
Nutritional Therapy in Pediatric Crohn’s Disease—Are We Going to Change the Guidelines?


Abstract
:1. Introduction
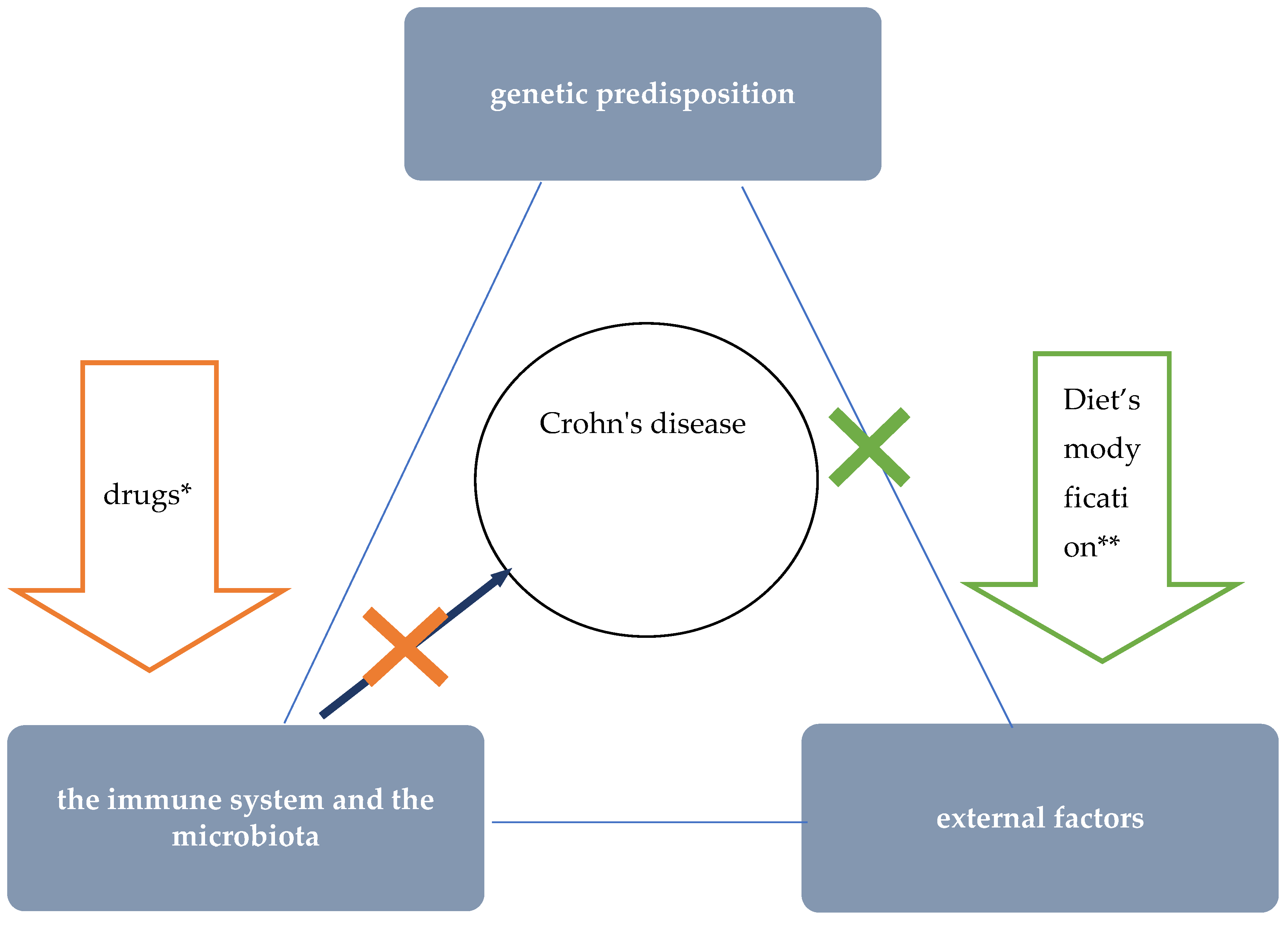
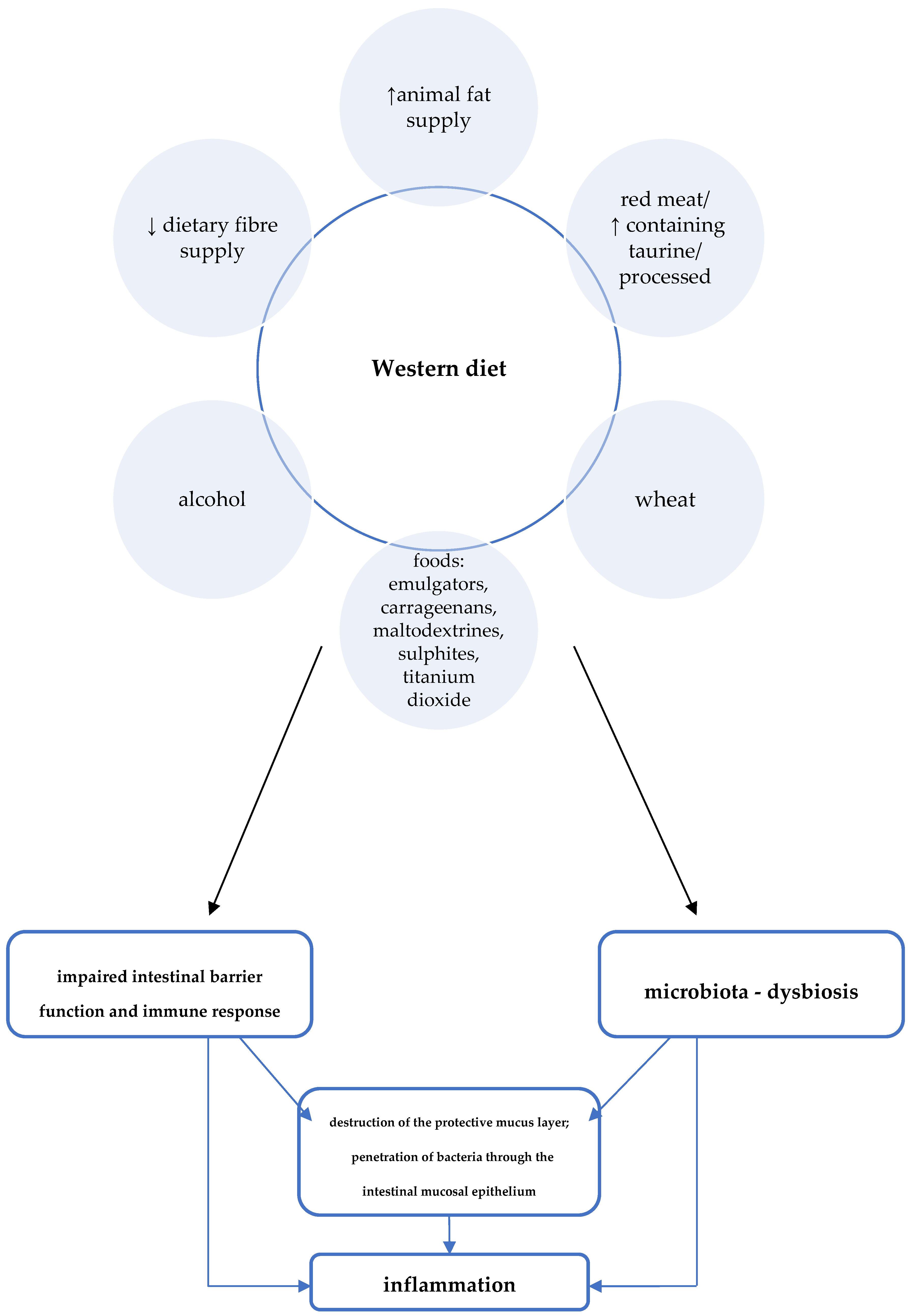
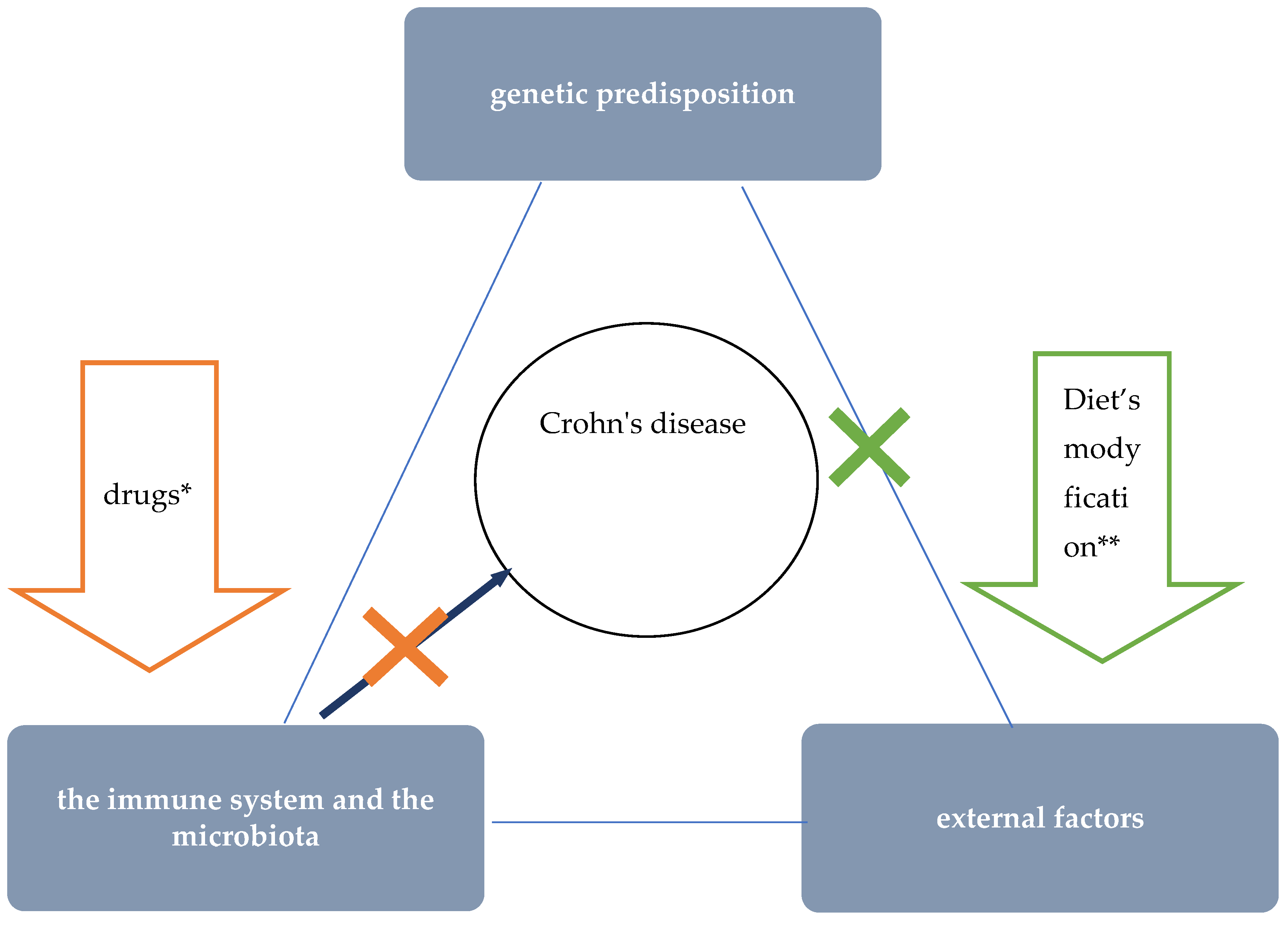
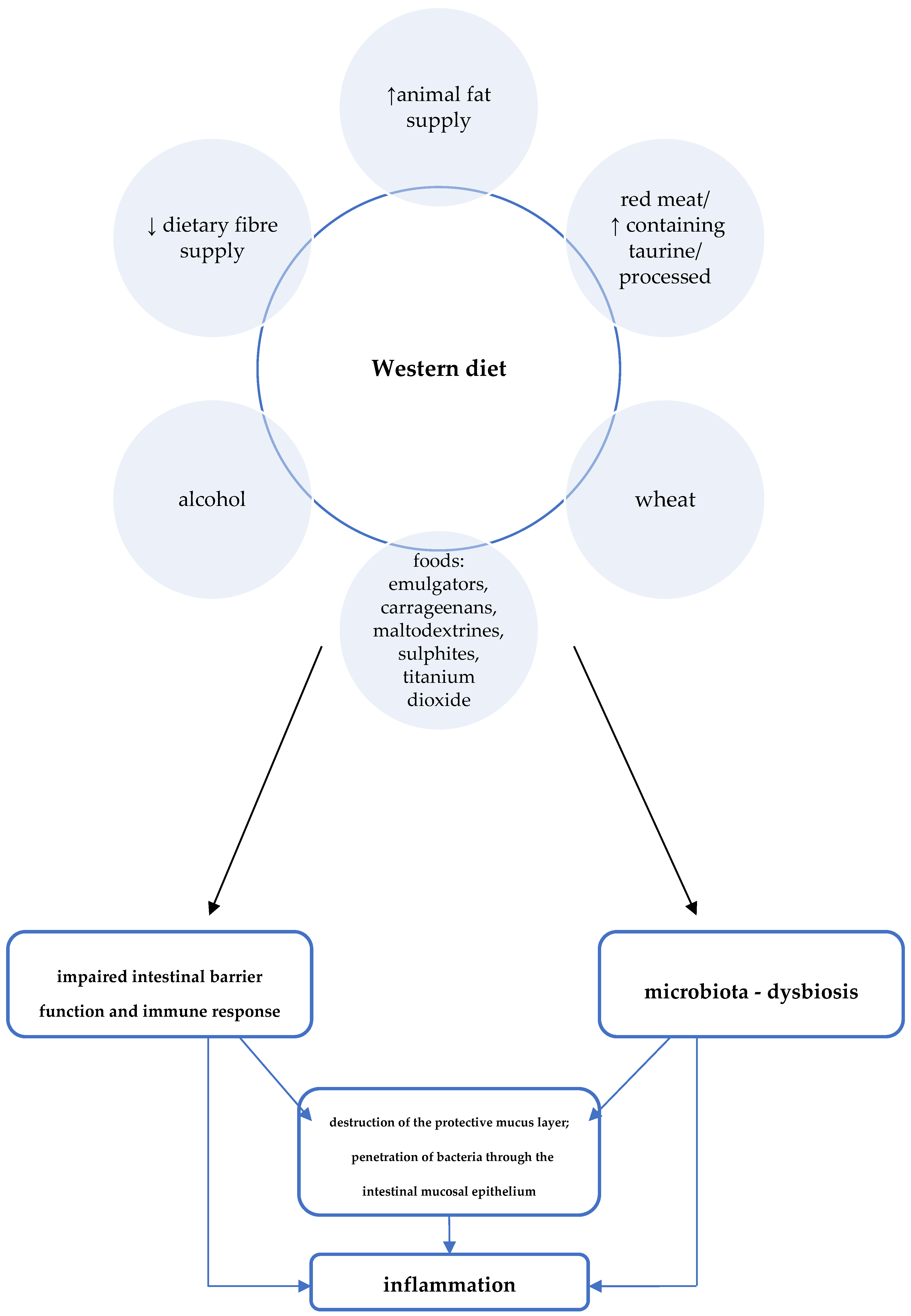
2. Diet and the Pathogenesis of Crohn’s Disease
- by influencing the activity of immune cells and their migration to the site of inflammation, they exhibit anti-inflammatory effects;
- by nourishing colonocytes, providing them with a primary source of energy;
- by reducing the pH in the intestine, positively influencing the composition of the intestinal microbiota (stimulating the growth of beneficial strains of bacteria and inhibiting the growth of pathogenic bacteria).
3. Why Are the Currently Recommended Nutritional Treatments in the Pediatric Population Not Fully Satisfying for Us?
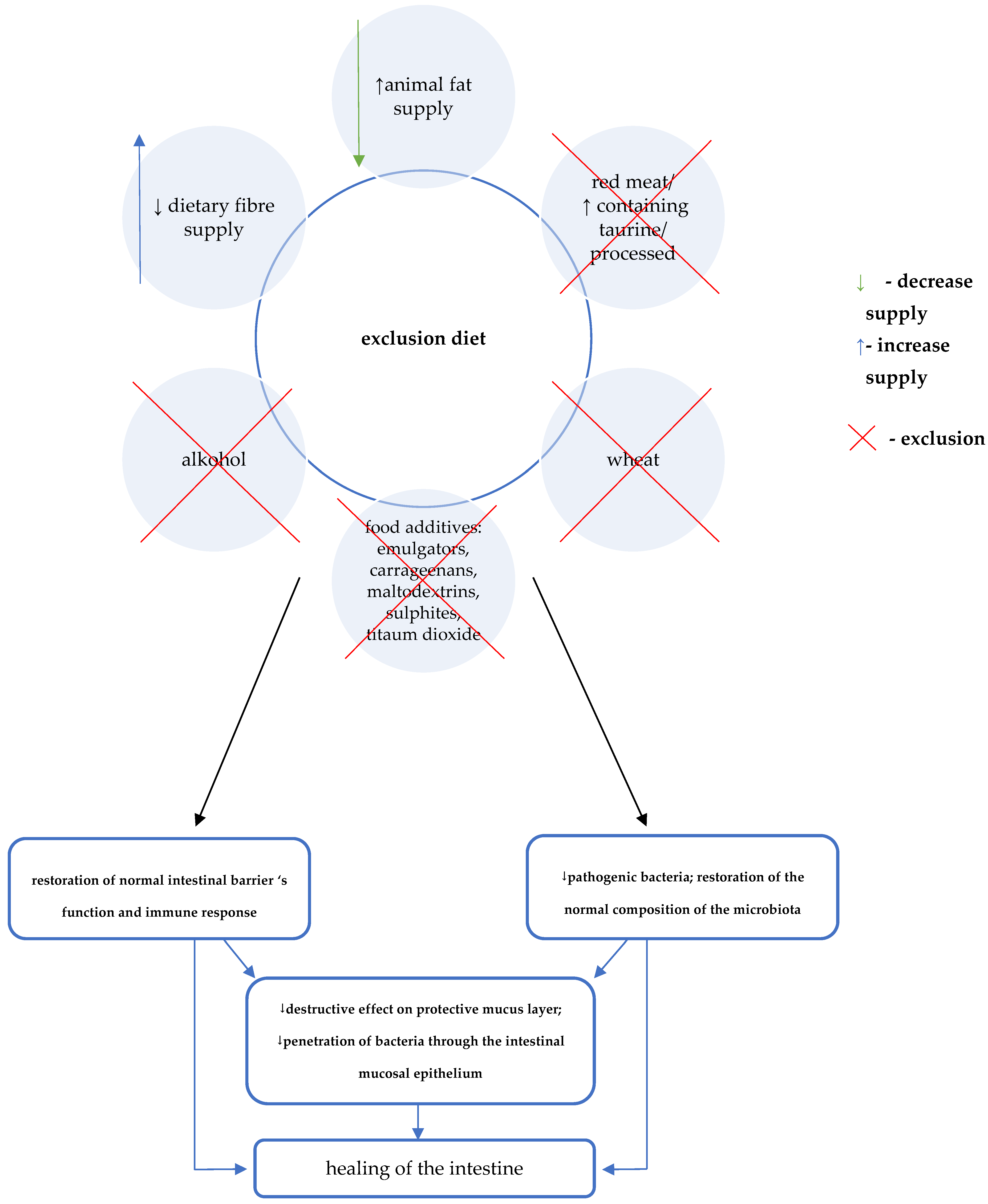
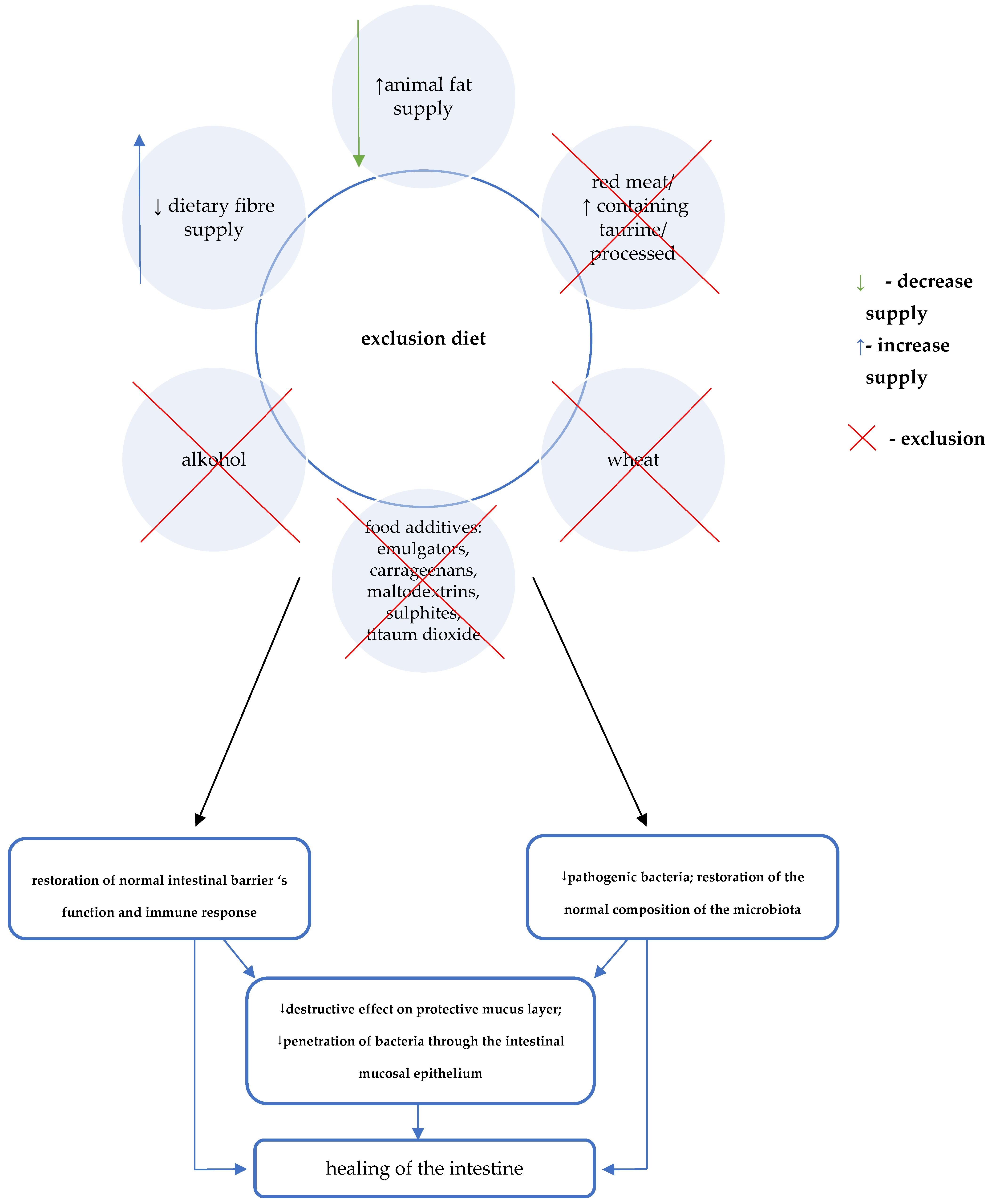
4. CDED—Protocol and Mechanism of Action
- –
- mandatory, i.e., recommended for daily consumption. Their role is to provide adequate nutritional value of the diet as well as substrates for the production of SCFA;
- –
- neutral, which are supposed to add variety to the daily menu, but do not necessarily have to be consumed.
- –
- forbidden.
5. Effectiveness of Crohn’s Disease Exclusion Diet in Studies
6. The ModuLife Project and Application
7. Summary
Author Contributions
Funding
Conflicts of Interest
References
- Kaplan, G.G. The global burden of IBD: From 2015 to 2025. Nat. Rev. Gastroenterol. Hepatol. 2015, 12, 720–727. [Google Scholar] [CrossRef] [PubMed]
- Ghione, S.; Sarter, H.; Fumery, M.; Armengol-Debeir, A.; Savoye, G.; Ley, D.; Spyckerelle, C.; Pariente, B.; Peyrin-Biroulet, L.; Turck, D.; et al. Dramatic increase in incidence of ulcerative colitis and Crohn’s disease [1988–2011]: A population-based study of French adolescents. Am. J. Gastroenterol. 2018, 113, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Olen, O.; Askling, J.; Sachs, M.C.; Frumento, P.; Neovius, M.; Smedby, K.E.; Ekbom, A.; Malmborg, P.; Ludvigsson, J.F. Increased mortality of patients with childhood-onset inflammatory bowel diseases, compared with the general population. Gastroenterology 2019, 156, 614–622. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Joosse, M.E.; Aardoom, M.A.; Kemos, P.; Turner, D.; Wilson, D.C.; Koletzko, S.; Martin-de-Carpi, J.; Fagerbelg, U.L.; Spray, C.; Tzivinikos, C.; et al. Malignancy and mortality in paediatric-onset inflammatory bowel disease: A 3-year prospective, multinational study from the paediatric IBD Porto group of ESPGHAN. Aliment. Pharmacol. Ther. 2018, 48, 523–537. [Google Scholar] [CrossRef] [PubMed]
- Grover, Z.; Lewindon, P. Two-year outcomes after exclusive enteral nutrition induction are superior to corticosteroids in pediatric Crohn’s disease treated early with thiopurines. Dig. Dis. Sci. 2015, 60, 3069–3074. [Google Scholar] [CrossRef]
- Levine, A.; Boneh, R.S.; Wine, E. Evolving role of diet in the pathogenesis and treatment of inflammatory bowel diseases. Gut 2018, 67, 1726–1738. [Google Scholar] [CrossRef]
- Levine, A.; Wine, E.; Assa, A.; Sigall Boneh, R.; Shaoul, R.; Kori, M.; Cohen, S.; Peleg, S.; Shamaly, H.; On, A.; et al. Crohn’s Disease Exclusion Diet Plus Partial Enteral Nutrition Induces Sustained Remission in a Randomized Controlled Trial. Gastroenterology 2019, 157, 440–450. [Google Scholar] [CrossRef] [Green Version]
- Lewis, J.D.; Abreu, M.T. Diet as a Trigger or Therapy for Inflammatory Bowel Diseases. Gastroenterology 2017, 152, 398–414. [Google Scholar] [CrossRef]
- Devkota, S.; Wang, Y.; Musch, M.W.; Leone, V.; Fehlner-Peach, H.; Nadimpalli, A.; Antonopoulos, D.A.; Jabri, B.; Chang, E.B. Dietary-fat-induced taurocholic acid promotes pathobiont expansion and colitis in Il10-/- mice. Nature 2012, 487, 104–108. [Google Scholar] [CrossRef] [Green Version]
- Khalili, H.; Hakansson, N.; Chan, S.S.; Chen, Y.; Lochhead, P.; Ludvigsson, J.F.; Chan, A.T.; Hart, A.R.; Olén, O.; Wolk, W. Adherence to a Mediterranean diet is associated with a lower risk of later-onset Crohn’sdisease: Results from two large prospective cohort studies. Gut 2020, 69, 1637–1644. [Google Scholar] [CrossRef]
- Torres, J.; Bonovas, S.; Doherty, G.; Kucharzik, K.; Gisbert, J.P.; Raine, T.; Adamina, M.; Armuzzi, A.; Bachmann, O.; Bager, P.; et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Medical Treatment. J. Crohns Colitis 2020, 14, 4–22. [Google Scholar] [CrossRef] [PubMed]
- Maconi, G.; Armuzzi, A. Beyond remission and mucosal healing in Crohn’s disease. Exploring the deep with cross sectional imaging. Dig. Liver Dis. 2017, 49, 457–458. [Google Scholar] [CrossRef]
- Borrelli, O.; Cordischi, L.; Cirulli, M.; Paganelli, M.; Labalestra, V.; Uccini, S.; Russo, P.M.; Cucchiara, S. Polymeric diet alone versus corticosteroids in the treatment of active pediatric Crohn’s disease: A randomized controlled open-label trial. Clin. Gastroenterol. Hepatol. 2006, 4, 744–753. [Google Scholar] [CrossRef]
- Pigneur, B.; Lepage, P.; Mondot, S.; Schmitz, J.; Goulet, O.; Dore, J.; Romuelle, F. Mucosal healing and bacterial composition in response to enteral nutrition vs steroid-based induction therapy-a randomised prospective clinical trial in children with Crohn’s disease. J. Crohns Colitis 2019, 13, 846–855. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.; Turner, D.; Gik, T.P.; Dias, J.A.; Veres, G.; Shaoul, R.; Staiano, A.; Escher, J.; Kolho, K.L.; Paerregaard, A.; et al. Comparison of outcomes parameters for induction of remission in new onset pediatric Crohn’s disease: Evaluation of the porto IBD group growth relapse and outcomes with therapy (GROWTH CD) study. Inflamm. Bowel Dis. 2014, 20, 278–285. [Google Scholar] [CrossRef] [PubMed]
- van Rheenen, P.F.; Aloi, M.; Assa, A.; Bronsky, J.; Escher, J.C.; Fagerberg, U.L.; Gasparetto, M.; Gerasimidis, K.; Griffiths, A.; Henderson, P.; et al. The Medical Management of Paediatric Crohn’s Disease: An ECCO-ESPGHAN Guideline Update. J. Crohns Colitis 2020, 15, 171–194. [Google Scholar] [CrossRef]
- Van Limbergen, J.; Haskett, J.; Griffiths, A.M.; Critch, J.; Huynh, H.; Ahmed, N.; deBruyn, J.C.; Issenman, R.; El-Matary, W.; Walters, T.D.; et al. Toward enteral nutrition for the treatment of pediatric Crohn disease in Canada: A workshop to identify barriers and enablers. Can. J. Gastroenterol. Hepatol. 2015, 29, 351–356. [Google Scholar] [CrossRef]
- Lawley, M.; Wu, J.W.; Navas-Lopez, V.M.; Huynh, Q.H.; Carroll, M.W.; Chen, M.; Medvedev, P.; Day, A.S.; Hussey, S.; Sigall-Boneh, R.; et al. Global variation in use of enteral nutrition for pediatric Crohn disease. J. Pediatr. Gastroenterol. Nutr. 2018, 67, e22–e29. [Google Scholar] [CrossRef]
- Miele, E.; Shamir, R.; Aloi, M.; Assa, A.; Braegger, C.; Bronsky, J.; de Ridder, L.; Escher, J.C.; Hojsak, I.; Kolaček, S.; et al. Nutrition in Paediatric Inflammatory Bowel Disease: A Position Paper on Behalf of The Porto IBD Group of ESPGHAN. J. Pediatr. Gastroenterol. Nutr. 2018, 66, 687–708. [Google Scholar] [CrossRef] [Green Version]
- Svolos, V.; Hansen, R.; Nichols, B.; Quince, C.; Ijaz, U.Z.; Papadopoulou, R.T.; Edwards, C.A.; Watson, D.; Alghamdi, A.; Brejnrod, A.; et al. Treatment of active Crohn’s disease with an ordinary food-based diet that replicates exclusive enteral nutrition. Gastroenterology 2019, 156, 1354–1367. [Google Scholar] [CrossRef] [Green Version]
- Charlebois, A.; Rosenfeld, G.; Bressler, B. The impact of dietary interventions on the symptoms of inflammatory bowel disease: A systematic review. Crit. Rev. Food Sci. Nutr. 2016, 56, 1370–1378. [Google Scholar] [CrossRef]
- Roberts, C.L.; Rushworth, S.L.; Richman, E.; Rhodes, J.M. Hypothesis: Increased consumption of emulsifiers as an explanation for the rising incidence of Crohn’s disease. J. Crohns Colitis 2013, 7, 338–341. [Google Scholar] [CrossRef] [Green Version]
- Chassaing, B.; Koren, O.; Goodrich, J.K.; Poole, A.C.; Srinivasan, S.; Ley, R.E.; Gewirtz, A.T. Dietary emulsifiers impact the mouse gut microbiota promoting colitis and metabolic syndrome. Nature 2015, 519, 92–96. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Chassaing, B.; Van de Wiele, T.; De Bodt, J.; Marzorati, M.; Gewirtz, A.T. Dietary emulsifiers directly alter human microbiota composition and gene expression ex vivo potentiating intestinal inflammation. Gut 2017, 66, 1414–1427. [Google Scholar] [CrossRef]
- Czajkowska, A.; Szponar, B. Krótkołańcuchowe kwasy tłuszczowe (SCFA) jako produkty metabolizmu bakterii jelitowych oraz ich znaczenie dla organizmu gospodarza. Postepy. Hig. Med. Dosw. 2018, 72, 131–142. [Google Scholar] [CrossRef]
- Agus, A.; Denizot, J.; Thévenot, J.; Martinez-Medina, M.; Massier, S.; Sauvanet, P.; Bernalier-Donadille, A.; Denis, S.; Hofman, P. Western diet induces a shift in microbiota composition enhancing susceptibility to Adherent-Invasive, E. coli infection and intestinal inflammation. Sci. Rep. 2016, 6, 19032. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Swaminath, A.; Feathers, A.; Ananthakrishnan, A.; Falzon, L.; Ferry, S.L. Systematic Review with Meta-Analysis: Enteral Nutrition Therapy for the Induction of Remission in Pediatric Crohn’s Disease. Aliment. Pharmacol. Ther. 2017, 46, 645–656. [Google Scholar] [CrossRef] [Green Version]
- Matuszczyk, M.; Gawecka, A.; Grzybowska-Chlebowczyk, U.; Książyk, J.; Lebensztejn, D.; Popińska, K.; Romanowska, H.; Sładek, M.; Socha, P.; Szlagatys-Sidorkiewicz, A.; et al. Polskie wytyczne leczenia żywieniowego w nieswoistych chorobach zapalnych jelit u dzieci. Wytyczne Polskiego Towarzystwa Gastroenterologii, Hepatologii i Żywienia Dzieci oraz Polskiego Towarzystwa Żywienia Klinicznego Dzieci. Stand. Med. Pediatr. 2017, 14, 195–226. [Google Scholar]
- Nakar, I.; Focht, G.; Church, P.; Church, P.; Walters, T.D.; Abitbol, G.; Anupindi, S.; Berteloot, L.; Hulst, J.M.; Ruemmele, F.; et al. The association of mucosal healing (MH), transmural healing (TH) and calprotectin in paediatric Crohn’s disease: A report from the ImageKids study. Clin. Gastroenterol. Hepatol. 2018, 16, 1089–1097. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Sigall-Boneh, R.; Pfeffer-Gik, T.; Segal, I.; Zangen, T.; Boaz, M.; Levine, A. Partial enteral nutrition with a Crohn’s Disease exclusion diet is effective for induction of remission in children and young adults with Crohn’s disease. Inflamm. Bowel Dis. 2014, 20, 1353–1360. [Google Scholar] [CrossRef] [PubMed]
- Sigall Boneh, R.; Sarbagili Shabat, C.; Yanai, H.; Chermesh, I.; Avraham, S.B.; Mona Boaz, M.; Levine, A. Dietary therapy with the Crohn’s Disease exclusion diet is a successful strategy for induction of remission in children and adults failing biological therapy. J. Crohns Colitis 2017, 11, 1205–1212. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Levine, A.; El-Matary, W.; Van Limbergen, J. A Case-Based Approach to New Directions in Dietary Therapy of Crohn’s Disease: Food for Thought. Nutrients 2020, 12, 880. [Google Scholar] [CrossRef] [PubMed] [Green Version]
- Available online: https://modulifexpert.com (accessed on 6 July 2021).

{kind=link}
{kind=link}
{kind=link}
| Natural Products—Exclusion or Controlled Exposure | Food Additives—Exclusion |
|---|---|
|
|
| Mandatory Foods (Stages 1 and 2) | ||
|---|---|---|
| A balanced diet—source of complete protein with low taurine content | Additional benefits—sources of water-soluble dietary fibre (pectins) and resistant starch | |
|
| |
| Group of foods | allowed in stage 1 (weeks 1—6) | Additionally allowed in stage 1 (weeks 1—6) *** |
| Cereals | white rice, rice flour and rice pasta (in unlimited amounts) | - quinoa (in unlimited amounts) - sweet potato (½ can replace 1 potato, once a day) - oatmeal—½ cup 1—2 times a week (can be used to make oatmeal or oatmeal cookies) - one slice of whole-grain bread/day (without yeast) |
| Meat/fish/eggs | instead of chicken breast, a serving of lean white fish once a week. | - fresh lean beef (lean meat i.e., sirloin) can be eaten once a week instead of chicken breast - a serving of tuna in canola oil or olive oil once a week |
| Vegetables | - 2 tomatoes or 6 cherry tomatoes - 2 peeled cucumbers - 1 young carrot - fresh spinach (a cup once a day) - lettuce leaves (3 per day) - avocado (1 a day; max. ½/meal) | gradual introduction of new vegetables: - initially those containing lower amounts of dietary fibre (e.g., 1 small zucchini, 2 broccoli or cauliflower florets) - starting from week 10 other vegetables can br introduced (except for cabbage, leak, asparagus, artichoke and celery)—e.g., ½ of sweet red bell pepper, beet |
| Fruits | - strawberries (several a day) - a slice of melon | gradual introduction of new fruit: in weeks 7–9 1 pear, peach or kiwi/a day can be eaten—instead of a serving of strawberries, 10 bilberries (or a cup) can be eaten - form week 10 other fruits can be introduced (which contain more fibre), but in limited quantities—i.e., ½ cup of mango, pineapple cubes or orange slices (except for passion fruit, pomegranate, cactus, kaki) |
| Fats | - olive oil - canola oil | |
| Sugar and sweets | - honey (3 teaspoons a day) or - sugar (4 teaspoons a day) | |
| other | - legumes (lentils, chickpeas, beans, peas)—½ cup dry seeds a day) - almonds or walnuts (unsalted, unroasted, unprocessed)—8 pieces a day - tahini (without emulsifying agents and sulphites)—2 spoons a day | |
| fluids | - water (slices of lemon, lime, orange or mint leaves can be added to taste) - herbal teas (preferable from fresh leaves) - 1 glass of freshly squeezed orange juice | |
| Spices | -salt, pepper, paprika, cinnamon, cumin, turmeric - fresh herbs i.e.: mint, oregano, cilantro, rosemary, sage, basil, thyme, dill, parsley - other spices: onion, garlic, ginger, fresh lemon juice | |
| Foods Allowed 5 Days a Week * | Examples of Products Allowed 2 Days a Week ** | |
|---|---|---|
| Examples of Foods That Can Be Consumed for Breakfast: | Examples of Foods That Can Be Consumed for Lunch (Dinner): | |
| - other parts of chicken (except for skin or giblets) - fresh seafood, salmon (once a week)—1 serving of unprocessed, full-fat natural yoghurt (without additives) a day - 2 slices of whole-grain bread (without yeast), or 1 serving of pasta a day - all vegetables except for leak, celery stalks and large amounts of kale - all fruits (including dried fruits, without sulphites) except for passion fruit, pomegranate, cactus, kaki - 1 cup of black coffee (not instant) or tea | - any kind of bread - milk, cheese - crêpes - jams - 1 bowl of cereal with milk | - steaks, burgers, pork, seafood, fish, i.e., salmon and tuna, - any type of pasta - dairy products, including cheese - 1 serving of home-made dessert (e.g., cake) or one scoop of ice-cream - cocoa/dark chocolate |
| - or 1 meal eaten out instead of unrestricted meals prepared at home | ||
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Matuszczyk, M.; Kierkus, J. Nutritional Therapy in Pediatric Crohn’s Disease—Are We Going to Change the Guidelines? J. Clin. Med. 2021, 10, 3027. https://doi.org/10.3390/jcm10143027
Matuszczyk M, Kierkus J. Nutritional Therapy in Pediatric Crohn’s Disease—Are We Going to Change the Guidelines? Journal of Clinical Medicine. 2021; 10(14):3027. https://doi.org/10.3390/jcm10143027
Chicago/Turabian StyleMatuszczyk, Malgorzata, and Jaroslaw Kierkus. 2021. "Nutritional Therapy in Pediatric Crohn’s Disease—Are We Going to Change the Guidelines?" Journal of Clinical Medicine 10, no. 14: 3027. https://doi.org/10.3390/jcm10143027
APA StyleMatuszczyk, M., & Kierkus, J. (2021). Nutritional Therapy in Pediatric Crohn’s Disease—Are We Going to Change the Guidelines? Journal of Clinical Medicine, 10(14), 3027. https://doi.org/10.3390/jcm10143027