
Association between Objectively Measured Physical Activity and Arterial Stiffness in Children with Congenital Heart Disease

 ,
,
Abstract
:1. Introduction
2. Materials and Methods
2.1. Study Participants
2.2. Assessment of Arterial Stiffness
2.3. Objective Assessment of Physical Activity
2.4. Data Analysis
3. Results
4. Discussion
Limitation
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Conflicts of Interest
References
- Bigras, J.-L. Cardiovascular Risk Factors in Patients with Congenital Heart Disease. Can. J. Cardiol. 2020, 36, 1458–1466. [Google Scholar] [CrossRef]
- Laurent, S.; Cockcroft, J.; Van Bortel, L.; Boutouyrie, P.; Giannattasio, C.; Hayoz, D.; Pannier, B.; Vlachopoulos, C.; Wilkinson, I.; Struijker-Boudier, H.; et al. Expert consensus document on arterial stiffness: Methodological issues and clinical applications. Eur. Heart J. 2006, 27, 2588–2605. [Google Scholar] [CrossRef] [Green Version]
- Laurent, S.; Boutouyrie, P.; Asmar, R.; Gautier, I.; Laloux, B.; Guize, L.; Ducimetiere, P.; Benetos, A. Aortic Stiffness Is an Independent Predictor of All-Cause and Cardiovascular Mortality in Hypertensive Patients. Hypertension 2001, 37, 1236–1241. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- McEniery, C.M.; Yasmin; McDonnell, B.; Munnery, M.; Wallace, S.M.; Rowe, C.V.; Cockcroft, J.R.; Wilkinson, I.B. Central pressure: Variability and impact of cardiovascular risk factors: The Anglo-Cardiff Collaborative Trial II. Hypertension 2008, 51, 1476–1482. [Google Scholar] [CrossRef] [Green Version]
- Sharman, J.E.; Marwick, T.H.; Gilroy, D.; Otahal, P.; Abhayaratna, W.P.; Stowasser, M. Randomized trial of guiding hypertension management using central aortic blood pressure compared with best-practice care: Principal findings of the BP GUIDE study. Hypertension 2013, 62, 1138–1145. [Google Scholar] [CrossRef] [PubMed]
- Häcker, A.-L.; Reiner, B.; Oberhoffer, R.; Hager, A.; Ewert, P.; Müller, J. Increased arterial stiffness in children with congenital heart disease. Eur. J. Prev. Cardiol. 2018, 25, 103–109. [Google Scholar] [CrossRef] [PubMed]
- Müller, J.; Ewert, P.; Hager, A. Increased aortic blood pressure augmentation in patients with congenital heart defects—A cross-sectional study in 1125 patients and 322 controls. Int. J. Cardiol. 2015, 184, 225–229. [Google Scholar] [CrossRef]
- Longmuir, P.E.; Brothers, J.A.; De Ferranti, S.D.; Hayman, L.L.; Van Hare, G.F.; Matherne, G.P.; Davis, C.K.; Joy, E.A.; McCrindle, B.W. Promotion of physical activity for children and adults with congenital heart disease: A scientific statement from the American Heart Association. Circulation 2013, 127, 2147–2159. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Takken, T.; Giardini, A.; Reybrouck, T.; Gewillig, M.; Hövels-Gürich, H.; Longmuir, P.; McCrindle, B.; Paridon, S.; Hager, A. Recommendations for physical activity, recreation sport, and exercise training in paediatric patients with congenital heart disease: A report from the Exercise, Basic & Translational Research Section of the European Association of Cardiovascular Prevention and Rehabilitation, the European Congenital Heart and Lung Exercise Group, and the Association for European Paediatric Cardiology. Eur. J. Prev. Cardiol. 2012, 19, 1034–1065. [Google Scholar] [CrossRef]
- Brudy, L.; Hock, J.; Häcker, A.-L.; Meyer, M.; Oberhoffer, R.; Hager, A.; Ewert, P.; Müller, J. Children with Congenital Heart Disease Are Active but Need to Keep Moving: A Cross-Sectional Study Using Wrist-Worn Physical Activity Trackers. J. Pediatr. 2020, 217, 13–19. [Google Scholar] [CrossRef] [Green Version]
- Moola, F.; McCrindle, B.W.; Longmuir, P.E. Physical activity participation in youth with surgically corrected congenital heart disease: Devising guidelines so Johnny can participate. Paediatr. Child Health 2009, 14, 167–170. [Google Scholar] [CrossRef] [Green Version]
- Siaplaouras, J.; Niessner, C.; Helm, P.C.; Jahn, A.; Flemming, M.; Urschitz, M.S.; Sticker, E.; Abdul-Khaliq, H.; Bauer, U.M.; Apitz, C. Physical Activity Among Children with Congenital Heart Defects in Germany: A Nationwide Survey. Front. Pediatr. 2020, 8. [Google Scholar] [CrossRef]
- Ewalt, L.A.; Danduran, M.J.; Strath, S.J.; Moerchen, V.; Swartz, A.M. Objectively assessed physical activity and sedentary behaviour does not differ between children and adolescents with and without a congenital heart defect: A pilot examination. Cardiol. Young 2011, 22, 34–41. [Google Scholar] [CrossRef]
- Böhm, B.; Oberhoffer, R. Vascular health determinants in children. Cardiovasc. Diagn. Ther. 2019, 9, S269–S280. [Google Scholar] [CrossRef] [PubMed]
- Schack-Nielsen, L.; Mølgaard, C.; Larsen, D.; Martyn, C.; Michaelsen, K.F. Arterial stiffness in 10-year-old children: Current and early determinants. Br. J. Nutr. 2005, 94, 1004–1011. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sakuragi, S.; Abhayaratna, K.; Gravenmaker, K.J.; O’Reilly, C.; Srikusalanukul, W.; Budge, M.M.; Telford, R.D.; Abhayaratna, W.P. Influence of adiposity and physical activity on arterial stiffness in healthy children: The lifestyle of our kids study. Hypertension 2009, 53, 611–616. [Google Scholar] [CrossRef] [Green Version]
- Heil, L.; Oberhoffer, R.; Böhm, B. Association Between Physical Activity Intensity Levels and Arterial Stiffness in Healthy Children. J. Phys. Act. Health 2020, 17, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Khadilkar, A.V.; Chiplonkar, S.A.; Khadilkar, V.V.; Kinare, A.S.; Pandit, D.S. Arterial stiffness in obese children: Role of adiposity and physical activity. Indian J. Endocrinol. Metab. 2014, 18, 70–76. [Google Scholar] [CrossRef]
- Baumgartner, L.; Weberruß, H.; Oberhoffer-Fritz, R.; Schulz, T. Vascular Structure and Function in Children and Adolescents: What Impact Do Physical Activity, Health-Related Physical Fitness, and Exercise Have? Front. Pediatr. 2020, 8, 103. [Google Scholar] [CrossRef] [PubMed]
- Boyes, N.G.; Stickland, M.K.; Fusnik, S.; Hogeweide, E.; Fries, J.T.; Haykowsky, M.J.; Baril, C.L.; Runalls, S.; Kakadekar, A.; Pharis, S.; et al. Physical activity modulates arterial stiffness in children with congenital heart disease: A CHAMPS cohort study. Congenit. Heart Dis. 2018, 13, 578–583. [Google Scholar] [CrossRef]
- Lopez, J.R.; Voss, C.; Kuan, M.T.; Hemphill, N.M.; Sandor, G.G.; Harris, K.C. Physical activity is associated with better vascular function in children and adolescents with congenital heart disease. Can. J. Cardiol. 2020, 36, 1474–1481. [Google Scholar] [CrossRef]
- Hock, J.; Häcker, A.-L.; Reiner, B.; Oberhoffer, R.; Hager, A.; Ewert, P.; Müller, J. Functional outcome in contemporary children and young adults with tetralogy of Fallot after repair. Arch. Dis. Child. 2018, 104, 129–133. [Google Scholar] [CrossRef] [PubMed]
- Häcker, A.-L.; Reiner, B.; Oberhoffer, R.; Hager, A.; Ewert, P.; Müller, J. Functional outcomes in children with anatomically repaired transposition of the great arteries with regard to congenital ventricular septal defect and coronary pattern. Arch. Dis. Child. 2019, 104, 851–856. [Google Scholar] [CrossRef] [PubMed]
- Hametner, B.; Wassertheurer, S.; Kropf, J.; Mayer, C.; Eber, B.; Weber, T. Oscillometric estimation of aortic pulse wave velocity: Comparison with intra-aortic catheter measurements. Blood Press. Monit. 2013, 18, 173–176. [Google Scholar] [CrossRef]
- Weiss, W.; Gohlisch, C.; Zidek, W.; Van Der Giet, M. Oscillometric Estimation of Central Blood Pressure: Validation of the Mobil-O-Graph® in Comparison to the Sphygmocor® Device. J. Hypertens. 2011, 29, e1–e2. [Google Scholar] [CrossRef]
- Sharman, J.E.; Avolio, A.P.; Baulmann, J.; Benetos, A.; Blacher, J.; Blizzard, C.L.; Boutouyrie, P.; Chen, C.-H.; Chowienczyk, P.; Cockcroft, J.R.; et al. Validation of non-invasive central blood pressure devices: ARTERY Society task force consensus statement on protocol standardization. Eur. Heart J. 2017, 38, 2805–2812. [Google Scholar] [CrossRef]
- Shiraishi, M.; Murakami, T.; Higashi, K. The accuracy of central blood pressure obtained by oscillometric noninvasive method using Mobil-O-Graph in children and adolescents. J. Hypertens. 2020, 38, 813–820. [Google Scholar] [CrossRef]
- Elmenhorst, J.; Hulpke-Wette, M.; Barta, C.; Pozza, R.D.; Springer, S.; Oberhoffer, R. Percentiles for central blood pressure and pulse wave velocity in children and adolescents recorded with an oscillometric device. Atherosclerosis 2015, 238, 9–16. [Google Scholar] [CrossRef]
- Salvi, P.; Scalise, F.; Rovina, M.; Moretti, F.; Salvi, L.; Grillo, A.; Gao, L.; Baldi, C.; Faini, A.; Furlanis, G.; et al. Noninvasive estimation of aortic stiffness through different approaches: Comparison with intra-aortic recordings. Hypertension 2019, 74, 117–129. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Alsubheen, S.A.; George, A.M.; Baker, A.; Rohr, L.E.; Basset, F.A. Accuracy of the vivofit activity tracker. J. Med. Eng. Technol. 2016, 40, 298–306. [Google Scholar] [CrossRef]
- Price, K.; Bird, S.R.; Lythgo, N.; Raj, I.S.; Wong, J.Y.; Lynch, C. Validation of the Fitbit One, Garmin Vivofit and Jawbone UP activity tracker in estimation of energy expenditure during treadmill walking and running. J. Med. Eng. Technol. 2017, 41, 208–215. [Google Scholar] [CrossRef]
- Bull, F.C.; Al-Ansari, S.S.; Biddle, S.; Borodulin, K.; Buman, M.P.; Cardon, G.; Carty, C.; Chaput, J.-P.; Chastin, S.; Chou, R.; et al. World Health Organization 2020 guidelines on physical activity and sedentary behaviour. Br. J. Sports Med. 2020, 54, 1451–1462. [Google Scholar] [CrossRef] [PubMed]
- Niwa, K.; Perloff, J.K.; Bhuta, S.M.; Laks, H.; Drinkwater, D.C.; Child, J.S.; Miner, P.D. Structural abnormalities of great arterial walls in congenital heart disease: Light and electron microscopic analyses. Circulation 2001, 103, 393–400. [Google Scholar] [CrossRef] [PubMed]
- Murakami, T.; Tateno, S.; Kawasoe, Y.; Niwa, K. Aortic surgery is one of the risk factors for enhancement of pressure wave reflection in adult patients with congenital heart disease. Int. J. Cardiol. 2014, 175, 451–454. [Google Scholar] [CrossRef]
- Giannattasio, C.; Mancia, G. Arterial distensibility in humans. Modulating mechanisms, alterations in diseases and effects of treatment. J. Hypertens. 2002, 20, 1889–1899. [Google Scholar] [CrossRef] [PubMed]
- Lubans, D.R.; Morgan, P.J.; Callister, R.; Collins, C.E. Effects of Integrating Pedometers, Parental Materials, and E-mail Support Within an Extracurricular School Sport Intervention. J. Adolesc. Health 2009, 44, 176–183. [Google Scholar] [CrossRef]
- Schwartz, J.E.; Feig, P.U.; Izzo, J.L., Jr. Pulse wave velocities derived from cuff ambulatory pulse wave analysis: Effects of age and systolic blood pressure. Hypertension 2019, 74, 111–116. [Google Scholar] [CrossRef] [PubMed]

{kind=link}
| Subgroup CHD | n | Sex ♀ | Age (Years) | BMI z-Score | PWV (m/s) | cSBP (mmHg) | MVPA (min/Day) | Steps/Day |
|---|---|---|---|---|---|---|---|---|
| Total | 387 | 162 (42) | 12.2 ± 3.3 | −0.32 ± 1.19 | 4.60 ± 0.44 | 99.3 ± 10.8 | 83.3 ± 28.1 | 9386 ± 3090 |
| CHD Diagnosis | ||||||||
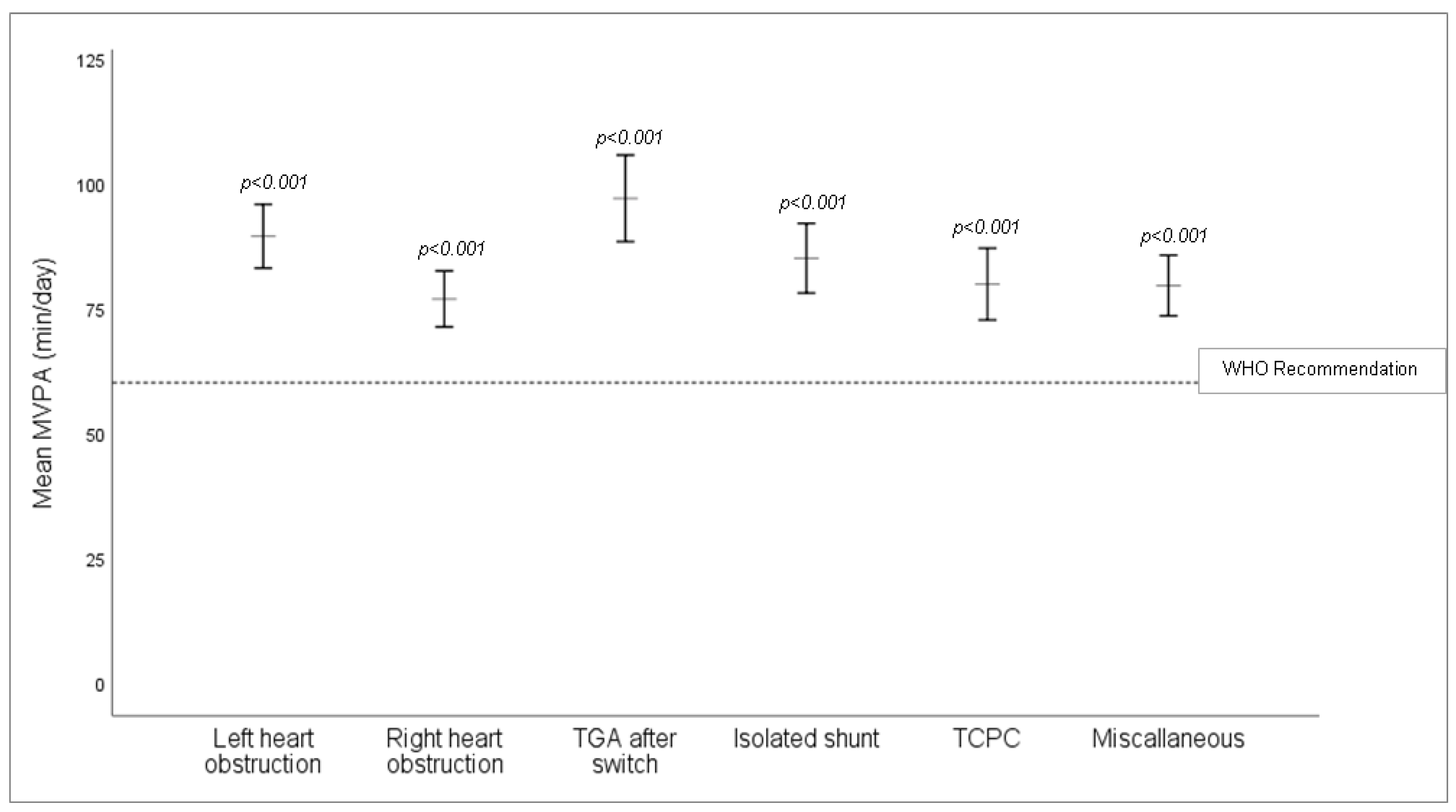
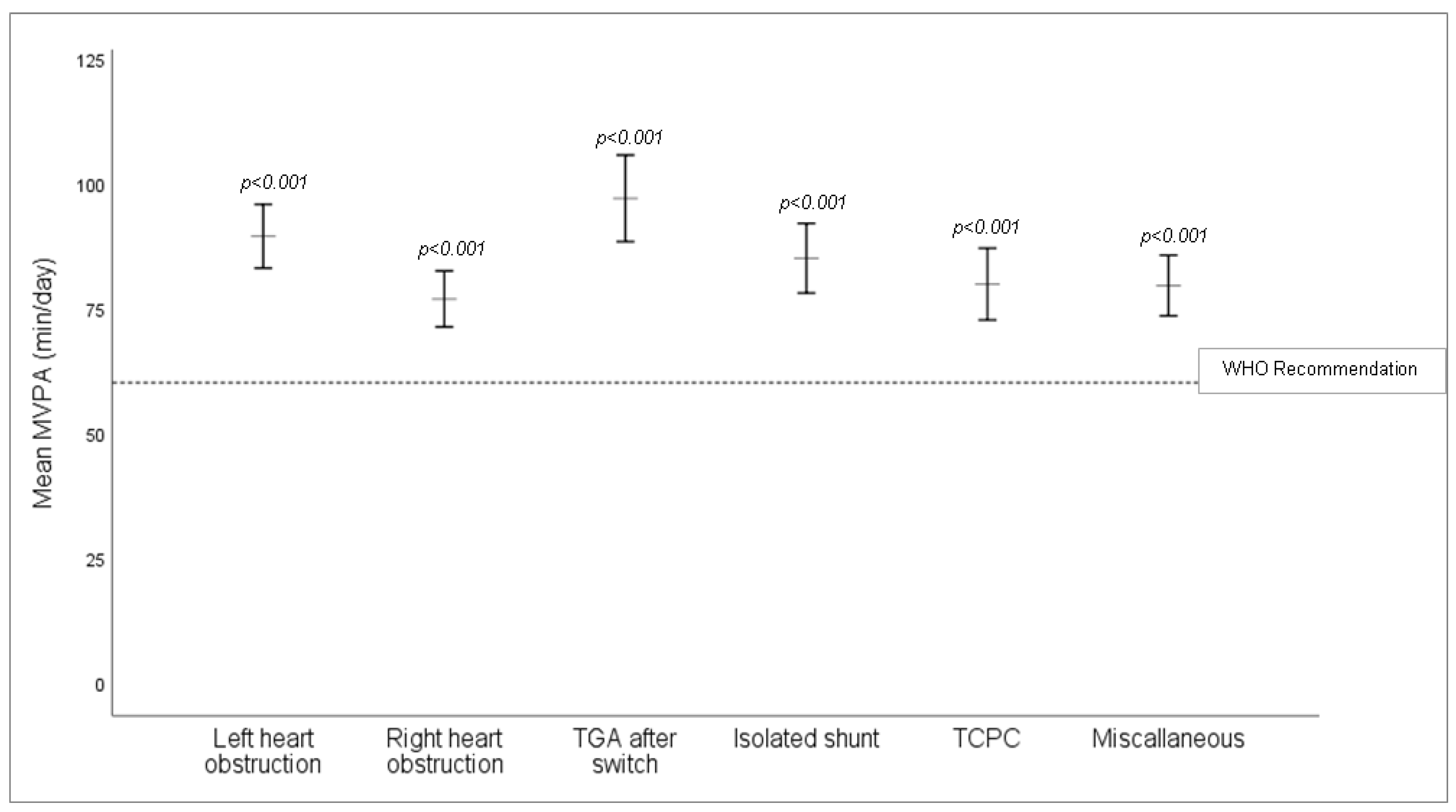
| Left heart obstruction | 69 | 21 (30) | 12.3 ± 3.3 | −0.58 ± 1.18 | 4.55 ± 0.46 | 101 ± 13.8 | 89.2 ± 29.8 | 9976 ± 3387 |
| Right heart obstruction | 89 | 35 (39) | 12.1 ± 3.0 | −0.44 ± 1.43 | 4.58 ± 0.42 | 98.1 ± 10.1 | 77.2 ± 29.1 | 9233 ± 3084 |
| Isolated shunts | 57 | 31 (54) | 12.3 ± 3.5 | −0.02 ± 1.05 | 4.58 ± 0.42 | 99.8 ± 11.1 | 83.8 ± 26.0 | 9309 ± 2905 |
| TGA after switch | 37 | 9 (24) | 11.8 ± 3.1 | −0.12 ± 0.97 | 4.60 ± 0.38 | 98.7 ± 10.9 | 98.3 ± 29.7 | 11,260 ± 3460 |
| TCPC | 57 | 19 (33) | 12.9 ± 3.5 | −0.18 ± 1.03 | 4.66 ± 0.47 | 100 ± 10.4 | 98.3 ± 29.7 | 9043 ± 2768 |
| Miscellaneous | 78 | 47 (60) | 11.9 ± 3.6 | −0.39 ± 1.17 | 4.55 ± 0.32 | 98.4 ± 7.9 | 79.2 ± 23.4 | 8456 ± 2560 |
| Surgical status | ||||||||
| Native CHD | 112 | 51 (46) | 11.8 ± 3.4 | −0.26 ± 1.09 | 4.49 ± 0.37 | 98.2 ± 10.8 | 83.1 ± 28.8 | 9383 ± 3061 |
| Heart surgery | 275 | 111 (40) | 12.4 ± 3.3 | −0.35 ± 1.23 | 4.62 ± 0.42 | 99.8 ± 10.8 | 83.3 ± 27.8 | 9387 ± 3107 |
| CHD severity * | ||||||||
| Simple | 74 | 36 (49) | 12.3 ± 3.6 | −0.07 ± 1.12 | 4.57 ± 0.41 | 99.7 ± 11.1 | 85.4 ± 26.9 | 9653 ± 3034 |
| Moderate | 119 | 46 (39) | 11.7 ± 3.1 | −0.39 ± 1.16 | 4.57 ± 0.47 | 100.3 ± 13.1 | 81.7 ± 28.6 | 9365 ± 3161 |
| Complex | 171 | 65 (38) | 12.4 ± 3.3 | −0.42 ± 1.26 | 4.61 ± 0.38 | 98.7 ± 9.1 | 84.8 ± 28.7 | 9551 ± 3083 |
| Yes | 58 | 24 (41) | 12.1 ± 3.4 | −0.45 ± 1.09 | 4.41 ± 0.34 | 96.4 ± 11.7 | 74.1 ± 23.3 | 8336 ± 3240 |
| No | 329 | 138 (42) | 12.2 ± 3.3 | −0.30 ± 1.21 | 4.61 ± 0.41 | 99.8 ± 10.6 | 84.9 ± 28.5 | 9571 ± 3030 |
| Adjusted R2 | ß | 95%CI | p-Value | |
|---|---|---|---|---|
| PWV (m/s) | 0.748 | −0.025 | [−0.001; 0.001] | 0.446 |
| cSBP (mmHg) | 0.748 | −0.020 | [−0.035; 0.019] | 0.552 |
| Low-Active CHD (n = 78) | High-Active CHD (n = 309) | p-Value | |
|---|---|---|---|
| Sex, female | 40 (51%) | 122 (40%) | 0.079 |
| Age, years | 13.3 ± 3.3 | 11.9 ± 3.3 | 0.002 † |
| BMI, z-score | −0.20 ± 1.6 | −0.36 ± 1.1 | 0.298 † |
| MVPA, min/day | 47.8 ± 11.8 | 92.1 ± 23.6 | <0.001 † |
| Steps/day | 6150 ± 2014 | 10,203 ± 2762 | <0.001 † |
| PWV, m/s | 4.70 ± 0.4 | 4.55 ± 0.4 | 0.467 ‡ |
| cSBP, mmHg | 101.1 ± 9.9 | 98.9 ± 11.0 | 0.359 ‡ |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Willinger, L.; Brudy, L.; Oberhoffer-Fritz, R.; Ewert, P.; Müller, J. Association between Objectively Measured Physical Activity and Arterial Stiffness in Children with Congenital Heart Disease. J. Clin. Med. 2021, 10, 3266. https://doi.org/10.3390/jcm10153266
Willinger L, Brudy L, Oberhoffer-Fritz R, Ewert P, Müller J. Association between Objectively Measured Physical Activity and Arterial Stiffness in Children with Congenital Heart Disease. Journal of Clinical Medicine. 2021; 10(15):3266. https://doi.org/10.3390/jcm10153266
Chicago/Turabian StyleWillinger, Laura, Leon Brudy, Renate Oberhoffer-Fritz, Peter Ewert, and Jan Müller. 2021. "Association between Objectively Measured Physical Activity and Arterial Stiffness in Children with Congenital Heart Disease" Journal of Clinical Medicine 10, no. 15: 3266. https://doi.org/10.3390/jcm10153266
APA StyleWillinger, L., Brudy, L., Oberhoffer-Fritz, R., Ewert, P., & Müller, J. (2021). Association between Objectively Measured Physical Activity and Arterial Stiffness in Children with Congenital Heart Disease. Journal of Clinical Medicine, 10(15), 3266. https://doi.org/10.3390/jcm10153266