.; Tanaka, K. Outcomes of fertility-sparing surgery for women of reproductive age with FIGO stage IC epithelial ovarian cancer. Int. J. Gynaecol. Obstet. Off. Organ. Int. Fed. Gynaecol. Obstet. 2013, 121, 53–55. [Google Scholar] [CrossRef]
- Kajiyama, H.; Mizuno, M.; Shibata, K.; Yamamoto, E.; Kawai, M.; Nagasaka, T.; Kikkawa, F. Recurrence-predicting prognostic factors for patients with early-stage epithelial ovarian cancer undergoing fertility-sparing surgery: A multi-institutional study. Eur. J. Obstet. Gynecol. Reprod. Biol. 2014, 175, 97–102. [Google Scholar] [CrossRef]
- Lee, J.-Y.; Jo, Y.R.; Kim, T.H.; Kim, H.S.; Kim, M.A.; Kim, J.W.; Park, N.H.; Song, Y.-S. Safety of fertility-sparing surgery in primary mucinous carcinoma of the ovary. Cancer Res. Treat. 2015, 47, 290–297. [Google Scholar] [CrossRef]
- Ditto, A.; Martinelli, F.; Bogani, G.; Lorusso, D.; Carcangiu, M.; Chiappa, V.; Reato, C.; Donfrancesco, C.; De Carrillo, K.J.A.; Raspagliesi, F. Long-term safety of fertility sparing surgery in early stage ovarian cancer: Comparison to standard radical surgical procedures. Gynecol. Oncol. 2015, 138, 78–82. [Google Scholar] [CrossRef]
- Bentivegna, E.; Gouy, S.; Maulard, A.; Pautier, P.; Leary, A.; Colombo, N.; Morice, P. Fertility-sparing surgery in epithelial ovarian cancer: A systematic review of oncological issues. Ann. Oncol. 2016, 27, 1994–2004. [Google Scholar] [CrossRef]
- Gouy, S.; Saidani, M.; Maulard, A.; Bach-Hamba, S.; Bentivegna, E.; Leary, A.; Pautier, P.; Devouassoux-Shisheboran, M.; Genestie, C.; Morice, P. Results of Fertility-Sparing Surgery for Expansile and Infiltrative Mucinous Ovarian Cancers. Oncologist 2018, 23, 324–327. [Google Scholar] [CrossRef] [Green Version]
- Jiang, X.; Yang, J.; Yu, M.; Xie, W.; Cao, D.; Wu, M.; Pan, L.; Huang, H.; You, Y.; Shen, K. Oncofertility in patients with stage I epithelial ovarian cancer: Fertility-sparing surgery in young women of reproductive age. World J. Surg. Oncol. 2017, 15, 154. [Google Scholar] [CrossRef]
- Melamed, A.; Rizzo, A.E.; Nitecki, R.; Gockley, A.A.; Bregar, A.J.; Schorge, J.O.; Del Carmen, M.G.; Rauh-Hain, J.A. All-Cause Mortality After Fertility-Sparing Surgery for Stage I Epithelial Ovarian Cancer. Obstet. Gynecol. 2017, 130, 71–79. [Google Scholar] [CrossRef] [PubMed]
- Ratanasrithong, P.; Benjapibal, M. Pregnancy Outcomes after Conservative Surgery for Early-Stage Ovarian Neoplasms. Asian Pac. J. Cancer Prev. 2017, 18, 2083–2087. [Google Scholar] [PubMed]
- Hanatani, M.; Yoshikawa, N.; Yoshida, K.; Tamauchi, S.; Ikeda, Y.; Nishino, K.; Niimi, K.; Suzuki, S.; Kawai, M.; Kajiyama, H.; et al. Impact of age on clinicopathological features and survival of epithelial ovarian neoplasms in reproductive age. Int. J. Clin. Oncol. 2020, 25, 187–194. [Google Scholar] [CrossRef] [PubMed]
- Kajiyama, H.; Suzuki, S.; Niimi, K.; Tamauchi, S.; Kawai, M.; Nagasaka, T.; Shibata, K.; Kikkawa, F. Oncologic and reproductive outcomes of cystectomy as a fertility-sparing treatment for early-stage epithelial ovarian cancer. Int. J. Clin. Oncol. 2019, 24, 857–862. [Google Scholar] [CrossRef]
- Bogani, G.; Ditto, A.; Pinelli, C.; Lopez, S.; Chiappa, V.; Raspagliesi, F. Ten-year follow-up study of long-term outcomes after conservative surgery for early-stage ovarian cancer. Int. J. Gynaecol. Obstet. Off. Organ. Int. Fed. Gynaecol. Obstet. 2020, 150, 169–176. [Google Scholar] [CrossRef]
- Liu, D.; Cai, J.; Gao, A.; Wang, Z.; Cai, L. Fertility sparing surgery vs radical surgery for epithelial ovarian cancer: A meta-analysis of overall survival and disease-free survival. BMC Cancer 2020, 20, 320. [Google Scholar] [CrossRef] [Green Version]
- Watanabe, T.; Soeda, S.; Nishiyama, H.; Kiko, Y.; Tokunaga, H.; Shigeta, S.; Yaegashi, N.; Yamada, H.; Ohta, T.; Nagase, S.; et al. Clinical and reproductive outcomes of fertility-sparing surgery in stage I epithelial ovarian cancer. Mol. Clin. Oncol. 2020, 12, 44–50. [Google Scholar] [CrossRef] [Green Version]
- Zhang, Y.; Li, C.; Luo, S.; Su, Y.; Gang, X.; Chu, P.; Zhang, J.; Wu, H.; Liu, G. Retrospective Study of the Epidemiology, Pathology, and Therapeutic Management in Patients with Mucinous Ovarian Tumors. Technol. Cancer. Res. Treat. 2020, 19, 1533033820946423. [Google Scholar] [CrossRef] [PubMed]
- Colombo, N.; Chiari, S.; Maggioni, A.; Bocciolone, L.; Torri, V.; Mangioni, C. Controversial issues in the management of early epithelial ovarian cancer: Conservative surgery and role of adjuvant therapy. Gynecol. Oncol. 1994, 55, S47–S51. [Google Scholar] [CrossRef] [PubMed]
- DiSaia, P.J. Conservative management of the patient with early gynecologic cancer. CA Cancer J. Clin. 1989, 39, 135–154. [Google Scholar] [CrossRef] [PubMed]
- Bentivegna, E.; Fruscio, R.; Roussin, S.; Ceppi, L.; Satoh, T.; Kajiyama, H.; Uzan, C.; Colombo, N.; Gouy, S.; Morice, P. Long-term follow-up of patients with an isolated ovarian recurrence after conservative treatment of epithelial ovarian cancer: Review of the results of an international multicenter study comprising 545 patients. Fertil. Steril. 2015, 104, 1319–1324. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kajiyama, H.; Shibata, K.; Suzuki, S.; Ino, K.; Yamamoto, E.; Mizuno, K.; Sakakibara, K.; Matsuzawa, K.; Takeda, A.; Kinoshita, Y.; et al. Is there any possibility of fertility-sparing surgery in patients with clear-cell carcinoma of the ovary? Gynecol. Oncol. 2008, 111, 523–526. [Google Scholar] [CrossRef]
- Park, J.-Y.; Suh, D.-S.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Nam, J.-H. Outcomes of fertility-sparing surgery among young women with FIGO stage I clear cell carcinoma of the ovary. Int. J. Gynaecol. Obstet. Off. Organ. Int. Fed. Gynaecol. Obstet. 2016, 134, 49–52. [Google Scholar] [CrossRef]
- Petrillo, M.; Legge, F.; Ferrandina, G.; Monterisi, A.; Pedone Anchora, L.; Scambia, G. Fertility-sparing surgery in ovarian cancer extended beyond the ovaries: A case report and review of the literature. Gynecol. Obstet. Investig. 2014, 77, 1–5. [Google Scholar] [CrossRef] [PubMed]
- Peccatori, F.; Bonazzi, C.; Chiari, S.; Landoni, F.; Colombo, N.; Mangioni, C. Surgical management of malignant ovarian germ-cell tumors: 10 years’ experience of 129 patients. Obstet. Gynecol. 1995, 86, 367–372. [Google Scholar] [CrossRef]
- Mitchell, P.L.; Al-Nasiri, N.; A’Hern, R.; Fisher, C.; Horwich, A.; Pinkerton, C.R.; Shepherd, J.H.; Gallagher, C.; Slevin, M.; Harper, P.; et al. Treatment of nondysgerminomatous ovarian germ cell tumors: An analysis of 69 cases. Cancer 1999, 85, 2232–2244. [Google Scholar] [CrossRef]
- Brewer, M.; Gershenson, D.M.; Herzog, C.E.; Mitchell, M.F.; Silva, E.G.; Wharton, J.T. Outcome and reproductive function after chemotherapy for ovarian dysgerminoma. J. Clin. Oncol. 1999, 17, 2670–2675. [Google Scholar] [CrossRef]
- Perrin, L.C.; Low, J.; Nicklin, J.L.; Ward, B.G.; Crandon, A.J. Fertility and ovarian function after conservative surgery for germ cell tumours of the ovary. Aust. N. Z. J. Obstet. Gynaecol. 1999, 39, 243–245. [Google Scholar]
- Tewari, K.; Cappuccini, F.; Disaia, P.J.; Berman, M.L.; Manetta, A.; Kohler, M.F. Malignant germ cell tumors of the ovary. Obstet Gynecol. 2000, 95, 128–133. [Google Scholar]
- Low, J.J.; Perrin, L.C.; Crandon, A.J.; Hacker, N.F. Conservative surgery to preserve ovarian function in patients with malignant ovarian germ cell tumors. A review of 74 cases. Cancer 2000, 89, 391–398. [Google Scholar] [CrossRef]
- Zanetta, G.; Bonazzi, C.; Cantù, M.; Binidagger, S.; Locatelli, A.; Bratina, G.; Mangioni, C. Survival and reproductive function after treatment of malignant germ cell ovarian tumors. J. Clin. Oncol. 2001, 19, 1015–1020. [Google Scholar] [CrossRef]
- Tangir, J.; Zelterman, D.; Ma, W.; Schwartz, P.E. Reproductive function after conservative surgery and chemotherapy for malignant germ cell tumors of the ovary. Obstet. Gynecol. 2003, 101, 251–257. [Google Scholar] [CrossRef] [PubMed]
- Zanagnolo, V.; Sartori, E.; Galleri, G.; Pasinetti, B.; Bianchi, U. Clinical review of 55 cases of malignant ovarian germ cell tumors. Eur. J. Gynaecol. Oncol. 2004, 25, 315–320. [Google Scholar] [PubMed]
- Boran, N.; Tulunay, G.; Caliskan, E.; Köse, M.F.; Haberal, A. Pregnancy outcomes and menstrual function after fertility sparing surgery for pure ovarian dysgerminomas. Arch. Gynecol. Obstet. 2005, 271, 104–108. [Google Scholar] [CrossRef] [PubMed]
- Ayhan, A.; Celik, H.; Taskiran, C.; Bozdag, G.; Aksu, T. Oncologic and reproductive outcome after fertility-saving surgery in ovarian cancer. Eur. J. Gynaecol. Oncol. 2003, 24, 223–232. [Google Scholar] [PubMed]
- Kang, H.; Kim, T.-J.; Kim, W.Y.; Choi, C.H.; Lee, J.-W.; Kim, B.-G.; Bae, D.-S. Outcome and reproductive function after cumulative high-dose combination chemotherapy with bleomycin, etoposide and cisplatin (BEP) for patients with ovarian endodermal sinus tumor. Gynecol. Oncol. 2008, 111, 106–110. [Google Scholar] [CrossRef]
- de La Motte Rouge, T.; Pautier, P.; Duvillard, P.; Rey, A.; Morice, P.; Haie-Meder, C.; Kerbrat, P.; Culine, S.; Troalen, F.; Lhommé, C. Survival and reproductive function of 52 women treated with surgery and bleomycin, etoposide, cisplatin (BEP) chemotherapy for ovarian yolk sac tumor. Ann. Oncol. 2008, 19, 1435–1441. [Google Scholar] [CrossRef] [PubMed]
- Ertas, I.E.; Taskin, S.; Goklu, R.; Bilgin, M.; Goc, G.; Yildirim, Y.; Ortaç, F.; Taşkın, S. Long-term oncological and reproductive outcomes of fertility-sparing cytoreductive surgery in females aged 25 years and younger with malignant ovarian germ cell tumors. J. Obstet. Gynaecol. Res. 2014, 40, 797–805. [Google Scholar] [CrossRef]
- Satoh, T.; Aoki, Y.; Kasamatsu, T.; Ochiai, K.; Takano, M.; Watanabe, Y.; Kikkawa, F.; Takeshima, N.; Hatae, M.; Yokota, H.; et al. Administration of standard-dose BEP regimen (bleomycin+etoposide+cisplatin) is essential for treatment of ovarian yolk sac tumour. Eur. J. Cancer 2015, 51, 340–351. [Google Scholar] [CrossRef]
- Yang, Z.; Liu, Z.; Wei, R.; Li, L. An Analysis of Prognostic Factors in Patients with Ovarian Malignant Germ Cell Tumors Who Are Treated with Fertility-Preserving Surgery. Gynecol. Obstet. Investig. 2016, 81, 1–9. [Google Scholar] [CrossRef]
- Ghalleb, M.; Bouzaiene, H.; Slim, S.; Hadiji, A.; Hechiche, M.; Hassouna, J.B.; Rahal, K. Fertility-sparing surgery in advanced stage malignant ovarian germ cell tumor: A case report. J. Med. Case. Reports 2017, 11, 350. [Google Scholar] [CrossRef] [Green Version]
- Park, J.-Y.; Kim, D.-Y.; Suh, D.-S.; Kim, J.-H.; Kim, Y.-M.; Kim, Y.-T.; Nam, J.-H. Analysis of outcomes and prognostic factors after fertility-sparing surgery in malignant ovarian germ cell tumors. Gynecol. Oncol. 2017, 145, 513–518. [Google Scholar] [CrossRef] [PubMed]
- de Bénazé, G.D.; Pacquement, H.; Faure-Conter, C.; Patte, C.; Orbach, D.; Corradini, N.; Berger, C.; Sudour-Bonnange, H.; Vérité, C.; Martelli, H.; et al. Paediatric dysgerminoma: Results of three consecutive French germ cell tumours clinical studies (TGM-85/90/95) with late effects study. Eur. J. Cancer 2018, 91, 30–37. [Google Scholar] [CrossRef] [PubMed]
- Lakshmanan, M.; Gupta, S.; Kumar, V.; Akhtar, N.; Chaturvedi, A.; Misra, S.; Jain, K.; Garg, S. Germ Cell Tumor Ovary: An Institutional Experience of Treatment and Survival Outcomes. Indian J. Surg. Oncol. 2018, 9, 215–219. [Google Scholar] [CrossRef]
- Tamauchi, S.; Kajiyama, H.; Yoshihara, M.; Ikeda, Y.; Yoshikawa, N.; Nishino, K.; Utsumi, F.; Niimi, K.; Suzuki, S.; Kikkawa, F. Reproductive outcomes of 105 malignant ovarian germ cell tumor survivors: A multicenter study. Am. J. Obstet. Gynecol. 2018, 219, 385.e1–385.e7. [Google Scholar] [CrossRef] [Green Version]
- Dellino, M.; Silvestris, E.; Loizzi, V.; Paradiso, A.; Loiacono, R.; Minoia, C.; Daniele, A.; Cormio, G. Germinal ovarian tumors in reproductive age women: Fertility-sparing and outcome. Medicine 2020, 99, e22146. [Google Scholar] [CrossRef] [PubMed]
- Turkmen, O.; Karalok, A.; Basaran, D.; Kimyon, G.C.; Tasci, T.; Ureyen, I.; Tulunay, G.; Turan, T. Fertility-Sparing Surgery Should Be the Standard Treatment in Patients with Malignant Ovarian Germ Cell Tumors. J. Adolesc. Young Adult Oncol. 2017, 6, 270–276. [Google Scholar] [CrossRef] [PubMed]
- Sahoo, T.K.; Kar, T.; Kar, A.; Panda, S. Poorly Differentiated Sertoli-Leydig Cell Tumour of Ovary with Heterologous Elements. J. Clin. Diagn. Res. 2017, 11, XD01–XD02. [Google Scholar] [CrossRef]
- Gouy, S.; Arfi, A.; Maulard, A.; Pautier, P.; Bentivegna, E.; Leary, A.; Chargari, C.; Genestie, C.; Morice, P. Results from a Monocentric Long-Term Analysis of 23 Patients with Ovarian Sertoli-Leydig Cell Tumors. Oncologist 2019, 24, 702–709. [Google Scholar] [CrossRef] [Green Version]
- Xu, Q.; Zou, Y.; Zhang, X.F. Sertoli-Leydig cell tumors of ovary: A case series. Medicine 2018, 97, e12865. [Google Scholar] [CrossRef] [PubMed]
- Durmuş, Y.; Kılıç, Ç.; Çakır, C.; Yüksel, D.; Boran, N.; Karalök, A.; Boyraz, G.; Turan, A.T. Sertoli-Leydig cell tumor of the ovary: Analysis of a single institution database and review of the literature. J. Obstet. Gynaecol. Res. 2019, 45, 1311–1318. [Google Scholar] [CrossRef]
- Seidler, S.J.; Huber, A.; Nef, J.; Huber, D.E. Sertoli-Leydig Cell Ovarian Tumors: Is Fertility or Endocrine-Sparing Surgery an Option upon Relapse? Case Rep. Oncol. 2020, 13, 935–940. [Google Scholar] [CrossRef]
- Guo, Y.; Wang, J.; Li, Y.; Wang, Y. Ovarian Sertoli-Leydig cell tumors: An analysis of 13 cases. Arch. Gynecol. Obstet. 2020, 302, 203–208. [Google Scholar] [CrossRef]
- Zhang, M.; Cheung, M.K.; Shin, J.Y.; Kapp, D.S.; Husain, A.; Teng, N.N.; Berek, J.S.; Osann, K.; Chan, J.K. Prognostic factors responsible for survival in sex cord stromal tumors of the ovary--an analysis of 376 women. Gynecol. Oncol. 2007, 104, 396–400. [Google Scholar] [CrossRef] [PubMed]
- Iavazzo, C.; Gkegkes, I.D.; Vrachnis, N. Fertility sparing management and pregnancy in patients with granulosa cell tumour of the ovaries. J. Obstet. Gynaecol. 2015, 35, 331–335. [Google Scholar] [CrossRef] [PubMed]
- Rinne, N.; Farthing, A.; Borley, J. Fertility sparing surgery in advanced and recurrent granulosa cell tumours of the ovary. J. Obstet. Gynaecol. 2018, 38, 143–145. [Google Scholar] [CrossRef] [PubMed]
- Wang, D.; Cao, D.; Jia, C.; Huang, H.; Yang, J.; Wu, M.; Pan, L.; Shen, K.; Xiang, Y. Analysis of oncologic and reproductive outcomes after fertility-sparing surgery in apparent stage I adult ovarian granulosa cell tumors. Gynecol. Oncol. 2018, 151, 275–281. [Google Scholar] [CrossRef]
- Bergamini, A.; Cormio, G.; Ferrandina, G.; Lorusso, D.; Giorda, G.; Scarfone, G.; Bocciolone, L.; Raspagliesi, F.; Tateo, S.; Cassani, C.; et al. Conservative surgery in stage I adult type granulosa cells tumors of the ovary: Results from the MITO-9 study. Gynecol. Oncol. 2019, 154, 323–327. [Google Scholar] [CrossRef]
- Makhija, A.; Patel, B.M.; Kenkre, M.A.; Desai, A.D.; Patel, S.M.; Mankad, M.H.; Parekh, C.D. Retrospective Analysis of 32 Cases of Ovarian Granulosa Cell Tumours. J. Obstet. Gynaecol. India 2020, 70, 50–56. [Google Scholar] [CrossRef]
- Colombo, N.; Peiretti, M.; Garbi, A.; Carinelli, S.; Marini, C.; Sessa, C.; ESMO Guidelines Working Group. Non-epithelial ovarian cancer: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up. Ann. Oncol. 2012, 23 (Suppl. 7), vii20–vii26. [Google Scholar] [CrossRef]
- Schneider, D.T.; Orbach, D.; Cecchetto, G.; Stachowicz-Stencel, T.; Brummel, B.; Brecht, I.B.; Bisogno, G.; Ferrari, A.; Reguerre, Y.; Godzinski, J.; et al. Ovarian Sertoli Leydig cell tumours in children and adolescents: An analysis of the European Cooperative Study Group on Pediatric Rare Tumors (EXPeRT). Eur. J. Cancer 2015, 51, 543–550. [Google Scholar] [CrossRef]
- Zhang, H.-Y.; Zhu, J.-E.; Huang, W.; Zhu, J. Clinicopathologic features of ovarian Sertoli-Leydig cell tumors. Int. J. Clin. Exp. Pathol. 2014, 7, 6956–6964. [Google Scholar] [PubMed]
- Young, R.H.; Scully, R.E. Ovarian Sertoli-Leydig cell tumors. A clinicopathological analysis of 207 cases. Am. J. Surg. Pathol. 1985, 9, 543–569. [Google Scholar] [CrossRef] [PubMed]
- Schumer, S.T.; Cannistra, S.A. Granulosa cell tumor of the ovary. J. Clin. Oncol. 2003, 21, 1180–1189. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Fertility-Sparing Surgery (n) | Pregnancy Rate (%) | |
|---|---|---|
| Boran et al. (2005) [16] Early Advanced | 25 25 0 | 40 |
| Fauvet et al. (2005) [17] Early Advanced | 62 62 0 | 32 |
| Park et al. (2009) [18] Early Advanced | 184 181 3 | 73 |
| Kanat-Pektas et al. (2011) [19] | 55 | 52 |
| Koskas et al. (2011) (*) [20] | 31 | 38 |
| Song et al. (2011) [21] Early Advanced | 155 150 5 | 88 |
| Lee et al. (2017) [22] Early Advanced | 108 105 3 | 81 |
| Delle Marchette et al. (2019) [23] Early Advanced | 535 438 97 | 84 |
| Lu et al. (2019) [24] Early Advanced | 21 0 21 | 40 |
| Candotti et al. (2020) [25] Early Advanced | 85 74 11 | 73 |
| Chevrot et al. (2020) [26] Early Advanced | 52 30 22 | 63 |
| Jia et al. (2020) [14] Early Advanced | 79 43 36 | 47 |
| Gouy et al. (2020) [12] Early Advanced | 65 0 65 | 69 |
| Plett et al. (2020) [27] Early Advanced | 95 77 18 | 82.9 |
| Number of Patients n | Histologic Type | Stage IA n | Stage IB n | Stage IC n | Grade 1 n | Grade 2 n | Grade 3 n | Recurrence n (%) | Death n (%) | 5 Year Recurrence Free Survival % | |
|---|---|---|---|---|---|---|---|---|---|---|---|
| Zanetta et al. (1997) [51] | 56 | All types | 32 | 2 | 22 | 35 | 14 | 7 | 5 (8.9) | 3 (5.3) | |
| Schilder et al. (2002) [52] | 52 | All types | 42 | 0 | 10 | 38 | 9 | 5 | 5 (9.6) S 2/10, M 2/25, E 1/10, CC 0/5 | 2 (3.8) | |
| Morice et al. (2005) [53] | 34 | All types | 30 | 0 | 3 | 15 | 15 | 4 | 10 (29.4) S 2/3, M 5/21, E 1/5, CC 1/2 | 4 (11.7) | |
| Borgfeldt et al. (2007) [54] | 11 | All types | 10 | 0 | 1 | 9 | 1 | 1 | 1 (9) | 1 (9) | |
| Park et al.(2008) [55] | 62 | All types | 36 | 2 | 21 | 48 | 5 | 9 | 11 (17.7) S 0/7, M 7/41, E 1/8, CC 2/4 | 6 (9.7) | |
| Anchezar et al. (2009) [56] | 16 | All types | 11 | 0 | 5 | 14 | 1 | 1 | 2 (12.5) | 1 (6.2) | |
| Schlaerth et al. (2009) [57] | 20 | All types | 11 | 0 | 9 | 15 | 5 | 1 | 3 (15) | 3 (15) | |
| Kwon et al. (2009) [58] | 21 | All types | 17 | 0 | 4 | 16 | 3 | 2 | 1 (4.7) | 0 | |
| Wright et al. (2009) * [59] | 432 | All types | 370 | 0 | 62 | 157 | 92 | 37 | NA | 94% | |
| Satoh et al. (2010) [60] | 211 | All types | 126 | 0 | 85 | 160 | 15 | 36 | 18 (8.5) S 3/27, M 6/126, E 4/27, CC 5/30 | 5 (2.4) | |
| Kajiyama et al. (2010) [61] | 60 | All types | 30 | 1 | 29 | 41 | 7 | 12 | 8 (13.3) | 7 (11.7) | |
| Hu et al. (2011) [62] | 94 | All types | 46 | 8 | 28 | 64 | 13 | 1 | 2 (2.4) | NA | |
| Kajiyama et al. (2011) [63] | 40 | Mucinous | 27 | 0 | 14 | NA | NA | NA | NA | NA | 97.5% |
| Cheng et al. (2012) [64] | 17 | All types | 10 | 0 | 6 | 15 | 2 | 0 | 1 (5.9) | 0 | |
| Fruscio et al. (2013, 2016) [65,66] | 240 | All types | 130 | 2 | 105 | 141 | 70 | 29 | 27 (11.2) S 11/62, M 8/99, E 6/60, CC 2/17 | 11 (4.6) | |
| Kashima et al. (2013) [67] | 18 | All types | 0 | 0 | 18 | 14 | 0 | 4 | 5 (27.7) | 4 (22.2) | |
| Kajiyama et al. (2014) [68] | 94 | All types | 43 | 0 | 51 | 59 | 14 | 4 | 14 | 11 | 84.3% |
| Lee et al. (2015) [69] | 35 | Mucinous | 21 | 0 | 13 | 27 | 5 | 1 | 6 (17.1) | 91% | |
| Ditto et al. (2015) [70] | 70 | All types | 46 | 2 | 15 | 36 | 24 | 9 | NA | 98% | |
| Bentivegna et al. * (2016) [71] | 673 | All types | 396 | 46 | 231 | 442 ** | 126 ** | 58 ** | 79/673 (12) S 20/128 (16) M 30/344 (9) E 16/128 (12) CC 10/60 (17) | ||
| Gouy et al. (2017) [72] | 21 | Mucinous | 9 | 0 | 12 | 9 | 5 | 1 | 2 (9,5%) | 0 | 90.5% (median follow: 46 months (r 1–169) |
| Jiang et al. (2017) [73] | 52 | All types | 19 | 33 | 45 | 4 | 1 | 5 (9,6%) | NA | 91% | |
| Melamed et al. (2017) [74] | 825 | All types | 546 | 0 | 279 | 298 | 201 | 111 | 30 (3.6) | ||
| Ratanasrithong et al. (2018) [75] | 28 | All types | 17 | 1 | 5 | 4 (14.3) | 1 (3.6) | ||||
| Hanatani et al. (2019) [76] | All types | 325 | |||||||||
| Kajiyama et al. (2019) [77] | 8 (with cystectomy) | All types | 3 | 0 | 5 | 8 | 0 | 0 | 2 (25) | 1 (12.5) | |
| Bogani et al. (2020) [78] | 34 | All types | 21 | 2 | 9 | 28 | 6 | 7 (20.6) | 2 (5.9) | ||
| Liu et al. *** (2020) [79] | 2223 | All types | |||||||||
| Watanabe et al. (2020) [80] | 29 | All types | 14 | 0 | 15 | 13 | 10 | 3 | 5 (17.2) | 2 (6.9) | 90.9 for IA/IC1 43.8 for IC3 |
| Zhang et al. (2020) [81] | 5 | Mucinous | 5 | 0 | 0 | 0 | 0 | ||||
| Author (Year) | Number of Patients n | Number of Patients Wishing to Conceive n (%) | Number of Pregnant Patients n (%) | Live Births n |
|---|---|---|---|---|
| Schilder et al. (2002) [52] | 52 | 24 (46%) | 17 (71%) | 26 |
| Park et al. (2008) [55] | 62 | 19 (30%) | 15 (79%) | 22 |
| Schlaerth et al. (2009) [57] | 20 | 15 (75%) | 6 (40%) | 9 |
| Kwon et al. (2009) [58] | 21 | 5 (24%) | 5 (100%) | 5 |
| Satoh et al. (2010) [60] | 211 | 84 (40%) | 45 (53%) | 56 |
| Cheng et al. (2012) [64] | 17 | 8 (47%) | 5 (62%) | 6 |
| Fruscio et al. (2013, 2016) [65,66] | 240 | 105 (44%) | 84 (80%) | 91 |
| Kashima et al. (2013) [67] | 18 | 10 (55%) | 5 (50%) | 7 |
| Gouy et al. (2017) [72] | 21 | 21 (100%) | 4 (19%) | 6 |
| Jiang et al. (2017) [73] | 52 | 34 (65%) | 32 (94%) | 28 |
| Ratanasrithong et al. (2018) [75] | 28 | 7 (25%) | 4 (6%) | 4 |
| Kajiyama et al. (2019) [77] | 8 | 7 (88%) | 4 (6%) | 4 |
| Total | 802 | 339/802 (42%) | 226/339 (67%) | 264 |
| Author | N pts | N Conservative | Menstruation Maintained | N Pregnancies | N Conservative II/III/IV |
|---|---|---|---|---|---|
| Peccatori et al. 1995 [88] | 129 | 108 | ? | ? | 37 |
| Mitchell et al. * 1999 [89] | 69 | 50 | 24/26 | 11 | ? |
| Brewer et al. ** 1999 [90] | 26 | 16 | 14 | 5 | ? |
| Perrin et al. 1999 [91] | 45 | 45 | During chemotherapy 50% became amenorrhoeic 96% resumed normal menstrual function on completion | 7 healthy babies in the chemotherapy group | |
| Tewari et al. 2000 [92] | 72 | 46 | ? | ? | 1 ***** |
| Low et al. 2000 [93] | 74 | 74 | 43/45 | 19/20 | 19 |
| Zanetta et al. 2001 [94] | 169 | 138 | 128/130 | 55 in 32 pts | 46 |
| Tangir et al. 2003 [95] | 106 | 64 | 32/40 *** | 38 in 29 pts | 11 (9 pregnancies) |
| Zanagnolo et al. 2004 [96] | 55 | 39 | 26 | 11 | 11 |
| Boran et al. ** 2005 [97] | 23 | 23 | 19/23 *** | 6 in 5 pts | 8 (4 pregnancies) |
| Ayhan et al. * 2005 [98] | 29 | 15 | 10 **** | 3 | ? |
| Kang et al. * 2008 [99] | 20 | 15 | 15 | 2 | ? |
| De la Motte Rouge et al. * 2008 [100] | 52 | 41 | 39/40 | 19 in 12 pts | 4 pregnancies |
| Ertas et al. 2014 [101] | 42 | 31 | 23/27 with chemotherapy | 17 by 21 patients who attempted conception | 13 |
| Satoh et al. * 2015 [102] | 211 | 157 | 109/109 | 29 in 40 pts | ? |
| Yang et al. (2016) [103] | 106 | 59 | 45 | 33 in 31 pts (39 desired a pregnancy) | |
| Ghalleb et al. (2017) [104] | 1 | 1 | 1 | 3 | 1 |
| Park et al. (2017) [105] | 171 | 171 | 106/124 patients (85.5%) had regular menstruation, 12/124 patients (9.7%) had irregular menstruation, and 6/124 patients (4.8%) had premature menopause | 15/20 patients (75%) succeeded in achieving 21 pregnancies, 13/20 of the patients (65%) gave birth to 20 healthy babies. | 46 |
| Ratanasrithong et al. (2018) [75] | 22 | 22 | 4 in 4 patients (8 desired a pregnancy) | ||
| Duhil (2018) et al. ** [106] | 48 | 36 | 13 patients (36%) had 22 pregnancies resulting in 17 healthy born children | ||
| Lakshmanan et al. (2018) [107] | 39 | 14 | 9 | 1 | |
| Tamauchi et al. (2018) [108] | 105 | 105 | 57 (among 72 with chemotherapy, and NA = 13) | 42 patients (45 desired a pregnancy) had 64 pregnancies resulting in 56 healthy born children (among 40 patients) | 31 |
| Dellino et al. (2020) [109] | 28 | 24 | Of 19 women with chemotherapy, 15 (78%) reported regular menstrual cycles during and after chemotherapy; the remaining 4 (21%) presented amenorrhea during chemotherapy but reported regular cycles after the end of treatment. | 5 of 5 women who tried to get pregnant succeeded spontaneously. | 5 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Canlorbe, G.; Chabbert-Buffet, N.; Uzan, C. Fertility-Sparing Surgery for Ovarian Cancer. J. Clin. Med. 2021, 10, 4235. https://doi.org/10.3390/jcm10184235
Canlorbe G, Chabbert-Buffet N, Uzan C. Fertility-Sparing Surgery for Ovarian Cancer. Journal of Clinical Medicine. 2021; 10(18):4235. https://doi.org/10.3390/jcm10184235
Chicago/Turabian StyleCanlorbe, Geoffroy, Nathalie Chabbert-Buffet, and Catherine Uzan. 2021. "Fertility-Sparing Surgery for Ovarian Cancer" Journal of Clinical Medicine 10, no. 18: 4235. https://doi.org/10.3390/jcm10184235
APA StyleCanlorbe, G., Chabbert-Buffet, N., & Uzan, C. (2021). Fertility-Sparing Surgery for Ovarian Cancer. Journal of Clinical Medicine, 10(18), 4235. https://doi.org/10.3390/jcm10184235