
Comparison of Effectiveness Using Different Dual Bronchodilator Agents in Chronic Obstructive Pulmonary Disease Treatment

Abstract
1. Introduction
2. Methods
2.1. Study Objectives
2.2. Evaluation of Therapeutic Effects
2.3. Statistical Analysis
3. Results
4. Discussion
5. Conclusions
Author Contributions
Funding
Institutional Review Board Statement
Informed Consent Statement
Data Availability Statement
Conflicts of Interest
References
- Chen, J.C.; Mannino, D.M. Worldwide epidemiology of chronic obstructive pulmonary disease. Curr. Opin. Pulm. Med. 1999, 5, 93–99. [Google Scholar] [CrossRef]
- Murray, C.J.; Lopez, A.D. Alternative projections of mortality and disability by cause 1990–2020: Global Burden of Disease Study. Lancet 1997, 349, 1498–1504. [Google Scholar] [CrossRef]
- Ko, F.W.S.; Hui, D.; Lai, C.K.W. Worldwide burden of COPD in high- and low-income countries. Part III. Asia-Pacific studies. Int. J. Tuberc. Lung Dis. 2008, 12, 713–717. [Google Scholar] [PubMed]
- Cheng, S.-L.; Chan, M.-C.; Wang, C.-C.; Lin, C.-H.; Wang, H.-C.; Hsu, J.-Y.; Hang, L.-W.; Chang, C.-J.; Perng, D.-W.; Yu, C.-Y. COPD in Taiwan: A National Epidemiology Survey. Int. J. Chron. Obstruct. Pulm. Dis. 2015, 10, 2459–2467. [Google Scholar] [CrossRef]
- Lim, S.; Lam, D.C.-L.; Muttalif, A.R.; Yunus, F.; Wongtim, S.; Lan, L.T.T.; Shetty, V.; Chu, R.; Zheng, J.; Perng, D.-W.; et al. Impact of chronic obstructive pulmonary disease (COPD) in the Asia-Pacific region: The EPIC Asia population-based survey. Asia Pac. Fam. Med. 2015, 14, 4. [Google Scholar] [CrossRef]
- Kuo, L.-C.; Yang, P.-C.; Kuo, S.-H. Trends in the mortality of chronic obstructive pulmonary disease in Taiwan, 1981–2002. J. Formos. Med. Assoc. 2005, 104, 89–93. [Google Scholar]
- Barrecheguren, M.; Monteagudo, M.; Ferrer, J.; Borrell, E.; Llor, C.; Esquinas, C.; Miravitlles, M. Treatment patterns in COPD patients newly diagnosed in primary care. A population-based study. Respir. Med. 2016, 111, 47–53. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Banerji, D.; Chapman, K.R.; Vestbo, J.; Roche, N.; Ayers, R.T.; Thach, C.; Fogel, R.; Patalano, F.; Vogelmeier, C.F. Indacaterol–Glycopyrronium versus Salmeterol–Fluticasone for COPD. N. Engl. J. Med. 2016, 374, 2222–2234. [Google Scholar] [CrossRef]
- Vogelmeier, C.F.; Criner, G.J.; Martinez, F.J.; Anzueto, A.; Barnes, P.J.; Bourbeau, J.; Celli, B.R.; Chen, R.; Decramer, M.; Fabbri, L.M.; et al. Global Strategy for the Diagnosis, Management, and Prevention of Chronic Obstructive Lung Disease 2017 Report. GOLD Executive Summary. Am. J. Respir. Crit. Care Med. 2017, 195, 557–582. [Google Scholar] [CrossRef]
- Siler, T.M.; Donald, A.C.; O’Dell, D.; Church, A.; Fahy, W.A. A randomized, parallel-group study to evaluate the efficacy of umeclidinium/vilanterol 62.5/25 µg on health-related quality of life in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 971–979. [Google Scholar] [CrossRef][Green Version]
- Calverley, P.M.A.; Anzueto, A.R.; Carter, K.; Grönke, L.; Hallmann, C.; Jenkins, C.; Wedzicha, J.; Rabe, K.F. Tiotropium and olodaterol in the prevention of chronic obstructive pulmonary disease exacerbations (DYNAGITO): A double-blind, randomised, parallel-group, active-controlled trial. Lancet Respir. Med. 2018, 6, 337–344. [Google Scholar] [CrossRef]
- Blair, H.A. Tiotropium/Olodaterol: A Review in COPD. Drugs 2019, 79, 997–1008. [Google Scholar] [CrossRef]
- Dhillon, S. Tiotropium/Olodaterol: A Review in COPD. Drugs 2015, 76, 135–146. [Google Scholar] [CrossRef]
- Ichinose, M.; Taniguchi, H.; Takizawa, A.; Grönke, L.; Loaiza, L.; Voß, F.; Zhao, Y.; Fukuchi, Y. The efficacy and safety of combined tiotropium and olodaterol via the Respimat® inhaler in patients with COPD: Results from the Japanese sub-population of the Tonado® studies. Int. J. Chronic Obstr. Pulm. Dis. 2016, 11, 2017–2027. [Google Scholar] [CrossRef] [PubMed]
- Ichinose, M.; Nishimura, M.; Akimoto, M.; Kurotori, Y.; Zhao, Y.; de la Hoz, A.; Mishima, M. Tiotropium/olodaterol versus tiotropium in Japanese patients with COPD: Results from the DYNAGITO study. Int. J. Chronic Obstr. Pulm. Dis. 2018, 13, 2147–2156. [Google Scholar] [CrossRef] [PubMed]
- Vogelmeier, C.; Hederer, B.; Glaab, T.; Schmidt, H.; Molken, M.R.-V.; Beeh, K.M.; Rabe, K.F.; Fabbri, L.M. Tiotropium versus Salmeterol for the Prevention of Exacerbations of COPD. N. Engl. J. Med. 2011, 364, 1093–1103. [Google Scholar] [CrossRef]
- Decramer, M.L.; Chapman, K.R.; Dahl, R.; Frith, P.; Devouassoux, G.; Fritscher, C.; Cameron, R.; Shoaib, M.; Lawrence, D.; Young, D.; et al. Once-daily indacaterol versus tiotropium for patients with severe chronic obstructive pulmonary disease (INVIGORATE): A randomised, blinded, parallel-group study. Lancet Respir. Med. 2013, 2013 7, 524–533. [Google Scholar] [CrossRef]
- Koch, A.; Watz, H.; Maleki-Yazdi, M.R.; Bothner, U.; Tetzlaff, K.; Voß, F.; McGarvey, L. Comprehensive assessment of the safety of olodaterol 5 µg in the Respimat® device for maintenance treatment of COPD: Comparison with the long-acting β2-agonist formoterol. NPJ Prim. Care Respir. Med. 2017, 27, 60. [Google Scholar] [CrossRef] [PubMed]
- Joos, G.F.; Aumann, J.-L.; Coeck, C.; Korducki, L.; Hamilton, A.L.; Kunz, C.; Aalbers, R. A randomised, double-blind, four-way, crossover trial comparing the 24-h FEV1 profile for once-daily versus twice-daily treatment with olodaterol, a novel long-acting β2-agonist, in patients with chronic obstructive pulmonary disease. Respir. Med. 2015, 109, 606–615. [Google Scholar] [CrossRef][Green Version]
- Wedzicha, J.A.; Calverley, P.M.A.; Seemungal, T.A.; Hagan, G.; Ansari, Z.; Stockley, R.A. The Prevention of Chronic Obstructive Pulmonary Disease Exacerbations by Salmeterol/Fluticasone Propionate or Tiotropium Bromide. Am. J. Respir. Crit. Care Med. 2008, 177, 19–26. [Google Scholar] [CrossRef]
- Wedzicha, J.A.; Decramer, M.; Ficker, J.H.; Niewoehner, D.E.; Sandström, T.; Taylor, A.F.; D’Andrea, P.; Arrasate, C.; Chen, H.; Banerji, D. Analysis of chronic obstructive pulmonary disease exacerbations with the dual bronchodilator QVA149 compared with glycopyrronium and tiotropium (SPARK): A randomised, double-blind, parallel-group study. Lancet Respir. Med. 2013, 1, 199–209. [Google Scholar] [CrossRef]
- Decramer, M.; Anzueto, A.; Kerwin, E.; Kaelin, T.; Richard, N.; Crater, G.; Tabberer, M.; Harris, S.; Church, A. Efficacy and safety of umeclidinium plus vilanterol versus tiotropium, vilanterol, or umeclidinium monotherapies over 24 weeks in patients with chronic obstructive pulmonary disease: Results from two multicentre, blinded, randomised controlled trials. Lancet Respir. Med. 2014, 2, 472–486. [Google Scholar] [CrossRef]
- Feldman, G.J.; Bernstein, J.A.; Hamilton, A.; Nivens, M.C.; Korducki, L.; LaForce, C. The 24-h FEV1 time profile of olodaterol once daily via Respimat® and formoterol twice daily via Aerolizer® in patients with GOLD 2–4 COPD: Results from two 6-week crossover studies. Springerplus 2014, 3, 419. [Google Scholar] [CrossRef] [PubMed]
- Ferguson, G.; Feldman, G.; Hofbauer, P.; Hamilton, A.; Allen, L.; Korducki, L.; Sachs, P. Efficacy and safety of olodaterol once daily delivered via Respimat® in patients with GOLD 2–4 COPD: Results from two replicate 48-week studies. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 629–645. [Google Scholar] [CrossRef] [PubMed]
- Koch, A.; Pizzichini, E.; Hamilton, A.; Hart, L.; Korducki, L.; De Salvo, M.; Paggiaro, P. Lung function efficacy and symptomatic benefit of olodaterol once daily delivered via Respimat® versus placebo and formoterol twice daily in patients with GOLD 2–4 COPD: Results from two replicate 48-week studies. Int. J. Chronic Obstr. Pulm. Dis. 2014, 9, 697–714. [Google Scholar] [CrossRef]
- Buhl, R.; Maltais, F.; Abrahams, R.; Bjermer, L.; Derom, E.; Ferguson, G.; Fležar, M.; Hébert, J.; McGarvey, L.; Pizzichini, E.; et al. Tiotropium and olodaterol fixed-dose combinationversusmono-components in COPD (GOLD 2–4). Eur. Respir. J. 2015, 45, 969–979. [Google Scholar] [CrossRef] [PubMed]
- Beeh, K.-M.; Westerman, J.; Kirsten, A.-M.; Hébert, J.; Grönke, L.; Hamilton, A.; Tetzlaff, K.; Derom, E. The 24-h lung-function profile of once-daily tiotropium and olodaterol fixed-dose combination in chronic obstructive pulmonary disease. Pulm. Pharmacol. Ther. 2015, 32, 53–59. [Google Scholar] [CrossRef]
- Singh, D.; Ferguson, G.T.; Bolitschek, J.; Grönke, L.; Hallmann, C.; Bennett, N.; Abrahams, R.; Schmidt, O.; Bjermer, L. Tiotropium + olodaterol shows clinically meaningful improvements in quality of life. Respir. Med. 2015, 109, 1312–1319. [Google Scholar] [CrossRef] [PubMed]
- Profita, M.; Bonanno, A.; Montalbano, A.M.; Albano, G.D.; Riccobono, L.; Siena, L.; Ferraro, M.; Casarosa, P.; Pieper, M.P.; Gjomarkaj, M. β2 long-acting and anticholinergic drugs control TGF-β1-mediated neutrophilic inflammation in COPD. Biochim. Biophys. Acta BBA Mol. Basis Dis. 2012, 1822, 1079–1089. [Google Scholar] [CrossRef]
- Beeh, K.M.; Burgel, P.-R.; Franssen, F.M.E.; Lopez-Campos, J.L.; Loukides, S.; Hurst, J.R.; Fležar, M.; Ulrik, C.S.; Di Marco, F.; Stolz, D.; et al. How Do Dual Long-Acting Bronchodilators Prevent Exacerbations of Chronic Obstructive Pulmonary Disease? Am. J. Respir. Crit. Care Med. 2017, 196, 139–149. [Google Scholar] [CrossRef]
- Ciciliani, A.-M.; Langguth, P.; Wachtel, H. In vitro dose comparison of Respimat® inhaler with dry powder inhalers for COPD maintenance therapy. Int. J. Chronic Obstr. Pulm. Dis. 2017, 12, 1565–1577. [Google Scholar] [CrossRef]
- Feldman, G.J.; Sousa, A.R.; Lipson, D.A.; Tombs, L.; Barnes, N.; Riley, J.H.; Patel, S.; Naya, I.; Compton, C.; Alcázar-Navarrete, B. Comparative Efficacy of Once-Daily Umeclidinium/Vilanterol and Tiotropium/Olodaterol Therapy in Symptomatic Chronic Obstructive Pulmonary Disease: A Randomized Study. Adv. Ther. 2017, 34, 2518–2533. [Google Scholar] [CrossRef]
- Navarrete, B.A.; Boucot, I.; Naya, I.; Tombs, L.; Lipson, D.A.; Compton, C.; Sousa, A.R.; Feldman, G. Umeclidinium/Vilanterol Versus Tiotropium/Olodaterol in Maintenance-Naïve Patients with Moderate Symptomatic Chronic Obstructive Pulmonary Disease: A Post Hoc Analysis. Pulm. Ther. 2018, 4, 171–183. [Google Scholar] [CrossRef]
- Kerwin, E.; Ferguson, G.T.; Sanjar, S.; Goodin, T.; Yadao, A.; Fogel, R.; Maitra, S.; Sen, B.; Ayers, T.; Banerji, D. Dual Bronchodilation with Indacaterol Maleate/Glycopyrronium Bromide Compared with Umeclidinium Bromide/Vilanterol in Patients with Moderate-to-Severe COPD: Results from Two Randomized, Controlled, Cross-over Studies. Lung 2017, 195, 739–747. [Google Scholar] [CrossRef]
- Moretz, C.; Bengtson, L.G.; Sharpsten, L.; Koep, E.; Le, L.; Tong, J.; Stanford, R.H.; Hahn, B.; Ray, R. Evaluation of rescue medication use and medication adherence receiving umeclidinium/vilanterol versus tiotropium bromide/olodaterol. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 2047–2060. [Google Scholar] [CrossRef]
- Tebboth, A.; Ternouth, A.; Guix, N.G.-R. UK-specific cost-effectiveness of tiotropium + olodaterol fixed-dose combination versus other LAMA + LABA combinations in patients with COPD. Clin. Outcomes Res. 2016, 8, 667–674. [Google Scholar] [CrossRef] [PubMed]
- Muraki, M.; Kunita, Y.; Shirahase, K.; Yamazaki, R.; Hanada, S.; Sawaguchi, H.; Tohda, Y. A randomized controlled trial of long-acting muscarinic antagonist and long-acting β2 agonist fixed-dose combinations in patients with chronic obstructive pulmonary disease. BMC Pulm. Med. 2021, 21, 28. [Google Scholar] [CrossRef] [PubMed]
- Schlueter, M.; Gonzalez-Rojas, N.; Baldwin, M.; Groenke, L.; Voss, F.; Reason, T. Comparative efficacy of fixed-dose combinations of long-acting muscarinic antagonists and long-acting β2-agonists: A systematic review and network meta-analysis. Ther. Adv. Respir. Dis. 2016, 10, 89–104. [Google Scholar] [CrossRef] [PubMed]
- Price, D.B.; Østrem, A.; Thomas, M.; Welte, T. Dual bronchodilation in COPD: Lung function and patient-reported outcomes—A review. Int. J. Chronic Obstr. Pulm. Dis. 2016, 12, 141–168. [Google Scholar] [CrossRef]
- Lee, H.W.; Park, J.; Jang, E.J.; Lee, C.-H. Comparisons of exacerbations and mortality among LAMA/LABA combinations in stable chronic obstructive pulmonary disease: Systematic review and Bayesian network meta-analysis. Respir. Res. 2020, 21, 310. [Google Scholar] [CrossRef]
- Albertson, T.E.; Bowman, W.S.; Harper, R.W.; Godbout, R.M.; Murin, S. Evidence-based review of data on the combination inhaler umeclidinium/vilanterol in patients with COPD. Int. J. Chronic Obstr. Pulm. Dis. 2019, 14, 1251–1265. [Google Scholar] [CrossRef]
- Ridolo, E.; Pellicelli, I.; Gritti, B.; Incorvaia, C. Patient-reported outcomes and considerations in the management of COPD: Focus on indacaterol/glycopyrronium bromide. Patient Prefer. Adherence 2019, 13, 145–150. [Google Scholar] [CrossRef] [PubMed]
- Derom, E.; Brusselle, G.G.; Joos, G.F. The once-daily fixed-dose combination of olodaterol and tiotropium in the management of COPD: Current evidence and future prospects. Ther. Adv. Respir. Dis. 2019, 13, 1753466619843426. [Google Scholar] [CrossRef]
- Miravitlles, M.; Baek, S.; Vithlani, V.; Lad, R. Optimal Bronchodilation for COPD Patients: Are All Long-Acting β2-Agonist/Long-Acting Muscarinic Antagonists the Same? Tuberc. Respir. Dis. 2018, 81, 198–215. [Google Scholar] [CrossRef] [PubMed]
- Bulkhi, A.; Tabatabaian, F.; Casale, T.B. Long-Acting Muscarinic Antagonists for Difficult-to-Treat Asthma: Emerging Evidence and Future Directions. Drugs 2016, 76, 999–1013. [Google Scholar] [CrossRef] [PubMed][Green Version]




{kind=link}
{kind=link}
{kind=link}
| Characteristics | COPD Medication | p-Value 1 | ||
|---|---|---|---|---|
| Ultibro (n = 177) | Anoro (n = 176) | Spiolto (n = 183) | ||
| Demographics | ||||
| Sex | ||||
| Female | 20 (11.3) | 26 (14.8) | 18 (9.8) | 0.47 |
| Male | 157 (88.7) | 150 (85.2) | 165 (90.2) | 0.61 |
| Age | 71.4 ± 7.37 | 71.3 ± 7.6 | 69.6 ± 7.8 | 0.47 |
| Weight | 72.3 ± 6.75 | 73.8 ± 7.6 | 73.3 ± 6.7 | 0.39 |
| Height | 167.5 ± 7.9 | 168.2 ± 5.01 | 165.2 ± 4.9 | 0.18 |
| Smoking (pack/year) | 36.9 ± 16.8 | 37.8 ± 27.94 | 36.6 ± 19.3 | 0.72 |
| Comorbidities | ||||
| Diabetes | 87 (49.2) | 81 (46.0) | 97 (53.0) | 0.17 |
| Hypertension | 67 (37.8) | 60 (34.1) | 68 (37.1) | 0.32 |
| Coronary artery disease | 58 (32.8) | 51 (28.9) | 53 (28.9) | 0.75 |
| Chronic heart failure | 49 (27.7) | 53 (30.1) | 55 (30.1) | 0.48 |
| Stratified by Type of Medication | COPD Medication | p-Value 1 | ||
|---|---|---|---|---|
| Ultibro (n = 177) | Anoro (n = 176) | Spiolto (n = 183) | ||
| Lung function parameters | ||||
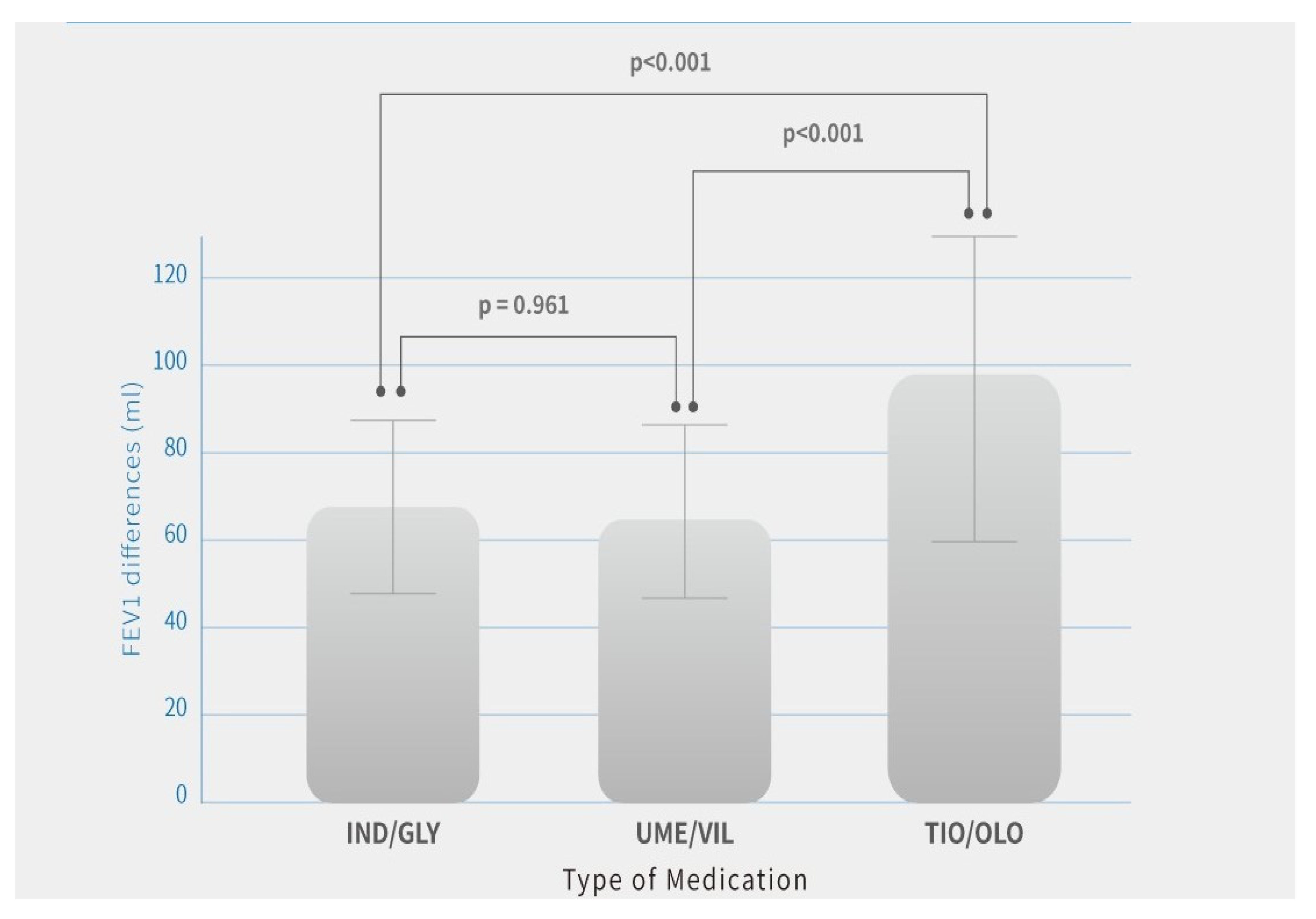
| FEV1 base (L) | 1.41 ± 0.18 | 1.4 ± 0.13 | 1.37 ± 0.17 | 0.64 |
| FEV1 base (% of predicted) | 46.74 ± 11.9 | 45.72 ± 8.0 | 45.59 ± 9.3 | 0.81 |
| FEV1 12 months (L) | 1.42 ± 0.16 | 1.45 ± 0.14 | 1.47 ± 0.16 | 0.52 |
| FEV1 difference after 12 months (mL) 2 | 65.2 ± 23.8 | 64.4 ± 24.1 | 98.7 ± 38.0 | <0.0001 |
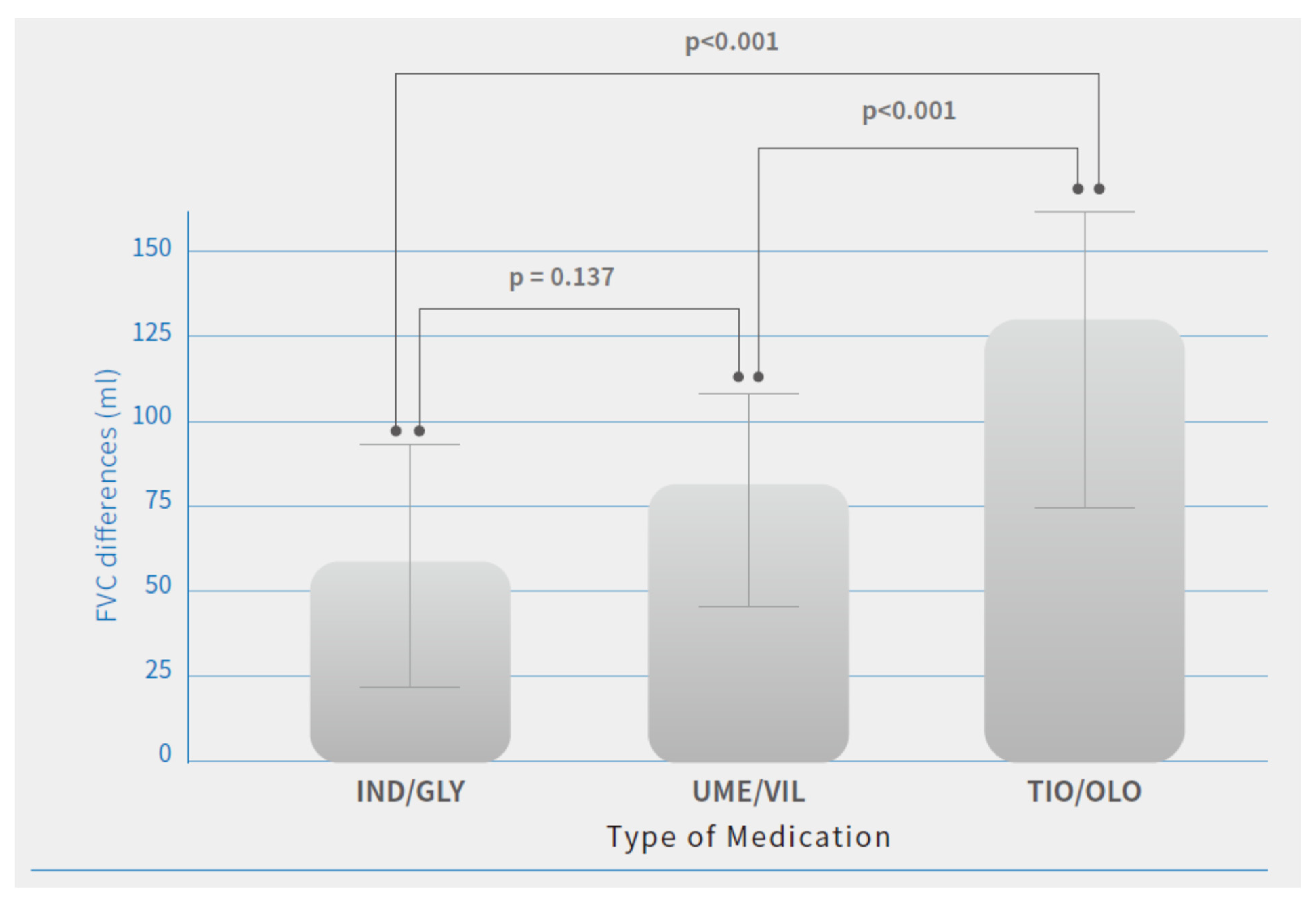
| FVC base (L) | 2.35 ± 0.26 | 2.36 ± 0.19 | 2.39 ± 0.22 | 0.61 |
| FVC base (% of predicted) | 47.6 ± 10.9 | 47.7 ± 7.2 | 48.1 ± 8.4 | 0.75 |
| FVC 12 months (L) | 2.42 ± 0.48 | 2.43 ± 0.19 | 2.52 ± 0.21 | 0.63 |
| FVC difference (mL) 2 | 58.2 ± 35.7 | 79.1 ± 35.2 | 127.3 ± 39.4 | <0.0001 |
| Symptoms Scores | ||||
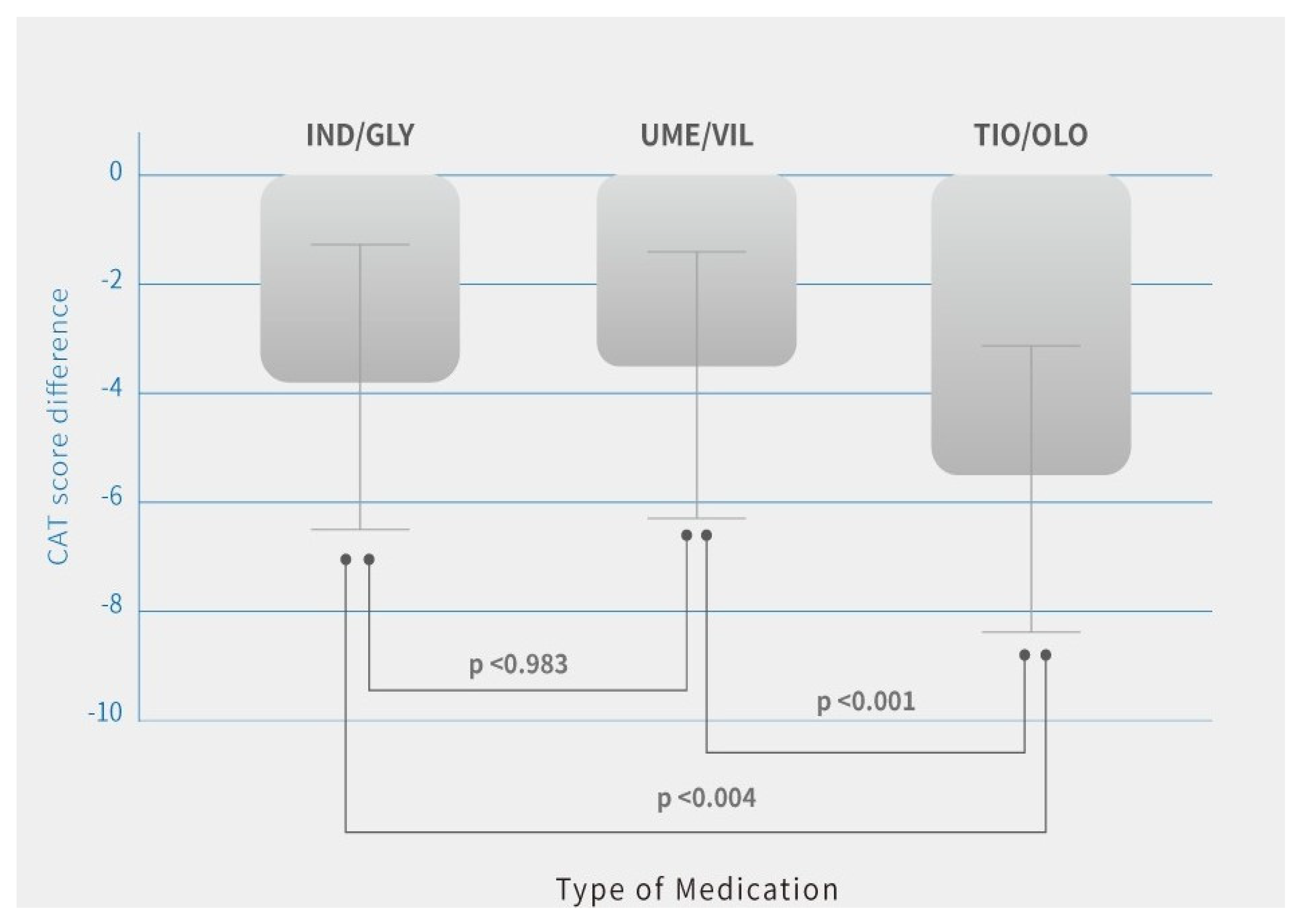
| CAT base | 14.8 ± 5.9 | 15.2 ± 5.8 | 15.7 ± 6.3 | 0.74 |
| CAT 12 months | 10.9 ± 6.1 | 11.3 ± 5.4 | 10.1 ± 5.1 | 0.37 |
| CAT score difference 2 | −3.8 ± 2.5 | −3.9 ± 2.2 | −5.6 ± 2.6 | 0.03 |
| Acute exacerbation of COPD | ||||
| No | 159 (89.8) | 155 (88.1) | 174 (95.1) | 0.58 |
| Yes | 18 (10.2) | 21 (11.9) | 9 (4.9) | 0.01 |
Publisher’s Note: MDPI stays neutral with regard to jurisdictional claims in published maps and institutional affiliations. |
© 2021 by the author. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Share and Cite
Cheng, S.-L. Comparison of Effectiveness Using Different Dual Bronchodilator Agents in Chronic Obstructive Pulmonary Disease Treatment. J. Clin. Med. 2021, 10, 2649. https://doi.org/10.3390/jcm10122649
Cheng S-L. Comparison of Effectiveness Using Different Dual Bronchodilator Agents in Chronic Obstructive Pulmonary Disease Treatment. Journal of Clinical Medicine. 2021; 10(12):2649. https://doi.org/10.3390/jcm10122649
Chicago/Turabian StyleCheng, Shih-Lung. 2021. "Comparison of Effectiveness Using Different Dual Bronchodilator Agents in Chronic Obstructive Pulmonary Disease Treatment" Journal of Clinical Medicine 10, no. 12: 2649. https://doi.org/10.3390/jcm10122649
APA StyleCheng, S.-L. (2021). Comparison of Effectiveness Using Different Dual Bronchodilator Agents in Chronic Obstructive Pulmonary Disease Treatment. Journal of Clinical Medicine, 10(12), 2649. https://doi.org/10.3390/jcm10122649