
Improved Visibility of Early Gastric Cancer after Successful Helicobacter pylori Eradication with Image-Enhanced Endoscopy: A Multi-Institutional Study Using Video Clips

 , , ,
, , ,  , ,
, ,  ,
,  and add
Show full author list
and add
Show full author list
Abstract
:1. Introduction
2. Materials and Methods
2.1. Participating Institutions
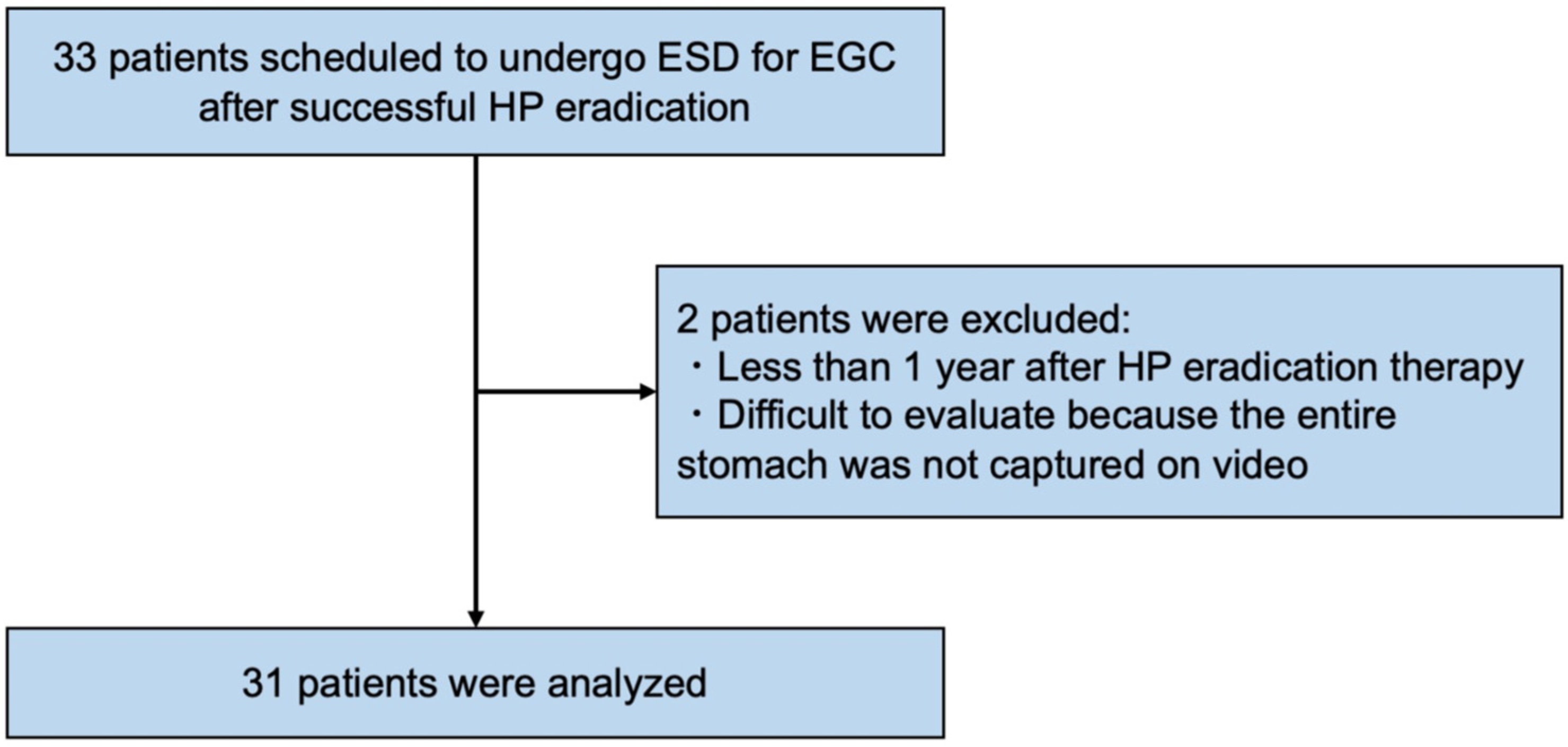
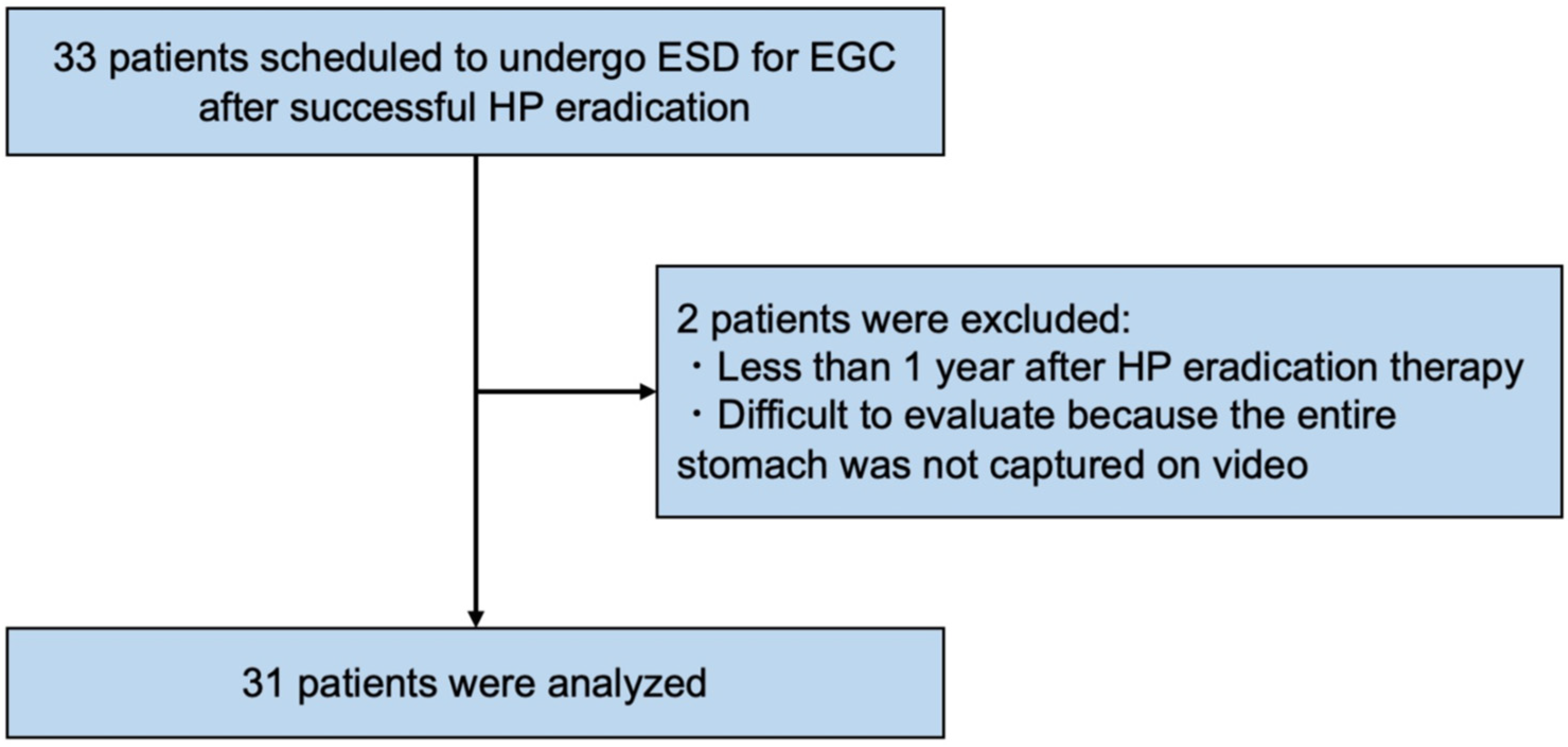
2.2. Patients
2.3. Outcomes
2.4. Endoscopic System, Devices, and Settings for the Movies
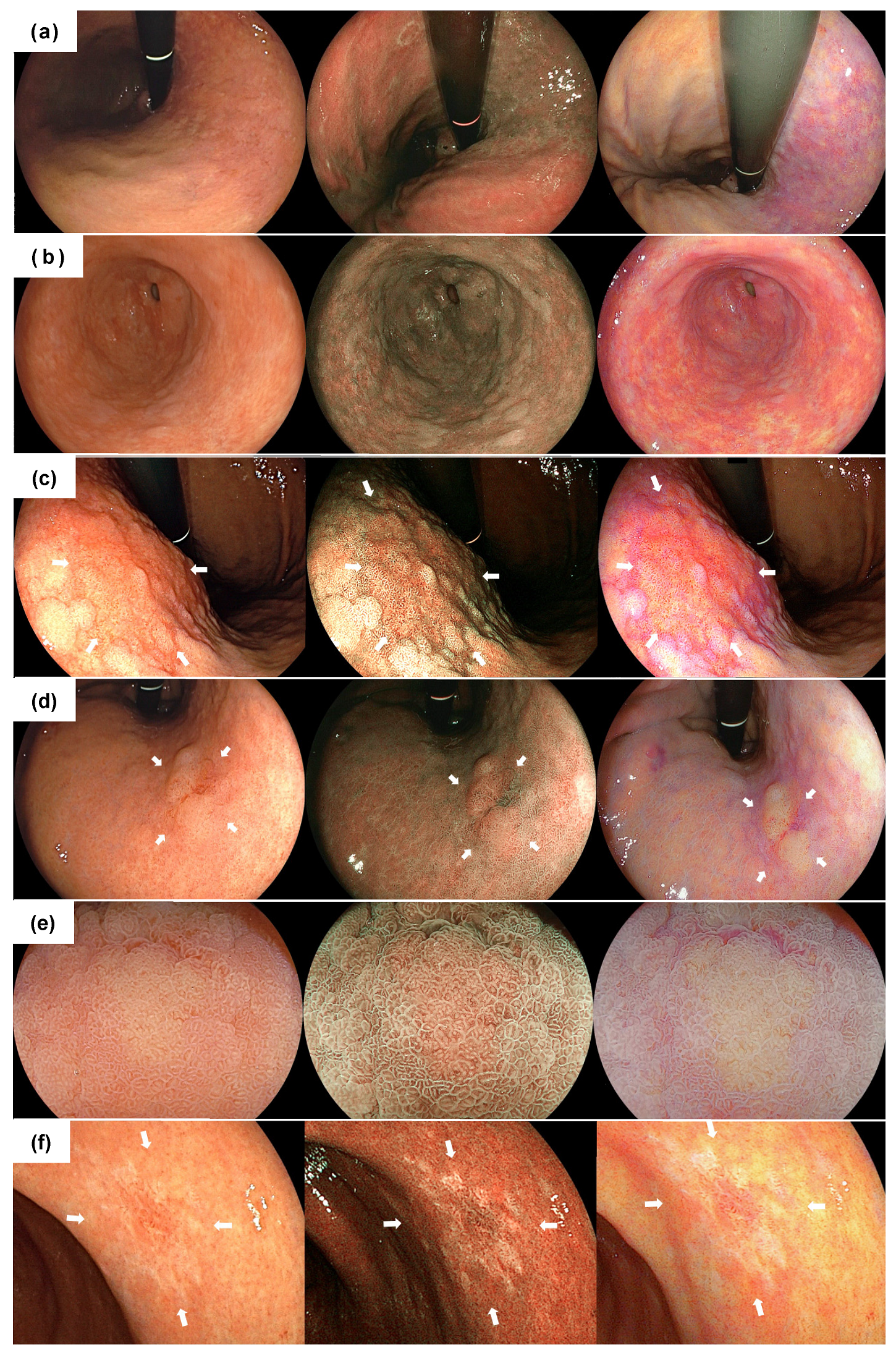
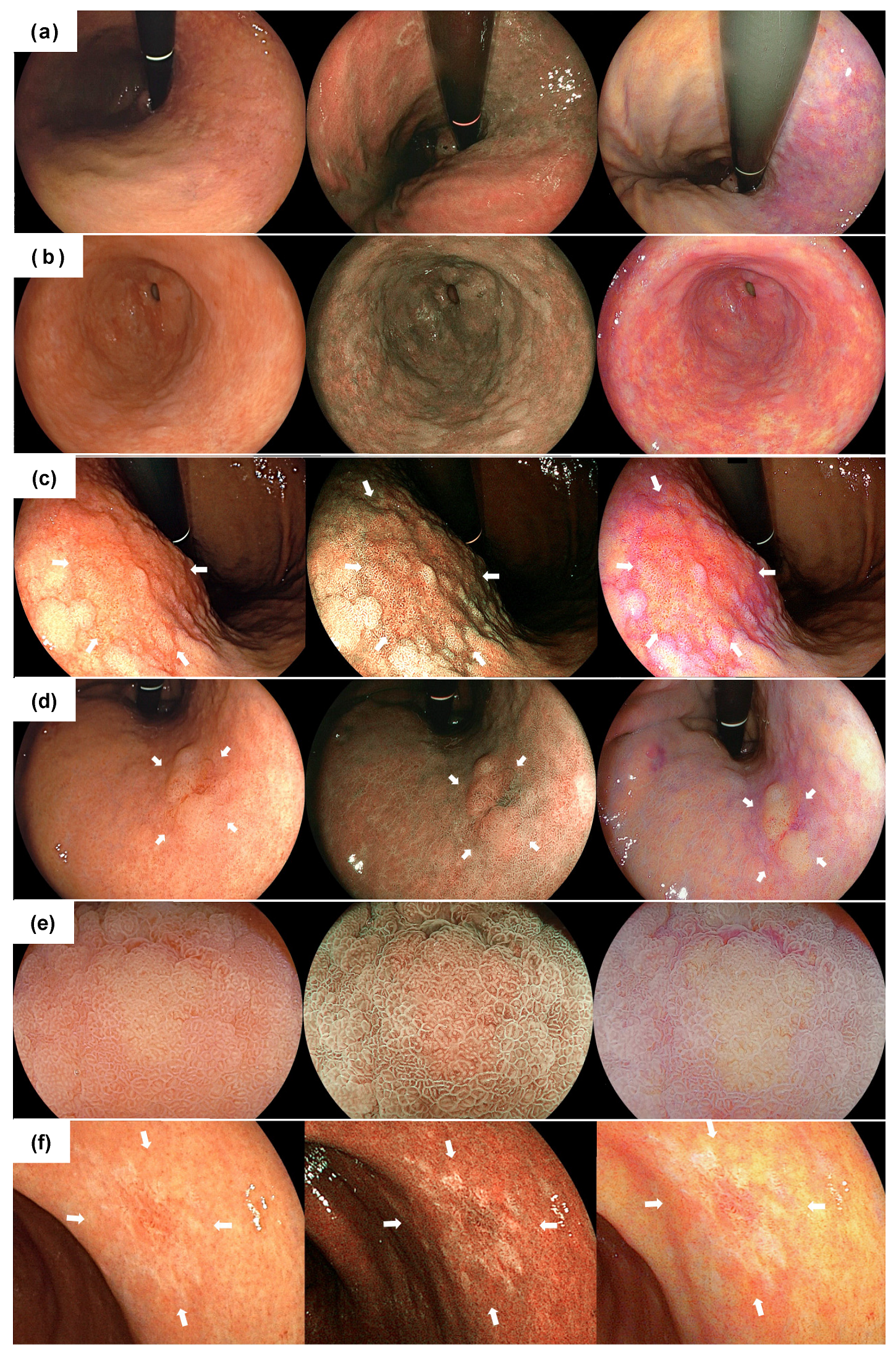
2.5. The Evaluation of Endoscopic Findings
2.6. Definition of Endoscopic Findings
2.7. Diagnostic Criteria of Successful HP Eradication
2.8. Calculation of the Sample Size
2.9. Statistical Analyses
3. Results
3.1. Clinicopathological Features
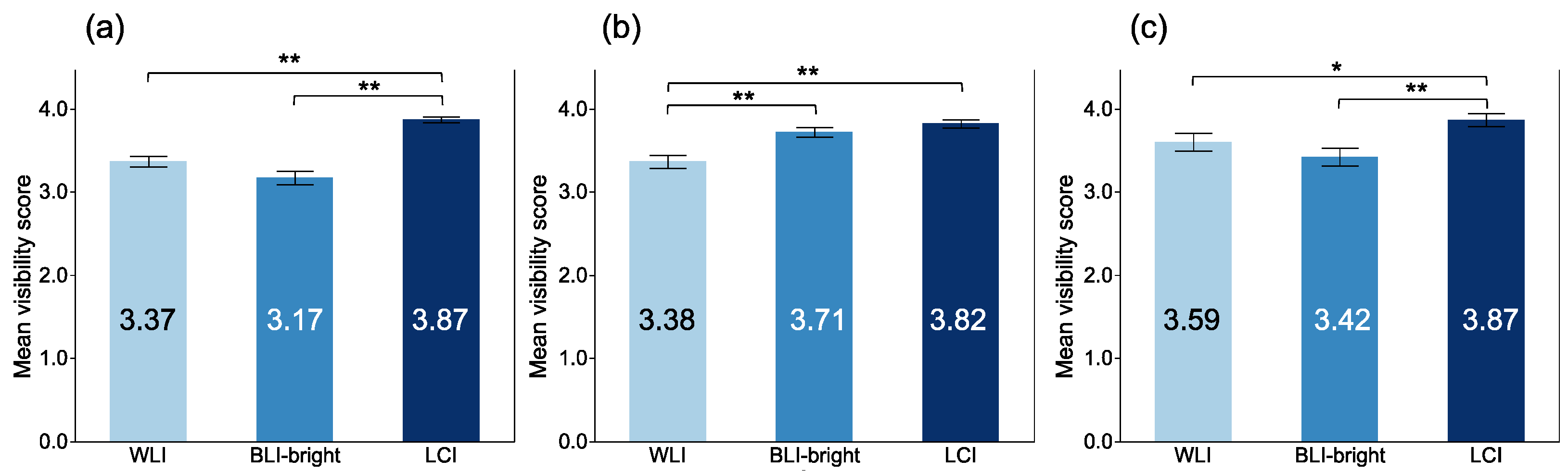
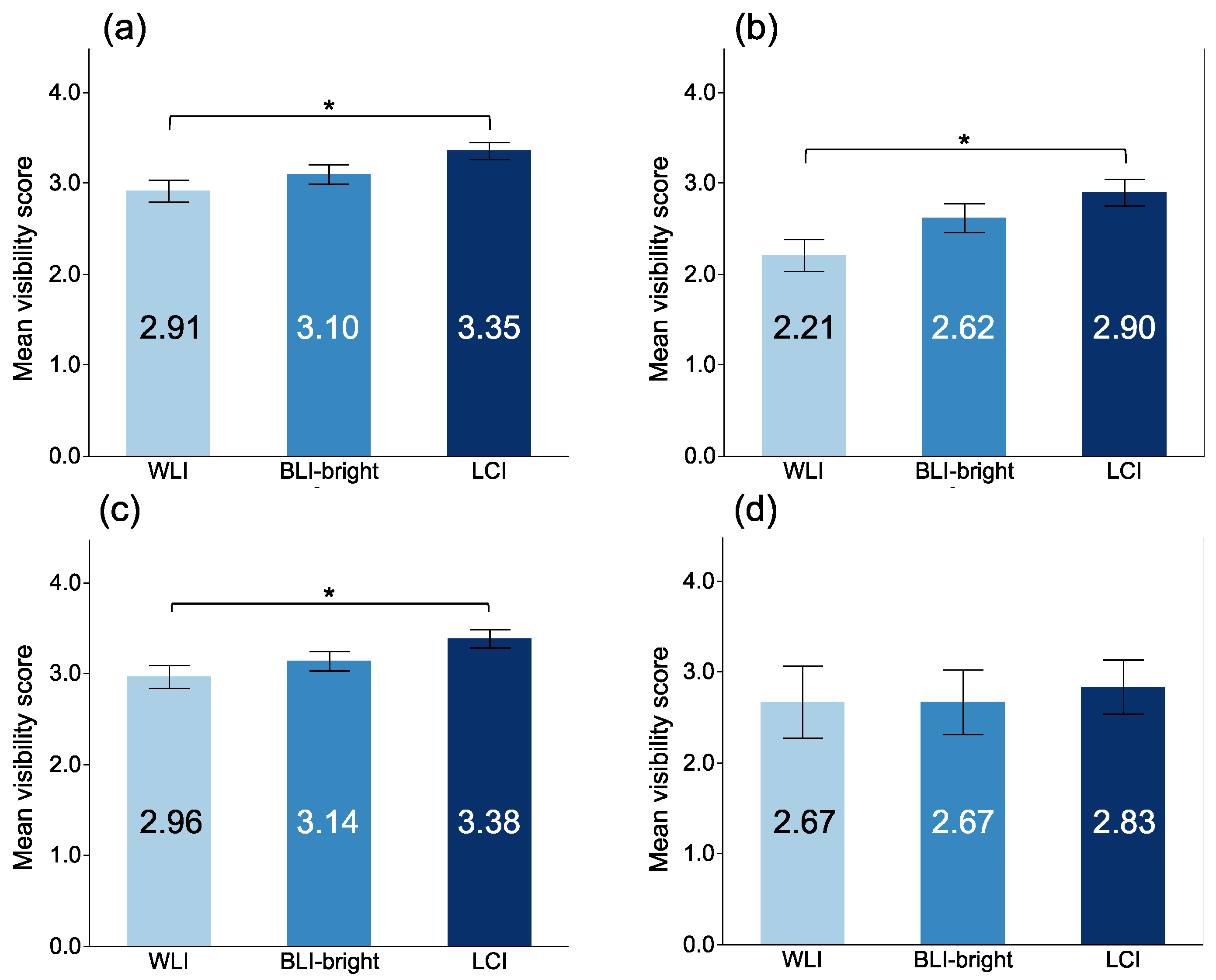
3.2. The Visibility of EGC after Successful HP Eradication
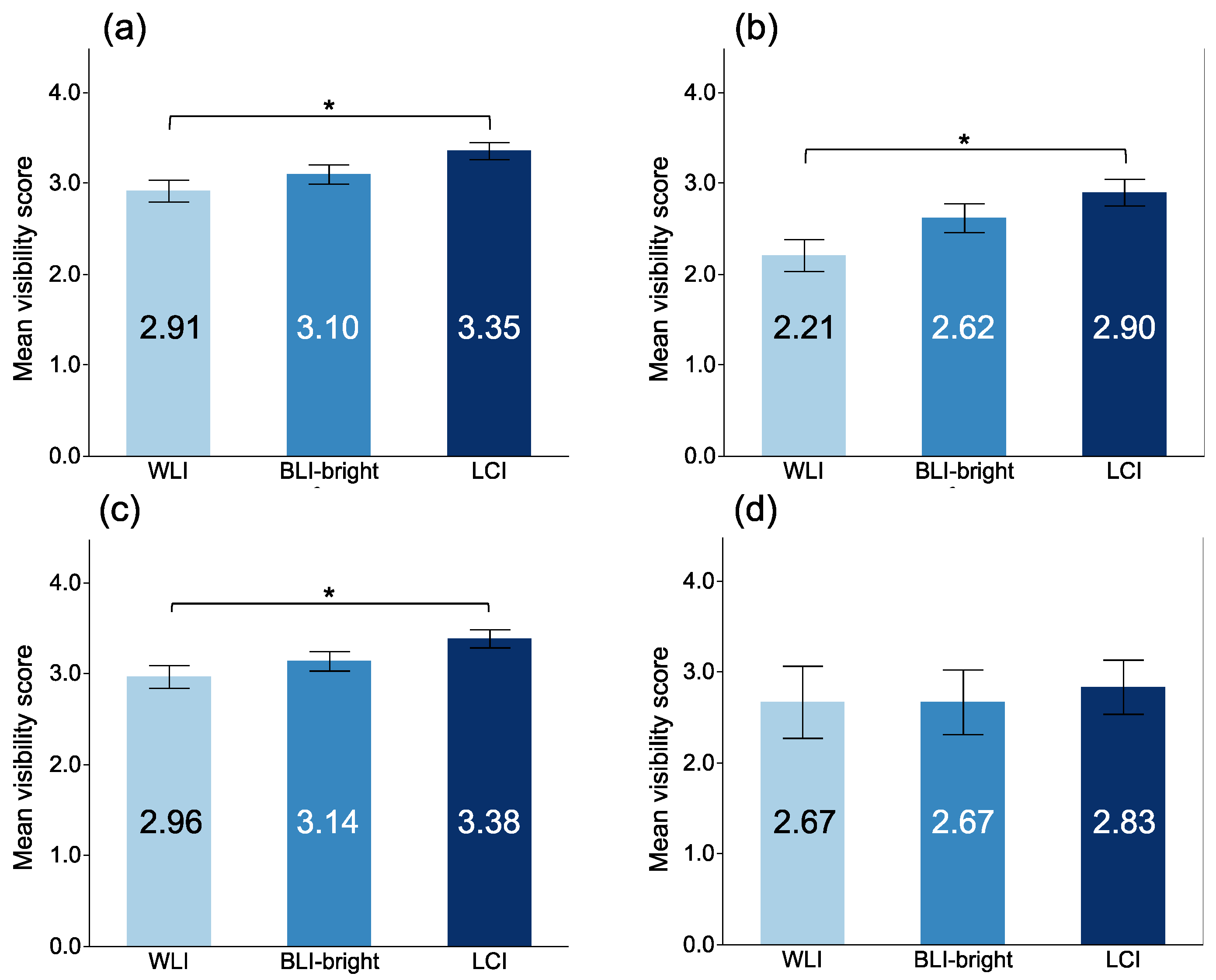
3.3. The Visibility of Gastric Mucosal Findings after Successful HP Eradication
3.4. Relative Evaluation of the Visibility
3.5. Inter-Observer Variability
4. Discussion
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Acknowledgments
Conflicts of Interest
References
- Herrero, R.; Park, J.Y.; Forman, D. The fight against gastric cancer—The IARC Working Group report. Best Pract. Res. Clin. Gastroenterol. 2014, 28, 1107–1114. [Google Scholar] [CrossRef] [PubMed]
- Asaka, M.; Kato, M.; Sakamoto, N. Roadmap to eliminate gastric cancer with Helicobacter pylori eradication and consecutive surveillance in Japan. J. Gastroenterol. 2014, 49, 1–8. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Majima, A.; Handa, O.; Naito, Y.; Dohi, O.; Okayama, T.; Yoshida, N. Early-Stage Gastric Cancer Can Be Found in Improved Atrophic Mucosa over Time from Successful Helicobacter pylori Eradication. Digestion 2017, 95, 194–200. [Google Scholar] [CrossRef] [PubMed]
- Kamada, T.; Hata, J.; Sugiu, K.; Kusunoki, H.; Ito, M.; Tanaka, S.; Inoue, K.; Kawamura, Y.; Chayama, K.; Haruma, K. Clinical features of gastric cancer discovered after successful eradication of Helicobacter pylori: Results from a 9-year prospective follow-up study in Japan. Aliment. Pharm. Ther. 2005, 21, 1121–1126. [Google Scholar] [CrossRef]
- Take, S.; Mizuno, M.; Ishiki, K.; Yoshida, T.; Ohara, N.; Yokota, K.; Oguma, K.; Okada, H.; Yamamoto, K. The long-term risk of gastric cancer after the successful eradication of Helicobacter pylori. J. Gastroenterol. 2011, 46, 318–324. [Google Scholar] [CrossRef]
- Saka, A.; Yagi, K.; Nimura, S. Endoscopic and histological features of gastric cancers after successful Helicobacter pylori eradication therapy. Gastric. Cancer 2016, 19, 524–530. [Google Scholar] [CrossRef]
- Dohi, O.; Yagi, N.; Majima, A.; Horii, Y.; Kitaichi, T.; Onozawa, Y.; Suzuki, K.; Tomie, A.; Kimura-Tsuchiya, R.; Tsuji, T.; et al. Diagnostic ability of magnifying endoscopy with blue laser imaging for early gastric cancer: A prospective study. Gastric Cancer 2017, 20, 297–303. [Google Scholar] [CrossRef]
- Yoshifuku, Y.; Sanomura, Y.; Oka, S.; Kuroki, K.; Kurihara, M.; Mizumoto, T.; Urabe, Y.; Hiyama, T.; Tanaka, S.; Chayama, K. Clinical Usefulness of the VS Classification System Using Magnifying Endoscopy with Blue Laser Imaging for Early Gastric Cancer. Gastroenterol. Res. Pract. 2017, 2017, 3649705. [Google Scholar] [CrossRef] [PubMed]
- Dohi, O.; Yagi, N.; Naito, Y.; Fukui, A.; Gen, Y.; Iwai, N.; Ueda, T.; Yoshida, N.; Kamada, K.; Uchiyam, K.; et al. Blue laser imaging-bright improves the real-time detection rate of early gastric cancer: A randomized controlled study. Gastrointest Endosc. 2019, 89, 47–57. [Google Scholar] [CrossRef]
- Kanzaki, H.; Takenaka, R.; Kawahara, Y.; Kawai, D.; Obayashi, Y.; Baba, Y.; Sakae, H.; Gotoda, T.; Kono, Y.; Miura, K.; et al. Linked color imaging (LCI), a novel image-enhanced endoscopy technology, emphasizes the color of early gastric cancer. Endosc. Int. Open. 2017, 5, E1005–E1013. [Google Scholar] [CrossRef] [Green Version]
- Yoshifuku, Y.; Sanomura, Y.; Oka, S.; Kurihara, M.; Mizumoto, T.; Miwata, T.; Urabe, Y.; Hiyama, T.; Tanaka, S.; Chayama, K. Evaluation of the visibility of early gastric cancer using linked color imaging and blue laser imaging. BMC Gastroenterol. 2017, 17, 150. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Kitagawa, Y.; Suzuki, T.; Nankinzan, R.; Ishigaki, A.; Furukawa, K.; Sugita, O.; Hara, T.; Yamaguchi, T. Comparison of endoscopic visibility and miss rate for early gastric cancers after Helicobacter pylori eradication with white-light imaging versus linked color imaging. Dig. Endosc. 2019, 32, 769–777. [Google Scholar] [CrossRef] [PubMed]
- Ono, S.; Kawada, K.; Dohi, O.; Kitamura, S.; Koike, T.; Hori, S.; Kanzaki, H.; Murao, T.; Yagi, N.; Sasaki, F.; et al. Linked Color Imaging Focused on Neoplasm Detection in the Upper Gastrointestinal Tract: A Randomized Trial. Ann. Intern. Med. 2021, 174, 18–24. [Google Scholar] [CrossRef] [PubMed]
- Dohi, O.; Yagi, N.; Onozawa, Y.; Kimura-Tsuchiya, R.; Majima, A.; Kitaichi, T.; Hori, Y.; Suzuki, K.; Tomie, A.; Okayama, T.; et al. Linked color imaging improves endoscopic diagnosis of active Helicobacter pylori infection. Endosc. Int. Open 2016, 4, E800–E805. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Ono, S.; Kato, M.; Tsuda, M.; Miyamoto, S.; Abiko, S.; Shimizu, Y.; Sakamoto, N. Lavender Color in Linked Color Imaging Enables Noninvasive Detection of Gastric Intestinal Metaplasia. Digestion 2018, 98, 222–230. [Google Scholar] [CrossRef] [PubMed]
- Mizukami, K.; Ogawa, R.; Okamoto, K.; Shuto, M.; Fukuda, K.; Sonoda, A.; Matsunari, O.; Hirashita, Y.; Okimoto, T.; Kodama, M.; et al. Objective Endoscopic Analysis with Linked Color Imaging regarding Gastric Mucosal Atrophy: A Pilot Study. Gastroenterol. Res. Pract. 2017, 2017, 5054237. [Google Scholar] [CrossRef] [PubMed]
- Shichijo, S.; Hirata, Y. Characteristics and predictors of gastric cancer after Helicobacter pylori eradication. World J. Gastroenterol. 2018, 24, 2163–2172. [Google Scholar] [CrossRef] [PubMed]
- Majima, A.; Dohi, O.; Takayama, S.; Hirose, R.; Inoue, K.; Yoshida, N.; Kamada, K.; Uchiyama, K.; Ishikawa, T.; Takagi, T.; et al. Linked color imaging identifies important risk factors associated with gastric cancer after successful eradication of Helicobacter pylori. Gastrointest Endosc. 2019, 90, 763–769. [Google Scholar] [CrossRef]
- Dohi, O.; Majima, A.; Naito, Y.; Yoshida, T.; Ishida, T.; Azuma, Y.; Kitae, H.; Matsumura, S.; Mizuno, N.; Yoshida, N.; et al. Can image-enhanced endoscopy improve the diagnosis of Kyoto classification of gastritis in the clinical setting? Dig. Endosc. 2020, 32, 191–203. [Google Scholar] [CrossRef] [Green Version]
- Yoshida, N.; Naito, Y.; Murakami, T.; Hirose, R.; Ogiso, K.; Inada, Y.; Dohi, O.; Kamada, K.; Uchiyama, K.; Handa, O.; et al. Linked color imaging improves the visibility of colorectal polyps: A video study. Endosc. Int. Open 2017, 05, E518–E525. [Google Scholar] [CrossRef] [Green Version]
- Sugano, K.; Tack, J.; Kuipers, E.J.; Graham, D.Y.; El-Omar, E.M.; Miura, S.; Haruma, K.; Asaka, M.; Uemura, N.; Malfertheiner, P.; et al. Kyoto global consensus report on Helicobacter pylori gastritis. Gut 2015, 64, 1353–1367. [Google Scholar] [CrossRef] [Green Version]
- Dohi, O.; Iwai, N.; Ueda, T.; Majima, A.; Horii, Y.; Kitaichi, T.; Onozawa, Y.; Okayama, T.; Yoshida, N.; Kamada, K.; et al. What is the Best Choice of Image-Enhanded Laser Endoscopy for Early Gastric Cancer? Gastrointest Endosc. 2016, 83 (Suppl. S5), AB458. [Google Scholar] [CrossRef]
- Nahathai, W.; Tinakon, W.; Danny, W.; Gwet, K.L. A comparison of Cohen’s Kappa and Gwet’s AC1when calculating inter-rater reliability coefficients: A study conducted with personality disorder samples. BMC Med. Res. Methodol. 2013, 13, 61. [Google Scholar]
- Yoshida, N.; Naito, Y.; Yasuda, R.; Murakami, T.; Hirose, R.; Ogiso, K.; Inada, Y.; Dohi, O.; Kamada, K.; Uchiyama, K.; et al. Linked color imaging improves the visibility of various featured colorectal polyps in an endoscopist’s visibility and color difference value. Int. J. Colorectal. Dis. 2017, 32, 1253–1260. [Google Scholar] [CrossRef]
- Kobayashi, M.; Hashimoto, S.; Nishikura, K.; Mizuno, K.; Takeuchi, M.; Sato, Y.; Ajioka, Y.; Aoyagi, Y. Magnifying narrow-band imaging of surface maturation in early differentiated-type gastric cancers after Helicobacter pylori eradication. J. Gastroenterol. 2013, 48, 1332–1342. [Google Scholar] [CrossRef]
- Dohi, O.; Ishida, T.; Yoshida, N. Linked color imaging followed by magnifying blue laser imaging identifies early gastric cancer in map-like redness after successful Helicobacter pylori eradication. Dig. Endosc. 2020, 32, e109–e110. [Google Scholar] [CrossRef]


{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
| n = 31 | |
|---|---|
| Age, years, median (range) | 72.1 (61–85) |
| Sex, n (%) | |
| Male | 17 (54.8) |
| Female | 14 (45.2) |
| Time since H pylori eradication, y | 5.58 |
| Atrophic border, n (%) | data |
| C-1·C-2 | 1 (3.2) |
| C-3·O-1 | 1 (3.2) |
| O-2·O-3 | 29 (93.5) |
| Intestinal metaplasia, n (%) | |
| − | 16 (51.6) |
| + | 15 (48.4) |
| Location, n (%) | |
| U | 1 (3.2) |
| M | 20 (64.5) |
| L | 10 (32.3) |
| Macroscopic type, n (%) | |
| 0-IIa | 14 (45.2) |
| 0-IIb | 2 (6.5) |
| 0-IIc | 15 (48.4) |
| Mean tumor size, mm (range) | 21.2 (10–50) |
| Color, n (%) | |
| Normal | 2 (6.5) |
| Reddish | 22 (71.0) |
| Discolored | 7 (22.6) |
| Histological type, n (%) | |
| Differentiated | 27 (87.1) |
| Undifferentiated | 4 (12.9) |
| Relative Visibility, n (%) | p-Value | |||
|---|---|---|---|---|
| BLI-Bright/BLI | LCI | |||
| Atrophic border | Improved | 9 (9.7) | 42 (45.2) | <0.001 |
| Unchanged | 58 (62.4) | 51 (53.8) | ||
| Worsened | 26 (28.0) | 0 | ||
| Intestinal metaplasia | Improved | 31 (33.3) | 35 (37.6) | <0.001 |
| Unchanged | 58 (62.4) | 57 (61.3) | ||
| Worsened | 4 (4.3) | 1 (1.1) | ||
| Map-like redness | Improved | 11 (11.8) | 23 (24.7) | <0.001 |
| Unchanged | 64 (68.8) | 70 (75.3) | ||
| Worsened | 18 (19.4) | 0 | ||
| Recognition of EGC | Improved | 21 (22.6) | 34 (36.6) | <0.001 |
| Unchanged | 62 (66.7) | 58 (62.4) | ||
| Worsened | 10 (10.8) | 1 (1.1) | ||
| Microsurface | Improved | 86 (92.5) | 66 (71.0) | <0.001 |
| Unchanged | 7 (7.5) | 25 (26.9) | ||
| Worsened | 0 | 2 (2.2) | ||
| Microvascular | Improved | 90 (98.9) | 76 (81.7) | <0.001 |
| Unchanged | 3 (3.2) | 16 (17.2) | ||
| Worsened | 0 | 1 (1.1) | ||
| Demarcation line | Improved | 85 (91.4) | 85 (91.4) | <0.001 |
| Unchanged | 8 (8.6) | 8 (8.6) | ||
| Worsened | 0 | 0 | ||
| Inter-Observer Variability, Mean (Range) | |
|---|---|
| Atrophic border | |
| WLI | 0.78 (0.67–0.86) |
| BLI-bright | 0.62 (0.50–0.79) |
| LCI | 0.97 (0.96–0.98) |
| Intestinal metaplasia | |
| WLI | 0.61 (0.35–0.91) |
| BLI-bright | 0.88 (0.87–0.90) |
| LCI | 0.94 (0.92–0.96) |
| Map-like redness | |
| WLI | 0.73 (0.60–0.93) |
| BLI-bright | 0.75 (0.67–0.84) |
| LCI | 0.93 (0.88–0.97) |
| Recognition of EGC | |
| WLI | 0.74 (0.72–0.76) |
| BLI-bright | 0.69 (0.62–0.74) |
| LCI | 0.85 (0.84–0.86) |
| Microsurface | |
| WLI | 0.78 (0.75–0.82) |
| BLI | 0.99 (0.98–0.99) |
| LCI | 0.84 (0.78–0.93) |
| Microvascular | |
| WLI | 0.70 (0.53–0.84) |
| BLI | 0.97 (0.95–1.00) |
| LCI | 0.79 (0.72–0.89) |
| Demarcation line | |
| WLI | 0.78 (0.68–0.84) |
| BLI | 0.93 (0.89–0.96) |
| LCI | 0.88 (0.84–0.97) |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matsumura, S.; Dohi, O.; Yamada, N.; Harusato, A.; Yasuda, T.; Yoshida, T.; Ishida, T.; Azuma, Y.; Kitae, H.; Doi, T.; et al. Improved Visibility of Early Gastric Cancer after Successful Helicobacter pylori Eradication with Image-Enhanced Endoscopy: A Multi-Institutional Study Using Video Clips. J. Clin. Med. 2021, 10, 3649. https://doi.org/10.3390/jcm10163649
Matsumura S, Dohi O, Yamada N, Harusato A, Yasuda T, Yoshida T, Ishida T, Azuma Y, Kitae H, Doi T, et al. Improved Visibility of Early Gastric Cancer after Successful Helicobacter pylori Eradication with Image-Enhanced Endoscopy: A Multi-Institutional Study Using Video Clips. Journal of Clinical Medicine. 2021; 10(16):3649. https://doi.org/10.3390/jcm10163649
Chicago/Turabian StyleMatsumura, Shinya, Osamu Dohi, Nobuhisa Yamada, Akihito Harusato, Takeshi Yasuda, Takuma Yoshida, Tsugitaka Ishida, Yuka Azuma, Hiroaki Kitae, Toshifumi Doi, and et al. 2021. "Improved Visibility of Early Gastric Cancer after Successful Helicobacter pylori Eradication with Image-Enhanced Endoscopy: A Multi-Institutional Study Using Video Clips" Journal of Clinical Medicine 10, no. 16: 3649. https://doi.org/10.3390/jcm10163649
APA StyleMatsumura, S., Dohi, O., Yamada, N., Harusato, A., Yasuda, T., Yoshida, T., Ishida, T., Azuma, Y., Kitae, H., Doi, T., Hirose, R., Inoue, K., Yoshida, N., Kamada, K., Uchiyama, K., Takagi, T., Ishikawa, T., Konishi, H., Morinaga, Y., ... Itoh, Y. (2021). Improved Visibility of Early Gastric Cancer after Successful Helicobacter pylori Eradication with Image-Enhanced Endoscopy: A Multi-Institutional Study Using Video Clips. Journal of Clinical Medicine, 10(16), 3649. https://doi.org/10.3390/jcm10163649