
Analysis of Effectiveness and Psychological Techniques Implemented in mHealth Solutions for Middle-Aged and Elderly Adults with Type 2 Diabetes: A Narrative Review of the Literature



Abstract
1. Introduction
2. Materials and Methods
2.1. Study Design
2.2. Study Selection
2.3. Information Sources
2.4. Search Terms
2.5. Data Extraction
3. Results
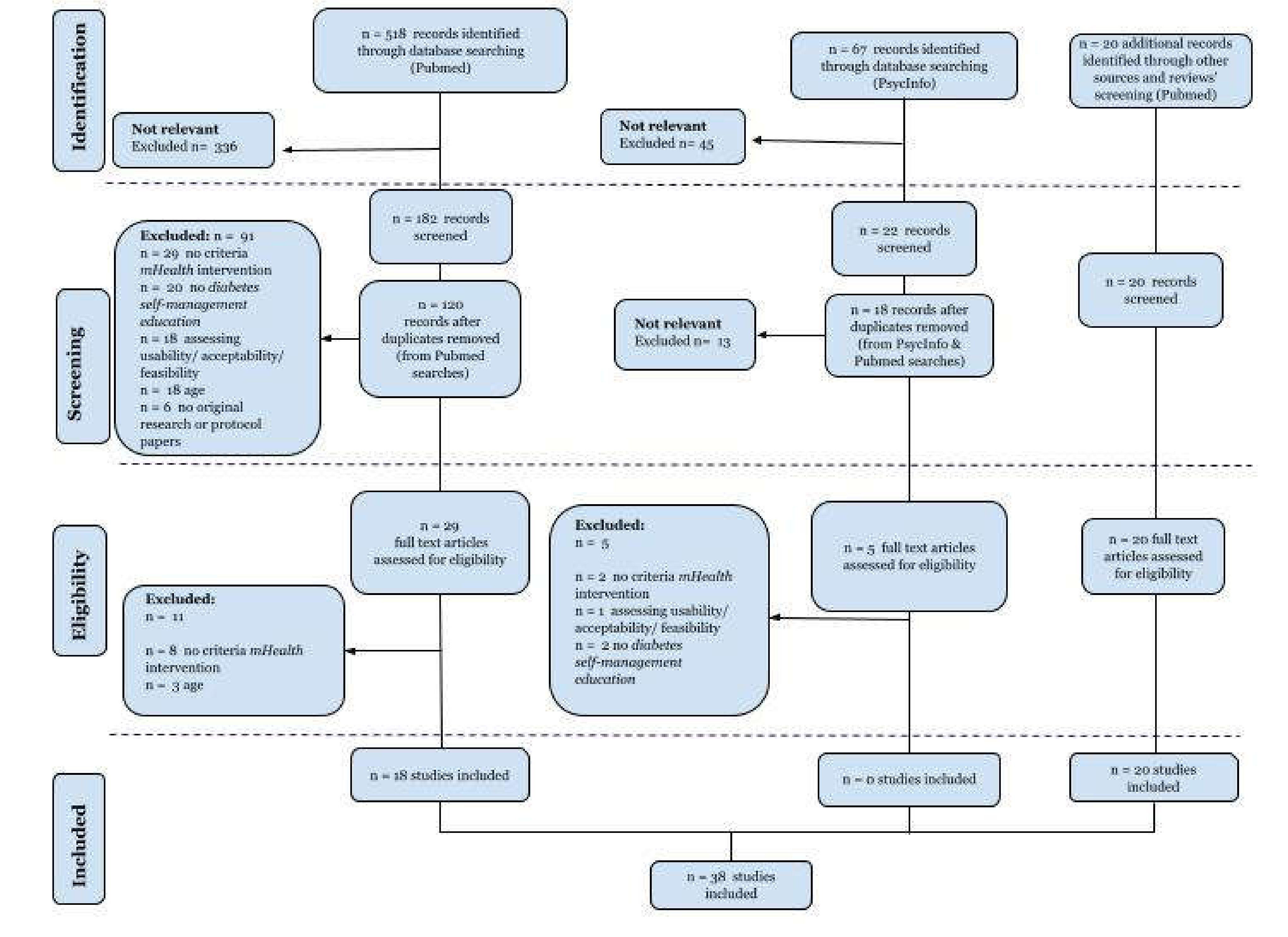
3.1. Synthesis of Search Results
3.2. Synthesis of Study Characteristics and Outcome Measures
3.3. Type of Interventions & Psychological Techniques
4. Discussion
4.1. Discussion of Main Findings
4.2. Weaknesses and Strengths of Studies Included in This Review
4.3. Implication of Policy Making and Further Research
5. Conclusions
Supplementary Materials
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Istepanian, R.; Laxminarayan, S.; Pattichis, C.S. M-Health: Emerging Mobile Health Systems; Springer Science & Business Media: Berlin, Germany, 2007; ISBN 9780387265599. [Google Scholar]
- Kay, M.; Santos, J. Report on the world health organization global observatory for ehealth strategic planning workshop, April 2008. Methods Inf. Med. 2008, 47, 381–387. [Google Scholar] [PubMed]
- Sloninsky, D. Towards the Development of an MHealth Strategy: A Literature Review; 2008; WHO: Geneva, Switzerland, 2008. [Google Scholar]
- Car, J.; Tan, W.S.; Huang, Z.; Sloot, P.; Franklin, B.D. eHealth in the future of medications management: Personalisation, monitoring and adherence. BMC Med. 2017, 15, 73. [Google Scholar] [CrossRef]
- Wong, R.; Ofstedal, M.B.; Yount, K.; Agree, E.M. Unhealthy lifestyles among older adults: Exploring transitions in Mexico and the US. Eur. J. Ageing 2008, 5, 311–326. [Google Scholar] [CrossRef] [PubMed]
- Global burden of diabetes. International Diabetes federation. Diabetic atlas 8th edition 2017, Brussels. Available online: https://www.idf.org/e-library/epidemiology-research/diabetes-atlas.html (accessed on 7 March 2019).
- 8940_IDF_Atlas_2017_Spanish_Interactive. Available online: https://diabetesatlas.org/IDF_Diabetes_Atlas_8e_interactive_ES/ (accessed on 25 April 2019).
- Shaw, J.E.; Sicree, R.A.; Zimmet, P.Z. Global Estimates of the Prevalence of Diabetes for 2010 and 2030. Diabetes Res. Clin. Pract. 2010, 87, 4–14. [Google Scholar] [CrossRef] [PubMed]
- Global Health and Aging. Available online: https://www.nia.nih.gov/sites/default/files/2017-06/global_health_aging.pdf (accessed on 25 April 2019).
- Wild, S.; Roglic, G.; Green, A.; Sicree, R.; King, H. Global Prevalence of Diabetes: Estimates for the Year 2000 and Projections for 2030. Diabetes Care 2004, 27, 1047–1053. [Google Scholar] [CrossRef] [PubMed]
- García-Pérez, L.-E.; Álvarez, M.; Dilla, T.; Gil-Guillén, V.; Orozco-Beltrán, D. Adherence to therapies in patients with type 2 diabetes. Diabetes Ther. 2013, 4, 175–194. [Google Scholar] [CrossRef]
- McGovern, A.; Tippu, Z.; Hinton, W.; Munro, N.; Whyte, M.; De Lusignan, S. Comparison of medication adherence and persistence in type 2 diabetes: A systematic review and meta-analysis. Diabetes Obes. Metab. 2018, 20, 1040–1043. [Google Scholar] [CrossRef]
- Del Cañizo-Gómez, F.J.; Del Cañizo-Gómez, F.J.; Moreira-Andrés, M.N. Cardiovascular risk factors in patients with type 2 diabetes. Diabetes Res. Clin. Pract. 2004, 65, 125–133. [Google Scholar] [CrossRef]
- Marín-Peñalver, J.J.; Martín-Timón, I.; Sevillano-Collantes, C.; Del Cañizo-Gómez, F.J. Update on the treatment of type 2 diabetes mellitus. World J. Diabetes 2016, 7, 354–395. [Google Scholar] [CrossRef]
- American Diabetes Association 6. Glycemic targets: Standards of medical care in diabetes—2018. Diabetes Care 2018, 41, S55–S64. [Google Scholar] [CrossRef]
- Beck, J.; Greenwood, D.A.; Blanton, L.; Bollinger, S.T.; Butcher, M.K.; Condon, J.E.; Cypress, M.; Faulkner, P.; Fischl, A.H.; Francis, T.; et al. 2017 national standards for diabetes self-management education and support. Diabetes Care 2017, 40, 1409–1419. [Google Scholar] [CrossRef]
- American Diabetes Association 4. Lifestyle Management: Standards of medical care in diabetes—2018 Diabetes Care 2018, 41, S38–S50.
- Bergenstal, R.M.; Layne, J.E.; Zisser, H.; Gabbay, R.A.; Barleen, N.A.; Lee, A.A.; Majithia, A.R.; Parkin, C.G.; Dixon, R.F. Remote application and use of real-time continuous glucose monitoring by adults with type 2 diabetes in a virtual diabetes clinic. Diabetes Technol. Ther. 2021, 23, 128–132. [Google Scholar] [CrossRef]
- Triberti, S.; Bigi, S.; Rossi, M.G.; Caretto, A.; Laurenzi, A.; Dozio, N.; Scavini, M.; Pergolizzi, E.; Ozzello, A.; Serino, S.; et al. The activeageing mobile app for diabetes self-management: First adherence data and analysis of patients’ in-app notes. Lect. Notes Inst. Comput. Sci. Soc. Inform. Telecommun. Eng. 2018, 253, 129–138. [Google Scholar]
- Martínez-Pérez, B.; De la Torre-Díez, I.; López-Coronado, M. Mobile health applications for the most prevalent conditions by the world health organization: Review and analysis. J. Med. Internet Res. 2013, 15, e120. [Google Scholar] [CrossRef]
- Årsand, E.; Frøisland, D.H.; Skrøvseth, S.O.; Chomutare, T.; Tatara, N.; Hartvigsen, G.; Tufano, J.T. Mobile health applications to assist patients with diabetes: Lessons learned and design implications. J. Diabetes Sci. Technol. 2012, 6, 1197–1206. [Google Scholar] [CrossRef]
- Bovbjerg, M.L.; Lee, J.; Wolff, R.; Bangs, B.; May, M.A. Pilot study for managing complex chronic care medicaid patients with diabetes using a mobile health application achieves “triple aim” improvement in a primary care setting. Clin. Diabetes 2017, 35, 227–231. [Google Scholar] [CrossRef] [PubMed]
- Whitehead, L.; Seaton, P. The effectiveness of self-management mobile phone and tablet apps in long-term condition management: A systematic review. J. Med. Internet Res. 2016, 18, e97. [Google Scholar] [CrossRef] [PubMed]
- Chomutare, T.; Fernandez-Luque, L.; Årsand, E.; Hartvigsen, G. Features of mobile diabetes applications: Review of the literature and analysis of current applications compared against evidence-based guidelines. J. Med. Internet Res. 2011, 13, e65. [Google Scholar] [CrossRef] [PubMed]
- Goyal, S.; Nunn, C.A.; Rotondi, M.; Couperthwaite, A.B.; Reiser, S.; Simone, A.; Katzman, D.K.; Cafazzo, J.A.; Palmert, M.R. A mobile app for the self-management of type 1 diabetes among adolescents: A randomized controlled trial. JMIR Mhealth Uhealth 2017, 5, e82. [Google Scholar] [CrossRef] [PubMed]
- Lee, K.; Kwon, H.; Lee, B.; Lee, G.; Lee, J.H.; Park, Y.R.; Shin, S.-Y. Effect of self-monitoring on long-term patient Engagement with mobile health applications. PLoS ONE 2018, 13, e0201166. [Google Scholar] [CrossRef]
- Rossi, M.G.; Bigi, S. mHealth for diabetes support: A systematic review of apps available on the italian market. Mhealth 2017, 3, 16. [Google Scholar] [CrossRef][Green Version]
- Mercer, K.; Li, M.; Giangregorio, L.; Burns, C.; Grindrod, K. Behavior change techniques present in wearable activity trackers: A critical analysis. JMIR Mhealth Uhealth 2016, 4, e40. [Google Scholar] [CrossRef]
- Arnhold, M.; Quade, M.; Kirch, W. Mobile applications for diabetics: A systematic review and expert-based usability evaluation considering the special requirements of diabetes patients age 50 years or older. J. Med. Internet Res. 2014, 16, e104. [Google Scholar] [CrossRef] [PubMed]
- Priesterroth, L.; Grammes, J.; Holtz, K.; Reinwarth, A.; Kubiak, T. Gamification and behavior change techniques in diabetes self-management apps. J. Diabetes Sci. Technol. 2019, 13, 954–958. [Google Scholar] [CrossRef]
- Hoppe, C.D.; Cade, J.E.; Carter, M. An evaluation of diabetes targeted apps for android smartphone in relation to behaviour change techniques. J. Hum. Nutr. Diet. 2017, 30, 326–338. [Google Scholar] [CrossRef] [PubMed]
- Silva, B.M.C.; Rodrigues, J.J.P.C.; De la Torre Díez, I.; López-Coronado, M.; Saleem, K. Mobile-health: A review of current state in 2015. J. Biomed. Inform. 2015, 56, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Kim, B.Y.; Lee, J. Smart devices for older adults managing chronic disease: A scoping review. JMIR Mhealth Uhealth 2017, 5, e69. [Google Scholar] [CrossRef]
- Moher, D.; Liberati, A.; Tetzlaff, J.; Altman, D.G. PRISMA group reprint—Preferred reporting items for systematic reviews and meta-analyses: The PRISMA statement. Phys. Ther. 2009, 89, 873–880. [Google Scholar] [CrossRef]
- Bashshur, R.; Shannon, G.; Krupinski, E.; Grigsby, J. The taxonomy of telemedicine. Telemed. e-Health 2011, 17, 484–494. [Google Scholar] [CrossRef]
- Agarwal, S.; LeFevre, A.E.; Lee, J.; L’Engle, K.; Mehl, G.; Sinha, C.; Labrique, A. Guidelines for reporting of health interventions using mobile phones: Mobile health (mHealth) evidence reporting and assessment (mERA) checklist. BMJ 2016, 352, i1174. [Google Scholar] [CrossRef]
- Glasgow, R.E.; Vogt, T.M.; Boles, S.M. Evaluating the public health impact of health promotion interventions: The RE-AIM framework. Am. J. Public Health 1999, 89, 1322–1327. [Google Scholar] [CrossRef] [PubMed]
- Eysenbach, G.; CONSORT-EHEALTH Group. CONSORT-EHEALTH: Improving and standardizing evaluation reports of web-based and mobile health interventions. J. Med. Internet Res. 2011, 13, e126. [Google Scholar] [CrossRef]
- Yu, K.; Wu, S.; Lee, P.-J.; Wu, D.-A.; Hsiao, H.-Y.; Tseng, Y.-C.; Wang, Y.-W.; Cheng, C.-F.; Wang, Y.-H.; Lee, S.-P.; et al. Longitudinal effects of an intergenerational mHealth program for older type 2 diabetes patients in Rural Taiwan. Diabetes Educ. 2020, 46, 206–216. [Google Scholar] [CrossRef] [PubMed]
- Doocy, S.; Paik, K.E.; Lyles, E.; Hei Tam, H.; Fahed, Z.; Winkler, E.; Kontunen, K.; Mkanna, A.; Burnham, G. Guidelines and mHealth to improve quality of hypertension and type 2 diabetes care for vulnerable populations in Lebanon: Longitudinal cohort study. JMIR Mhealth Uhealth 2017, 5, e158. [Google Scholar] [CrossRef] [PubMed]
- Wayne, N.; Ritvo, P. Smartphone-enabled health coach intervention for people with diabetes from a modest socioeconomic strata community: Single-arm longitudinal feasibility study. J. Med. Internet Res. 2014, 16, e149. [Google Scholar] [CrossRef]
- Wayne, N.; Perez, D.F.; Kaplan, D.M.; Ritvo, P. Health coaching reduces HbA1c in type 2 diabetic patients from a lower-socioeconomic status community: A randomized controlled trial. J. Med. Internet Res. 2015, 17, e224. [Google Scholar] [CrossRef] [PubMed]
- Dugas, M.; Crowley, K.; Gao, G.G.; Xu, T.; Agarwal, R.; Kruglanski, A.W.; Steinle, N. Individual differences in regulatory mode moderate the effectiveness of a pilot mHealth trial for diabetes management among older veterans. PLoS ONE 2018, 13, e0192807. [Google Scholar] [CrossRef] [PubMed]
- Baron, J.S.; Hirani, S.; Newman, S.P. A randomised, controlled trial of the effects of a mobile telehealth intervention on clinical and patient-reported outcomes in people with poorly controlled diabetes. J. Telemed. Telecare 2017, 23, 207–216. [Google Scholar] [CrossRef]
- Mora, P.; Buskirk, A.; Lyden, M.; Parkin, C.G.; Borsa, L.; Petersen, B. Use of a novel, remotely connected diabetes management system is associated with increased treatment satisfaction, reduced diabetes distress, and improved glycemic control in individuals with insulin-treated diabetes: First results from the personal diabetes management study. Diabetes Technol. Ther. 2017, 19, 715–722. [Google Scholar]
- Zhou, W.; Chen, M.; Yuan, J.; Sun, Y. Welltang—A smart phone-based diabetes management application—Improves blood glucose control in Chinese people with diabetes. Diabetes Res. Clin. Pract. 2016, 116, 105–110. [Google Scholar] [CrossRef] [PubMed]
- Takenga, C.; Berndt, R.-D.; Musongya, O.; Kitero, J.; Katoke, R.; Molo, K.; Kazingufu, B.; Meni, M.; Vikandy, M.; Takenga, H. An ICT-based diabetes management system tested for health care delivery in the African context. Int. J. Telemed. Appl. 2014, 2014, 437307. [Google Scholar] [CrossRef] [PubMed][Green Version]
- Brath, H.; Morak, J.; Kästenbauer, T.; Modre-Osprian, R.; Strohner-Kästenbauer, H.; Schwarz, M.; Kort, W.; Schreier, G. Mobile health (mHealth) based medication adherence measurement—A pilot trial using electronic blisters in diabetes patients. Br. J. Clin. Pharmacol. 2013, 76, 47–55. [Google Scholar] [CrossRef]
- Prabhakaran, D.; Jha, D.; Prieto-Merino, D.; Roy, A.; Singh, K.; Ajay, V.S.; Jindal, D.; Gupta, P.; Kondal, D.; Goenka, S.; et al. Effectiveness of an mHealth-based electronic decision support system for integrated management of chronic conditions in primary care: The mWellcare cluster-randomized controlled trial. Circulation 2018, 139, 380–391. [Google Scholar] [CrossRef]
- Yoo, H.J.; Park, M.S.; Kim, T.N.; Yang, S.J.; Cho, G.J.; Hwang, T.G.; Baik, S.H.; Choi, D.S.; Park, G.H.; Choi, K.M. A ubiquitous chronic disease care system using cellular phones and the internet. Diabet. Med. 2009, 26, 628–635. [Google Scholar] [CrossRef]
- Bramwell, S.E.; Meyerowitz-Katz, G.; Ferguson, C.; Jayaballa, R.; McLean, M.; Maberly, G. The effect of an mHealth intervention for titration of insulin for type 2 diabetes: A pilot study. Eur. J. Cardiovasc. Nurs. 2020, 19, 386–392. [Google Scholar] [CrossRef]
- Kim, H.-S.; Choi, W.; Baek, E.K.; Kim, Y.A.; Yang, S.J.; Choi, I.Y.; Yoon, K.-H.; Cho, J.-H. Efficacy of the smartphone-based glucose management application stratified by user satisfaction. Diabetes Metab. J. 2014, 38, 204–210. [Google Scholar] [CrossRef]
- Waki, K.; Fujita, H.; Uchimura, Y.; Omae, K.; Aramaki, E.; Kato, S.; Lee, H.; Kobayashi, H.; Kadowaki, T.; Ohe, K. DialBetics: A Novel smartphone-based self-management support system for type 2 diabetes patients. J. Diabetes Sci. Technol. 2014, 8, 209–215. [Google Scholar] [CrossRef]
- Sittig, S.; Wang, J.; Iyengar, S.; Myneni, S.; Franklin, A. Incorporating behavioral trigger messages into a mobile health app for chronic disease management: Randomized clinical feasibility trial in diabetes. JMIR Mhealth Uhealth 2020, 8, e15927. [Google Scholar] [CrossRef]
- Kardas, P.; Lewandowski, K.; Bromuri, S. Type 2 diabetes patients benefit from the COMODITY12 mHealth system: Results of a randomised trial. J. Med. Syst. 2016, 40, 259. [Google Scholar] [CrossRef] [PubMed]
- Karhula, T.; Vuorinen, A.-L.; Rääpysjärvi, K.; Pakanen, M.; Itkonen, P.; Tepponen, M.; Junno, U.-M.; Jokinen, T.; Van Gils, M.; Lähteenmäki, J.; et al. Telemonitoring and mobile phone-based health coaching among finnish diabetic and heart disease patients: Randomized controlled trial. J. Med. Internet Res. 2015, 17, e153. [Google Scholar] [CrossRef]
- Larsen, M.E.; Turner, J.; Farmer, A.; Neil, A.; Tarassenko, L. Telemedicine-supported insulin optimisation in primary care. J. Telemed. Telecare 2010, 16, 433–440. [Google Scholar] [CrossRef] [PubMed]
- Nes, A.A.G.; Van Dulmen, S.; Eide, E.; Finset, A.; Kristjánsdóttir, O.B.; Steen, I.S.; Eide, H. The development and feasibility of a web-based intervention with diaries and situational feedback via smartphone to support self-management in patients with diabetes type 2. Diabetes Res. Clin. Pract. 2012, 97, 385–393. [Google Scholar] [CrossRef] [PubMed]
- Koot, D.; Goh, P.S.C.; Lim, R.S.M.; Tian, Y.; Yau, T.Y.; Tan, N.C.; Finkelstein, E.A. A mobile lifestyle management program (GlycoLeap) for people with type 2 diabetes: Single-arm feasibility study. JMIR Mhealth Uhealth 2019, 7, e12965. [Google Scholar] [CrossRef]
- Orsama, A.-L.; Lähteenmäki, J.; Harno, K.; Kulju, M.; Wintergerst, E.; Schachner, H.; Stenger, P.; Leppänen, J.; Kaijanranta, H.; Salaspuro, V.; et al. Active assistance technology reduces glycosylated hemoglobin and weight in individuals with type 2 diabetes: Results of a theory-based randomized trial. Diabetes Technol. Ther. 2013, 15, 662–669. [Google Scholar] [CrossRef]
- Quinn, C.C.; Clough, S.S.; Minor, J.M.; Lender, D.; Okafor, M.C.; Gruber-Baldini, A. WellDoc mobile diabetes management randomized controlled trial: Change in clinical and behavioral outcomes and patient and physician satisfaction. Diabetes Technol. Ther. 2008, 10, 160–168. [Google Scholar] [CrossRef] [PubMed]
- Turner, J.; Larsen, M.; Tarassenko, L.; Neil, A.; Farmer, A. Implementation of telehealth support for patients with type 2 diabetes using insulin treatment: An exploratory study. Inform. Prim. Care 2009, 17, 47–53. [Google Scholar] [CrossRef] [PubMed]
- Peltz, C.B.; Gratton, G.; Fabiani, M. Age-related changes in electrophysiological and neuropsychological indices of working memory, attention control, and cognitive flexibility. Front. Psychol. 2011, 2, 190. [Google Scholar] [CrossRef]
- Quinn, C.C.; Shardell, M.D.; Terrin, M.L.; Barr, E.A.; Ballew, S.H.; Gruber-Baldini, A.L. Cluster-randomized trial of a mobile phone personalized behavioral intervention for blood glucose control. Diabetes Care 2011, 34, 1934–1942. [Google Scholar] [CrossRef]
- Quinn, C.C.; Sareh, P.L.; Shardell, M.L.; Terrin, M.L.; Barr, E.A.; Gruber-Baldini, A.L. Mobile diabetes intervention for glycemic control: Impact on physician prescribing. J. Diabetes Sci. Technol. 2014, 8, 362–370. [Google Scholar] [CrossRef]
- Quinn, C.C.; Khokhar, B.; Weed, K.; Barr, E.; Gruber-Baldini, A.L. Older adult self-efficacy study of mobile phone diabetes management. Diabetes Technol. Ther. 2015, 17, 455–461. [Google Scholar] [CrossRef]
- Young, H.M.; Miyamoto, S.; Dharmar, M.; Tang-Feldman, Y. Nurse coaching and mobile health compared with usual care to improve diabetes self-efficacy for persons with type 2 diabetes: Randomized controlled trial. JMIR Mhealth Uhealth 2020, 8, e16665. [Google Scholar] [CrossRef]
- Hunt, C.W.; Sanderson, B.K.; Ellison, K.J. Support for diabetes using technology: A pilot study to improve self-management. Medsurg Nurs. 2014, 23, 231–237. [Google Scholar]
- Kim, E.K.; Kwak, S.H.; Baek, S.; Lee, S.L.; Jang, H.C.; Park, K.S.; Cho, Y.M. Feasibility of a patient-centered, smartphone-based, diabetes care system: A pilot study. Diabetes Metab. J. 2016, 40, 192–201. [Google Scholar] [CrossRef]
- Steinert, A.; Haesner, M.; Steinhagen-Thiessen, E. [App-based self-monitoring in type 2 diabetes]. Z. Gerontol. Geriatr. 2017, 50, 516–523. [Google Scholar] [CrossRef]
- Sun, C.; Sun, L.; Xi, S.; Zhang, H.; Wang, H.; Feng, Y.; Deng, Y.; Wang, H.; Xiao, X.; Wang, G.; et al. Mobile phone-based telemedicine practice in older chinese patients with type 2 diabetes mellitus: Randomized controlled trial. JMIR Mhealth Uhealth 2019, 7, e10664. [Google Scholar] [CrossRef]
- Holmen, H.; Torbjørnsen, A.; Wahl, A.K.; Jenum, A.K.; Småstuen, M.C.; Arsand, E.; Ribu, L. A mobile health intervention for self-management and lifestyle change for persons with type 2 diabetes, part 2: One-year results from the norwegian randomized controlled trial RENEWING HEALTH. JMIR Mhealth Uhealth 2014, 2, e57. [Google Scholar] [CrossRef] [PubMed]
- Torbjørnsen, A.; Jenum, A.K.; Småstuen, M.C.; Arsand, E.; Holmen, H.; Wahl, A.K.; Ribu, L. A low-intensity mobile health intervention with and without health counseling for persons with type 2 diabetes, part 1: Baseline and short-term results from a randomized controlled trial in the norwegian part of RENEWING HEALTH. JMIR Mhealth Uhealth 2014, 2, e52. [Google Scholar] [CrossRef] [PubMed]
- Alanzi, T.; Alanazi, N.R.; Istepanian, R.; Philip, N. Evaluation of the effectiveness of mobile diabetes management system with social networking and cognitive behavioural therapy (CBT) for T2D. Mhealth 2018, 4, 35. [Google Scholar] [CrossRef] [PubMed]
- Li, J.; Sun, L.; Wang, Y.; Guo, L.; Li, D.; Liu, C.; Sun, N.; Xu, Z.; Li, S.; Jiang, Y.; et al. A mobile-based intervention for glycemic control in patients with type 2 diabetes: Retrospective, propensity score-matched cohort study. JMIR Mhealth Uhealth 2020, 8, e15390. [Google Scholar] [CrossRef]
- Quinn, C.C.; Shardell, M.D.; Terrin, M.L.; Barr, E.A.; Park, D.; Shaikh, F.; Guralnik, J.M.; Gruber-Baldini, A.L. Mobile diabetes intervention for glycemic control in 45- to 64-year-old persons with type 2 diabetes. J. Appl. Gerontol. 2016, 35, 227–243. [Google Scholar] [CrossRef]
- Kardas, P.; Lewandowski, K. Type 2 diabetes patients assessment of the COMODITY12 mHealth system. EAI Endorsed Trans Pervasive Health Technol. 2015, 1. [Google Scholar]
- Yu, K.; Wu, S.; Liu, R.; Chi, I. Mobile technology adoption for type 2 diabetes management among Chinese and Hispanic immi-grants: A qualitative pilot study. In APHA’s 2020 VIRTUAL Annual Meeting and Expo, 24–28 October 2020; American Public Health Association: Washington, DC, USA, 2020. [Google Scholar]
- Michie, S.; Richardson, M.; Johnston, M.; Abraham, C.; Francis, J.; Hardeman, W.; Eccles, M.P.; Cane, J.; Wood, C.E. The behavior change technique taxonomy (v1) of 93 hierarchically clustered techniques: Building an international consensus for the reporting of behavior change interventions. Ann. Behav. Med. 2013, 46, 81–95. [Google Scholar] [CrossRef]
- Ng, A.H.; Crowe, T.C.; Ball, K.; Rasmussen, B. A mHealth support program for australian young adults with type 1 diabetes: A mixed methods study. Digit. Health 2019, 5, 2055207619882179. [Google Scholar] [CrossRef]
- Lygidakis, C.; Uwizihiwe, J.P.; Kallestrup, P.; Bia, M.; Condo, J.; Vögele, C. Community- and mHealth-based integrated management of diabetes in primary healthcare in rwanda (D2Rwanda): The protocol of a mixed-methods study including a cluster randomised controlled trial. BMJ Open 2019, 9, e028427. [Google Scholar] [CrossRef]
- Herrera, A.P.; Snipes, S.A.; King, D.W.; Torres-Vigil, I.; Goldberg, D.S.; Weinberg, A.D. Disparate inclusion of older adults in clinical trials: Priorities and opportunities for policy and practice change. Am. J. Public Health 2010, 100 (Suppl.1), S105–S112. [Google Scholar] [CrossRef]
- Cajita, M.I.; Hodgson, N.A.; Lam, K.W.; Yoo, S.; Han, H.-R. Facilitators of and barriers to mHealth adoption in older adults with heart failure. Comput. Inform. Nurs. 2018, 36, 376–382. [Google Scholar] [CrossRef] [PubMed]
- Kruse, C.S.; Mileski, M.; Moreno, J. Mobile health solutions for the aging population: A systematic narrative analysis. J. Telemed. Telecare 2017, 23, 439–451. [Google Scholar] [CrossRef] [PubMed]
- Holzinger, A.; Searle, G.; Nischelwitzer, A. On some aspects of improving mobile applications for the elderly. Lect. Notes Comput. Sci. 2007, 923–932. [Google Scholar]
- Eland-de Kok, P.; Van Os-Medendorp, H.; Vergouwe-Meijer, A.; Bruijnzeel-Koomen, C.; Ros, W. A systematic review of the effects of e-health on chronically ill patients. J. Clin. Nurs. 2011, 20, 2997–3010. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.H. Educational attainment moderates the associations of diabetes education with health outcomes. Int. J. Nurs. Pract. 2016, 22, 444–450. [Google Scholar] [CrossRef]
- Sarid, O.; Berger, R.; Guez, J. Reduced HbA1c levels in type 2 diabetes patients: An interaction between a pedagogical format for students and psycho-educational intervention for patients. Diabetes Metab. Syndr. 2019, 13, 2280–2284. [Google Scholar] [CrossRef] [PubMed]
- Siminerio, L.; Hamm, M.; Kanter, J.; Cameron, F. de A.; Krall, J. A diabetes education model in primary care: Provider and staff perspectives. Diabetes Educ. 2019, 45, 498–506. [Google Scholar] [CrossRef] [PubMed]
- Nilsen, W.; Kumar, S.; Shar, A.; Varoquiers, C.; Wiley, T.; Riley, W.T.; Pavel, M.; Atienza, A.A. Advancing the science of mHealth. J. Health Commun. 2012, 17, 5–10. [Google Scholar] [CrossRef] [PubMed]
- Van Vugt, M.; De Wit, M.; Cleijne, W.H.J.J.; Snoek, F.J. Use of behavioral change techniques in web-based self-management programs for type 2 diabetes patients: Systematic review. J. Med. Internet Res. 2013, 15, e279. [Google Scholar] [CrossRef]
- Caperon, L.; Sykes-Muskett, B.; Clancy, F.; Newell, J.; King, R.; Prestwich, A. How effective are interventions in improving dietary behaviour in low- and middle-income countries? A systematic review and meta-analysis. Health Psychol. Rev. 2018, 12, 312–331. [Google Scholar] [CrossRef]
- Fredrix, M.; McSharry, J.; Flannery, C.; Dinneen, S.; Byrne, M. Goal-setting in diabetes self-management: A systematic review and meta-analysis examining content and effectiveness of goal-setting interventions. Psychol. Health 2018, 33, 955–977. [Google Scholar] [CrossRef] [PubMed]
- O’Brien, N.; McDonald, S.; Araújo-Soares, V.; Lara, J.; Errington, L.; Godfrey, A.; Meyer, T.D.; Rochester, L.; Mathers, J.C.; White, M.; et al. The features of interventions associated with long-term effectiveness of physical activity interventions in adults aged 55-70 years: A systematic review and meta-analysis. Health Psychol. Rev. 2015, 9, 417–433. [Google Scholar] [CrossRef]
- Castellano-Tejedor, C.; Moreno, J.; Knittle, K.; Nurmi, J.; Ginchev, T.; Parramón, G.; Ciudin, A.; Ramos-Quiroga, J.A.; Lusilla-Palacios, P. Assessing the user experience and usability of the PRECIOUS system: A randomized controlled trial in obese patients. Inform. Health Soc. Care 2020, 45, 410–427. [Google Scholar] [CrossRef]
- Castellano-Tejedor, C.; Moreno, J.; Ciudin, A.; Parramón, G.; Lusilla-Palacios, P. PREventive care infrastructure based on ubiquitous sensing (PRECIOUS): A study protocol. JMIR Res. Protoc. 2017, 6, e105. [Google Scholar] [CrossRef] [PubMed]
- Nurmi, J.; Knittle, K.; Ginchev, T.; Khattak, F.; Helf, C.; Zwickl, P.; Castellano-Tejedor, C.; Lusilla-Palacios, P.; Costa-Requena, J.; Ravaja, N.; et al. Engaging users in the behavior change process with digitalized motivational interviewing and gamification: Development and feasibility testing of the precious app. JMIR Mhealth Uhealth 2020, 8, e12884. [Google Scholar] [CrossRef] [PubMed]
- Edwards, E.A.; Lumsden, J.; Rivas, C.; Steed, L.; Edwards, L.A.; Thiyagarajan, A.; Sohanpal, R.; Caton, H.; Griffiths, C.J.; Munafò, M.R.; et al. Gamification for health promotion: Systematic review of behaviour change techniques in smartphone apps. BMJ Open 2016, 6, e012447. [Google Scholar] [CrossRef] [PubMed]
- Mayberry, L.S.; Lyles, C.R.; Oldenburg, B.; Osborn, C.Y.; Parks, M.; Peek, M.E. mHealth interventions for disadvantaged and vulnerable people with type 2 diabetes. Curr. Diab. Rep. 2019, 19, 148. [Google Scholar] [CrossRef] [PubMed]
- Geboers, B.; Uiters, E.; Reijneveld, S.A.; Jansen, C.J.M.; Almansa, J.; Nooyens, A.C.J.; Verschuren, W.M.M.; De Winter, A.F.; Picavet, H.S.J. Health literacy among older adults is associated with their 10-years’ cognitive functioning and decline—The doetinchem cohort study. BMC Geriatr. 2018, 18, 77. [Google Scholar] [CrossRef]
- Okan, O.; Bauer, U. International Handbook of Health Literacy: Research, Practice and Policy across the Life-Span; Policy Press: Bristol, UK, 2019; ISBN 9781447344513. [Google Scholar]


{kind=link}
| Search Number | PubMed Search String |
|---|---|
| 1 | (((diabet*[Title/Abstract]) AND adherence[Title/Abstract]) AND education*[Title/Abstract]) AND older adults[Title/Abstract] |
| 2 | (((diabet*[Title/Abstract]) AND adherence[Title/Abstract]) AND management*[Title/Abstract]) AND elderly[Title/Abstract] |
| 3 | (((diabet*[Title/Abstract]) AND adherence[Title/Abstract]) AND self*[Title/Abstract]) AND elderly[Title/Abstract] |
| 4 | (((diabet*[Title/Abstract]) AND adherence[Title/Abstract]) AND mHealth[Title/Abstract]) AND elderly[Title/Abstract] |
| 5 | (((diabet*[Title/Abstract]) AND e-blister[Title/Abstract]) |
| 6 | (((diabet*[Title/Abstract]) AND mhealth[Title/Abstract]) AND older adults[Title/Abstract] |
| Search Number | PsycInfo Search String |
| 1 | diabetes AND adherence AND education AND older adults |
| 2 | diabetes AND adherence AND management AND elderly |
| 3 | diabetes AND adherence AND self AND elderly |
| 4 | diabetes AND adherence AND mHealth AND elderly |
| 5 | diabetes AND mHealth AND older adults |
| 6 | diabetes AND mHealth OR pill dispenser |
| Author(s) & Year of Publication | mHealth Solution | Psychological Framework | Modules/Main Features of the mHealth Solution | Specific Techniques (Based on Michie et al. (2013) [79] |
|---|---|---|---|---|
| Alanzi et al., 2018 [74] | SANAD System (app + web portal + peripheral device) | CBT | Three modules: (1) glucose management, (2) social network (educational), and (3) behavior change module. | Psychoeducation, Tailored feedback from medical staff on outcome behavior, Automatic feedback on behavior, Behavior substitution, Rehearsal, Self-monitoring of outcome behavior, Social support general, practical, emotional |
| Baron et al., 2016 [44] | Mobile Telehealth (App + web portal + peripheral devices) | CBT | Patients received feedback from mobile SW (colored graphics) and nurses, supporting out-of-range clinical readings, insulin titration, and education calls on lifestyle changes and T2DM medication adherence. | Psychoeducation, Tailored feedback from medical staff on outcome behavior, Automatic feedback on behavior, Behavior substitution, Rehearsal, Self-monitoring of outcome behavior |
| Bovbjerg et al., 2017 [22] | mHealth app | n.e. | Technical training and support providing interactive biometric data and alerts. | Automatic feedback on behavior, Self-monitoring of outcome behavior, Reminders |
| Bramwell et al., 2019 [51] | Health2Sync (app) | n.e. | Standard insulin titration advice from a diabetes educator. | Psychoeducation, Self-monitoring of outcome behavior |
| Brath et al., 2013 [48] | Medication Adherence measurement system (mAms) (app + web + e-blisters) | n.e. | Calls from a coordinator to patients with poor adherence to increase adherence and motivation | Psychoeducation, Tailored feedback on outcome behavior, Self-monitoring of outcome behavior, Pharmacological support |
| Doocy et al., 2017 [40] | Sana Telehealth Platform (app) | n.e. | Personally controlled health record and informational printouts for patients on prescriptions and lifestyle behaviors. | Psychoeducation, Tailored feedback from medical staff on outcome behavior, Self-monitoring of outcome behavior |
| Dugas et al., 2018 [43] | DiaSocial app (app + Fitbit one) | CBT with gamification principles | Four conditions with different features embedded in the app: (1) individual user, (2) user + clinician, (3) user + peers (other users), (4) user + clinician + peers. | Psychoeducation, Rewards, Goal-setting, Behavioral rehearsal, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on behavior, Social support general, practical, emotional, Reminders |
| Holmen et al., 2014 [72] | Few touch app (FTA) (device + app) | CBT combined with the transtheoretical model of stages of change & the problem- solving model | Two conditions: (1) the FTA system provided the user with a diabetes diary app designed to increase self-management through awareness, an overview of relevant factors, and symbols such as smiling faces and color codes in the app. (2) FTA + health counseling (as a booster for the first 4 months) | Psychoeducation, Self-monitoring of outcome behavior, Automatic feedback on behavior MI techniques, Problem-solving, Counseling |
| Hunt et al., 2014 [68] | Diabetes Buddy® (Apple iPad app) | SDT | Self-management behaviors tracked and reviewed through a visual representation of how day-to-day activities affect outcomes (monitoring BGL diet, exercise, medication). | Psychoeducation, Self-monitoring of outcome behavior, Automatic feedback on behavior MI techniques |
| Kardas et al., 2016 [55] | COMMODITY12 system | n.e. | Tracking of T2DM self-management | Self-monitoring of outcome behavior, Automatic feedback on behavior |
| Karhula et al., 2015 [56] | Mobile phone-based health coaching program, supported by the Remote Patient Monitoring system (app + peripheral devices) | CBT SDT | Health coaches called patients every 4 to 6 weeks, and patients were encouraged to self-monitor their weight, BP, BGL, and steps once per week. | Action planning, Goal setting, MI techniques, Self-monitoring of outcome behavior, Automatic feedback on behavior, Tailored feedback from medical staff on outcome behavior (health coach), Reminders |
| Kim et al., 2014 [52] | Mobile Smartcare, version 1.0.7 | n.e. | Warning messages, clinician feedback, and tailored recommendations to the patient an average of once per week (exercise & diet) | Psychoeducation, Self-monitoring of outcome behavior, Automatic feedback on behavior, Tailored feedback from medical staff on outcome behavior, MI techniques, Reminders |
| Kim et al., 2016 [69] | Patient-centered smartphone-based diabetes care system (PSDCS) (app + web + peripheral devices) | n.e. | Four modules: (1) glucose (feedback, alarm messages, recommendations), (2) diet (records of daily dietary intake, total calories, and nutrients intake) (3) physical activity (tracks activity and energy expenditure calculator, exercise video-clips), and (4) Social Network System (patients post their thoughts, opinions, and tips for diabetes self-care). PSDCS also contained diabetes self-management educational material about managing various diabetes-related conditions and specific situations. | Psychoeducation, Goal setting, Self-monitoring of outcome behavior, Automatic feedback on behavior, Tailored feedback from medical staff on outcome behavior, Social support general, practical, emotional |
| Koot et al., 2019 [59] | Glyco app (app + peripheral devices) | CBT | Lifestyle management program: lessons about self-management and BG monitoring with a health coaching feature. | Psychoeducation (Health coach), MI techniques, Automatic feedback on behavior |
| Larsen et al., 2010 [57] | App + peripheral devices | n.e. | Electronic diary with BG self-management features. The nurse provided general advice, motivation and assisted with technical problems. | Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, MI techniques |
| Li et al., 2020 [75] | App + web platform + data sharing cloud platform + peripheral devices | n.e. | Automatic and clinicians’ health advice (calls) for T2DM self-management (hypoglycemia and abnormal BGL, medication, diet, exercise). Patients record (pictures, descriptions) their meals and get clinicians’ feedback. Patients also have access to educational information (articles, videos, and attractive posters). | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, MI techniques, Problem-solving |
| Mora et al., 2017 [45] | Accu-Chek Connect diabetes management system (app + web portal + peripheral device) | n.e. | System use, treatment changes, and recommendations (adjustments in medication, lifestyle/behavioral counseling, address skill deficit, and address nonadherence) through calls and visits. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior |
| Nes et al., 2012 [58] | Few Touch Application (FTA) (app + web-based) | ACT CBT | Participants recorded their health behaviors and FBG daily on a web-based diary. A therapist had immediate access to submitted diaries and used the situational information to formulate personalized feedback. Patients have access to audio files with mindfulness and relaxation exercises. | Psychoeducation, Goal setting, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, Stress regulation/Relaxation techniques |
| Orsama et al., 2013 [60] | Monica app (app + peripheral devices) | CBT | Diabetes lifestyle self-management promotion program involving remote patient reporting and automated feedback. | Psychoeducation, Goal setting, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques, Problem-solving |
| Prabhakaran et al., 2018 [49] | mWellcare (app) | n.e. | Self-management DSR generated based on patients collected data. The nurse provides lifestyle advice using prompts of the DSR. SMS service reminders (to take medication and attend follow-up visits). | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior Automatic feedback on outcome behavior, Reminders |
| Quinn et al., 2008 [61] | WellDoc’s Diabetes Management SW (app) | n.e. | Patients received personalized real-time feedback messages regarding BG readings. When problematic readings are detected, an email with specific educational material is sent. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior |
| Quinn et al., 2011 [64] | Mobile diabetes SW (app + web portal) | CBT | Three interventions: (1) Coach (2) Coach PCP Portal (3) Coach PCP Portal with CPDS self-management patient coaching system and provider decision support. Patients received automated, real-time educational, behavioral, and motivational messaging in response to individually analyzed data. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques |
| Quinn et al., 2016 [76] | Mobile diabetes SW (app + web portal) | CBT | Automated, real-time messages that were educational, behavioral, motivational, and specific to the data. The diabetes educators could supplement it with messages based on longitudinal diabetes self-care data trends. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques |
| Quinn et al., 2014 [65] | Mobile diabetes SW (app + web portal) | CBT | The coaching system involved patients using mobile phones to record information about their diabetes self-management. Patients received real-time (automatic) and personalized coaching feedback consistent with their treatment plans. Physicians could review patient-recorded data accessible through the provider Internet portal and received quarterly facsimile reports, including diabetes treatment recommendations. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques |
| Quinn et al., 2015 [66] | WellDoc’s Diabetes Management SW (app) | CBT | Patients enter diabetes self-care healthy data, and the system sends automated messages in addition to personalized messages to a web portal containing educational and motivational elements. The web portal also included health records that patients were encouraged to update (laboratory values, eye examinations, foot screenings, results from provider visits), a learning library, and a historical logbook. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques |
| Sittig et al., 2020 [54] | CapABILITY (app) Interactive Health Communication Application (IHCA) | Social Cognitive Theory (SCT) focused on self-efficacy. Fogg Behavior Model (FBM) | Patients interact and receive spark and facilitators educational messages (media and text) about diet, exercise, and self-management (e.g., medication adherence, BGL). | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, Reminders Social support |
| Steinert et al., 2017 [70] | My Therapy (app) | n.e. | Patients transfer self-management data. The app acts as a reminder of taking medication, measurements, or physical activity. | Self-monitoring of outcome behavior, Reminders |
| Sun et al., 2019 [71] | mHealth management app (app + medical server + peripheral devices) | n.e. | Patients uploaded the glucometer data to the app transmitted to the medical server. The medical team sent medical advice and reminders to monitor their BG by message or telephonically. The dietitian received daily dietary records and once per month sent nutritional recommendations. Patients sent information about physical activity and were provided guidance related to aerobic and resistance-based exercises. | Psychoeducation, Reminders, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior. |
| Takenga et al., 2014 [47] | Mobil Diab System (web portals + app + peripheral device) | n.e. | Patients enter diabetes-related data, received in real-time by medical care providers. Therapy plans, instructions, and recommendations sent by the doctor from the doctor portal are received directly in the app. Patients without smartphones can still get these doctors’ feedback in the protected patients’ portal through their email addresses or SMS. Doctors receive messages from their patients directly in the web portal. An SMS is automatically generated and sent to the treating physician for emergency cases and gives direct instructions to the patient. | Psychoeducation, Goal setting, Planning, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior |
| Torbjornsen et al., 2014 [73] | The Few Touch Application (FTA) diabetes diary with or without health counseling(app + peripheral devices) | CBT (The Transtheoretical Model + The Problem Solving Model) | Five components for data management: (1) BGL, (2) food habits, (3) physical activity, (4) personal goal-setting system, and (5) general diabetes information look-up system. Patients receive calls from nurses, and they can contact via text messages. | Psychoeducation, Goal setting, Planning, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques, Problem-solving, Health counseling |
| Turner et al., 2009 [62] | t+ Diabetes app (app + peripheral devices) | n.e. | Provides real-time data transmission and feedback to patients on their mobile phone through (1) transmission of blood glucose test results and real-time feedback of trends to the mobile phone; (2) an electronic patient diary with the facility to record insulin doses; and (3) a facility to transmit blood pressure results and weight. Immediate feedback is delivered with summaries and charts to make self-management decisions. Nurses and clinicians send automated alerts and reminders. Nurses encourage patients to follow insulin titration recommendations, advised by the GP. | Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, Psychoeducation, Reminders |
| Waki et al., 2014 [53] | DialBetics System (app + peripheral devices) | n.e. | Patients measure their health data, and if readings are abnormal, these are reported to a physician that interacts with the patient. If reading is abnormal or missed, the medical staff can email the patient to measure their data and involve the specialists and experts if their help was required. The participants can contact the nurse by smartphone or email for equipment failures, technical questions, or in response to alerts. For inquiries related to their health status, they consult their GP. Patients send voice/text messages about behaviors and receive immediate advice on lifestyle modification. Patients can view their measurement data and graphic outputs of their diet and exercise history. | Psychoeducation, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques |
| Wayne & Ritvo, 2014 [41] | Connected Health and Wellness Platform (CHWP) Health Coach app 1.0 version | n.e. | The app tracks health behaviors and self-monitors health data. Wellness plans, collaboratively created in multiple interactions focused on exercise instruction and reviews of electronic monitoring entries. The program prompts to engage in health behaviors and reports on satiety levels. | Psychoeducation, Goal setting, Self-monitoring of outcome behavior, Behavior substitution rehearsal, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, Reminders |
| Wayne et al., 2015 [42] | Connected Wellness Platform (CWP) (app) | CBT | Platform supported patients in health-related goal setting and progress monitoring. Participants could track key metrics, including diabetes self-care, health data, and mood. They could communicate with their health coach at any time via messaging, scheduled phone contact, and in-person meetings. Based on patient goals, clinicians guide healthy lifestyle choices while providing support when clients diverge from intended health goals and routines. All attended weekly team meetings to discuss behavior theory applications in specific strategies for each participant. Intervention and control group assisted an exercise education program that featured exercise prescription, monitoring, and adherence support. | Psychoeducation, Goal setting, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques, Reminders |
| Yoo et al., 2009 [50] | The Ubiquitous Chronic Disease Care (UCDC) system (web Portal + peripheral devices) | n.e. | Participants received SMS and reminders concerning practice and recording different behaviors and disease self-management. Immediate feedback, messages of encouragement, and recommendations (automatic and from physicians) are received regularly and displayed on the website. | Psychoeducation, Goal setting, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques, Reminders |
| Young et al., 2020 [67] | MyFitnessPal mobile app Health Record (app + peripheral devices + connectors + Health Record system) | CBT | The tracking device generated real-time information about healthy data. Participants can log and track nutritional consumption in the mobile app. In-person or telephonic technical support is available. Participants, primary care providers, and nurse health coaches view trends on their smartphones or computers. | Goal setting, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques |
| Yu et al., 2020 [39] | Intergenerational Mobile Technology Opportunities Program (IMTOP) (app + web database) | n.e. | Participants can record their health data, medication adherence and mood. Recorded data is transmitted to the web-based database. | Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior |
| Zhou et al., 2016 [46] | Welltang app (app + peripheral device) | n.e. | A virtual educator for diabetes and a virtual endocrinologist for clinicians, facilitating the integration of diabetes care among existing resources. Patients-clinician communication comprised patients receiving advice from the study team, usually within the day based on their entered questions (BGL, target goals, individualized medication regimens). The database also triggers alerts for missed readings. Patients received an electronic action plan per month as pre-visit summaries for physician office visits. | Action planning, Goal setting, Self-monitoring of outcome behavior, Tailored feedback from medical staff on outcome behavior, Automatic feedback on outcome behavior, MI techniques, Reminders |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Vázquez-de Sebastián, J.; Ciudin, A.; Castellano-Tejedor, C. Analysis of Effectiveness and Psychological Techniques Implemented in mHealth Solutions for Middle-Aged and Elderly Adults with Type 2 Diabetes: A Narrative Review of the Literature. J. Clin. Med. 2021, 10, 2701. https://doi.org/10.3390/jcm10122701
Vázquez-de Sebastián J, Ciudin A, Castellano-Tejedor C. Analysis of Effectiveness and Psychological Techniques Implemented in mHealth Solutions for Middle-Aged and Elderly Adults with Type 2 Diabetes: A Narrative Review of the Literature. Journal of Clinical Medicine. 2021; 10(12):2701. https://doi.org/10.3390/jcm10122701
Chicago/Turabian StyleVázquez-de Sebastián, Julia, Andreea Ciudin, and Carmina Castellano-Tejedor. 2021. "Analysis of Effectiveness and Psychological Techniques Implemented in mHealth Solutions for Middle-Aged and Elderly Adults with Type 2 Diabetes: A Narrative Review of the Literature" Journal of Clinical Medicine 10, no. 12: 2701. https://doi.org/10.3390/jcm10122701
APA StyleVázquez-de Sebastián, J., Ciudin, A., & Castellano-Tejedor, C. (2021). Analysis of Effectiveness and Psychological Techniques Implemented in mHealth Solutions for Middle-Aged and Elderly Adults with Type 2 Diabetes: A Narrative Review of the Literature. Journal of Clinical Medicine, 10(12), 2701. https://doi.org/10.3390/jcm10122701